
Abstract
Introduction: It is well-known that specific foods trigger migraine attacks in some patients. We aimed to investigate the effect of diet restriction, based on IgG antibodies against food antigens on the course of migraine attacks in this randomised, double blind, cross-over, headache-diary based trial on 30 patients diagnosed with migraine without aura.
Methods: Following a 6-week baseline, IgG antibodies against 266 food antigens were detected by ELISA. Then, the patients were randomised to a 6-week diet either excluding or including specific foods with raised IgG antibodies, individually. Following a 2-week diet-free interval after the first diet period, the same patients were given the opposite 6-week diet (provocation diet following elimination diet or vice versa). Patients and their physicians were blinded to IgG test results and the type of diet (provocation or elimination). Primary parameters were number of headache days and migraine attack count. Of 30 patients, 28 were female and 2 were male, aged 19–52 years (mean, 35 ± 10 years).
Results: The average count of reactions with abnormally high titre was 24 ± 11 against 266 foods. Compared to baseline, there was a statistically significant reduction in the number of headache days (from 10.5 ± 4.4 to 7.5 ± 3.7; P < 0.001) and number of migraine attacks (from 9.0 ± 4.4 to 6.2 ± 3.8; P < 0.001) in the elimination diet period.
Conclusion: This is the first randomised, cross-over study in migraineurs, showing that diet restriction based on IgG antibodies is an effective strategy in reducing the frequency of migraine attacks.
Introduction
The exact pathophysiology of migraine is still unclear. Besides different genetic mutations, there is evidence of a profound role of meningeal inflammation in migraine pathogenesis (1,2). Environmental trigger factors are thought to play an important role. Many contributing factors may trigger the occurrence of migraine attacks and food is one of the most well-known (3–8). These, however, as with most elements of migraine, need to be individualised to the patient with migraine.
Since the 1930s, hidden food allergy has been suspected to be linked to migraine. Several studies showed significant improvement when patients were put on an elimination diet (9–14). IgE-specific food allergy has been shown to be related with migraine supported by the success of individualised diet in controlling migraine attacks (4,15). Non-IgE antibody mediated mechanisms have also been proposed in food allergy (16). Aljada et al. (17) provided evidence for the pro-inflammatory effect of food intake. IgG antibodies against food antigens have been found to be correlated with inflammation and intima media thickness in obese juveniles (18). Several studies reported significant improvement in irritable bowel syndrome (IBS) by food elimination based on IgG antibodies against to food antigens (19–22). Rees et al. (23) showed a beneficial effect of a diet guided by IgG antibodies to food in migraine patients. Recently, Arroyave Hernandez et al. (24) reported preliminary evidence that IgG-based elimination diets successfully controlled the migraine without need of medication.
Some foods (such as cheese, chocolate or wine) are thought to be one of the well-known reasons triggering of migraine attacks according to consistent reports from the patients. It has been reported that diet with low-fat intake could reduce the headache frequency and intensity (25). On the other hand, some additives (such as triclorogalactosucrose or aspartame) may trigger attacks in some migraineurs (4,26–29). However, it is neither easy nor very useful to organise routine diet according to robust protocols for many patients (3,30). All this indicates that there is a need for an individualised approach of the diet to relieve migraine. One has to distinguish between inflammation-induced migraine and migraine caused by food via other mechanisms such as histamine-induced vasodilatation.
IgG could be one of the markers to identify food which causes inflammation and could cause migraine attacks in predisposed individuals.
In this study, we aimed to test the beneficial effect of diet based on specific total IgG antibodies (subclasses 1–4) against 266 food antigens in controlling migraine in a double-blind, randomised, controlled, cross-over clinical trial.
Subjects and methods
Experimental protocol
This study was designed as a double-blind, randomised, controlled, cross-over clinical trial (31). After the approval of the hospital ethics committee, patients giving their written informed consent were recruited from headache out-patient clinic with the diagnosis of migraine without aura according to the criteria of the International Classification of Headache Disorders, 2nd edition (32). For inclusion in the study, the patients should: (i) have had at least 4 attacks and 4 headache days per month within the last months; (ii) be aged 18–55 years; (iii) be treated with acute attack medications only or with preventive medications unchanged at least for 3 months; and (iv) be able to understand and co-operate with the needs of the study and the diet. The patients with suspected or clear-cut medication overuse, pure menstrual migraine or any other associated headache disorder were excluded.
The study consisted of three main phases – baseline phase, first diet
phase and second diet phase (Figure 1). In all phases, patients were asked not to change the
dosages of their preventive medications if they were using any. The patients
visited the same headache physician (first author, blinded to antibody test
results and the order of the patient’s diet phases) during the whole
study. At the first visit (Visit-1), the eligible patients recruited for the
study were evaluated and asked to complete a headache diary for 6 weeks. The
diary included headache attack frequency, headache days, attack duration in
hours, attack severity in visual analogue scale (VAS) and medication
information. During this 6-week baseline phase, the patients were followed in
their usual daily diet. At the second visit (Visit-2) at the end of this 6-week
baseline phase, the patients returned their diaries for evaluation and gave
venous blood samples for detection of IgG antibodies against 266 food antigens
(see Appendix 1) as described below. Then, the patients were allocated to one of
the two 6-week diets based on a randomisation schedule either excluding
(elimination diet) or including (provocation diet) specific foods with
abnormally raised IgG antibodies, as described below. They were also asked to
fill in a headache diary for 6 weeks. In this ‘first diet
phase’, half of the patients were randomised to elimination diet and
other half maintained provocation diet for 6 weeks. Neither the patients nor the
headache physician knew if the diet was for elimination or provocation as well
as IgG antibody test results. At the third visit (Visit-3) at the end of the
‘first diet phase’, the patients returned their diaries
for evaluation. Then, the patients were allowed to return to their usual diets
for 2 weeks without keeping diary. In ‘second diet
phase’ following this 2-week diet-free interval, the patients who
were on elimination diet in the ‘first diet phase’ were
given provocation diet for 6 weeks and vice versa. They were asked to fill a
headache diary for 6 weeks during the second diet phase. At the fourth visit
(Visit-4) following the ‘second diet phase’, diaries
were recollected and the diet codes were broken. Patients were informed about
their results and the order of the types of their diets. Cross-over design of the study.
IgG antibody detection against food antigens
IgG antibodies against 266 food antigens were detected using a commercially available enzyme linked immunosorbant assay (ELISA) test (ImuPro 300 test; Evomed/R-Biopharm AG, Darmstadt, Germany), previously used by Wilders-Truschnig et al. (18) IgG calibration was performed against the international reference material 1st WHO IRP 67/86 for human IgG. Quantitative measurements are reported in mg/l. Detection limit was 2.5 g/l, normalised cut-off value was 7.5 mg/l, according to the validation protocol provided by the manufacturer. All values above 7.5 mg/l were considered as positive reaction to the corresponding food. Positive reaction was graded as: ‘low’ for titres between 7.50–12.50 mg/l; ‘moderate’ for 12.51–20 mg/l; ‘high’ for 20.1–50 mg/l; and ‘very high’ for 50.1–200 mg/l. Since IgG antibodies against food disappear within 3 months to 2 years depending upon initial titre, antibody detection was not repeated after the diet phases which were not long enough to see any change in antibody titres.
Diet preparation
Diets were arranged according to the IgG antibody results; eating habits for individual patients were taken into account and patients were educated about keeping diet by a dietician (DKU, co-author). Diets were assembled by this dietician, trying to offer a nutritionally balanced diet. The elimination diet consisted of a defined panel of IgG-negative food, while the provocation diet consisted in a panel of IgG-positive food and IgG-negative food necessary to comply with a balanced diet. Both elimination diet and provocation diet did not differ in calorie content. Patients were not allowed to eat any other food as specified by the dietician. In both diet phases, patients were never forced to eat or avoid from certain foods to protect the blindness of patients and their physician for the type of diet phase (elimination or provocation). Instead, they were asked to follow their specially arranged diet list exactly and not to consume any other food in any diet phase.
Statistical analysis
The primary parameters used for comparisons were number of headache days, migraine attack count, mean attack duration, median attack severity (in VAS score from 0–10), number of migraine attacks with acute medication and total medication intake within 6-week periods of each three phases. Statistical analyses included parametric tests to compare means (paired and unpaired two sample t-test), non-parametric tests to compare medians (Wilcoxon test and Mann–Whitney test) and 2 × 2 chi-square test. For comparisons between baseline phase and provocation phase or between baseline phase and elimination phase or between provocation phase and elimination phase, both paired t-tests (parametric test and Wilcoxon signed test as non-parametric test) were used. For comparisons between patients whose first diet phase was elimination diet and patients whose second diet phase was elimination diet (to test the ‘period effect’), both unpaired t-tests (parametric test and Mann–Whitney unpaired test as a non-parametric test) were used.
Results
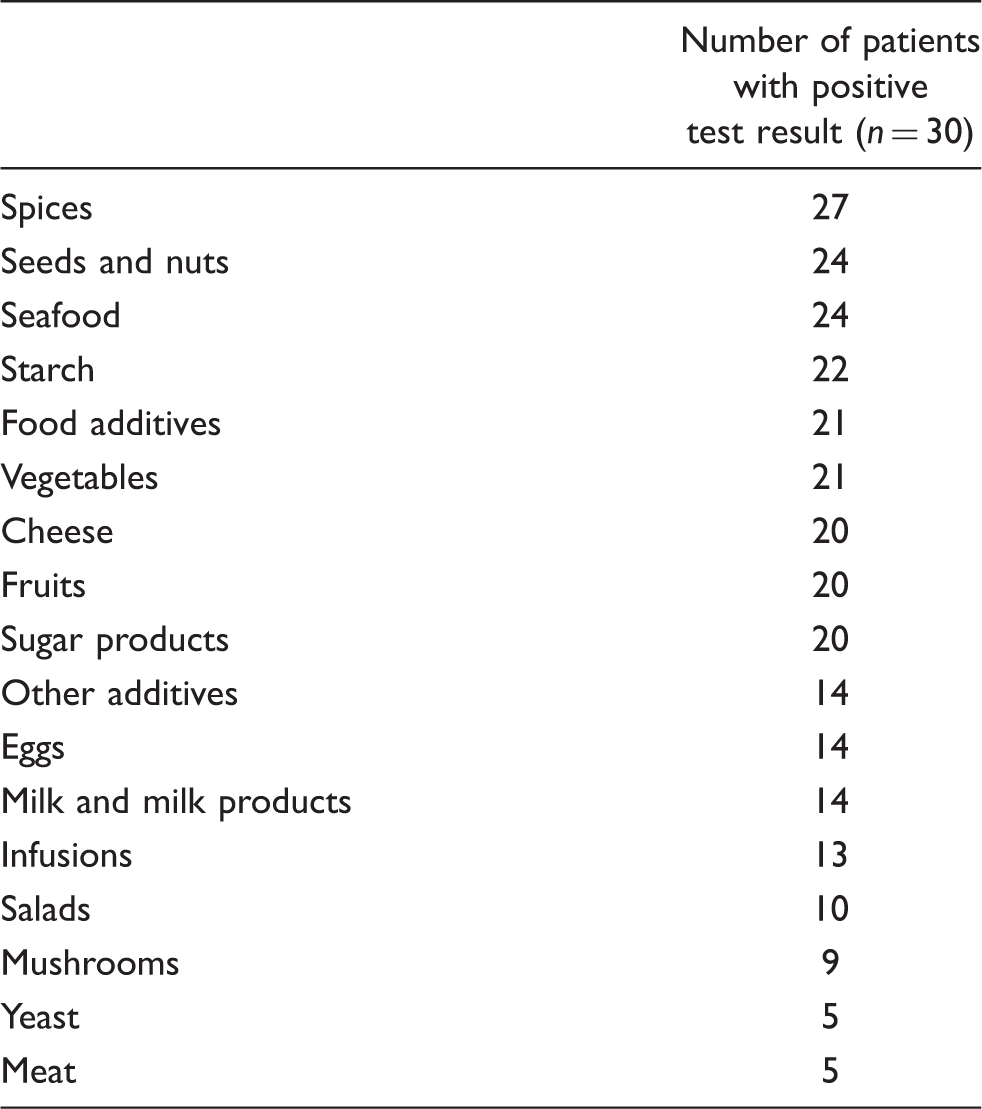
The food categories from most frequent IgG positivity to least
Headache and medication parameters during study phases
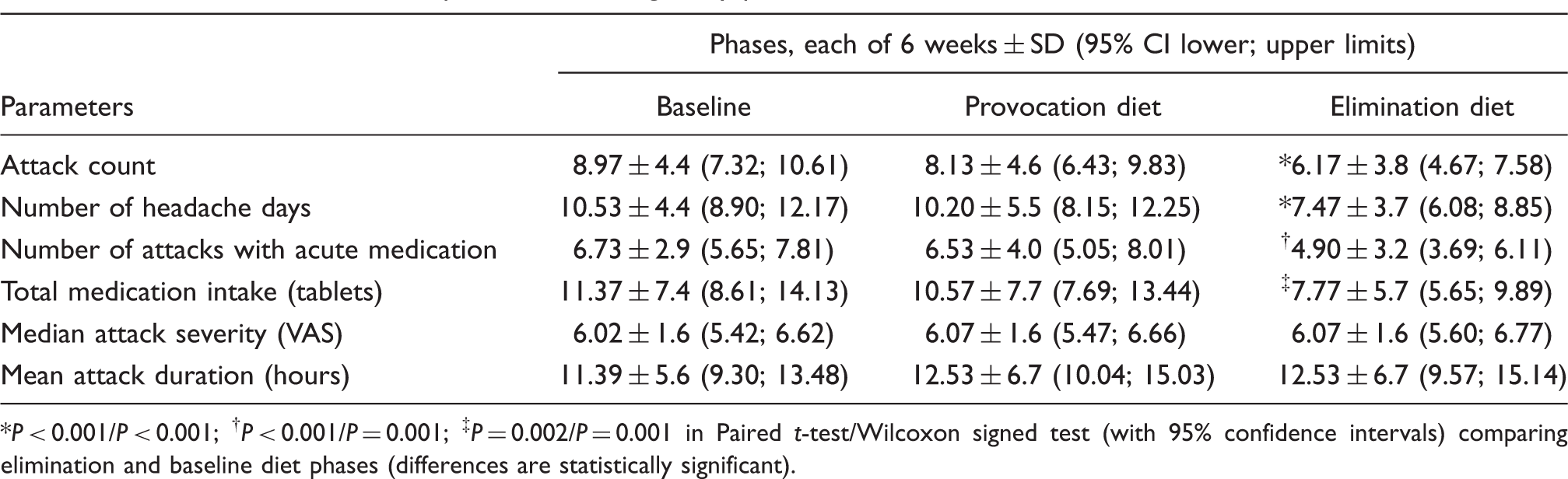
*P < 0.001/P < 0.001; † P < 0.001/P = 0.001; ‡ P = 0.002/P = 0.001 in Paired t-test/Wilcoxon signed test (with 95% confidence intervals) comparing elimination and baseline diet phases (differences are statistically significant).
Percentage difference of parameters from baseline period
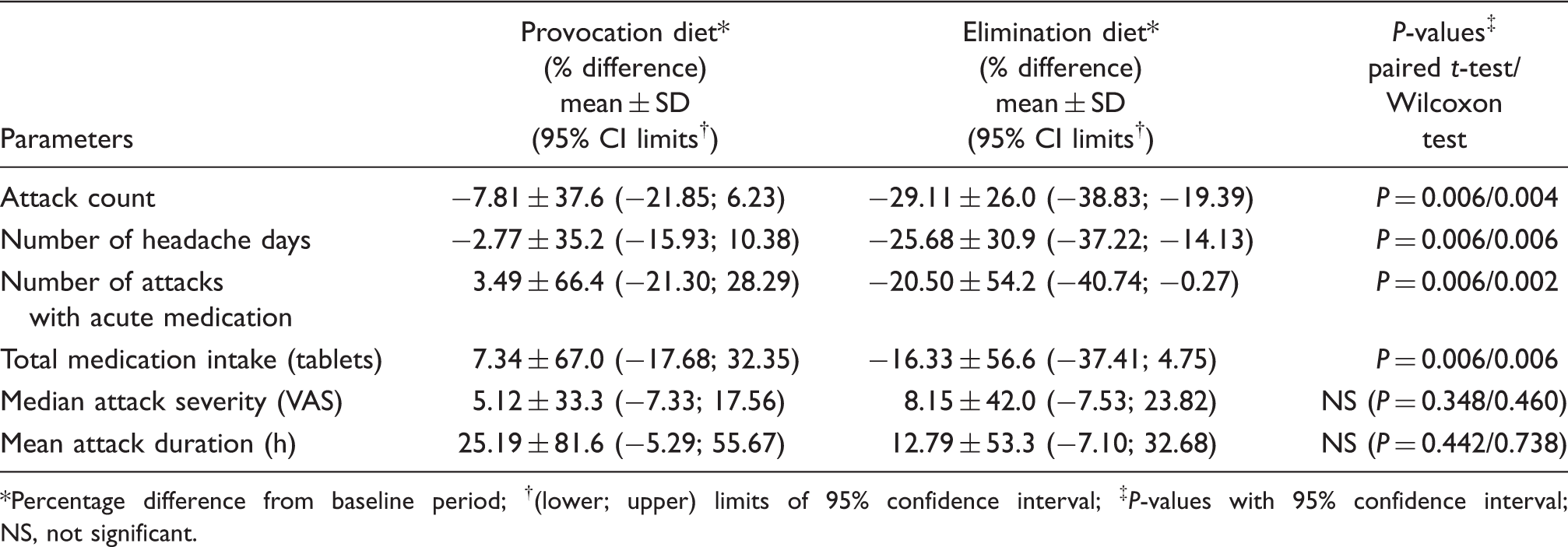
*Percentage difference from baseline period; †(lower; upper) limits of 95% confidence interval; ‡ P-values with 95% confidence interval; NS, not significant.
Percentage difference of elimination diet parameters from baseline period between the groups starting with elimination diet and starting with provocation diet

*Patients starting with elimination diet; **patients starting with provocation diet; † percentage difference from baseline period; ‡(25%; 75%) percentiles.
NS, not significant in Mann-Whitney test with 95% confidence interval.
We also calculated if the patient showed at least a 30% reduction and at least a 50% reduction for attack count and number of headache days using elimination diet compared to provocation diet and to the baseline period. In comparison between elimination and baseline phases, for parameters of the number of headache days and attack count, reduction was ≥30% in 16 (53%) and 16 (53%) patients, respectively, and reduction was ≥50% in 7 (23%) and 6 (20%) patients, respectively. In comparison between elimination and provocation phases, for the number of headache days and attack count, reduction was ≥30% in 15 (50%) and 12 (40%) patients, respectively, and reduction was ≥50% in 6 (20%) and 4 (13%) patients, respectively.
Discussion
The concept that food may trigger some symptoms creates an increasing pressure on the healthcare system to investigate possible causal relationships between food intake and specific diseases. In the case of migraine, it seems evident that food is not the primary cause but, via different mechanisms, is able to induce or aggravate migraine attacks. In some individuals, the consumption of chocolate or red wine is enough to provoke an attack; whereas, in others, a combination of food is required, even sometimes with food which has never been related to migraine for other migraineurs. However, it is neither easy nor very useful to organise routine diet according to robust protocols for many patients (3,30). All this indicates that there is a need for an individualised approach to diet to relieve migraine.
A recent study addressed a relationship between IgG antibodies against food antigens and systemic inflammation measured by C-reactive protein (CRP) in obese juvenile patients (18). Obesity was also shown as an important risk factor in the development of chronic daily headache and chronic migraine (33,34). The therapeutic potential of dietary elimination on the basis of the presence of IgG antibodies against food in patients with IBS has been investigated. Patients were randomised to receive either a diet excluding all foods to which they had raised IgG antibodies or a sham diet excluding the same number of foods but not those to which they had antibodies (19). The true diet resulted in a statistically significant reduction in symptom scores compared to the sham diet and the authors concluded that this technique is worthy of further clinical research in IBS.
There is growing evidence that inflammation plays an important role in the pathogenesis of migraine (2). The calcitonin gene-related peptide (CGRP), and nitric oxide (NO) may participate in immune and inflammatory responses. Some patients report that certain foods only trigger migraine in conjunction with stress or extended physical exercise. Both conditions, recognised as triggers of migraine, cause the release of pro-inflammatory cytokines. In these cases, inflammation caused by food could create the pro-inflammatory milieu necessary for the induction of migraine by other triggers. If we focus on inflammation induced by food, a specific marker is needed. All IgG subclasses, except IgG4 lead to an inflammatory response when in contact with the respective antigen. Determination of specific IgG to a large number of foods is an ideal tool to detect individually suspected food and enables a modification of nutritional habits in order to prevent chronic inflammation and onset of migraine in sensitised patients. Susceptibility to other triggers such as histamine, caused by impaired detoxification by low activity of di-amino-oxidase, may play an additional role and could be considered in the proposed diet.
A recent study from Mexico investigated 56 patients with recurrent attacks of migraine (at least once a month) and 56 control subjects without migraine and measured their allergen-specific IgG against 108 food allergens by enzyme immunoassay (24). The authors reported that there was a statistically significant difference in the number of positive results for IgG food allergens between patients and controls and the elimination diet successfully controls the migraine without need of medication. As distinct from this study, we used a randomised, cross-over design with clear definition of diagnostic and follow-up criteria and study set-up. We used a baseline period and provocative diet periods to compare elimination diet period of the same individuals as their own controls instead of using other healthy volunteers.
Our data confirm the importance of determination of specific IgG antibodies against food antigens for prevention and cure of food-induced migraine attacks, leading to lower drug consumption, fewer adverse drug reactions and fewer days with migraine.
Conclusions
Diet restriction based on IgG antibodies might be an effective strategy in reducing the frequency of migraine attacks and could be implemented for therapy-resistant patient. However, because of the small sample size of this study, caution is required while translating these results into daily practice. Further research is also needed to determine the mechanism of IgG positive, food-induced migraine and its relation to other triggers.
Footnotes
Acknowledgements
Kadriye Alpay and Mustafa Ertaş contributed equally to the study. Mustafa Ertaş conducted the statistical analyses; he is a lecturer in biostatistics.