
Abstract
Trigeminal autonomic cephalgias (TACs) include a spectrum of primary headache syndromes associated with cranial autonomic dysfunction. Other types of headache and facial pain syndromes can be associated with marked localized facial or ear autonomic changes. We report on a group of patients suffering from episodic migraine with cranial autonomic features, patients with different presentations of the ‘red ear syndrome’ (RES), cluster headache with prominent lower facial involvement and crossover cases. In our experience crossover between TACs and migraine, RES and cluster headache is not uncommon. We propose that all these conditions belong to the same group and a unifying causative mechanism is proposed.
Introduction
Trigeminal autonomic cephalgias (TACs) are important to recognize as accurate diagnosis can lead to effective therapy in many cases. TACs include cluster headache (CH), episodic and chronic paroxysmal hemicrania (EPH and CPH), short-lasting unilateral neuralgiform headache with conjunctival injection and tearing (SUNCT), and cluster–tic syndrome (1). TACs usually cause severe unilateral orbital, supraorbital or temporal pain of variable frequency and duration. Autonomic symptoms can include a combination of conjunctival injection, lacrimation, nasal congestion, rhinorrhoea, ptosis, eyelid oedema and Horner's syndrome.
Trigeminal autonomic dysfunction has been reported to occur in otherwise typical cases of migraine (2–4), perhaps representing a crossover between CH and migraine.
Lance reported a small group of patients who suffered from episodic pain and erythema in the C2 and C3 distribution, describing this as the ‘red ear syndrome’ (RES) (5, 6). We report our experience with a spectrum of cases with similarities to the TACs, including RES, but in whom the type or localization of the pain and the pattern of autonomic dysfunction differ from that previously described.
Case reports
The patients reported were seen in the Headache Service at the Mid-Yorkshire NHS Trust, Wakefield, UK over a period of 6 years.
Migraine headache presenting with clustering and/or trigeminal autonomic dysfunction
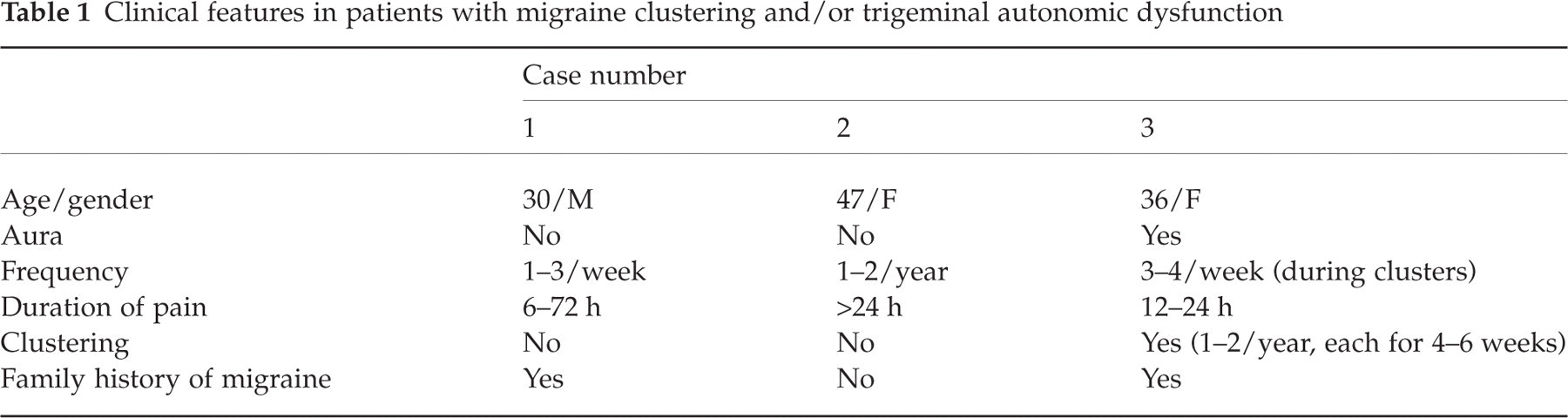
We have seen three such cases (Table 1); two presented with episodic migraine without aura and one with aura. All experienced variable degrees of ptosis, conjunctival injection and tearing, nasal congestion and rhinorrhoea. This started after the onset of the pain and was most prominent at the height of the pain. The autonomic symptoms resolved within 30–60 min but the pain lasted for more than 6 h.
Clinical features in patients with migraine clustering and/or trigeminal autonomic dysfunction
Red ear syndrome
Twelve patients were seen over a period of 6 years (Table 2). With the exception of cases 12 and 14, all experienced provoked or unprovoked episodic non-side shifting attacks of pain, redness, and hotness of one ear. Change in temperature was a common trigger. This included having a shower as well as exposure to cold weather. In those with temporomandibular joint (TMJ) dysfunction, lying on the affected side of the face and touching the TMJ could trigger the condition. Pain in some cases, although most pronounced in the ear, also affected the cheek, the area behind the ear, the upper posterior aspect of the neck on the same side, and, in some, the temple. The hotness and redness were limited to the ear. None of the patients experienced changes in the lid, eye, or nose. The attacks were of variable frequency (less than one per month to a maximum of four per day) and duration (10 min to 3 h). In none was an abnormality found on imaging of the brain or the cervical spine. Six experienced TMJ pain and tenderness (cases 5, 7, 9, 10, 11, and 13). In three (cases 6, 8, and 9) of the five also known to have migraine, the attacks of RES did not happen in association with their migraine. In the other two (cases 12 and 14) the RES happened in strict association with migraine headaches. In case 12 the migraine headache could affect either the right or the left side, but the RES occurred only in the more severe right-sided attacks. In case 14 the migraine and RES were non-side shifting (left side). In both, the RES developed as the migraine headache built up in severity.
Clinical features of patients with red ear syndrome (RES)

Standard analgesics and non-steroidal anti-inflammatory drugs were of little help. Only two patients (both having RES with TMJ dysfunction) tried triptans during flare ups with limited benefit. Only those with more frequent attacks agreed to take preventative medication (cases 4, 6, 8, 9, 10, 11, 13 and 15). With the exception of case 13, gabapentin proved to be particularly helpful in reducing the frequency of the attacks, including the pain and the changes in the affected ear. Indomethacin was tried in four patients (initial dose 25 mg once daily, gradually increasing to 50 mg three times a day after 7–10 days, keeping highest dose achieved for 5 days and stopping if ineffective), only one (case 13) responding well (25 mg twice daily). In her, the improvement was quite dramatic. Prior to indomethacin she was almost housebound in cold weather as exposure to cold was a significant trigger factor.
Red ear syndrome associated with widespread facial pain and autonomic dysfunction (red ear syndrome plus)
We report on six such patients (Table 3). The pain was of variable frequency (less than one per month to five or more per day) and duration (10 min to non-remitting). In four (cases 16–19) the pain as well as the change in temperature and colour affected a wide area and included the ear, face and in one (case 17) the upper part of the neck on the same side. The same patient reported symptoms typical of TACs (conjunctival injection, tearing and nasal blockage) occurring at the same time as the more widespread symptoms. Furthermore, her attacks happened in clusters but were not sleep related. Similar symptoms affecting the inside of the mouth and the throat on the same side were reported (cases 16 and 20). None reported increased sweating on the side of the ear involved. None of these episodes was triggered by exercise.
Clinical features of patients with red ear syndrome (RES) plus

Two patients (cases 20 and 21) presented with similar features but reddening affected a circumscribed area on the cheek rather than the ear. Magnetic resonance imaging (MRI) of the brain and cervical spine in all and computed tomography of the head in case 21 were normal.
Cluster headache with lower facial pain
We have seen four patients presenting with features highly suggestive of CH, in whom the pain was either predominately or selectively lower facial (Table 4). The first three patients (cases 22, 23 and 24) experienced orbital and temporal as well as lower facial pain during their clusters. In the last (case 25) some of the clusters affected the orbit and temple and some only the lower face. All four patients experienced autonomic dysfunction, in the form of conjunctival injection, tearing and rhinorrhoea in association with the headache. Case 24 is particularly interesting. She presented with episodic CH, averaging one cluster per year, each lasting nearly 5 weeks. The pain, which was sleep related, was a non-side shifting right-sided pain, which always affected the right side of the head, face and ear. The pain was most marked in the eye and lower jaw. In addition to the conjunctival injection, tearing and rhinorrhoea, the right side of the face and the right ear felt hot and was red.
Clinical features of patients with lower facial cluster headache

Discussion
We report on a spectrum of clinical presentations where headache, ear and/or facial pain were associated with features suggestive of localized hyperaemia/autonomic dysfunction. These include migraine sufferers who experienced symptoms suggestive of cranial autonomic dysfunction as is seen in TACs, patients with RES, some with hyperaemia spread beyond the affected ear, and patients with CH with a tendency for the pain and sometimes the autonomic changes to be more prominent outside the ophthalmic division of trigeminal nerve distribution.
In the first group, migraineurs experienced cranial autonomic symptoms during their migraine attacks. There was a tendency for clustering in one and the symptoms of autonomic dysfunction were similar to those seen in TACs. The characteristics, the duration, and the associated features were those of migraine rather than of CH. Migraine with cranial autonomic features has been reported in a number of patients (2–4). This association, though of uncertain frequency, raises the possibility that the trigeminal-autonomic reflex can be active in some cases of migraine to account for the parasympathetic vasodilatation. Goadsby and Lipton suggested that in TACs there should be a pain threshold above which autonomic symptoms can develop (1).
Lance described a condition characterized by episodic unilateral ear discomfort or burning pain associated with hotness and redness (5, 6). He found an association with a variety of conditions including C2/C3 radiculopathy, and TMJ dysfunction in 10 of his 12 patients. Two had atypical glossopharyngeal neuralgia and one had atypical trigeminal neuralgia. Thus some had ‘central causes’ (upper cervical root disease and the different neuralgias) and some had a ‘peripheral cause’ (those with TMJ) for their RES. No associated pathology was detected in two of his patients.
We were unable to document any pathology of upper cervical roots or meninges on MRI studies in any of our patients. In one the condition followed neck trauma as a result of a road traffic accident, yet no MRI abnormalities were found.
Several other cases of ‘primary’ or ‘secondary’ RES have been reported (7–14). A strong association with migraine has been described (7, 8, 14). Sometimes the RES developed during the headache phase (7, 14), and sometimes as a trigger or ‘aura’ for migraine (8). RES has also been reported to happen during PH (9), in association with ‘extratrigeminal EPH’ (10), and SUNCT (11).
The association with migraine is interesting. Eight of our 18 patients with RES and RES plus (groups II and III) had migraine as well. In only two (cases 12 and 14) did the RES seem to develop during the migraine attacks. Raieli et al. reported on eight patients with a similar association (7). Hirsch suggested that bilateral bright red discoloration of the ears was not rare in migraine (17). It therefore seems that neuronal mechanisms in migraine are not only capable of stimulating the trigemino-autonomic reflex (to account for the cranial autonomic features in group I) but can also stimulate a cervical autonomic reflex resulting in the RES.
In eight out of 18 of our patients with RES or RES plus, there was an association with TMJ dysfunction, lying on the affected side and a change in temperature, particularly exposure to cold as well as having a shower. RES usually followed exacerbations in the TMJ pain, thus perhaps exceeding the pain threshold required to trigger autonomic dysfunction.
Lance postulated that where an upper cervical lesion is present, an antidromic discharge of impulses along the C2, C3 roots causes pain and vasodilation in the ear by the release of vasodilator peptides such as calcitonin gene-related peptide (CGRP), substance P and nitric oxide. A local axon reflex, leading to the release of vasodilator peptides, could explain cases of RES associated with TMJ dysfunction. There is experimental evidence to suggest that stimulation of the third cervical root caused vasodilation in the ear, the part of the cheek immediately in front of the ear and a strip running down the lower border of the mandible to the neck (15). These two mechanisms offer an explanation for the ‘secondary’ cases of RES. They suggest that there is stimulation of a localized ear/TMJ reflex in some patients and a spinal-autonomic reflex arc in others.
Most of our patients with RES or RES plus (10 out of 18) either had migraine or no associated conditions. An inclusive hypothesis is required to explain both the ‘primary’ as well as the ‘secondary’ cases. The presence of a cervico-autonomic reflex, perhaps connected to or influenced by the trigemino-autonomic reflex, might explain both. Antidromic discharge of impulses along the C3 root, either arising peripherally (TMJ) or arising in the root itself, can induce autonomic changes by stimulating the presumed cervico-autonomic reflex. Primary cases can be caused by either a centrally or a peripherally generated stimulation, which can also involve the trigemino-autonomic reflex. This is particularly true where the autonomic features are not limited to the ear.
The lower facial presentation of CH and the association of some TACs with RES (9–11) are challenging. It is recognized that the pain in CH can affect the lower face as well as the upper face in up to 65% of patients with chronic CH and 40% in episodic CH (16). Interestingly, in the same group of patients the pain was reported to have affected the ear in 15–17% of patients but the autonomic changes did not. In patient 24 the pain was predominantly upper facial in the majority of his clusters, but in two of his clusters the pain was predominantly lower facial. Identical features of autonomic dysfunction were present in all attacks. Case 23 presented with attacks of CH with its classical clustering, relation to sleep and typical autonomic features, yet the hyperaemia was not limited to the eye as it also affected the side of the face and the ear on the same side. Case 16 had similar presentation concerning the pain and autonomic dysfunction, the only difference from case 23 being that the pain and hyperaemia were more marked in the ear than the eye.
A unifying hypothesis is required to explain TACs, RES, RES plus, and crossover cases. The facial skin has sympathetic vasoconstrictor and vasodilator fibres (18). We propose that in TACs parasympathetic vasodilation explains the autonomic dysfunction via a reflex connection between the trigeminal and parasympathetic fibres in the facial nerve (19, 20). In RES (group II), where the autonomic dysfunction was limited to the ear, inhibition of sympathetic vasoconstriction or activation of parasympathetic vasodilation can offer the explanation for the RES. This, as suggested by Lance, can be through either central or peripheral mechanisms (6). Crossover cases suggest connection to and cross-reactivity between the trigemino-autonomic reflex suggested by Goadsby and Lipton and the cervico-autonomic reflex suggested by Lance.
Two patients presenting with otalgia and a sensation of external ear obstruction were reported to respond well to indomethacin, leading to a conclusion that this was a variant of chronic paroxysmal hemicrania (9), and a further case with left occipital headache associated with left ptosis, conjunctival injection and redness of left ear, again responding well to indomethacin, was considered to be extratrigeminal EPH (11). We feel that despite possible crossover cases, RES is a separate syndrome. We have not observed response to indomethacin in the cases where it was tried. We recommend gabapentin as the first-line management, with appropriate attention to any associated conditions. Verapamil is helpful in some patients.
In our experience, RES and crossover cases are not uncommon. This group of conditions is perhaps better grouped together with TACs and we propose the term ‘trigeminal cephalgias and facial pain syndromes associated with autonomic dysfunction’. Moreover, these symptoms should not be confused with Harlequin syndrome, where the complaints of unilateral facial flushing and sweating are actually normal functions compared with the abnormal opposite side due to contralateral sympathetic deficit (22).