
Abstract
Aim: The purpose of the study was to estimate the one-year prevalence of migraine among a population-based sample of Spanish adults.
Method: Men and women aged 18−65 years were selected at random according to quotas for age, sex, size of habitat (<10,000 inhabitants, 10,001−50,000 inhabitants, 50,001−200,000 inhabitants and >200,000 inhabitants) and residence proportional to the population size of the geographical location. A random-digit-dial, computer-assisted telephone interview (CATI) survey was conducted between April and July 2006. The 2004 International Headache Society operational diagnostic criteria were applied.
Results: From a total of 70,692 telephone calls and 26,255 (31.7%) valid contacts, 5,668 (21.6%) respondents completed the CATI survey. A total of 476 subjects (8.4%, 95% confidence interval [CI] 7.7−9.1%) with strict migraine and 236 with probable migraine (4.2%, 95% CI 3.7−4.7%) were recorded. The 1-year prevalence of total migraine (N = 712) was 12.6% (95% CI 11.6−13.6) (17.2% in females, 8.0% in males). The prevalence rates showed significant geographic variations, from 7.6% in Navarra to 18% in the Canary Islands. One-half of the subjects had migraine with aura. One-third of subjects were never diagnosed for migraine.
Conclusions: The one-year prevalence of migraine in Spain is 12.6%, with a prevalence of migraine with and without aura of 8.4% and probable migraine of 4.2%. These findings add data to the current understanding of migraine.
Introduction
There is an increasing awareness that migraine constitutes a major public health problem worldwide. Migraine is a very common disorder, affecting about 11−13% of adult populations in Western countries, that has a substantial impact on the individual and society (1,2). Migraine is most prevalent during the peak productive years and has a negative influence of the quality of life, and health economic studies have consistently documented the high medical care use and indirect costs associated with this disabling medical condition (3−6). Remarkably, despite high levels of temporary disability, many migraineurs have never consulted a physician for the problem, which in turn has introduced selection bias in migraine studies based on patients who seek treatment rather than persons from the general population (7).
Although numerous studies of migraine prevalence have been published, reviews of the epidemiological literature have shown a large variation in the prevalence rates, which is mostly explained by differences in sociodemographic profiles of the study subjects, survey methods and case definition (8−12). The introduction of the International Headache Society (IHS) criteria for migraine in 1988 (13) has been a major step toward the standardization of the diagnosis of migraine and toward overcoming methodological heterogeneity across studies. However, knowledge of the migraine-related burden is still incomplete and it is necessary to add data from population-based prevalence surveys in a variety of countries using the IHS criteria to gain an overall picture of the prevalence of this disorder. The aim of the present study was to estimate the one-year prevalence of migraine among a population-based sample of Spanish adults. This is the first epidemiological study of migraine in Spain in which the 2004 IHS operational diagnostic criteria (14) have been applied.
Methods
Sample and survey
A cross-sectional, population-based study was conducted between April and July 2006 in the framework of the PALM program (Action Plan Against Migraine; Plan de Acción en la Lucha contra la Migraña). The primary aim of the study was to determine the one-year prevalence of migraine in Spain. The secondary aim was to assess the criteria validity of a questionnaire based on the 2004 IHS criteria for migraine (14) for a computer-assisted telephone interview (CATI). Estimating the social, work-related and personal impact of migraine in Spanish adults was also an aim of the PALM program, but these results will be reported separately. For the purpose of the present survey, men and women aged 18−65 years from mainland Spain, the Balearic Islands and the Canary Islands were eligible provided that he/she was a permanent resident of the contacted household, conversely easily in Spanish and gave express oral consent for the telephone interview. The study protocol was approved by the Ethics Committee of Hospital Clínico San Carlos of Madrid.
Sampling was performed using a non-proportional stratified procedure for the variable geographical location (200 households per autonomous community) and a proportional stratified procedure for the size of habitat (<10,000 inhabitants, 10,001−50,000 inhabitants, 50,001−200,000 inhabitants, and >200,000 inhabitants). Eligible respondents were selected at random according to quotas for age, sex and size of habitat proportional to the population size of the geographical location. Household samples were drawn by the random-digit-dialing procedure using the computerized telephone directory database, in which 96.3% of Spanish households are included (15). Up to 10 attempts were made to contact each household by 43 interviewers with specific training for the study.
According to a prevalence of migraine in the general population of 12% (16), for a 95.5% confidence level (CI) (coverage factor k = 2) in the most unfavorable sampling conditions (p = q = 50%), with a maximal error per province of ± 10% and a total error sampling of ± 1.4%, a total of 5,000 valid interviews were needed. To obtain this sample size, it was estimated that approximately 30,200 telephone contacts were required.
Interview
The survey was conducted using a CATI procedure as described by Lipton and co-workers (16). Briefly, before proceeding to the interview, the purpose of the survey was described. Subjects were told that the interview would require 10 to 20 minutes to complete. Verbal informed consent was obtained. The survey was conducted using the CATI procedure. The CATI was required because of the complex branching patterns in the questionnaire. To obtain a census of the household and identify all eligible subjects (between the ages of 18 and 65 years), the gender and age of each household member were first ascertained.
The interview began with the following question: “In the past year, have you had al least one headache, other than those cause by a head injury, a hangover, pregnancy, or an illness such as a cold or the flu?” If this question was answered in the affirmative, detailed questions were asked about whether headache was diagnosed by a clinician and the severe types of headaches that occurred in the previous 12 months, including all of the diagnostic features of migraine specified by the IHS, including age at onset, headache frequency, duration, pain intensity and disability (e.g. missed work, interference with daily activities, amount of bed rest required). Subsequently, questions were asked about location and quality of pain, exacerbation of pain by physical activity and the occurrence of nausea, vomiting, photophobia, phonophobia and visual or sensorimotor aura. For each headache feature reported, a follow-up question established how often it occurred (rarely, less than half the time, half the time or more), and when nausea, photophobia or phonophobia was reported, a further question was asked about its intensity (mild, moderate, severe). At the end of the interview, besides age and sex, which were the first items ascertained, the following demographic data were recorded: education level, income and work status. Finally, in case of suspicion of migraine, the subject was asked if he/she would grant a face-to-face interview at home to collect data on the impact of migraine on the social, work and personal spheres (data not shown).
Case definition
Respondents were identified as suffering from migraine with aura (category 1.1), without aura (category 1.2) and probable migraine (category 1.6) as defined by the diagnostic criteria of the IHS (14). Migraine cases without aura had to fulfill criteria A (five or more lifetime attacks), B (duration of attacks between 4 and 72 hours), C (at least two of the following characteristics: moderate to severe intensity, exacerbation on movement, unilateral location and pulsatile quality), D (nausea/vomiting or photophobia and phonophobia) and E (not attributed to another disorder). To meet IHS criteria for migraine with aura, individuals had to fulfill criteria A (at least two lifetime attacks), B (aura with at least one of the following characteristics: reversible visual symptoms [e.g. spots, stars, lines, flashing lights], reversible sensorimotor symptoms [numbness or tingling] and reversible aphasia or unclassifiable speech difficulty), C (at least two of the following characteristics: homonymous visual disturbance and/or unilateral sensorimotor symptoms, and at least one aura symptom that develops gradually over more than four minutes, or two or more symptoms occuring in succession, with no aura symptom lasting more than 60 minutes), D (headache starting with aura or following aura with free interval of at least 60 minutes) and E (not attributed to another disorder). Probable migraine (category 1.6) was defined when one criterion from the definition of migraine with or without aura was missed. ‘Strict migraine’ was defined as migraine with or without aura (categories 1.1 or 1.2) and ‘total migraine’ as the sum of strict migraine (categories 1.1 or 1.2) and probable migraine (category 1.6). ‘Mixed type’ of migraine was defined as fulfilling criteria for both migraine with and without aura.
In order to assess the criteria validity of the migraine diagnostic questionnaire adapted from the IHS criteria (16) and used in the telephone interview, a pilot sample of subjects selected at random with and without fulfilling diagnostic criteria of strict migraine in the CATI survey were visited by a neurologist who was blind to the results of the interview. For a CI of 95.5% and a sampling error between 12% and 15%, a sample size of 44 subjects with positive migraine diagnosis and 70 subjects with negative migraine diagnosis were required. According to results of the validation study, which involved 50 subjects (17), the migraine diagnostic questionnaire used in the CATI survey and based on the 2004 IHS criteria (14) had a sensitivity of 81.5% (95% CI 66.8–96.1%), specificity of 91.3% (95% CI 79.8–100%), positive predictive value of 91.7% (95% CI 80.6–100%), and negative predictive value 80.8% (95% CI 65.6–95.9%).
Analysis
Overall and autonomous community-specific estimates of migraine prevalence were adjusted for age, gender and size of habitat. Data are expressed as percentages for categorical variables or mean and standard deviation (SD) and the 95% CI for continuous data. The Chi-square (χ2) test was used in the univariate comparison of categorical variables. Statistical analyses were performed using the SPSS computer program (version 11.5) (SPSS, Chicago, IL, USA) for Windows. Statistical significance was set at p < 0.05.
Results
From a total of 70,692 telephone calls, 26,255 valid contacts were made, representing a rate of 37.1%. Of these, 5,668 (21.6%) completed the CATI survey. The remaining individuals were excluded for the following reasons: refusal to take part in the study (N = 11,981 [45.6%]), respondents were out of quota (N = 8,287 [31.6%]) and respondents withdrawn during the interview (N = 319 [1.2%]) (Figure 1).
Distribution of respondents to the CATI survey and one-year prevalence of migraine. CATI = computer-assisted telephone interview.
There were 2,861 (50.5%) males and 2,807 (49.5%) females. As shown in Table 1, the distribution of subjects by age and gender coincided with that of the Spanish general population (18). Of the total 5,668 respondents, 476 met the criteria of strict migraine (categories 1.1 and 1.2) and 236 met the criteria of probable migraine (category 1.6). Therefore, the one-year prevalence rate of total migraine was 12.6% (95% CI 11.6–13.6%) (712/5,668), with a prevalence rate of strict migraine of 8.4% (95% CI 7.7–9.1%) and prevalence rate of probable migraine of 4.2% (95% CI 3.7–4.7%). The prevalence of migraine in women was 17.2% (482/5,668) in females as compared with 8.0% (230/2861) in men. The prevalence of migraine was significantly higher in people under 40 years of age as compared with subjects in the 50−59 and 60−65-year strata (p < .01) (Table 2). On the other hand, the prevalence rate of total migraine was higher in women than in men for all age groups (18−29 years 8.1% vs. 5.2%; 30−39 years 10% vs. 5.1%; 40−49 years 10% vs, 3.2%; 50−59 years 8% vs. 3.5%; 60−65 years 3.9% vs. 1.5%) (Figure 2).
Prevalence rates of total migraine in men and women according to age. Demographic characteristics of the 5668 respondents that completed the CATI survey CATI = computer-assisted telephone interview. Distribution of 712 subjects with migraine by age group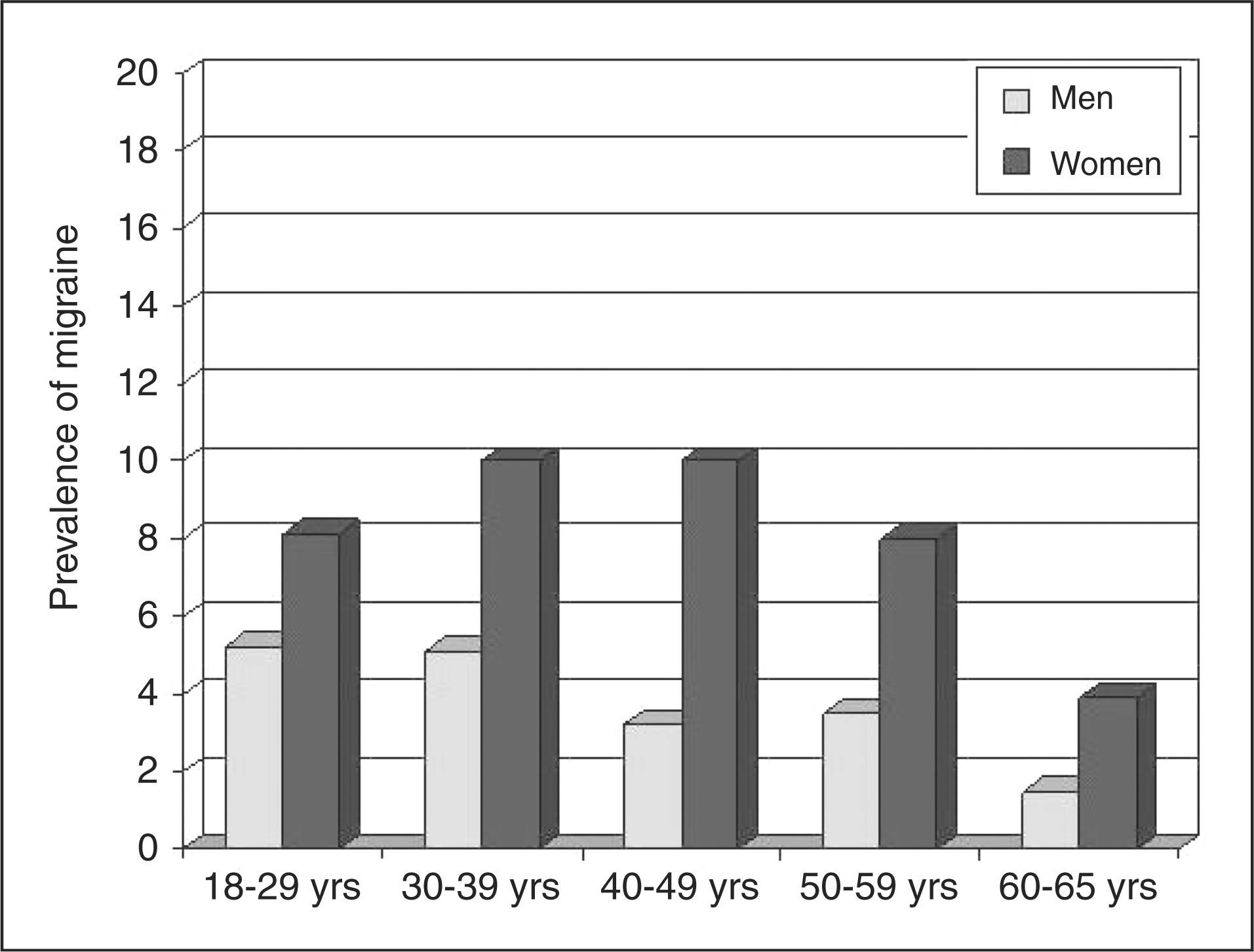


One-year prevalence rates of total migraine in the 17 autonomous communities

CI = confidence interval.
In the overall series of total migraine subjects (N = 712), migraine without aura occurred in 56% of cases (N = 399), migraine with aura in 23.3% (N = 166) and mixed type in 20.6% (N = 147). Subjects with strict migraine and those with probable migraine showed a similar percentage of migraine without aura (53% and 50%, respectively), although the percentage of migraine with aura was higher in the group of strict migraine (25% vs. 14%) and the percentage of mixed migraine higher among subjects with probable migraine (36% vs. 22%).
In subjects with probable migraine, duration of attack was the criterion most frequently not fulfilled (62.7%). In fact, 44.1% of subjects (N = 104) reported migraine lasting less than four hours and 18.6% (N = 44) had migraine lasting more than 72 hours. More than 75% of subjects with strict migraine and 60% with probable migraine reported duration of attacks between four and 72 hours (Figure 3). Finally, in one-third of individuals, the diagnosis of migraine was never made by a clinician.
Duration of attacks in subjects with strict migraine (N = 476) and probable migraine (N = 236).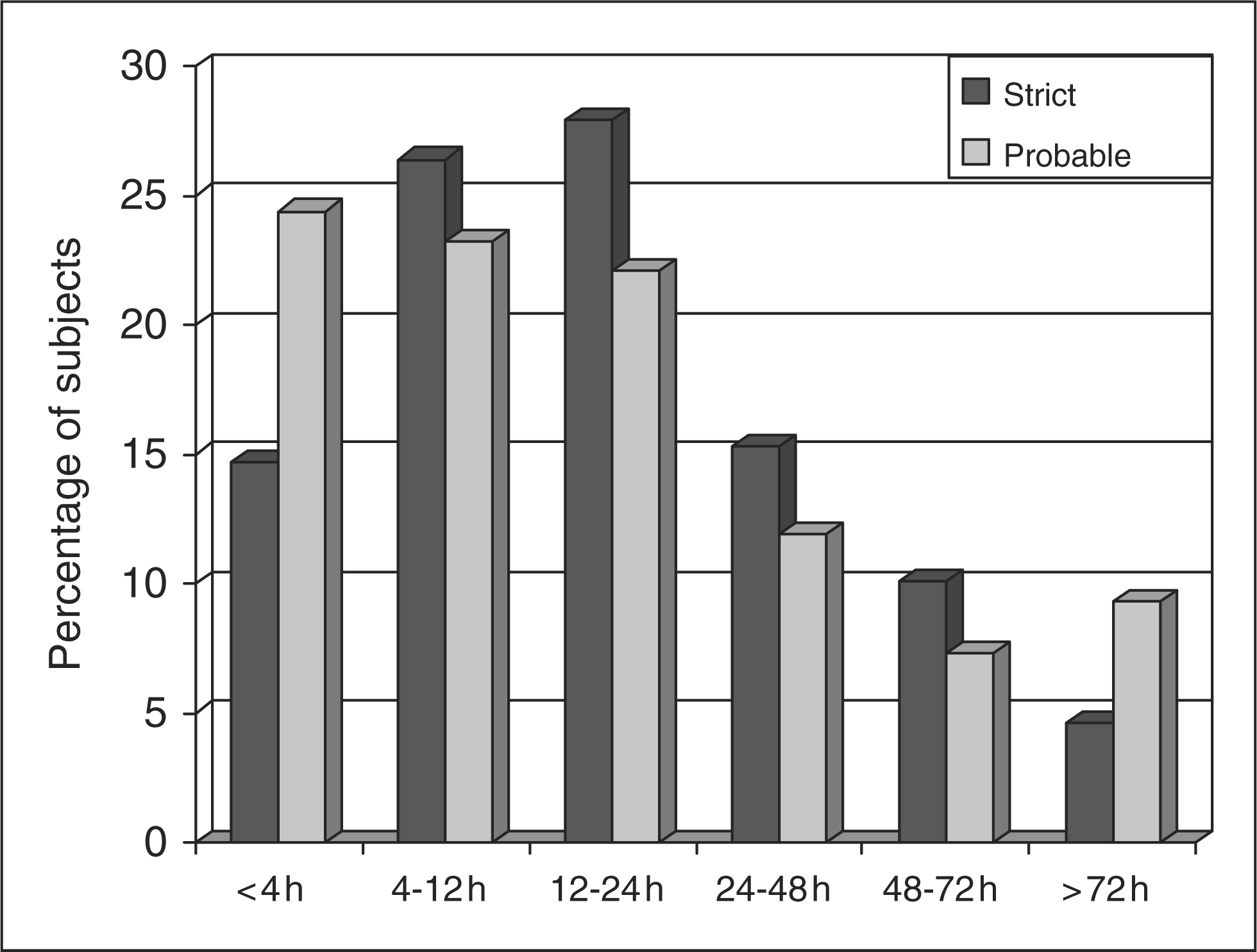
Discussion
The present study carried out in a representative sample of the Spanish adult population has shown that the one-year prevalence of total migraine was 12.6%. The prevalence rates of strict and probable migraine were 8.4% and 4.2%, respectively. The prevalence in women was 2.15 times higher than in men, and the highest figures were found in the 30−39-year stratum in both genders. If the subjects who withdrew from the study sample are considered as non-migraneurs, the one-year prevalence would be 11.9% (712/5987) instead of 12.6%.
The prevalence of total migraine found in the present study is consistent with data of previous studies carried out in our country in the 1990s, in which rates between 12% and 15% were reported (19−21). In a review of migraine and headache in Europe, summarizing the data on one-year prevalence, the proportion of adults in Europe reporting migraine was 14% (22). Other population-based studies have shown one-year prevalence of migraine of 13.2 ± 1.9% in Sweden (23), 10.6% in Germany (24), 10.2% in Austria (25), 7.9% in France (26) or a lifetime prevalence of 19% in Croatia (27). Using the IHS criteria, various large population-based prevalence studies have produced consistent estimates of one-year migraine prevalence ranging from 12% to 14% (7,28).
Prevalence rates of migraine showed geographic variations in the different autonomous communities, ranging from a lowest rate of 7.6% in Navarra (northern Spain) to the highest of 18% in the Canary Islands. Although it has been shown that there may be geographic variation within countries and continents based on either biological or environmental risk factors, these geographic differences in migraine prevalence require further study (29,30).
Most studies on migraine prevalence have reported variation by age, with prevalence figures following an inverted U-shaped distribution, increasing from age 15−18, peaking during the third and early fourth decades of life and declining thereafter (31,32). On average, migraine is 2.5 to 3 times more common in females than males. Prevalence remains elevated in females relative to males even at older ages (9). In our study, prevalence among women was 2.15 times higher than in men. In addition, in the stratum of 60–65 years of age, the prevalence in women was 3.9% as compared with 1.5% in men.
In our study, like others (27,33,34), migraine without aura was more common than migraine with aura. On the other hand, duration of migraine was the criterion most frequently missing for a case definition of strict migraine (categories 1.1 and 1.2). In a prevalence study of migraine in Taipei, Taiwan, migraine diagnoses were made according to the classification criteria of migraine without aura proposed by the IHS in 1988, except that attacks with a duration between two and four hours were also included (35). In a representative study of adults in the general Swedish population, in order to assess headache duration open-mindedly, the strict time criterion of 4−72 hours was deliberately disregarded as an inclusion criterion (36). In French nationwide survey carried out according to the 2004 IHS classification, probable migraine was also assessed, and in agreement with our data, the criterion most frequently missing was typical headache duration (4−72 hours) and most subjects with probable headache had shorter average headache duration (37).
The classification system proposed by the IHS has represented an enormous advance in headache classification. Epidemiological studies must be conducted in representative samples of some defined population. This is especially important for migraine, as individuals within the health care system (who seek medical care for headache) may be systematically different from those outside the health care system. High-quality studies also must use well-established, uniform methods for ascertaining the clinical features of migraine used for diagnosis. In the present study, a validated computed-assisted telephone survey was used (17). It has been previously shown that the CATI has a high sensitivity (85%) and specificity (96%) for diagnosing migraine with or without aura when compared with the standard of diagnosis through face-to-face history and physical examination conducted by a clinician applying IHS criteria (16). In our validation study, the CATI procedure using the migraine diagnostic questionnaire based on the IHS 2004 criteria had a sensitivity of 81.5% and a specificity of 91.3%. The validated CATI has been used in other studies in mainland Europe and in the United States (38−40).
The present results also provide evidence of the fact that many patients with migraine do not consult a physician for their headache. In one-third of the subjects, the diagnosis of migraine was never made. As reported from previous epidemiological studies, migraine is underdiagnosed and undertreated everywhere throughout the world, despite its considerable burden (41−43). Migraine patients are still not receiving adequate treatment and there remains a significant unmet need in migraine care, with the challenge being to diagnose migraine early and offer patients effective migraine-specific therapies.
The present results should be interpreted taking into account the limitations and strengths of the study. Patients contacted with headache/migraine may be more willing to participate than non-sufferers and this may be a source of bias that cannot be excluded. It may be argued that the non-participation rate was high (45.6% refused to take part in the study). However, in an epidemiological observational population-based cross-sectional study carried out by means of a telephone survey to assess the prevalence of pain in Spain, with a total of 5000 homes, the percentage of useful sample was 41.7% (44). Estimation of the one-year prevalence of migraine is more convenient than other epidemiological measures, as recall bias leads to major underestimation of the lifetime prevalence of this disease. One-year prevalence is also more relevant for costs analyses as well as the age range between 18 and 65 years. Other methodological strengths included quota sampling and random sampling, which ensured that the sample represented demographic characteristics in proportion to their prevalence in the population and that the probability of selection was the same for every case in the population. Moreover, the study participants were drawn from the general population rather than by region or specific group (e.g. students).
Although prior studies carried out in Spain (19–21) used somewhat different methodology and evaluated more specific populations, this study demonstrates that migraine prevalence in Spain seems stable and is not increasing. This finding is consistent with the epidemiological profile of migraine that has remained stable in the United States during the past 15 years (45). Finally, the apparently high prevalence of migraine with aura of 23.3% and mixed-type migraine group (20.6%) merits comment. This information on the frequency of migraine with aura has been included as a descriptive figure given that the questionnaire used in the present survey has been validated for total migraine and not strictly to differentiate between migraine with aura and migraine without aura. It has been suggested that more specific tools are needed for diagnosing migraine with aura in epidemiological settings (46). It has been shown that 48.6% of migraneurs without aura may experience some type of visual symptoms (47). In some studies, even higher rates have been described. For example, in a cross-sectional clinical study performed in two tertiary centers in Mexico City, migraine with aura was diagnosed in 53% of 1147 patients but the authors attributed this high percentage to a reference bias of the participating institutions (48). Despite these considerations, we also believe that the prevalence of 43.9% of migraine with aura and with sometimes having aura in our population may be high but it is mainly reported for informational purposes.
Conclusions
According to this population-based epidemiological study of migraine in Spain using validated CATI and the 2004 IHS operational diagnostic criteria, the one-year prevalence of migraine in our country is 12.6%, with a prevalence of migraine with and without aura of 8.4% and of probable migraine of 4.2%. These findings add data to the current understanding of migraine and highlight the need to perform nationwide population-based studies with validated methodology to elucidate differences and causes of such differences between various countries.
Scientific committee of the PALM program
Dr D. Adolfo Ramada Soriano, Dr D. Albert Jorge Jovell Fernández, Dr D. Enrique Arrieta; Antón, Dr D. Arturo Lopez-Gil, Dr D. Francisco Javier Sánchez Lores, Dr D. Jaume Morera Guitart, Dr D. Jesús Porta Etessam; Dr D. Julio Pascual Gómez, Prof. Jordi Matías-Guiú Guía (Chairman), Dr D. Samuel Díaz Insa, Dr D. Salvador Tranche Iparraguirre, Dr D. Valentín Mateos Marcos, Dr D. Vicente Baos Vicente.
Footnotes
Acknowledgements
We thank Marta Pulido, MD, for editing the manuscript and for editorial assistance.