
Abstract
The aim was to characterize the individual and socio-economic impact of headache in a patient population from The Danish Headache Centre. This was a cross-sectional study using a structured interview, prospective headache diaries and standardized self-administered questionnaires using the ICHD-II criteria. Fifty-five subjects (12 male and 43 female) with a median age of 41 years and a median headache frequency of 15 days/month participated. Very high utilization of the healthcare system and a high absence rate due to headache of 12 days/ year were reported. Eighty-one percent experienced a marked decrease in work effectiveness. Overall, 91% felt hampered by their headache on a daily basis and 98% had had expenses for headache medication. Frequent headache disorders are highly costly, especially due to indirect costs. Prevention, early intervention or effective treatment strategies for headache disorders may therefore be highly cost effective, not only for the individual but also for society.
Introduction
Few studies have characterized the patient population in specialized headache centres and only limited knowledge about the socio-economic impact for these patients is available (1, 2). Prior studies have mainly reported clinical characteristics such as headache diagnoses, frequency, sex and age distribution and duration of headache, whereas medical treatment and lost workdays have only rarely been studied in headache centres (2–4).
Headache is the most prevalent pain disorder. Most European and American studies report the 1-year prevalence period of migraine in adults as 10–12% and lifetime prevalence as 13–18% (5, 6). Tension-type headache (TTH) is the most prevalent primary headache disorder (7) and in a Danish study the life-time prevalence was as high as 78%, although the vast majority (59%) had infrequent TTH (≤1 day/month) and, because they had no specific need of medical attention, they could not be regarded as headache patients. Nevertheless, 24–37% had TTH several times per month, 10% had it weekly and 2–3% of the population had chronic TTH (≥15 days/month) usually lasting for the greater part of their lifetime (5, 8).
The prevalence of both migraine and TTH steadily increases from infancy to the fourth decade and, later on, decreases with increasing age; thus, headache is a highly prevalent chronic disease that normally affects people during their most productive years (5, 6, 9), and the socio-economic impact is considerable. Thus, migraine is listed by the World Health Organization as 19th of all diseases with regard to years lived with disability and headache accounts for approximately 20% of lost workdays (5, 10). In Denmark, the total cost of all headache disorders is estimated to be approximately 3 billion Danish kr, corresponding to approximately €74 million per million inhabitants per year (5). In the USA, migraineurs cost American employers about $US13 billion per year because of missed workdays and impaired work function and annual direct medical costs for migraine care are about US$1 billion (11).
Severely affected headache patients are expected to experience a higher impact on quality of life, have more absence from work, have a higher frequency of medical services use and have higher costs of medication compared with the general population, but the specific relation has never been studied in detail (1, 2, 12). Treating these patients and thereby reducing the frequency and intensity of headache is very important for the individual patient as well as for society as a whole.
The aim of this study was therefore to characterize the patient population in a specialized headache centre and to describe their general sickness absence from work and, more specifically, their headache-related sickness absence, effect on work performance, utilization of medical services, alternative treatment, costs of medicine and overall impact of headache.
Materials and methods
All the participants were out-patients referred to a tertiary referral headache clinic, The Danish Headache Centre (DHC), during a 1-month period either for their first or second visit. In the waiting room all newly referred patients were asked consecutively to participate in a structured interview, with emphasis on the socio-economic impact of their headache.
The interview contained a total of 116 questions about the socio-economic impact of headache disorders derived from a recent general population study (13). The interview included an extensive description of the influence on working ability, personal impact, utilization of health services and medicine, and was conducted by a trained medical student (R.T.N.) blinded to the remaining information about headache diagnosis, frequency and medication use.
The DHC is part of the Department of Neurology, Copenhagen University Hospital, Glostrup operating since 2001, with the main uptake area being Copenhagen County (600 000 inhabitants), besides functioning as the only national referral centre for severely affected headache patients in Denmark (5.5 million inhabitants). The annual intake is about 1000 new patients (3). The patients are referred to the Headache Centre by general practitioners, practising neurologists and other neurological departments (3).
The initial headache diagnosis was based on the information from a standardized case record, a prospectively recorded diagnostic headache diary (14) and a standardized questionnaire (3) recorded by the patient before first visit using the diagnostic criteria of the International Headache Society (ICHD-II) (15). Furthermore, data on the frequency, intensity and duration of headache and any medical prophylactic treatment were obtained independently of the structured interview from the three items (case record, diary and questionnaire).
We used the diagnosis probable medication-overuse headache (PMOH), as we were interested in the initial headache diagnosis. When a patient was given the diagnosis PMOH, this diagnosis overruled the primary headache diagnosis (3). All remaining types of headache were placed in the category ‘other headaches’ (3).
Absence rates were analysed among gainfully employed workers, i.e. subjects with paid work, apprenticeship or attending secondary education in the preceding year, both for full-time and part-time workers.
Data analysis
All data were recorded in an Access database by the main author (G.R.V.) and descriptive analysis was performed with SPSS version 12.0 (SPSS Inc., Chicago, IL, USA). Comparison of groups was performed with the Mann–Whitney test. Median values are presented unless otherwise specified.
Results
Fifty-six patients were asked to participate and none refused. Of the 56 initial patients, one was later excluded due to loss of the case report, leaving 55 patients. The median age was 41 years (20–78), with a male:female ratio of 1 : 3.6.
Clinical description
Table 1 presents headache diagnoses and clinical characterization of the 55 patients. Fifteen patients had PMOH, 11 had pure migraine, four had pure TTH, 17 had both migraine and TTH and eight had other headaches (of which two were cluster headache). There were 19 patients with only one diagnosis, 26 with two diagnoses, nine with three diagnoses and one with four IHCD-II diagnoses.
Clinical characterization

The groups are mutually exclusive. Median values with range are presented.
Missing values.
PMOH, Probable medication-overuse headache; TTH, tension-type headache.
On average, median headache frequency in the 30-day period prior to the interview was 15 days/month (0–30) and the headache intensity was 2 (on a 0–3 scale). The headache frequency of PMOH patients was significantly higher (24 days/month) than of the remaining group of patients (7.5 days/month) (P = 0.002). For patients without PMOH the duration of the headache was 10.5 years (0.1–67). The beginning of the PMOH could not be precisely determined.
At the initial visit, six of 55 patients (11%) were on prophylactic antimigraine treatment and four patients (7%) had previously tried prophylactic treatment before referral to the DHC.
Utilization of healthcare
Overall, 98% of all the patients had, at some time and because of headache, consulted their general practitioner (GP) (Table 2) and within the previous year 96% had consulted their GP because of headache. In the last year, due to their headache, 100% had used specialist care, with a median of 3.0 times (range 1–21) and 28% had used off-hour service with a median of 1.5 times (range 1–10). Thirty-six percent had at some time consulted a naturopath and, of these, 10 reported having spent between 500 and 20.000 Danish kr (€66.7–2666.7) on this treatment within the last year.
Participants who reported having consulted their general practitioner, other specialists, etc., due to their headache, ever and last year

Other specialist consists of: specialist care (out-patient and private specialty clinic care), and off-hour service (general practitioners on off-hour duty or emergency department).
Missing values.
Work absence and work effectiveness
Figure 1(a,b) presents work absence. In the previous year, patients had had a median of 12 days off work because of headache (range 0–365, mean 57 days) and a median of 20 days off totally because of all causes (range 0–365, mean 67 days). The absence rate is highly skewed as 19% (nine patients) had >60 days absent from work due to headache and of those 10% (n = 5) had been absent a full year. Due to headache, 90% (43/48) had been absent from work at least once and due to all causes 96% (47/49) had had at least one absent day during the last year. No significant difference in absence rates between PMOH and non-MOH patients could be detected (headache-related absence 19 vs. 11 days/year, P = 0.7; total absence 22 vs. 20 days/year, P = 0.9).

Work absence among the gainfully employed. (a) All-cause absence rates from work within the last year (one missing value). (b) Headache-related absence rates from work within the last year (one missing value).
Figure 2 shows work effectiveness. It illustrates that 81% (35/43) of the patients who did go to work with a headache had >20% decreased work effectiveness. The figure is bell-shaped, with the maximum of 40–60% reduction in work effectiveness.

Work effectiveness—working with headache.
Individual impact
Table 3 presents the individual impact of headache on the patient population. On a daily basis, 91% (50/55) stated that they felt hampered by their headache.
General impact on working capacity and other activities—how does the headache impair or abolish housework capacity or other activities?

During the last decade 27% had changed their diet, 56% their sleeping pattern, 53% their use of alcohol, 46% their exercise habits, 29% their place of work and 18% their family pattern because of their headache. Furthermore, 64% had ruled out social/spare-time occupation, 46% had ruled out particular jobs, 40% had had restrictions in their career because of headache, 58% stated that they were dependent on help from their family/friends and 9% had chosen not to have any more children.
Medication expenses
In the preceding year all but one of the patients had had personal expenses for medication for their headache. Two patients (4%) had spent >€1333.5 within the last year (Fig. 3).
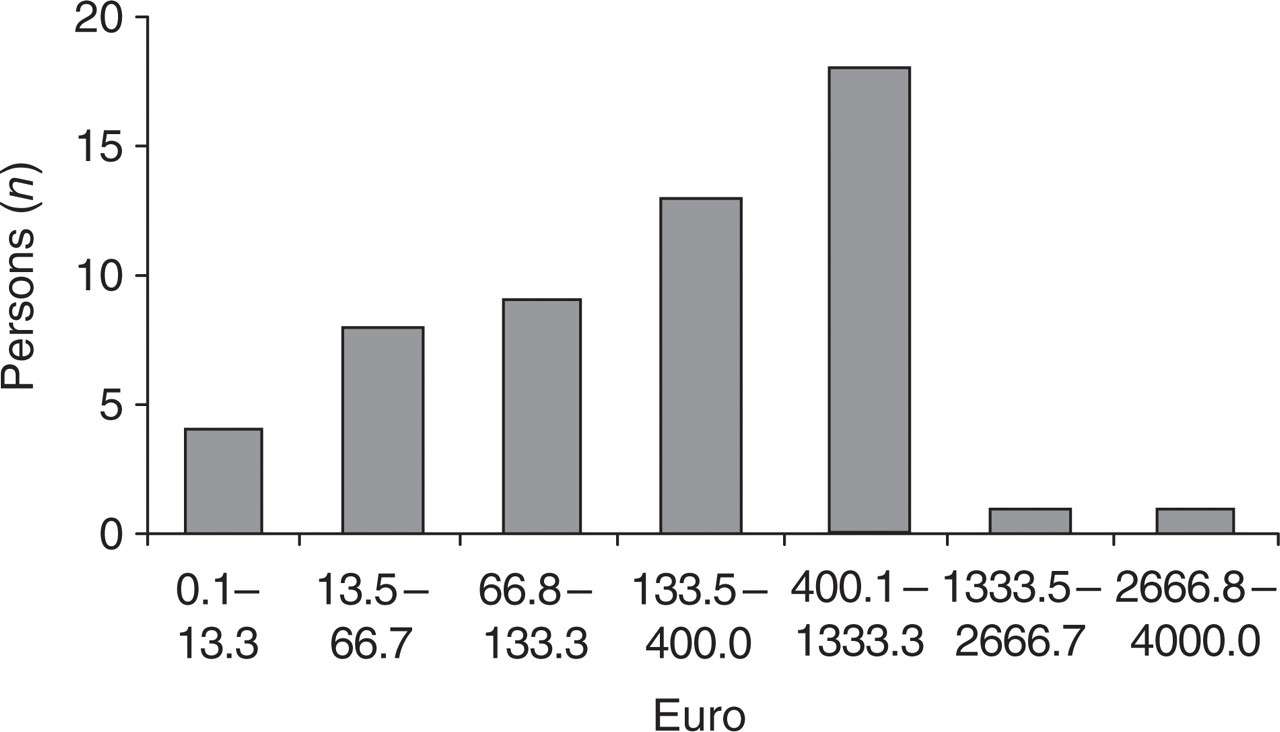
Personal medication expenses for headache in the preceding year.
Discussion
Knowledge about the impact of headache is important, both from an individual point of view and for society. The effects on individuals can be assessed by examining headache prevalence, distribution, attack frequency and duration and headache-related disability. The socio-economic burden includes both direct costs associated with healthcare utilization and indirect costs associated with missed work due to sickness absence or reduced effectiveness (16). A recent report from a specialized headache centre has demonstrated a significant treatment effect in a multidisciplinary headache centre (3), but the socio-economic impact was not estimated.
The present study characterizes a patient population at the DHC. On the individual level we found a median headache frequency of 15 days/month, moderate headache intensity and a headache duration of 10.5 years. Although a considerable impact was expected, it is noteworthy that as many as 91% of patients felt hampered by their headache on a daily basis. Regarding socio-economic impact, we found, as expected, very high utilization of the healthcare system and a high frequency of absence from work due to both headache and all causes. We also found a marked decrease in work effectiveness for 81% of the patients and almost all subjects had had expenses for headache medication, despite Denmark's very favourable healthcare system with partial reimbursement of costs of medication.
Relation to the general population
In 2001 a cross-sectional population-based headache study was conducted including the same questionnaire as in our study (13) and data can therefore indirectly be compared. Regarding healthcare utilization, a fairly high proportion (31%) of the general population had at some time consulted their GP because of headache, corresponding to our 98%. Moreover, only 3% had ever, and 0.3% within the last year, been hospitalized because of headache, compared with our proportion of 20% and 6%, respectively, probably illustrating a higher degree of complexity and intensity in our headache patients. Altogether, of the general population, 32% had at some time consulted a medical doctor because of headache, 10% within the last year, corresponding to our 100%. Likewise, no more than 3% of the general population had had specialist care and 2% off-hour service for headache within the last year, while the corresponding numbers in our patients were 100% and 28%, respectively. These data underline the importance of increased focus on headache disorders in both the general population and in selected patient groups (13).
Of the total general population, treatment of headache by physiotherapy had been received by 9%, chiropractor 5%, dental evaluation 0.5%, zone therapy 5%, acupuncture 5% and naturopaths 5%, also considerably lower than the corresponding numbers (24–56%) in our study (Table 2) (13).
In our patient population 90% of the gainfully employed subjects had been absent from work at least once during the last 12 months due to headache, whereas the corresponding percentage in the general population was 12%. Likewise, 96% of our patients had had at least one absence day from any cause within the last year compared with 54% from the general population (13). Lyngberg found a median of 0 days absent from work due to headache and 3 days absent from work due to all causes. The data were highly skewed, with a small proportion having a high number of absence days, while the majority of the population had no absence or a low number of absence days.
As expected, we found a much higher utilization of the healthcare system and a higher absence rate in our population, illustrating the very high impact of severely affected headache patients. Furthermore, the present data underline the need and the social gain that can be expected from effective treatment and rehabilitation of these severely affected individuals.
Clinical description
The overall sex and age distribution in the present study are in line with other studies of specialized headache centres in Scandinavia and America (1, 2, 17, 18). In three studies from the USA the mean age was found to be 37–44 years compared with our 41 years. There was also a pronounced female preponderance of 73–79% compared with our 78%.
A previous large clinical study from our group, which characterized all patients in the DHC discharged in 2002, had a slightly greater mean age at 46 years and a lower male:female ratio (1 : 2.4 vs. 1 : 3.6), a longer life-time duration of headache (16 years vs. 10.5 years) and a higher headache frequency (mean 21 days/month vs. median 15 days/month), but a similar headache intensity (3). The minor differences may be explained by the fact that the DHC opened in 2001 and the most severely affected patients were probably the first to be referred to the centre.
Our median headache frequency of 15 days/month is slightly lower than that reported by Saper et al. (2) with a mean of 5.3 days/week at referral. Saper made a comprehensive analysis (using in- and out-patients) of patients attending an American multidisciplinary headache centre for chronic, refractory headache. The sample consisted of intractable headache sufferers who had failed to benefit from prior primary, secondary or tertiary care, and they thereby describe a more severely affected patient population. Except for the prior study from our group (3) there are no comparable European studies.
Utilization of healthcare
To our knowledge, the utilization of healthcare has not been analysed in detail in other specialized headache centres. Mendizabal (1) has described a comparison of new patients visiting two headache clinics in the USA. In both clinics only 79% had previously seen a physician because of headache, in comparison with all of our patients.
The differences could easily be explained by different healthcare systems. The Danish healthcare system provides universal health insurance coverage for all citizens. The benefits are comprehensive, including primary care, off-hour services, ambulatory specialty care, hospital care, home visiting services and partial coverage for prescription drugs, physiotherapy and dental care (13, 19). In addition, a managed care system is used in Denmark, as patients have to be referred to specialists by a primary care physician, in contrast to a self-referral system in most other countries (1).
Furthermore, Saper et al. (2) found that 38% of their severely affected sample had received emergency medical care a mean of 4.39 times during the last 6 months, compared with 28% of our population who had used the off-hour services a median of 1.5 times during the last year and all the patients who had had specialist care a median of 3.0 times. This difference could perhaps be explained by the fact that the Danish welfare system makes it possible to visit a GP very easily during daytime and therefore ER and other off-hour services are used less frequently.
Work absence and working effectiveness
Our results, with a median of 12 missed workdays in the previous year due to headache, is also in accordance with those of Saper et al. (2), who reported a mean of 2.74 days off work in the past 3 months, leaving a total of 11 days/year, although it is not specified whether the absences were due to headache or other causes. Our present finding of 20 days/year off work due to all causes, including headache, is very high and of significance for society. Similar clinical data have not been previously reported.
Zeeberg et al. (3) found an even higher number of missed work days, namely a mean of 8.6 days/month due to headache for all their patients, comprising a total of 103 days/year. The variations may be due to a highly skewed distribution between the patients and to the above-mentioned variations in patient characteristics. The present study comprised a relatively small total number of patients and direct comparison with a large headache population is therefore complicated.
Mendizabal et al. (1), visiting the two headache clinics in the USA, found, respectively, 90% and 88% of the clinical patient population had had incapacitating headache days, although there was no information about the precise number of missed work days.
Von Korff et al. (20), in their representative population-based sample, found that migraineurs reported an average of 41% reduction in work effectiveness during migraine based on daily headache records, in line with our report of a 40–60% reduction in work performance during headache.
Individual impact
To our knowledge, there have been only very few studies of individual impact of headache on patients from a tertiary centre. On a daily basis, 50 out of our 55 patients (91%) stated that they had functional impairment because of their headache. Saper et al. reported that their patients were unable to carry out responsibilities in any setting 1.72 days per week (2). Bussone et al. (12) reported impaired SF-36 (a general quality of life measure) in migraine without aura, chronic migraine and cluster headache compared with the general Italian population for patients attending a tertiary care centre. By means of MIDAS (a specific headache disability measure) within the last 3 months, patients with migraine without aura had more evident disability in personal/family/social activities than in work activities. For 150 chronic migraine patients (all being medication overuse patients) all activities (paid work, household work and social/leisure/family activities) were impaired by the headache and non-work were more impaired than work activities (12). This is almost in concordance with our data, as we found that during headache only 4–9% of our patients had normal activity in housework/social/family life.
Several studies of the general population are available, especially regarding migraine. Lipton et al. (21) have described the burden of migraine on the general population in the USA and reported 91% of migraineurs as having functional impairment due to their headaches, and during severe headache 53% reporting severe impairment in activities or requiring bed rest, quite similar to our results. Lipton also found a household work productivity reduction of at least 50% for 67% of migraineurs in the previous 3 months (21).
Medication expenses
An explanation of why only two patients had spent more than €1333.5 on medication during the last year could be found in the Danish healthcare system. The system is totally free of cost for patients with regard to primary and most secondary healthcare. Most prescription medication is partially reimbursed up to a limit of approximately 20.000 Danish kr (€2667) and thereafter totally reimbursed (22). We therefore expect no economic restrictions in the recorded use of medical services and therefore the results may be representative of the general use of healthcare services. Nevertheless, society in general may have a very specific and general interest in the total costs of headache medication, especially due to the very high cost of triptans (23) and the frequency of MOH (3, 24).
Methodological considerations
This study has certain limitations. The total number of patients is relatively small and results could be skewed by a highly selected patient population. Direct comparisons with other patient populations, especially in pain clinics, may therefore be valuable.
With respect to headache diagnosis and frequency, the present data are considered reliable, as prospective recordings in diaries and structured interviews were used. Nevertheless, due to practicality, the patients' self-report and memories of headache-related activity and its associated consequences were recorded in interview rather than daily headache records. Other advantages are the detailed questions in the interview, which are similar to those used in a recent general population study (13). The data can therefore be compared indirectly, although direct comparison with the same interviewer would have been the optimal method. The daily diagnostic headache diaries, classification of all patients in accordance with ICHD-II and lack of social bias due to free treatment for all patients are also important advantages.
Conclusion
Severe and frequent headache is costly, in terms of both direct and indirect expenses. It is particularly in healthcare services, sick-leave and effectiveness in the work place where the high socioeconomic impact is felt. Prevention, early intervention or effective treatment strategies for headache disorders may therefore be highly cost effective not only for the individual but also for society. The present study from a specialized headache centre has demonstrated an urgent need for effective treatment and such strategies will, due to the high indirect expenses, probably be highly cost effective.
Conflict of interest
None declared.