
Abstract
Objective: The objective was to study the prevalence of cervicogenic headache (CEH) in the general population.
Methods: An age- and gender-stratified random sample of 30,000 persons aged 30–44 years received a mailed questionnaire. Those with self-reported chronic headache were interviewed by neurological residents. The criteria of the Cervicogenic Headache International Study Group and the International Classification of Headache Disorders, second edition, were applied.
Results: The questionnaire response rate was 71% and the participation rate of the interview was 74%. The prevalence of CEH was 0.17% in the general population, with a female preponderance. Fifty per cent had co-occurrence of medication overuse and 42% had co-occurrence of migraine. The pericranial muscle tenderness score was significantly higher on the pain than non-pain side (p < .005). The cervical range of motion was significantly reduced compared to healthy controls (p < .005). The mean duration of CEH was eight years. Based on patients' self-reports, greater occipital nerve (GON) blockage and cryotherapy was reported effective in 90% of those who had this procedure, while other treatment alternatives were reported less effective.
Introduction
Cervicogenic headache (CEH) is a symptomatic headache characterized by chronic unilateral headache and symptoms and signs of neck involvement (1–3). CEH is often worsened by neck movement, sustained awkward head position or external pressure over the upper cervical or occipital region on the symptomatic side (1,3). Abolition of the headache following diagnostic anesthetic blocks of cervical structures or its nerve may provide evidence that the pain is attributed to a neck disorder or lesion (1,3,4).
The prevalence of CEH varies considerably, depending on the applied diagnostic criteria. A Portuguese epidemiological survey of the general population found a prevalence of 1% in headache patients applying six positive criteria of the Cervicogenic Headache International Study Group (CHISG). The prevalence increased to 4.6% when only five criteria were used (5). A Norwegian population-based survey found a prevalence of CEH of 4.1% using the criteria of the CHISG (6–8). The prevalence of CEH was 2.5% in the Danish general population when applying criteria of the International Headache Society, and the prevalence increased in persons with frequent headache (9). CEH was not associated with migraine in a clinic population (9). Among patients from headache centers the prevalence data variy widely, from 0.4% to 80% (10–12). The prevalence differences are probably due to different study designs and populations. The challenge with identifying and classifying CEH is also reflected in the different classifications (1–3). Co-occurrence of migraine and/or tension-type headache further complicates the diagnostics of CEH (13,14). The pathophysiology of the cervical spine is complex, since both dysfunction of the neck muscles and mechanical cervical spine pathology can produce painful and limited cervical movements—that is, CEH (15–17).
The aim of this paper is to provide epidemiological and clinical data on CEH in persons from the general population.
Materials and methods
Sampling
An age- and gender-stratified random sample of 30,000 persons aged 30–44 years and residing in eastern Akershus County was drawn from the Norwegian Population Registry in January 2005. Akershus County has both rural and urban areas and is situated in close proximity to Oslo, Norway. The age range of 30–44 years was chosen because the headache prevalence is relatively higher than in younger age ranges, whereas in the targeted age range co-morbidity of other diseases is lower than in older age ranges. The sample size was reduced to 28,871 because of error in the address list (N = 1,065), emigration (N = 32), multihandicap (N = 28), insufficient Norwegian language skills (N = 2) and decease (N = 2). Data from Statistics Norway show that the sampling area was representative for the total Norwegian population regarding age, gender and marital status. Regarding employment, trade, hotel/restaurant and transport were overrepresented, while industry, oil and gas and financial services were underrepresented in the sampling area compared to the total Norwegian population. Figure 1 shows a flowchart of the study.
Flowchart of the epidemiological survey.
Questionnaire
All persons received a mailed questionnaire with a standard letter containing information about the project. Apart from ensuring confidentiality and emphasizing the importance of participation, it was stated that the object was to study headache. The questions “How many days during the last month have you had headache?” and “How many days during the last year have you had headache?” were used to screen for chronic headache. If the questionnaire evoked no response, a second and subsequently a third mailing was issued. The overall response rate of the questionnaire was 71% (20,598/28,871).
Clinical interview, physical and neurological examination
Diagnostic criteria of cervicogenic headache
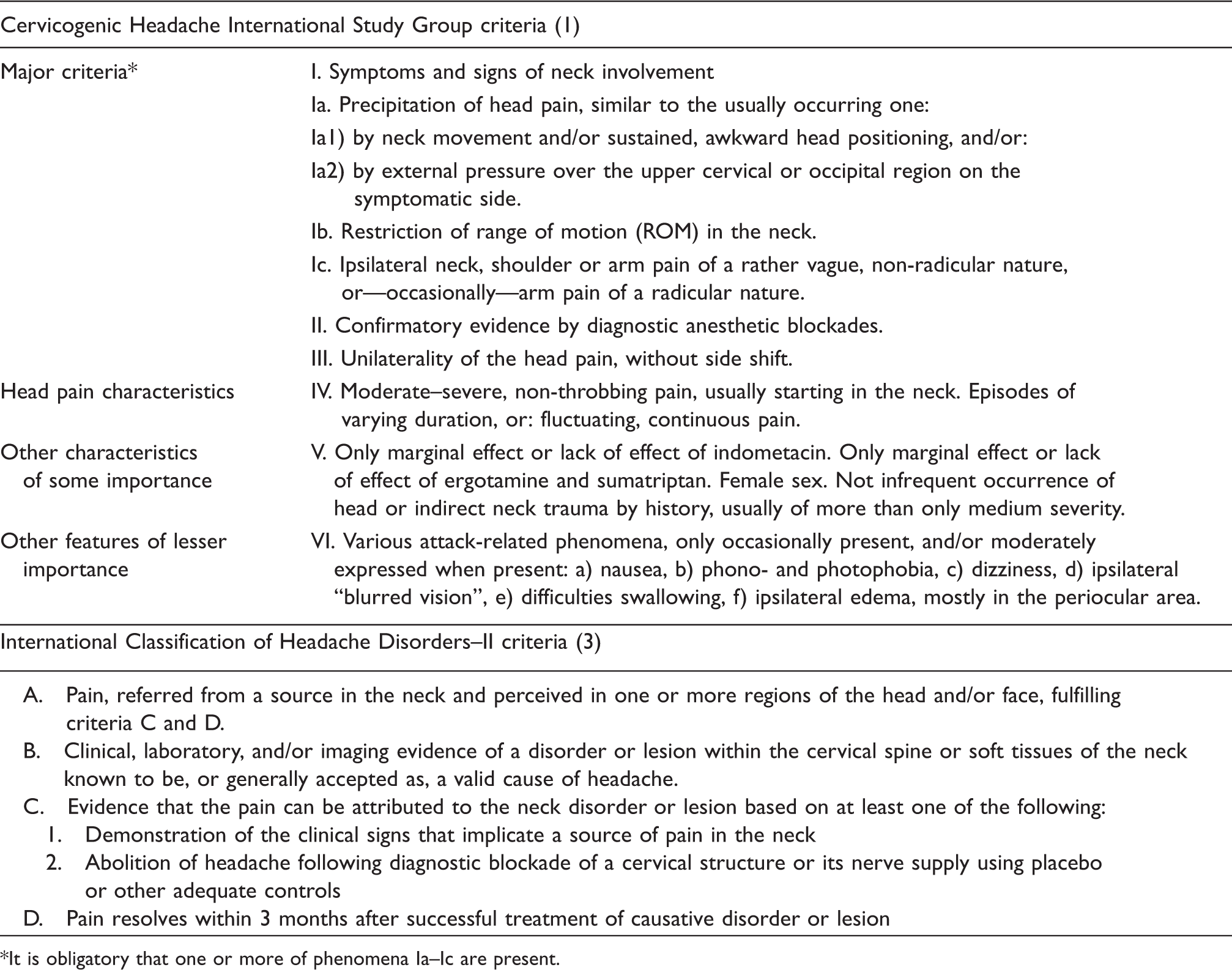
It is obligatory that one or more of phenomena Ia–Ic are present.
Pericranial muscle tenderness
The palpation of muscles and tendon insertion was conducted with the second and third fingers with small rotating movements and a certain pressure. The methodology was trained at the Danish Headache Center (20). The masseter, pterygoideus lateralis, temporalis, frontalis, sternocleidomastoideus, trapezius and occipital muscles and the tendon insertions on processus mastoideus were palpated. The muscles and tendon insertion on each side were palpated one at a time. Each trigger point was scored on a scale from 0 to 3 (0 = no visible reaction or verbal report of discomfort, 1 = mild mimic reaction but no verbal report of discomfort, 2 = verbal report and mimic reaction of painful tenderness and discomfort, and 3 = marked grimacing or withdrawal, verbal report of marked painful tenderness and pain). The maximum tenderness score is 24 on each side and total maximum score is 48.
Cervical range of motion
The passive cervical range of motion (ROM) was tested by manual flexion, extension, lateral flexion and rotation of the cervical spine and was visually estimated. Normal ROM was defined according to the results of the three-dimensional analysis of the cervical spine motion in normal individuals (21).
Greater occipital nerve blockade and other treatment modalities
All persons with CEH were invited to undergo GON blockade between August and September 2007. The GON blockade included a mixture of 1 ml xylocaine 20 mg/ml and 1 ml marcaine 5 mg/ml and was conducted on the symptomatic side by a neurological resident (HKK) according to the procedure (22). The efficacy evaluation of the GON blockage as well as other treatments modalities was based exclusively on the patients' self-reports.
Follow-up
Re-interview and re-examination by a neurological resident (HKK) were performed between August and September 2007. Of the 24 persons with CEH 19 were follow-up, 3 could not be reached by telephone after at least six attempts at different times and two were not eligible due to incorrect phone number. Thus, the participation rate among those eligible at the first follow-up was 86% (19/22).
Data processing
All questionnaires were scanned using TeleForm v9 (Autonomy Cardiff, Vista, CA, USA). Interviews were recorded electronically using SPSS Data Entry 4.0. The statistical analyses were performed using SPSS Base System for Windows 15.0 (SPSS, Chicago, IL, USA). Adjusted prevalence was calculated with a 95% confidence interval (CI) using the Vassar College (Poughkeepsie, NY, USA) statistics website. We used the χ2- test with a 5% level of significance.
Ethical issues
The Regional Committees for Medical Research Ethics and the Norwegian Social Science Data Services approved the project. The participants who received GON blockade were informed about the procedure and side effects. All participation was based on informed consent.
Results
Participants
A total of 24 persons (7 men and 17 women) had CEH according to revised criteria of CHISG (Figure 1). Two persons fulfilled six criteria, two persons fulfilled five criteria, 11 persons fulfilled four and nine persons fulfilled three.
Prevalence
The prevalence of CEH was 0.13% (95% CI 0.06–0.28%) in men and 0.21% (95% CI 0.13–0.34) in women, while the overall prevalence was 0, 17% (95% CI 0.11–0.26%).
Symptomatology
Clinical features of cervicogenic headache in relation to CHISG criteria (1)

CHISG = Cervicogenic Headache International Study Group.
Medication overuse
Analgesic overuse was seen in 50% (N = 12) of the persons with CEH. Fifty-eight per cent of those persons overused only one analgesic medication (43% paracetamol and 57% NSAIDs). Forty-two percent overused more than one analgesic medication. Five persons overused opioids, two persons overused tramadol and oxycodon and three persons overused codeine.
Co-occurrence of migraine
Forty-two per cent had co-occurrence of migraine. The mean age at migraine onset was 23 years for both migraine with (6–40) and without aura (12–34). The pain onset, intensity and duration of a migraine attack was distinct from the milder continuous pain related to CEH. Accompanying symptoms such as phono- and photophobia and nausea were present in 100% of migraine attacks and 50% had experienced vomiting during a migraine attack.
Pericranial muscle tenderness
Distribution of pericranial muscle tenderness scores (0–3) in seven muscle pairs and one pair of tendon insertions in the head and neck

dxt = right side. sin = left side.
Cervical range of motion
Cervical range of motion

SD = standard deviation.
Grater occipital nerve blockade
GON blockade on pain side resulted in ≥90% pain reduction on a Visual Analog Scale (VAS) in five of six persons who received it. The mean duration of the GON blockade effect was 2.4 days. Four persons reported to be pain-free after cryoanalgesic therapy with a mean pain-free period of 79 days (95% CI. 56–102). Those persons refused additional invasive treatment with GON blockade. Nine persons declined to participate due to the invasive nature of the procedure.
Management
Subjective positive efficacy of different treatment modalities

Discussion
Main findings
Our main finding is the 0.17% prevalence of CEH in the general population 30–44 years old. We found that the pericranial muscle tenderness score was significantly higher on the pain than non-pain side and that the cervical ROM was significantly reduced compared to healthy controls.
Prevalence
Our 0.17% prevalence of CEH in the general population is much lower than the 0.4–4.6% prevalence of CEH found in other studies, even though we used liberal inclusions criteria—that is, requiring only three of the six CHISG criteria to be fulfilled for the diagnosis of CEH. However, a risk for underestimation of the prevalence should be considered using a relatively young study population, while other epidemiological studies included individuals with older age (7,10). Because 77% of the participants were interviewed at the clinic and only 23% were interviewed by telephone, the telephone interview is not likely to account for the low prevalence of CEH in our study. Prevalence is highly affected by the classification applied. We differentiated between CEH and chronic headache attributed to whiplash injury, based on unilateral origin of the pain. CEH has been defined, in principle, as a unilateral headache without side shift. However, in the most recent version of CHISG criteria, the strict unilaterality criterion has been softened. CEH is a complex syndrome caused by a variety of lesions that might reproduce pain on the contralateral side (23). Many migraineurs report unilateral migraine, but sometimes when the pain is particularly intense pain may also occur, though less pronounced, on the other side. Patients with bilateral headache or neck pain after whiplash injury are diagnosed as CEH in many headache centers. It is also difficult to be absolutely sure of how strictly the criterion of unilaterality has been followed in other epidemiological studies.
If we had included the persons with chronic headache attributed to whiplash injury (2 men and 18 women) in the CEH group, our prevalence would have increased from 0.17% to 0.32%—still a lower prevalence compared to other studies (18).
The high prevalence of co-occurrence of migraine was due to episodic attacks of migraine and not chronic migraine. The majority of headache days were characterized by a unilateral moderate/severe pressing/tightening pain without accompanying symptoms, as shown in Table 2.
None of our participants with CEH had chronic migraine according to the ICHD-II criteria. The GON blockade was used as a diagnostic tool according to the CHISG diagnostic criteria. The diagnostic value of this procedure is controversial and it might only be useful in addition to a detailed clinical picture (24).
Clinical features
The nuchal onset of the pain correlates with the pericranial muscle tenderness of the occipital muscles. Another study showed that CEH had significantly more posterior onset of pain as compared to migraine without aura (25,26).The mean duration of CEH was eight years (95% CI 5–11). The long duration suggests that CEH often becomes chronic. Part of this is due to insufficient pharmacological and non-pharmacological treatment strategies. Medication overuse is likely secondary to the chronic pain rather than a confounding factor, as the medication overuse is of shorter duration than the CEH. Considering that CEH is a daily chronic pain, surprisingly only 29.2% had consulted a neurologist and only 21% had consulted a pain clinic. This may be due to moderate pain intensity. The lack of consulting a headache specialist may also contribute to medication overuse. Although only a small number of persons received the GON blockade, the treatment was quite effective in our population. The same applies to cryoanalgesic therapy although the data were from the patients' reports. This is quite interesting given that pericranial muscle tenderness was significantly more pronounced on the pain than the non-pain side. The reduced cervical ROM is likely to be secondary to the pericranial muscle tenderness, although pain elicited from other structures in the neck might also play a role.
Methodological considerations
The sample size was chosen to ensure adequate numbers of chronic headache patients for accurate descriptive and epidemiological statistics. The age range of 30–44 years was chosen because the prevalence of chronic headache is relatively higher than in a younger age range, while co-morbidity of other diseases is lower than in an older age range. In addition, use of possibly interfering medications increase after the age of 45–50 (27). As this is an epidemiological survey on headache, responders of the questionnaire may be overrepresented by those with headache. However, replies to the first, second and third questionnaires issued did not imply that this was important in relation to self-reported chronic headache. Questionnaires are generally not accurate enough for diagnosing headaches (28). However, single simple questions such as “Have you ever had tension-type headache?” and “How many days did you have tension-type headache within the last year?” are more valid, as these questions compared to a clinical interview by a physician showed kappa values of 0.74 and 0.77, respectively. Thus, our question about unspecified headache frequency is likely to be valid. The ‘gold standard’ has been suggested to be an interview and a physical and neurological examination by a physician experienced in headache diagnostics (28–31). For that reason, neurological residents with experience in headache diagnosis conducted the investigation. Because three physicians conducted the investigations, interobserver variation is possible. However, the third physician confirmed the diagnoses in all eligible participants, suggesting that interobserver variation is low regarding cervicogenic headache. The majority of participants were interviewed at the clinic. The neurological examination did not reveal abnormalities that caused a change of the headache diagnosis. We first applied the criteria of CHISG, fulfilling three of six criteria as a minimum. Then we also used the stricter revised criteria of CHISG. The central issue of the ICHD-II criteria is to find evidence that the pain can be attributed to a neck disorder or lesion. However, features like neck trauma, mechanical exacerbation of pain and reduced ROM are neither unique nor specific to CEH. According to the criteria of the ICHD-II and CHISG, GON blockade has a diagnostic value for CEH; it was performed in the follow-up in 25% of the persons with CEH. Four additional persons received cryoanalgesic treatment and were pain-free at the time of investigation. Our efficacy and treatment data for cryoanalgesic therapy are low in number and exclusively based on patients' reports. We considered them as positive responders in terms of nerve blockade as well. Nine persons who declined GON blockade because of the invasive character of the procedure were still diagnosed as CEH, since at least three of the other CHISG criteria were fulfilled. However, GON blockade is not an absolute requirement of ICHD-II criteria. The application of both ICHD-II and CHISG criteria makes the diagnoses unambiguous. Diagnoses for headache associated with head trauma and whiplash do not have specific criteria according to ICHD-II, while CHISG requires more specific criteria. Thus, patients with chronic headache and a head trauma/whiplash injury were classified so according to the ICHD-II criteria, and those with more specific criteria that fulfilled the criteria of CHISG were also classified CEH. If we had applied only the ICHD-II criteria, none of our participants would have fulfilled the criteria for CEH. Thus, the participants would be diagnosed with chronic headache due to post-traumatic headache/whiplash injury or chronic tension-type headache.
Thus, even with the many methodological challenges, our study population is likely to be representative for CEH in the general population, sas we applied the most used criteria for inclusion in our study.
Conclusion
CEH is a rare chronic headache in ages 30–44 years in the general population. Although the number of participants was relatively small, usual pharmacological management was not effective; GON blockade/cryotherapy seems to have an effect in 90%, while other treatment modalities were reported less effective. The nuchal onset of pain, reduced cervical ROM, unilaterality of the pain and the increased ipsilateral pericranial muscle tenderness score as well as the efficacy of GON blockade suggest that local factors in the neck are responsible for pain in CEH. Whether this mechanism is involved in other types of headache cannot be concluded from our study.
Footnotes
Acknowledgements
This study was supported by grants from South-Eastern Norway Regional Health Authority, Hospital Innlandet and Faculty Division Akershus University Hospital, University of Oslo. Hospital Innlandet and Akershus University Hospital kindly provided research facilities.