
Abstract
Aims: The aims of this study were to examine trajectories of headache in relation to retirement and to clarify the role of work stress and stress-prone personality.
Methods: Headache prevalence during the 7 years before and after retirement was measured by annual questionnaires from GAZEL cohort comprising French national gas and electricity company employees (n = 12,913). Odds ratios and 95% confidence intervals for headache during pre- peri- and post-retirement were calculated. The role of effect modifiers (work stress, type A or hostile personality) was tested by multiplicative interactions and synergy indices.
Results: An 11–13% reduction in headache prevalence was found during pre- and post-retirement, whereas decline was much steeper (46%) during the retirement transition. In absolute terms, the decline was greater among persons with high work stress or stress-prone personality than among other participants.
Conclusions: Retirement is associated with a decrease in headache prevalence, particularly among persons with a high amount of work stress or proneness to over-react to stress.
Introduction
Headaches are among the most frequent health complaints world-wide with substantial burden on individuals, their families and on society (1). As a neurological symptom, headache is experienced by nearly everyone at some point in life (2), while the global prevalence of headache disorders in general approaches 50% in the adult population (3). In Europe, migraine alone has been estimated to lead to annual costs of €27 billion, and the economic impact of other headache disorders, such as tension-type-headache (TTH), may be even greater due to higher prevalence rates (3).
While several factors may induce headaches, stress and psychological tension are among the most frequently reported (2,4–8). In epidemiological studies, both life and work stress have been found to be associated with an increased risk of future headache disorders (9–11). Certain personality traits, such as hostility, anger, aggression and type-A behaviour, which have long been associated with heightened cardiovascular (stress) reactivity (12–14), have also been reported to characterize persons with frequent headaches (15–21), One explanation to this latter association could be that certain types of personality may predispose an individual to heightened reactivity and vulnerability to work stress, which in turn may even further increase the overall risk of headaches.
Retirement transition is a life period when a natural relief from work-related stress occurs. In two recent studies on the French GAZEL cohort, statutory retirement was followed by improved sleep and lower rates of self-rated suboptimal health (22,23). Importantly, the burden of ill-health was substantially relieved by retirement for all but those with ideal working conditions. If an individual’s psychological attributes in combination with work stress play a role in headaches, the extent to which retirement affects the risk of headache could also be conditional on personality characteristics. However, evidence from large-scale prospective studies examining the magnitude and the temporal order of these associations is still lacking.
Thus, we explored the effects of statutory retirement on the prevalence of headache using a longitudinal study design with annual, self-reported measurements of headache from 7 years before to 7 years after retirement. We hypothesized that a decrease in headache prevalence would follow the retirement transition due to an overall relief from work-related stress. Further, we hypothesized that retirement-related decrease in headache prevalence would be more pronounced among participants who have high levels of stress at work as well as a personality type more prone to overreact to stress.
Subjects and methods
Study population and design
The GAZEL cohort was established in 1989 and is comprised of employees from the French national gas and electricity company, Electricité de France-Gaz de France (EDF-GDF) (24). At baseline, 20,625 employees (73% men), aged 35–50 years, agreed to participate. EDF-GDF employees hold a civil servant-like status that guarantees job security and opportunities for occupational mobility. Typically, employees are hired when they are in their 20s and stay with the company until retirement (usually around 55 years of age). Because of these characteristics, study follow-up is very thorough and losses to follow-up small (24).
The GAZEL participants are followed with an annual postal questionnaire mailed to the participants’ homes requesting data on health, life-style, individual, familial, social and occupational factors. Additionally, self-report data are linked to valid occupational and health data collected by the company, including data on retirement, long-standing work disability due to serious diseases, and sickness absence. The management, unions and the medical department of EDF-GDF gave their consent to the project and the usage of all personal and health data files (25).
In this study, we analyzed data from the GAZEL participants who retired on statutory basis between 1994 and 2006, inclusive (n = 15,837). Of these, we included only those who provided information on personality (measured in 1993) before retirement, and headache at least once before and once after the year of retirement. Thus, the sample consisted of 12,913 employees (10,354 men and 2559 women) whose mean age at retirement was 55 years (range, 41–63 years). The sample did not substantially differ from the eligible population in terms of mean age at retirement (55.2 years in the sample vs 55.2 years in the eligible population), the proportion of men (80% vs 79%) and occupational status (35% high, 54% intermediate, and 11% low grade vs 33% high, 54% intermediate and 13% low grade).
In this sample, we prospectively examined the long-term trajectories of self-reported headache 7 years before and after retirement among all statutory retirees, and further with only those with diagnosed migraine.
Data on retirement
All pensions are paid by a single employer, EDF-GDF, ensuring a homogeneous quality and comprehensiveness of the retirement data. Statutory age of retirement is 55–60 years, depending on the type of job. Partial retirement is rare but, in some cases, retirement can occur before the age of 55 years. For instance, women who have at least three children can retire after 15 years of service, their pensions being proportionate to the years served. In this study, we only included persons retiring on a statutory basis (96.2% of the sample), and excluded those retiring on health grounds, for example. We defined the year of statutory retirement based on the receipt of an official retirement pension.
Headache
Data on headache were obtained from responses to questionnaires during 1993–2007. An affirmative response (yes) to a question on the occurrence of migraine, headache (question: ‘Migraine’, ‘maux au tête’), from a checklist of over 50 medical conditions experienced during the past 12 months, was used as an indicator of headache in the survey year. We took into account all annual measurements of headache over a 15-year period which ranged from 7 years prior to retirement to 7 years after retirement using the year of retirement as year 0.
Effect modifiers
Work stress
Questions about psychological and physical job demands and job satisfaction, all assessed annually on an 8-point scale, were used to measure work-related stress. For each participant, we calculated the mean scores across all the pre-retirement period measurements (i.e. years −7 to −1) and dichotomized these. We defined the following three indicators of high work-related stress: being in the top quartile for psychological or physical work demands and being in the bottom quartile for job satisfaction. We also formed a combined dichotomous work–stress variable based on all above mentioned three stress indicators where having at least two of the above mentioned stress factors were considered as having high overall work related stress.
Personality
Personality was measured using two standardized personality scales widely considered in occupational stress research because of the possibility that these personality characteristics may moderate the effects of job stressors (26): The Bortner Rating Scale (27) to assess the type-A behaviour pattern and the Buss–Durkee Hostility Inventory (BDHI) (28) to measure general aggression and hostility. The Bortner Rating Scale consists of 14 different items, assessed on a 6-point Likert scale with high scores indicating type-A behaviour. The scale was validated for the French population against the Friedman and Rosenman structured interview for assessing Type-A with a 71.5% agreement. Type-A behaviour is characterized by traits such as impatience, aggressiveness, a sense of time urgency, and the desire to achieve recognition and advancement. The BDHI consists of 66 items with dichotomous ‘true/false’ answers. Total hostility score was calculated as a sum of seven different subscales: assault, verbal aggression, indirect hostility, irritability, negativism, resentment, and suspicion (internal consistency Cronbach’s α = 0.80). For both these personality scales, we used scores in the upper quartile to indicate type-A personality trait and high hostility.
Pre-retirement co-variates
Sociodemographic and work-related factors included sex, age at retirement, marital status, employment grade to assess socio-economic status (SES), and night work. Marital status (married or cohabiting vs single, divorced, or widowed), night work (never vs occasionally or regularly) and SES were defined according to the last measurement before retirement. SES was derived from the employer’s (EDF-GDF) records and classified into three groups: high grade (managers), intermediate grade (technical), and low grade (clerical and manual), based on categorisations of the French National Statistics Institute.
Health and health behaviour
All health-related variables were assessed using annual measures over the whole pre-retirement period (i.e. years −7 to −1) and even one affirmative response during this period was considered to indicate the presence of the particular health problem, medical condition or health behaviour. Presence of chronic diseases (cancer, diabetes, chronic bronchitis, asthma, angina, myocardial infarction, stroke, osteoarthritis, and rheumatoid arthritis) (0 = no chronic disease, 1 = at least one chronic disease), depression (0 = no depression, 1 = depression) and sleep disturbances (0 = no sleep disturbance, 1 = sleep disturbance) were derived from a checklist of over 50 medical conditions experienced during the past 12 months (29). Questionnaire data on the amount of beer, wine, and spirits consumed were transformed into units of alcohol per day. The average number of units per day over the pre-retirement period was classified as 0–3 units or more than 3 units (30). Survey reports on height and weight were used to calculate the average body mass index (BMI) over the pre-retirement period in order to identify normal weight (BMI < 25.0 kg/m2) and overweight (≥25.0 kg/m2) persons.
Statistical analysis
Associations between the pre-retirement co-variates and headache prior to retirement (0 = no headache in any of the 7 years before retirement, 1 = headache in any year before retirement) were analysed using logistic regression adjusted for sex and age at retirement. The changes in headache during 7 years before and after the retirement were analysed with a repeated-measures logistic regression analysis with the generalized estimating equations (GEE) method (31), which takes into account the within-subject correlation between headache measurements, and is not sensitive to missing measurements.
We calculated the annual prevalence estimates of headache and their 95% confidence intervals (CI) to characterize the headache trajectory in relation to statutory retirement for the 15-year period. The whole time window was then divided into three different periods referring to pre-, peri-, and post-retirement phases: Period 1 refers to the years before the retirement transition (years −7 to −2), Period 2 to those including the retirement transition (years −1 to +1), and Period 3 to the years after the retirement transition (years +2 to +7). We calculated the odds ratios (OR) and their 95% CIs for headache trend within each period, treating time as a continuous variable. The risk ratios were expressed as ORs per 3 years (this corresponds to the length of Period 2) within all periods. The model was adjusted for demographic characteristics (sex, SES, age at retirement), health (depression and chronic disease), work stress (psychological and physical work demands, and job satisfaction), personality (type-A personality and hostility,) and time of data collection (1993–1999 or 2000–2007; Model 1). Since sleep problems, a correlate of headache (32), have been found to decrease during retirement transition in this cohort, further adjustments were done using the annually measured sleep disturbances as a time-dependent co-variate (Model 2) (22). To test whether there were sex differences in trajectory patterns, we also added interaction terms ‘sex*year’ and ‘sex*year*period’ into the models. Since both interaction terms ‘sex*year’ and ‘sex*year*period’ were non-significant (P = 0.15 and P = 0.22, respectively) all subsequent analyses were calculated by combining men and women.
In further analyses, we explored the additive (synergistic) and multiplicative interactions by examining whether high work stress or personality (as potential effect modifiers) modified the headache trajectory. In order to assess the absolute risk differences, we explored the synergistic interaction between work, work stress and stress prone personality type (type A/hostile), by using the algorithm suggested by Andersson and colleagues (33). The synergy index (SI) is equal to calculation of [OR (AB)–1]/[(OR(Ab)–1 + (OR(aB)–1)], where A and B denote the presence of two risk factors and a and b are designated as the absence of the risk factors, respectively. We used being at work, type-A behaviour, hostility, and work stress (combined stress variable) as risk factors in our model, while being retired and having lower levels of type A behaviour, hostility or work stress were used as indicators of absence of risk. A synergy index of 1.0 implies perfect additivity and >1 indicates synergistic interaction. We also examined multiplicative interactions (i.e. the differences in headache trends within the periods by the level of each potential effect modifier) by testing the significance of an interaction term ‘effect modifier*year*period’ in a model including the main effects and all first level interactions. We calculated the odds ratios (95% CI) for headache by contrasting the trend of headache within each period for each level of the potential effect modifier. The models were adjusted for sociodemographic measures, pre-retirement health, sleep disturbances as a time-dependent co-variate and time of data collection.
Sensitivity analysis
We ran a sensitivity analysis using data from a sub-sample of 2500 subjects randomly selected from the GAZEL cohort from employees reporting regular headaches. They were sent a headache questionnaire in 1993 and migraine was diagnosed retrospectively using the International Headache Society (IHS) criteria of migraine (IHS categories 1.1 and 1.2), migrainous disorder (IHS category 1.7), or other episodic headaches (34,35). Of 2500 employees, 2051 (82%) answered to the questionnaire and 623 (30.4%) fulfilled the diagnostic criteria of migraine. Of these, a total of 417 individuals fulfilled the inclusion criteria of this study (i.e. retirement between 1994 and 2006, and at least 1-year follow-up of headache both in pre- and post-retirement) and were thus included in the sensitivity analysis. On this sample, we calculated the annual prevalence estimates of headache and ORs per 3 years and their 95% CIs within each period as described above, except that the length of pre- and post-retirement phases were determined as 5 years.
All analyses were conducted using the SAS v9.1 program (SAS, Inc., Cary, NC, USA).
Results
Characteristics of the study sample (n = 12,913), and associations between baseline co-variates and headache

Adjusted for sex, age at retirement and time of data collection.
Trajectories of headache
Figure 1 shows the annual prevalence (and 95% CI values) of headache in relation to retirement, adjusted for the time of data collection. There was an overall age-related decreasing trend in the annual prevalence of headache over the whole 15-year time-window. While a slight, but significant, decline in headache prevalence was found in Periods 1 and 3, a much steeper decline was noticed during peri-retirement years (Period 2), i.e. during the period covering retirement transition. Table 2 shows the trend in the occurrence of headache during the pre-, peri-, and post-retirement phases quantified as odds ratios per 3 years (95% CI). There was a highly significant difference between the trends in the three periods (interaction ‘time*period’; P < 0.0001) when adjusted for sociodemographic measures (sex, SES, age at retirement), health (depression and chronic disease), work stress (psychological and physical work demands, job satisfaction), personality (type A and hostility) and time of data collection. While the odds of headache per 3 years decreased by 11% (95% CI 8–14%) in the years preceding retirement and 13% (95% CI 9–17%) in the years following retirement, this decrease was 46% (95% CI 41–50%) during the retirement transition. These results remained mostly unchanged even after further adjustments for sleep problems used as a time-dependent co-variate.
Prevalence of headache in relation to retirement among all statutory retirees (n = 12,913), adjusted for time of data collection (1993–1999 or 2000–2007). The risk of headache during pre-, peri- and post-retirement phases among all statutory retirees (n = 12,913) and those with diagnosed migraine (n = 417) quantified as odds ratios (OR) per 3 years and their 95% confidence intervals (95% CI) Model 1 adjusted for demographics (age at retirement, sex and SES), health (chronic diseases and depression), work stress (psychological and physical work demands and job satisfaction), personality (type-A and total hostility), and time of data collection. Model 2 adjusted for (1) and sleep as a time-dependent co-variate.
P-value for year*period. Period 1 refers to the years before the retirement transition (years −7 to −2), Period 2 to those including the retirement transition (years −1 to +1), and Period 3 to the years after the retirement transition (years +2 to +7).

Synergistic effect of work stress and personality
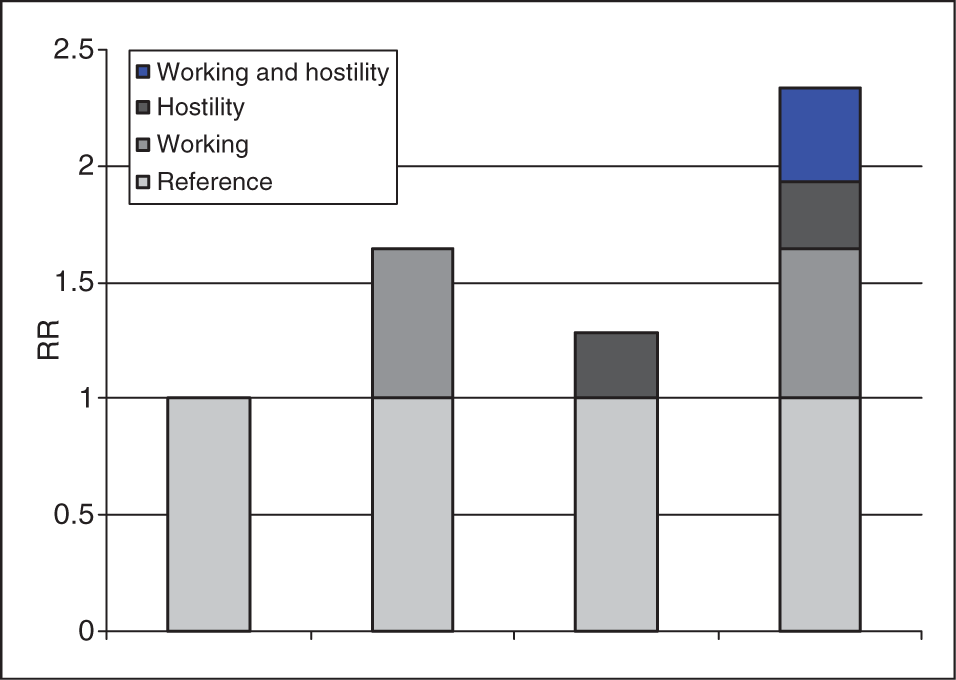
As indicated by synergy index (SI) > 1, the absolute risk of headache decreased more in persons with high-work stress compared to those with low-work stress (SI 1.79; 95% CI 1.42–2.27) when moving from working life to statutory retirement. Similarly, a synergistic interaction was found between retirement and type A personality (SI 1.39; 95% CI 1.20–1.59) and hostility (SI 1.43; 95% CI 1.27–1.61). These results suggest that persons with high-work stress, high hostility levels or type A personality benefited most from statutory retirement in absolute terms (Figures 2 and 3). Although a synergistic interaction was detected, in the multiplicative interaction testing, the assumed effect modifiers had no statistically significant impact on the headache trajectory profile on a logarithmic scale (i.e. all P-values for interactions ‘effect modifier*year*period’ were > 0.63, data not shown).
Relative risk of headache with contributions from different exposure categories (working status and type-A personality). Relative risk of headache with contributions from different exposure categories (working status and hostile personality).
Sensitivity analysis among a subgroup of migraineurs
The headache trajectory of migraineurs followed a similar pattern as found for headache among all retirees, with the sharpest decline in the prevalence of headache noticed during the retirement transition. The ORs showed that the headache prevalence declined by 46% during the retirement transition, while only 14% decline was noticed during pre-retirement and no changes during post-retirement years (Table 2).
Discussion
Main results
In this large, occupational cohort comprising French national gas and electricity company employees statutory retirement was associated with a substantial decrease in headache prevalence. The odds of reporting headaches decreased by 46% during the 3-year retirement transition compared to only a 11–13% age-related decrease per 3 years during pre- and post-retirement. This pattern was robust to adjustments for sociodemographic characteristics, health-related factors, personality, and work stress. In absolute terms, the decrease in headache around retirement was most pronounced in persons with high work stress or stress-prone personality, such as high hostility or type A personality. Our results support the hypothesis that a naturally occurring relief from work-related stress (i.e. transition to statutory retirement) leads to a substantial decrease in headache prevalence, one of the most common neurological symptoms in working-aged populations.
Strengths and limitations of the study
The main strength of this study is the annually repeated measurements of the outcome over an extended time window of 15 years. Even though causality cannot be inferred due to the observational study design, these results strongly suggest that the benefits in terms of decreased prevalence of headache are associated with retirement and that personality and work stress may drive these associations. Another strength is the large and stable occupational cohort with most employees retiring on a statutory basis.
The main limitation of our study was that we had to rely on self-reported data on headache. Since missing data of the headache were interpreted as absence of disease, some underestimation of the prevalence of headache is likely. Moreover, in the full sample, it was not possible to differentiate between headache in general and migraine. The headache question was derived from a checklist of different diseases inquiring about the existence of ‘migraine, headache’ using this exact phrasing. It is, thus, unclear whether the affirmative response to this item was prompted by the experience of migraine rather than headache in general. However, the sensitivity analysis restricted to randomly selected subsample of employees who reported headache and fulfilled the International Headache Society (IHS) criteria of migraine before retirement, showed a similar retirement-related trajectory in headache than that observed among all subjects. This suggests that a substantial decrease in headache prevalence over the transition to statutory retirement also applies to migraine. Moreover, from this subsample, we can estimate the portion of migraine sufferers among those reporting headache in the full sample of our study. When taking into account different sex distributions in the samples, the weighted mean of migraine prevalence in this study during the pre-retirement was 6.1% (4.3% men, 13.4% women), which is in line with previous prevalence studies (36,37). It is also noteworthy that even a formal diagnosis of migraine is rather unstable (35,38), and may fluctuate over time. In previous studies conducted on the GAZEL cohort, 1-year reproducibility of reporting migraine symptoms was only moderate (38), and only 37% of those with a migraine diagnosis retained it 10 years later (35).
Comparison with previous studies
To the best of our knowledge, the present study is the first to examine prospectively the effects of retirement on headache, rendering difficult comparisons with previous studies. Our findings of a substantial decrease in the occurrence of headache following retirement lend our hypothesis and are also in line with the results of previous studies published on the GAZEL cohort showing the benefits of statutory retirement on self-rated health and sleep (22,23). Improvements in health and psychological well-being around retirement transition have previously been reported also in some other studies (39–44). However, earlier cross-sectional analyses have found no differences in headache prevalence between working and retired persons (45).
Prior to retirement, headache was significantly related to both high work stress, and type-A and hostile personality types, which is in agreement with previous studies conducted especially among migraineurs (9,11,13,15). Recently, it has been suggested that stress may modify migraine in many different ways; it can be a predisposing factor for a headache disorder onset, or it can trigger migraine attacks and amplify their intensity and duration. Moreover, migraine itself may act as a considerable stressor in a person’s life and thus lead to a vicious cycle of increasing migraine attacks. Biologically, stress and migraine may be linked in at least two ways. First, activation of the hypothalamic–pituitary–adrenocortical (HPA)-axis and the sympathetic nervous system noticed in response to stress, may also trigger migraine attacks or affect migraine in other ways. Contrary to acute stress, chronic stress may also induce hyperalgesia and central sensitization, potentially by activating NMDA and µ-receptors. Second, chronic stress may alter the immune system so that pain transmission is facilitated at the neuronal level (46,47). Higher reactivity to stress found both among type-A and hostile personality types may, in turn, explain their association with headache.
Although tests for multiplicative interaction did not reach statistical significance at conventional levels, all tests of synergistic interaction were significant suggesting that high work stress and stress-prone personality affected the occurrence of headache synergistically. The absolute risk differences in headache prevalence between pre- and post-retirement were larger among retirees perceiving high work stress or having stress-prone personality. This implies that these groups benefited the most from retirement in absolute terms.
Generalizability
In the present context, the French national gas and electricity company, in which the workers enjoy substantial benefits (e.g. stable job status guaranteed by a civil-servant-like status, low statutory retirement age, and high pensions, 80% of the previous salary), it is likely that retirement was perceived as a positive, rather than stressful life event by the majority. Due to these particular characteristics, the results may not be generalizable to other working cohorts, even in other Western countries. Furthermore, in large cohorts, where the participants are followed by surveys for a long time, persons with severe illnesses or functional impairments are likely to drop out creating a healthy-survivor effect. Since headache and especially migraine is associated with many other health problems, it is possible that persons with the severest conditions were actually lost to follow-up. Further research is needed to examine whether our findings apply across different pension schemes, including settings where people retire later. The mechanisms explaining the post-retirement decrease in headache prevalence is also an important topic for future studies. Removal of a major source of stress (i.e. work) could explain the observed associations, but retirement may also allow people more time to engage in stimulating and restorative activities which, in turn, could decrease headaches as previously shown in migraine (48). Furthermore, a more detailed analysis about the effects of retirement and work stress on primary headaches (especially migraine and tension type headache) would be helpful when trying to clarify the role of work stress in specific headache disorders.
Conclusions
In this occupational cohort of 12,913 French national gas and electricity company employees, a clear decrease of headache prevalence was found at statutory retirement. These results add to the growing body of evidence that shows mainly beneficial health effects of statutory retirement. Our results also highlight the role of individual differences during major life transitions, suggesting that those with high stress during working life or dispositional over-reactivity to stress may actually benefit most from retirement.
Footnotes
Acknowledgements
The authors express their thanks to EDF-GDF, especially to the Service Général de Médecine de Contrôle, and to the Caisse centrale d’action sociale du personnel des industries électrique et gazière. We also wish to acknowledge the Cohortes team of the Unit Inserm 1018-Versailles St-Quentin University responsible for the GAZEL data base management.
The GAZEL Cohort Study was funded by EDF-GDF and INSERM, and received grants from the Cohortes Santé TGIR Program, Agence nationale de la recherché (ANR) and Agence française de sécurité sanitaire de l’environnement et du travail (AFSSET). The Hemicrania study (sub-cohort) was funded by GlaxoSmithKline laboratories. In addition, the study was supported by the BUPA Foundation, the Social Insurance Institution of Finland and the Academy of Finland (project numbers 117 604, 124 271, 124 322, 126 602).