
Abstract
Background: Transient, unilateral mydriasis has been reported in migraine patients, and this has been regarded as a possible co-morbidity between migraine and Adie’s tonic pupil. Mydriasis that outlasts the duration of migraine attacks is rare.
Methods: Through an eight-year period we have studied all patients referred to our neurological clinic because of migraine attack with mydriasis. All the patients underwent thorough neurologic and ophthalmologic examinations including MRI of the brain and testing of the pupil response to ocular instillation of dilute pilocarpine (0.125%).
Results: Seven women and two men, with a mean age of 33.8 ± 12.3 years (range: 19–52) were included. The patients presented during one hemicranial migraine attack with an ipsilateral mydriasis that persisted for a mean of three months, while migraine headaches remained with their typical episodic course. In all the patients a cholinergic supersensitivity in the symptomatic pupil was demonstrated, thus pointing to a dysfunction of the ipsilateral ganglionic parasympathetic fibers.
Conclusions: Synchronous co-localization of the features suggests a pathogenic link between the pupil dysfunction and migraine, rather than a simultaneous coexistence of two independent disorders. Likely explanations include a latent Adie’s pupil that could have been triggered during a particular migraine attack; a ciliar ganglionic lesion/dysfunction produced by the migrainous process; an ophthalmoplegic migraine with selective parasympathycoparesis; or an episodic ciliar ganglionitis with migrainous features. Ciliary ganglioplegic migraine is proposed as a nominal term pointing to the possible anatomic source of the migrainous-related pupil dysfunction; the pathogenesis remains unknown.
Introduction
Migraine attacks are frequently accompanied by signs and symptoms arising from the visual system, including visual field abnormalities with hemianoptic or monocular distribution, scintillations, scotomas and pupillary disturbances (1). Migraine-related visual dysfunction, either central or peripheral, is typically brief. When persistent, this is indicative of a migraine variant (e.g. prolonged aura); a complication of migraine (e.g. occipital migrainous infarction); or may even point to a co-morbid disorder.
Blurred vision during migraine may be due to mydriasis and/or impaired accommodation, thus indicating a peripheral dysfunction involving ciliary ganglionic cells or postganglionic nerves (1–3). Transient, unilateral mydriasis has been previously reported in patients with a medical history of migraine (2,3), and this has been regarded as an Adie’s-like tonic pupil apparently caused by migraine (4,5). Mydriasis outlasting the duration of migraine attacks is rare, but has also been reported in a few patients (6–8).
Ophthalmoplegic migraine (1) is characterized by recurrent attacks of migrainous headache accompanied by paresis of one or more of the ocular cranial nerves (most commonly the third cranial nerve). Admittedly, because the third cranial nerve also carries parasympathetic fibers to supply the sphincter pupillae and ciliary muscle, a prolonged mydriasis within a migrainous attack might be regarded as a parasympathetic variant of ophthalmoplegic migraine (1).
We herein describe nine patients suffering from regular migraine without aura who during one typical hemicranial migraine attack developed an ipsilateral mydriasis that by far outlasted the end of the migraine episode, and attained a rather persistent course, thus running independently of subsequent migraine attacks. The features were consistent with a ciliary ganglionic dysfunction that could be triggered by the migrainous process, thus constituting a “ciliary ganglioplegic migraine”.
Materials and methods
Demographic and clinical characteristics of patients with ciliary ganglioplegic migraine
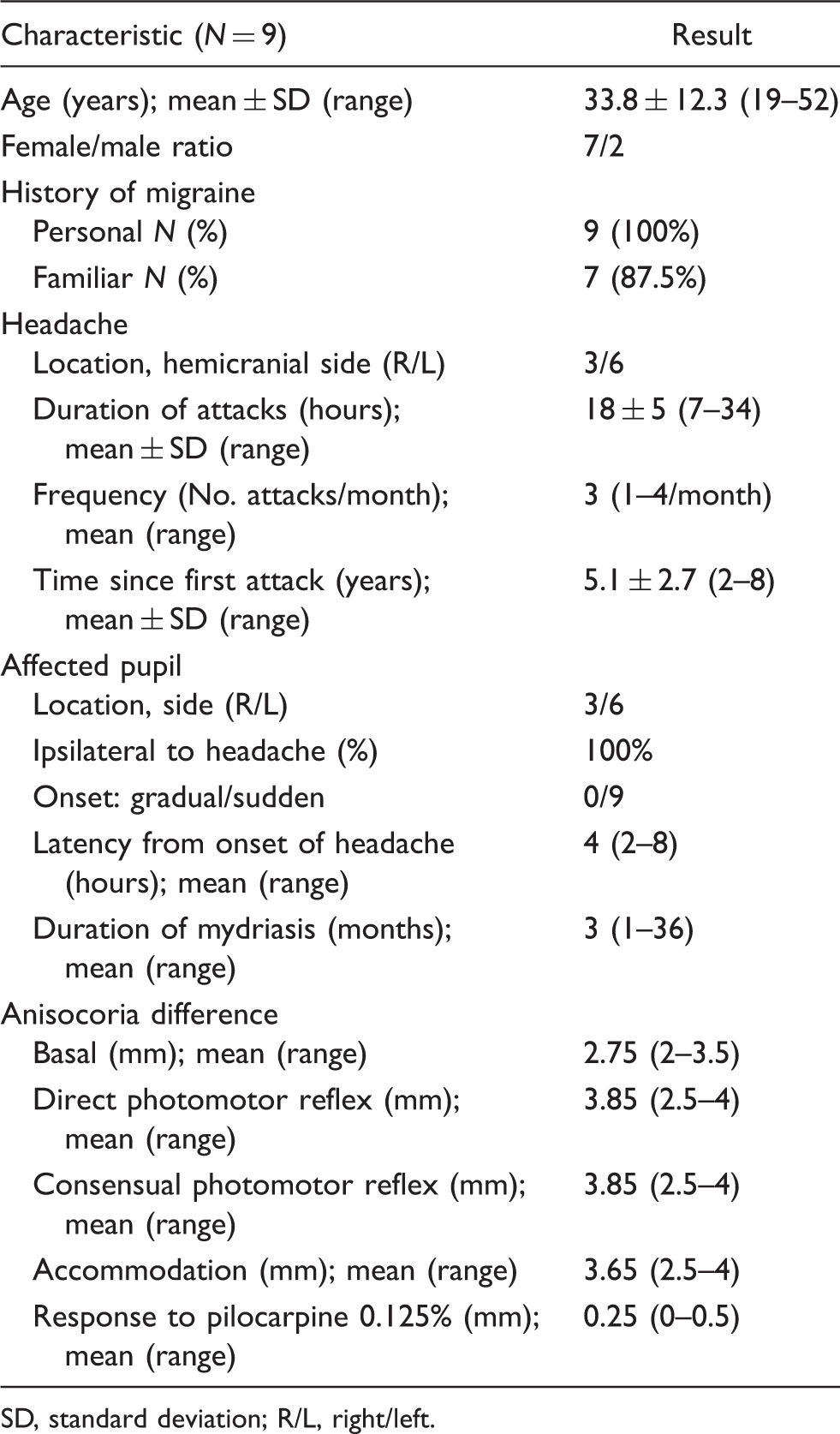
SD, standard deviation; R/L, right/left.
The patients were studied in the neurological department, and in addition ophthalmologic examinations were carried out on all the patients. Analysis with routine bloodwork was done, including cell count, erythrocyte sedimentation rate, thyroid function, antinuclear antibodies and rheumatoid factor. Electroneuronography (median, ulnar, tibial and sural nerve conduction studies) and imaging studies (orbit and brain MRI with 3-mm thickness axial sections and gadolinium administration) were performed in all the patients.
Pupil size was assessed clinically and exactly measured by precision photography. High-quality pictures centered in both eyes were taken under the same conditions of light, magnification and exposure parameters using a high-resolution camera (Zeiss FF 450 IR plus Fundus camera 786 × 576 pixels resolution) and a digital image archiving system (Visupac 451 Digital 3.2.1 version). Patients were examined and photographed in the basal state. The pupil response was analyzed and measured during direct photomotor reflex, consensual light reflex, accommodation and after ocular instillation of dilute pilocarpine (0.125%).
None of the patients were under preventive medication. Four patients had taken abortive drugs (triptan) before the mydriasis ensued.
Descriptive statistics were carried out with the SPSS statistical package (13.0 version) (SPSS, Chicago, IL, USA).
Resutlts
A total of nine patients (seven women and two men), with a mean age of 33.8 ± 12.3 years (range: 19–52) were studied. All had a personal history of migraine, ranging from two to eight years (mean: 5.1 ± 2.7). Most patients (87.5%) had family history of migraine. None of the nine patients had other remarkable antecedents. All the patients had strictly unilateral attacks: six patients had their attacks on the left hemicranial side, and three patients on the right. The mean duration of a migraine attack was 18 ± 5 hours (range: 7–34). The onset of mydriasis was always sudden and ipsilateral to the pain side. The headaches preceded the mydriasis by two to eight hours (mean time: four hours). The pupillary dysfunction persisted for 1 to 36 months following the cessation of headache, even becoming permanent in two patients. The follow-up period ranged from 3 to 11 years.
Except for anisocoria, all patients had normal neurologic and ophthalmologic exams. The mean basal anisocoria difference (symptomatic – non-symptomatic diameter) was 2.75 mm (range: 2–3.5 mm). There was no ocular muscle palsy or lid involvement. In all patients, the dilated pupil evidenced an absent or delayed response to light (both direct and consensual photomotor reflexes) with a mean increase of the anisocoria difference of 3.85 mm (range: 2.5–4 mm). A slow and prolonged reaction to convergence with a mean increase in anisocoria difference, averaging 3.65 mm (range: 2.5–4 mm), was documented. The symptomatic pupils responded to administration of pilocarpine 0.125%, thus indicating a supersensitivity to pilocarpine, pointing to a dysfunction of the ipsilateral ciliar ganglionic cells or postganglionic parasympathetic fibers.
Routine bloodwork, electroneuronography and brain MRI studies rendered normal results in all the patients.
Discussion
Our observations deal with a series of migrainous patients who during one regular hemicranial migraine attack had an associated ipsilateral mydriasis which by far outlasted the duration of the migraine attack. Clinical and pupillometric features were consistent with a denervation of the postganglionic supply to the sphincter pupillae and ciliary muscle
Pupillometric findings are consistent with an Adie’s pupil (9,10), but migraine and Adie’s pupil are acknowledged as two independent disorders. Although the possibility exists that the two disorders coexisted by sheer chance in the same individuals, the concurrence at random in the same side and during the same period of time seems highly unlikely. Adie’s tonic pupil may present in bouts, and admittedly, the stress linked to a migraine attack could have unveiled a latent Adie’s pupil. However, the bond between Adie’s tonic pupil and migraine is far from being demonstrated, and other explanations of the association of ciliary ganglioplegia and migraine are pertinent.
A migrainous process reaching the ipsilateral ciliary ganglion could produce a lesion/dysfunction of the ganglionic cells, giving rise to a rather persistent pupilloparesis. Likely, both pupillary dysfunction and migraine could depend on the same pathogenic process with the recovery of the respective signs and symptoms being asynchronous, either component following their natural course (phasic in migraine and tonic in ciliary ganglioplegia).
As miosis seems to be, as stated in previous papers (11–13), the most frequent pupillary phenomenon associated with migraine, the series we describe represents a somewhat paradoxical or at least a sufficiently “off road” variant within migrainous nosology for it to be considered in a separate category. A migraine-related mydriasis could be taken as a migraine variant. Indeed, a prolonged mydriasis is at variance with the expected duration of the features of a typical migraine attack. Therefore, such an event would better be considered as part of a complicated migraine episode (1).
Theoretically, a process such as ophthalmoplegic migraine (14–18) with a selective lesion of the parasympathetic fibers of the oculomotor nerve could bring about a picture of migraine-like headache and ipsilateral mydriasis
The ciliary ganglion receives its sensory innervation from the nasociliary branch of the ophthalmic division (V-1) of the trigeminal nerve in its way to supply the cornea. Theoretically, a pain originated in the ciliary ganglion would be projected to the V1 territory, giving rise to a unilateral headache. Otherwise, activation of these V1 afferents may trigger the trigeminovascular system, thus instigating a headache with migrainous features. Accordingly, a ciliary ganglionitis might present with unilateral headache and ipsilateral pupillary dysfunction. The association of migraine and autonomic ganglionitis and peripheral nerve neuritis has already been reported (24). We cannot dismiss the possibility that in addition to regular migraine attacks our patients had an episode of ciliary ganglionitis with secondary migrainous-like headache.
Examination of one patient with ganglioplegic migraine: (A) Left-sided mydriasis. Basal conditions. (B) Direct photomotor reflex: poor response to light of the left pupil. (C) Consensual photomotor reflex: poor response of the left pupil. (D) Convergence response: slow constriction of the left pupil. (E) Hypersensitivity to 0.125% pilocarpine. Constriction of the left pupil without response of the right pupil.
Given all the possible mechanisms raised, we propose the term ciliary ganglioplegic migraine as a preliminary, nominal concept, aimed at highlighting the association of persistent mydriasis developed during a migraine attack. So far the concept does not carry strict nosologic implications, but helps in localizing the origin of the apparently migraine-related mydriasis. Ciliary ganglioplegic migraine can be taken as a topographic syndrome. It seems to be a benign condition, yet requires exclusion of symptomatic headaches by appropriate investigations.
Conclusions
Ciliary ganglioplegic migraine describes the spatial and temporal concurrence of unilateral migraine and persistent ipsilateral mydriasis, suggesting a pathogenic link between both components, and marking the ciliary ganglion as the probable source of the migraine-related pupil dysfunction.
Ciliary ganglioplegic migraine could represent a complicated migraine; a new migraine category; an ophthalmoplegic migraine with selective parasympathycoparesis; an episodic ciliary ganglionitis with migrainous features; or an association of Adie’s pupil and migraine. Only by unraveling the pathogenesis can we obtain a better insight into establishing an accurate nomenclature.