
Abstract
There is a striking similarity between the migraine-provoking effect of the nitric oxide (NO) donor glyceryl trinitrate (GTN) and that of calcitonin gene-related peptide (CGRP). We tested the hypothesis that NO releases CGRP to cause the delayed migraine attack after GTN.
Methods: In a double-blind-cross-over study, 13 migraine without aura (MO) patients were administered GTN 0.5 µg/kg/minute for 20 minutes and subsequently BIBN4096BS (olcegepant) 10 mg or placebo. Headache scores and development of MO were followed for 24 hours.
Results: MO developed in seven of 13 with olcegepant and in nine of 13 with placebo (p = 0.68). The headache scores were similar after the two treatments (p = 0.58). Thus CGRP receptor blockade did not prevent GTN-induced migraine.
Conclusions: The present study indicates that NO does not induce migraine by liberating CGRP. The most likely explanation for our findings is that CGRP has its effect higher than NO in the cascade of events leading to MO attacks.
Keywords
Introduction
The nitric oxide (NO) donor glyceryl trinitrate (GTN) (1) and calcitonin gene-related peptide (CGRP) (2) both cause a vascular-type headache in human volunteers. In migraine patients they cause a biphasic pattern with an immediate headache during infusion and a delayed headache occurring several hours later. The delayed headache is described by the patients as similar to their spontaneous migraine attacks and in many patients it reaches a point where it fulfils the International Classification of Headache Disorders, second edition (ICHD-II), diagnostic criteria for migraine without aura (MO) (3–5). With such striking similarities between the migraine-provoking effects of GTN and CGRP, it is likely that their mode of action may be interrelated. The question is, however, whether they work in parallel until meeting at a common pathway, or, whether they work in series.
Access to the specific and potent inhibitor of CGRP receptors, BIBN4096BS (later called olcegepant), has offered an opportunity to study the question in human migraine patients. Our hypothesis was that NO releases CGRP from perivascular nerves or from central sites to cause the delayed migraine attack after GTN administration. If that was so, then olcegepant, which has been shown to block all effects of infused CGRP (2), should effectively prevent GTN-induced migraine. To test the hypothesis, we conducted a double-blind, randomised cross-over study in migraine patients. They all received an intravenous (IV) infusion of GTN followed randomly by placebo on one day and olcegepant on another day.
Methods and patients
Design and patients
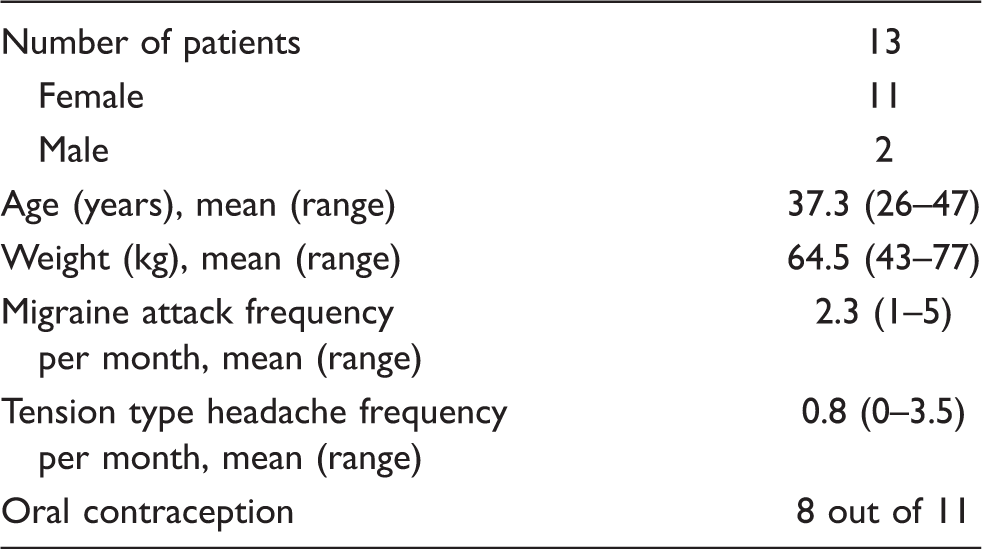
Patient characteristics
The migraine patients received on both trial days an initial 20 minutes infusion of GTN 0.5 µg ⋅ kg−1 ⋅ min−1 (3,6). This was followed 40 minutes later by olcegepant 10 mg or placebo (xylitol 5%) administered as a 10-minute IV infusion. The time delay of 60 minutes between the start of the GTN infusion and the start of the GCRP antagonist allowed the distinction between immediate headache caused directly by administered GTN and delayed migraine headache possibly caused by release of CGRP. Due to its long half-life, there was still a sufficient blood level of olcegepant when the delayed migraine headache developed. Furthermore, most haemodynamic effects of GTN were in previous studies stabile after 60 minutes.
Boehringer Ingelheim GmbH supplied olcegepant and performed a balanced randomisation and blinding (ClinPro version 6, Clinical Systems, Inc., Garden City, NY, USA). The dose of olcegepant was based on a previous phase 1 pre-clinical trial (7) and on a human study showing complete blockade of the majority of effects of CGRP at a dose of 2.5 mg olcegepant (2). Approvals were obtained from the Scientific Ethical Committee for the County of Copenhagen and the Danish Medicines Agency. Signed informed consent was obtained from each patient before randomisation. The study was conducted according to the Helsinki II Declaration as amended in Somerset West, Republic of South Africa, October 1996, and the guidelines for Good Clinical Practice.
Trial procedure
The migraine patients began the study at 7:45
Two intravenous catheters (Optiva*2, [18-gauge] Johnson & Johnson, Ethicon S.p.A., Pomezia, Italy) were inserted into the cubital veins, one for the administration of GTN, olcegepant or placebo, the other for blood sampling. The patients rested at least 30 minutes before recording baseline values of blood flow velocity in the middle cerebral artery (VMCA) with transcranial Doppler (TCD); temporal and radial artery diameter with C-scan; blood pressure (BP); heart rate (HR) (Omega 1400, In vivo Research Laboratories, Inc., Copiague, NY, USA); and electrocardiogram (ECG) (Cardiofax, Nihon Kohden Corp., Tokyo, Japan). The start of infusion of GTN was designated time zero (T0). The infusion (GTN 0.5 µg ⋅ kg−1 ⋅ min−1) lasted 20 minutes and was administered by a time- and volume-controlled infusion pump (Braun® Perfusor, B. Braun Melsong AG, Germany). This was followed 40 minutes later by olcegepant 10 mg or placebo (xylitol 5%) administered as a 10-minute IV infusion. The patients rested supine and BP, HR and ECG were recorded throughout the laboratory study period.
Headache and adverse events
Every tenth minute from T0 (baseline) to T240 (end of period in laboratory) the patients were questioned about the presence of headache. Headache was scored on a numerical verbal rating scale from 0 to 10, where 0 represents no headache; 1 represents a very mild headache, including a feeling of pressing or pulsation (pre-pain); 5 represents a moderate headache; and 10 represents the worst possible headache (1). Headache characteristics (unilateral/bilateral, quality and aggravation by physical activity) and accompanying symptoms (nausea/vomiting, phono- and photophobia) (5) were recorded by a physician in the clinic. Adverse events (AEs) were recorded repeatedly prior to start, during and after infusion of GTN.
The patients were asked to self-report any changes that they might experience between questioning. While patients were in the laboratory, the investigator recorded headache and AEs by means of standard non-guiding questions. After discharge the patient used a diary card to make an hourly recording of headache and AEs up to 12 hours after start of the study. The intensity of the AEs was graded as mild, moderate or severe. The patients were interviewed by phone after 24 hours about migraine and the use of escape medication.
Transcranial Doppler and C-scan
TCD ultrasonography (2 MHz, Multidop X Doppler, DWL, Sipplingen, Germany) was used for the measurement of blood flow velocity in middle cerebral artery (MCA). The recordings were done simultaneously bilaterally, as previously described (8,9). Simultaneous with the TCD recording, a mask covering the subject’s mouth and nose was placed for the measurement of end-tidal PCO2 (PetCO2) (Datex Normocap 200 Dameca, Roedovre, Denmark).
A high-resolution ultrasound scanner, C-scan (Dermascan C, 20 MHz, bandwidth 15 MHz, Hadsund, Denmark) (10) was used to measure the diameter of the left temporal and left radial arteries. To ensure that the repeated measurements with TCD and C-scan were performed in the same place, marks were drawn on the skin. After the last recording on the first trial day, the coordinates of the marks were kept for re-use on the following trial day. Recordings were done every 10 minutes for the first 120 minutes and thereafter every 30 minutes during laboratory stay.
Olcegepant analytical methods
Olcegepant concentrations in human EDTA plasma were quantified by means of competitive enzyme-linked immunosorbent assay (ELISA) using selective, immobilised rabbit anti-olcegepant antibodies and horseradish peroxidase–labeled olcegepant-tracer. The lower limit of quantification is 50 pg/ml plasma and the precision about 2% coefficient of variation (CV) in the middle of the calibration curve (9% at the lower limit of quantitation [LLOQ], precision profile, N = 886). The selectivity of the assay was proven by cross-validation versus a high-performance liquid chromatography (HPLC)–mass spectrometer (MS)/MS method.
H-CGRP analysis
The blood samples were collected into cooled 10-ml tubes prepared with EDTA and Trasylol, (500 µl 10,000 kIU Bayer, Leverkussen, Germany). They were immediately put on ice water, centrifuged at 2000 G for 15 minutes at 6°C, and plasma was transferred to polypropylene tubes (Nunc, Becton Dickenson, France) and stored below −20°C. Subsequently, plasma samples were measured blindly at the same time. The analysis was performed as previously described (11).
Statistics
The primary study parameter was the number of subjects developing delayed MO after olcegepant versus placebo.
Immediate headache was defined as any headache during the first 60 minutes after the start of the GTN infusion. Any headache occurring thereafter was regarded as delayed headache. Peak values and AUCheadache (area under the headache curve) were compared between the two trial days using Wilcoxon signed rank test. The occurrence of headache and AEs on the two trial days was compared with McNemar’s test.
T−10 was considered as baseline in the analysis. Values are presented as means ± standard deviation (SD); p < 0.05 was considered significant. All analyses were performed using SPSS statistical software, versions 10.0 and 11.1 (Chicago IL, USA).
For changes over time on each trial day, VMCA, diameter of the temporal and radial arteries, BP and PetCO2 were analysed by a univariate analysis of variance for the factors time and subject. If a significant change was found, a post hoc analysis (Dunnett’s multiple comparisons test) was performed to localise the change. To eliminate the risk of mass significance on measurements with numerous repeated measurements, four points of interest were chosen: baseline, 20, 60, 120 and 180 minutes post-infusion start. Absolute values were used for the statistical analysis. For the comparison between olcegepant and placebo, a paired t-test was performed for the following measurements: VMCA, diameter of the temporal and radial arteries, BP and PetCO2. The summary measure tested by the t-test was the area under curve (AUC) calculated on percentual changes from baseline for each parameter.
Power calculation was done in designing the study. If a risk of type 1 error of 5% and a risk of type 2 error of 10% (90% power) were accepted, with a standard variation below 50%, the necessary number of patients was estimated to be 15 (from Figure 15.2 in D.G. Altman, Practical Statistics for Medical Research, London, Chapman and Hall, 1991, p.455–60).
Because only 13 patients completed the study, an additional power calculation was made: (paired t-test, migraine 80% versus 40%, p = 0.05 power 80%) The needed sample size was estimated to 11 patients (1-sided), 14 patients (2-sided) (SAS statistics software, SAS Institute, Cary, NC, USA).
Results
Migraine and headache
Headache characteristics and associated symptoms *

The primary efficacy parameter was the number of patients developing delayed MO (5). The criteria for MO were fulfilled in nine patients after placebo and in seven patients after olcegepant (p = 0.68). No significant difference in AUCheadache (p = 0.58) was found between placebo and olcegepant. The mean headache curves for both trial days are displayed in Figure 1.
Mean headache scores (N = 13) from the beginning of glyceryl trinitrate (GTN) infusion to 800 minutes after GTN plus placebo and GTN plus olcegepant 10 mg intravenous. The individual maximal headache on a scale from 0–10 occurred at different time points, with mean of 4.8 (range 0–10) on placebo and mean 4.3 (range 1–9) on olcegepant. There was no difference in any headache parameters on the two treatment days. The diagnostic criteria for migraine without aura were fulfilled in nine out 13 patients after placebo and in seven patients after olcegepant (p = 0.68).
Delayed headache was induced by GTN in 12 out of the 13 patients. The range of peak headache score on GTN plus placebo was 0–10, median 5. On olcegepant, the median was 4 (range 0–9) (p = 0.69).
One of the immediate headaches fulfilled the IHS criteria for MO during GTN infusion (patient 7, Table 2). The only associated symptom was mild nausea which diminished after the GTN infusion. The headache at that time point was not rated by the patient as usual migraine, but later developed into a severe migraine attack (headache score 9, unilateral, pulsating with aggravation, severe nausea and moderate phono- and photophobia), and was not relieved by olcegepant.
Cerebral and peripheral haemodynamics
There was no difference between trial days with regards to baseline PetCO2 changes over time. The VMCA was therefore not corrected for changes in PetCO2. Overall, no significant differences between the two days where found, neither in bilateral mean VMCA (p = 0.20) nor analyzing left and right side separately (p = 0.14 and p = 0.49). There was no effect of olcegepant on VMCA (p = 0.21). On both trial days a significant decrease was recorded over time compared to baseline for mean VMCA (Figure 2).
Effect of glyceryl trinitrate 0.5 μg/kg/min intravenous (IV) for 20 minutes and subsequently placebo or BIBN4096BS (olcegepant) 10 mg IV on mean blood velocity in the middle cerebral artery (mean + standard deviation [SD]). On placebo days a significant decrease (p < 0.001) compared to baseline was seen at all time points with a maximum at time T20 (−19.3 ± 2.2 cm/sec). Similar significant decrease was seen on olcegepant days (p < 0.001) with a maximum decrease at T20 (−16.7 ± 2.7 cm/sec). No difference was seen between olcegepant and placebo, indicating that GTN’s vascular effect is without calcitonin gene-related peptide involvement.
GTN administration induced a significant increase in the diameter of both the superficial temporal artery (STA) (45% and 47%) and the radial artery (RA) (38% and 38%) over time compared to baseline (p < 0.001 for both). There was no difference between olcegepant and placebo STA (p = 0.29) or RA (p = 0.5) diameter.
Systemic haemodynamics
A significant decrease in mean BP was seen on both trial days compared to baseline (from 90.4 to 85.2 mmHg on placebo day and from 90.0 to 80.0 mmHg on olcegepant day (p = 0.01). The significant difference was seen at time point T20. The mean HR increased significantly with a maximum at 5 minutes into GTN infusion (64–72 beats/min on placebo day and 67–75 beats/min on olcegepant day) compared to baseline (p < 0.001 and p = 0.037).
For mean BP (baseline 90 mmHg) and HR (baseline 64 beats/min), no significant difference between placebo and olcegepant days was found.
Adverse events
All adverse events (AEs) were mild to moderate, the most prominent being short-lasting paresthesia during infusion with olcegepant (nine out of 13). They were typically described as a tickling and itching feeling starting on the back and spreading to chest, scalp, both arms and thighs. They disappeared in the same order within a few minutes. Facial flushing was seen in four out of 13 patients during olcegepant infusion. During GTN infusion facial flushing was seen in two patients.
Olcegepant blood levels
At the end of the olcegepant infusion, the mean plasma concentration was 919 ng/ml (range 540–1290 ng/ml). Thirty minutes after the start of the infusion, the mean concentration was 333 ng/ml (range 200–489 ng/ml). After 60 minutes it was 181 ng/ml (range 94–248 ng/ml); and after 180 minutes it was 54 ng/ml (range 14–95 ng/ml). Inspection of the concentration curve indicated that no formal pharmacokinetic analysis should be performed, due to the lack of blood samples at later time points, as was done in a formal pharmacokinetic study (7). However, the quick decrease in olcegepant concentration from 10 to 30 minutes indicates a quick distribution from blood to tissue.
CGRP plasma levels
Cubital CGRP plasma levels were measured to these time points: baseline, 30, 60, 90, 120, 180 and 240 minutes. The mean plasma levels of CGRP at baseline were 21 pmol/l (range 14–31) on olcegepant trial day and 23 pmol/l (range 8–31) on the placebo day. There were no changes in CGRP over time.
Discussion
The main finding in the present study was that the CGRP receptor antagonist olcegepant (BIBN4096BS) given in a high dose was ineffective in preventing GTN-induced migraine. Implications of this result shall be discussed here.
Olcegepant in a dose of 2.5 mg IV is effective in the treatment of spontaneous acute migraine attacks (12). Furthermore, olcegepant 2.5 mg completely blocked all effects of infused CGRP (2). Thus, receptor blockade in the present study must have been nearly complete. One possible exception are structures behind the blood-brain barrier (BBB) (2). If GTN were to release CGRP from nerves around these arteries, it is possible that olcegepant would not have been able to block its effect. However, many believe today that migraine attacks are caused by central release of CGRP acting on central nervous system (CNS) structures (13,14). They argue that olcegepant must be given in 1000 times higher dose in migraine than that needed to block CGRP receptors in human cerebral arteries (14,15). In the present study, the Cmax for olcegepant was 919 ng/ml, the same as in healthy volunteers (1090 ng/ml) (7). This concentration of olcegepant, corrected for the protein binding of 0.69 (Henri Doods, personal communication) corresponds to 0.3 μM and the EC50 is 0.1 nM on human cerebral arteries (15). The concentration of olcegepant in the present study therefore far exceeded the concentration needed to block CGRP. Despite the possibility of an action of olcegepant even behind the BBB, the number of subjects with delayed migraine was quite similar in the olcegepant-treated group (7/13) and the placebo-treated group (9/13). In a previous study olcegepant 2.5 mg was effective in spontaneous migraine attacks when given during the attack (12). In the present study the drug was given after GTN but before the delayed migraine attack. Thus, the drug had sufficient time to act; however, giving the drug before migraine may pose a problem in the light of previous experience with the triptans. Thus, two randomised, placebo-controlled, clinical trials where triptans were given in the aura phase of migraine were both negative (16,17). Because triptans are not effective when given before migraine headache, the same could possibly be the case for a CGRP receptor antagonist. However, because olcegepant 2.5 mg IV was effective in preventing CGRP-induced headache in healthy volunteers it seems likely that it should also prevent GTN-induced migraine if the latter were caused by CGRP release.
It has been suggested that the vasodilator effect of NO on cranial vessels is partly exerted by release of CGRP (18,19). Other animal studies (20,21) indicated that this is not the case. Whether such a pathway is present in humans is unknown. In healthy volunteers GTN infusion did not result in an increase in CGRP levels as measured in the external jugular vein for up to 80 minutes after start of GTN infusion (22). In the present study GTN did not increase CGRP in the cubital vein. CGRP was followed only up to 240 minutes after GTN infusion and therefore not in all patients during their GTN-induced migraine. This does not, however, exclude a delayed effect of GTN on CGRP. In the rat, release of NO continued at least one hour after an IV infusion of GTN (23). In one study sodium nitroprusside for 10 minutes caused a delayed increase in trigeminal neuronal activity with a latency of 50 minutes in a rat model of migraine (24). A similar mechanism in humans has been suggested in order to explain the delayed migraine. One would therefore expect a prolonged or biphasic NO release in migraine patients after 0.5 µg/kg/minute of GTN infusion, which is a relatively high dose (25). In the present study the CGRP antagonist olcegepant did not alter haemodynamic parameters, in contrast to an animal study (18) in which a CGRP antagonist, CGRP(8-37), inhibited the vasodilator effect of GTN. In the present study no difference was seen between olcegepant and placebo in the haemodynamic changes of the cerebral and temporal arteries or of HR or BP before, during and after GTN infusion. Olcegepant’s lack of effect indicates that CGRP is only to a minor extent or not at all involved in the dilator effect of NO in the cranial, extracranial or systemic vascular beds in humans.
In a rat model of migraine, GTN infusion (4 μg/kg/min for 2 hours) induced a persistent increase in activity of neurons in the spinal trigeminal nucleus. CGRP inhibition with IV olcegepant (900 μg/kg infused over 5 min) normalised the neuronal activity (26). By contrast, we did not find a similar effect in humans. This could be due to much higher doses in the animal study or to species difference.
We have recently reported that aspirin and zolmitriptan were ineffective in headache induced by a continuous and long-lasting infusion of GTN in healthy volunteers (27). This finding indicates, in consonance with the present results, that NO induction of headache is a very basic mechanism and difficult to treat. In the present study nine out of 13 patients experienced short-lasting paresthesia during infusion with olcegepant. This could possibly, to some degree, have unblinded some of the patients. However, that occurrence would have been of greater concern if the study had shown an effect of olcegepant.
During GTN infusion in the present study, the decrease in blood flow velocity in the MCA and increase in the diameter of the STA were similar to previous results (3,9). The cranial arteries of the migraine patients were thus dilated by GTN, and delayed migraine occurred in approximately 70% of cases (3,6,28).
In conclusion, the present study indicates that NO does not induce migraine by liberating CGRP, because blockade of the CGRP receptor had no effect on GTN-induced migraine.
The most likely explanation for our findings is that CGRP has its effect higher than NO in the cascade of events leading to migraine without aura attacks. In such a case GTN bypasses CGRP by delivering NO directly to the target site.
Footnotes
Acknowledgements
We are grateful to Dr Ulrich Kunz, Boehringer Ingelheim Pharma KG, Department of Pharmacokinetics and Drug Metabolism, Biberach, Germany, for analysis of olcegepant concentration. Lab technicians Lene Elkjær and Kirsten Brunsgaard are thanked for their skilful help with measuring the vessel response and handling the blood samples. The study was supported by the Lundbeck Foundation via the Lundbeck Foundation Center for Neurovascular Signaling (LUCENS).
Conflicts of interest
Peer Tfelt-Hansen has consulted for McNeil International. Jes Olesen has within the last two years received grants/research support from and/or has been a consultant/scientific advisor for, and/or has been on the speaker’s bureau of Merck, Pfizer, Minster Pharmaceuticals, RoxRo Pharma, MAP Pharmaceuticals, NeurAxon and Lundbeck. Kenneth A Petersen is employed by Lundbeck. Jesper F Tvedskov and Lars T Jensen report no conflicts of interest.