
Abstract
The objective of the present study was to investigate clinical and magnetic resonance imaging (MRI) features of idiopathic trigeminal neuropathy with transient MR abnormalities mimicking a neoplasm (ITNmn). We retrospectively evaluated clinical and MRI features in two cases of ITNmn seen in our institution in comparison with those of previously reported five cases. The most common symptom was altered facial sensation and numbness limited to one or more trigeminal nerve divisions (100%). ITNmn commonly affected not only the second and third divisions (86% and 57%, respectively) but also the first division (71%). The most common findings on MRI were enlargement and gadolinium enhancement of the trigeminal nerve, which were similar to those seen in neoplasms (100%). The abnormalities spontaneously regressed in all five evaluable cases. ITNmn should be added in the differential diagnosis of non-specific mass-like lesions in trigeminal neuropathy and be observed carefully without surgical treatment.
Introduction
Idiopathic trigeminal neuropathy (ITN) is a disorder with no identifiable underlying disease. The most common complaint from patients is facial numbness limited to one or more trigeminal nerve divisions (usually second and/or third) (1,2). There are some cases of ITN with abnormalities on magnetic resonance imaging (MRI). In addition to diffuse contrast enhancement of the trigeminal nerve, which is similarly seen in Bell’s palsy (4,5), transient enlargement of the nerve, usually seen in neoplasms (especially trigeminal neurinoma), has been reported as MRI findings (6–9). Such transient abnormalities may pose management problems for neurologists and neurosurgeons with respect to the differential diagnosis, because ITN and neoplasms existing around the trigeminal nerve request completely different management strategies. In this article, we present two cases of ITN with transient abnormalities mimicking a neoplasm (ITNmn) and review the radiological and clinical features of five reported cases.
Subjects and methods
In this study we have attempted to characterise clinical and MRI findings of ITNmn from the data source at our hospital and in the literature. The privacy of patients was completely protected. An approval by an institutional review board was not necessary for this type of study. Between January 2004 and October 2009, two patients were diagnosed with ITNmn at our institution. Their medical records were reviewed and MRI findings were evaluated. We also searched the PubMed database (<http://www.ncbi.nlm.nih.gov/entrez/query.fcgi>) using various combinations of key words like trigeminal neuropathy, transient, MRI and neoplasm. We found five patients from four case reports on ITNmn published between 1996 and 2009. We reviewed their patient characteristics, neurological findings and clinical course, and evaluated MRI signal intensity, contrast enhancement, location, morphology and sequential change.
Results
Case report 1
A 67-year-old woman with a past history of hyperlipidaemia developed left cheek numbness and mild left teeth pain 18 days before admission. The symptom of tingling and numbness with non-paroxysmal onset was different from that of typical trigeminal neuralgia. The pain gradually extended to the left maxillary region, lip and tongue. Eleven days after the onset, neurological examination revealed impairment of the sensation of touch, pain and temperature in the territory of the second and third divisions of the left trigeminal nerve and wasting of the left masseter muscle. There was no evidence of infectious disease and she had no rash and no upper respiratory and gastrointestinal symptoms. Other neurological examinations including the corneal reflex were normal. Routine blood chemistry results including markers of autoimmune diseases (anti-SS-A, anti-SS-B, PRS-ANCA, MPO-ANCA and rheumatoid factor). ACE and cerebrospinal fluid (CSF) studies were normal. Serum-soluble interleukin-2 receptor (803 U/ml: normal range, 220–530 U/ml) and neuron-specific enolase (12 ng/ml: normal range, <10 ng/ml) were slightly elevated, but there were no findings of malignancy on computed tomography (CT) from the chest to pelvis and gallium-67 whole-body scintigraphy. A cranial MRI obtained 18 days after the onset revealed a mass in the left Meckel cave (Figure 1). The mass extended to the masticator space through the foramen ovale (Figure 1B). The mass was iso-intense to the grey matter on T1-weighted image (T1WI), T2-weighted image (T2WI) and balanced fast-field-echo sequence and showed homogeneous contrast enhancement after gadolinium injection. These findings were interpreted to indicate a neoplasm such as trigeminal neurinoma. Biopsy was postponed because of the difficulty related to its location and improvement of her symptom by carbamazepine alone. Repeat MRIs obtained 36 days and 71 days after first MRI revealed chronological improvement of the enlargement (Figure 1C,D); finally, abnormal findings totally disappeared. Her symptoms slowly improved; 1 year later, only the numbness of the second division persisted. There has been no evidence of recurrence for 2 years and 4 months.
A 67-year-old woman with left trigeminal abnormality (case report 1). There is a mass-like lesion in the left Meckel cave (white arrows). It shows signal intensity iso-intense to the grey matter on balanced fast-field-echo sequence (repetition time [TR] = 6.9 ms, echo time [TE] = 3.4 ms, slice thickness [Thk] = 1.4 mm, field of view [FOV] = 150 mm) (A) and homogeneous enhancement on fat suppression 3-D T1-weighted image (TR = 33.9 ms, TE = 4.6 ms, Thk = 1.4 mm, FOV = 150 mm) after contrast media (B). It extends to the masticator space through the foramen ovale. Repeat 3-D T2-weighted image (TR = 1500 ms, TE = 250 ms, Thk = 1.4 mm, FOV = 150 mm) on 36 days (C) and 71 days (D) after first MRI show chronological regression of the left trigeminal nerve abnormality.
Case report 2
A 74-year-old woman presented with numbness and pain of the right middle and lower face. The onset was gradual and began 2 months before. Her past histories were pulmonary tuberculosis at about 14 years of age and pelvic herpes zoster at 64 years. There was no evidence of recent infectious disease and she had no rash and no upper respiratory and gastrointestinal symptoms. Neurological examination revealed impaired sensations to light touch and pinprick in the territories of the second and third divisions of the right trigeminal nerve, right ptosis and diplopia on superior gaze. Other neurological examinations including the motor function of the trigeminal nerve were normal. Blood chemistry data including markers of autoimmune disease (anti-SS-A, anti-SS-B, PRS-ANCA, MPO-ANCA and rheumatoid factor), and ACE and CSF data were normal except for moderate elevation of serum carcino-embryonic antigen (11.2 ng/ml: normal range, <5 ng/ml). CT from the chest to pelvis revealed no malignant neoplasms. A cranial MRI obtained 2 months after the onset revealed a mass in the right Meckel cave. The mass was located at the gasserian ganglion level and extended to the masticator space through the foramen ovale (Figure 2A). Its signal intensity and enhancement were similar to those of case 1. With a suspicion of trigeminal neurinoma, surgical resection was planned and a second MRI was performed 30 days after the first MRI for re-evaluation before operation. However, the second MRI revealed spontaneous regression, and an inflammatory change was suggested. Her diplopia and ptosis gradually improved without any medication but numbness deteriorated. Repeat MRI obtained 110 days after the second MRI revealed complete resolution of the abnormalities (Figure 2B). Her symptoms did not deteriorate for 9 months.
A 74-year-old woman with right trigeminal abnormality (case report 2). There is a mass-like lesion from the right Meckel cave to the masticator space (white arrows). It shows homogeneous enhancement on fat suppression T1-weighted image (TR = 510 ms, TE = 12 ms, Thk = 2 mm, FOV = 200 mm) after gadolinium injection at 105 days from onset (A). Its enhancement and enlargement spontaneously regressed after 215 days from onset (B).
Summary of clinical and radiological features
Patient characteristics of idiopathic trigeminal neuropathy mimicking a neoplasm

M, male; F, female.
Clinical features
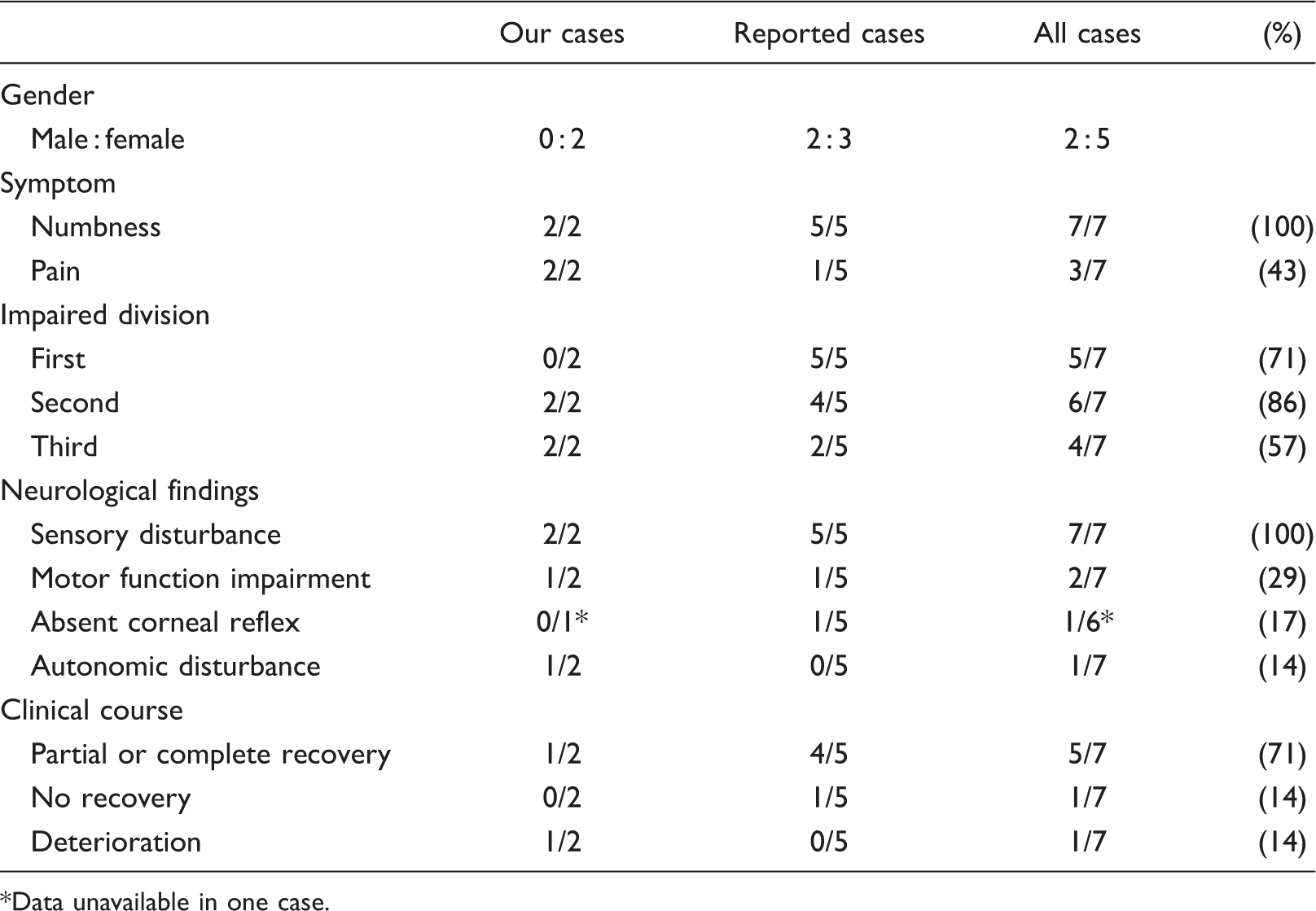
Data unavailable in one case.
MRI features
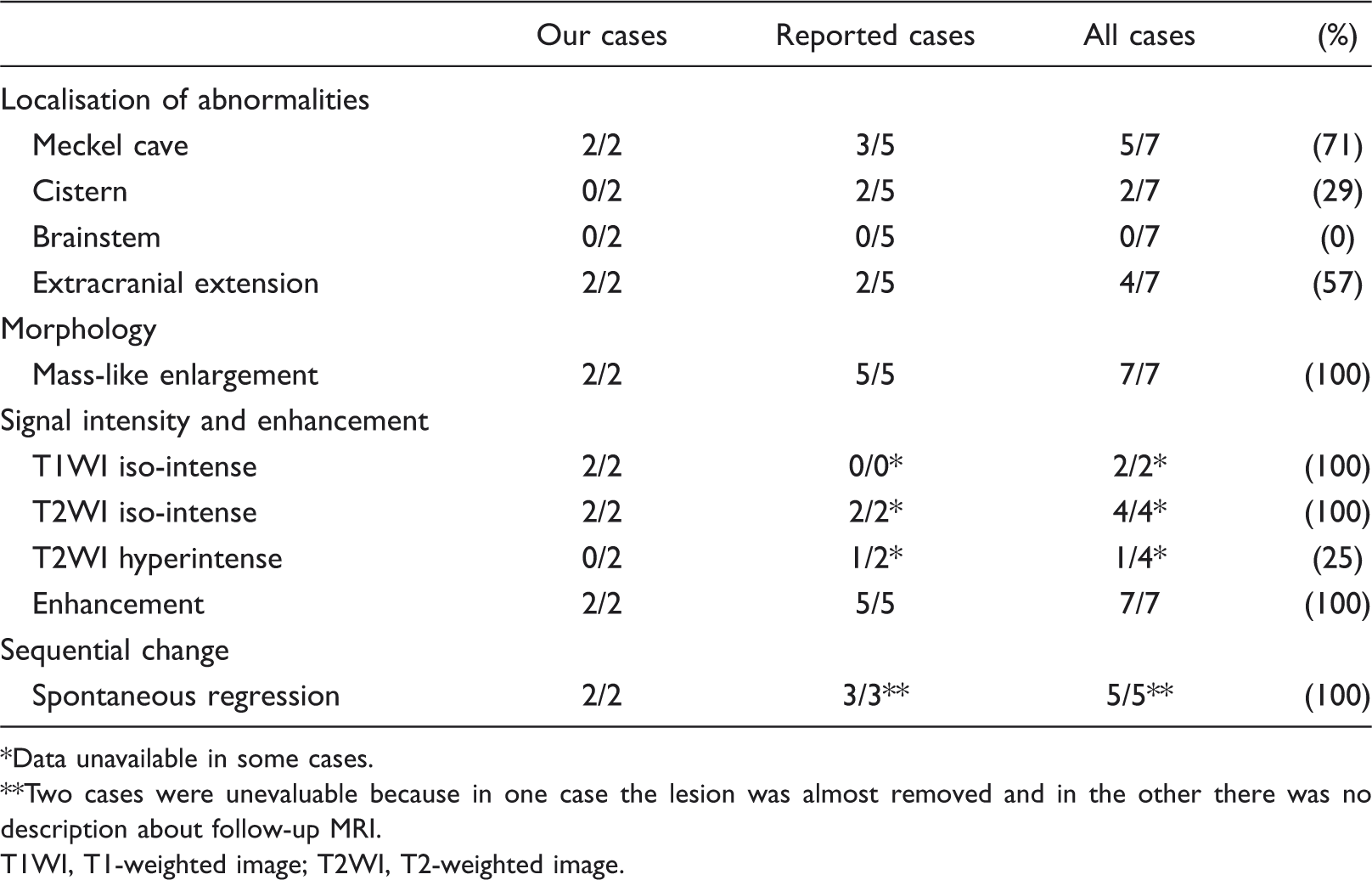
Data unavailable in some cases.
Two cases were unevaluable because in one case the lesion was almost removed and in the other there was no description about follow-up MRI.
T1WI, T1-weighted image; T2WI, T2-weighted image.
Discussion
Pathophysiology and histopathology
Trigeminal neuropathy has been described in association with various disorders including neoplasms of the cerebellopontine angle and skull base, trauma, demyelinating diseases, connective tissue disorders such as systemic sclerosis and Sjögren syndrome, sarcoidosis, and local amyloidosis (3,4,10–15). The cases with unclear underlying pathogenic mechanism are diagnosed as ITN. The aetiology of such conditions is unknown. Some authors proposed viral inflammation of the nerve root similar to that observed in Bell's palsy (2); others have implicated vasculitis secondary to the auto-immune disease (3). In seven cases of ITNmn including our two cases, however, there was no evidence indicating viral infection or autoimmune disease and they had no relevant past histories. Thus, aetiology could be identified in none of the cases.
Histopathologically, chronic inflammation composed of lymphocytes was observed in ITNmn (7–9). The pathogenesis of enlargement and enhancement was not discussed in previous reports (6–9). Pseudotumoural enlargement has been reported in other cranial nerves including the optic, facial, glossopharyngeal and vagus nerves (16–20). In idiopathic and herpetic facial nerve palsy, histopathological examination revealed inflammatory infiltrates of lymphocytes and plasma cells and intraneural oedema in the neuronal nerve sheaths (16,21,22). Adachi (18) proposed that these inflammatory cells and oedema were most likely to cause the swelling of the infected cranial nerves in the varicella zoster virus neuropathy. For pseudotumoural hypertrophic facial nerve neuritis, Zanoletti et al. (20) hypothesised that re-activation of the infection and chronic inflammatory changes would produce an accumulation of inflammatory cells, fibroblasts and macrophages with a localized peri- and intraneural enlargement. Considering these cases of neuritis, it may not be illogical to assume that inflammatory changes can cause the enhancement and enlargement of the trigeminal nerve. However, it is necessary to evaluate further the histopathology of ITNmn to prove this hypothesis.
Clinical and MRI features
Similar to ITN, the most common symptom of ITNmn was altered facial sensation and numbness limited to one or more trigeminal nerve divisions. Although the first division was uncommonly affected in ITN (1,2), ITNmn commonly affected not only the second and third but also the first division (86%, 57% and 71%, respectively). The frequency of pain is variable in ITN (1,2), and the pain of both ITN and ITMmn is different from that of typical trigeminal neuralgia. Although trigeminal motor nerve impairment is extremely rare in ITN (1,2), motor function was impaired in two cases of ITNmn (29%). The prognosis of ITN is diverse. In the largest series, most patient did not recover (1); however, in other 10 cases, most recovered partially or completely (2). In ITNmn, symptoms also resolved partially or completely in 71% of cases.
The most common MRI feature of ITNmn was enlargement and gadolinium enhancement of the trigeminal nerve resembling a neoplasm (100%). Although information on signal intensity was scarce in previous reports (6–8), Ahn et al. (9) reported that two lesions were iso-intense to the grey matter, and one showed central high signal intensity similar to necrosis on T2WI. In evaluable cases, the signal intensity was non-specifically iso-intense to the grey matter on T1WI and T2WI.
Many lesions occur around the trigeminal nerve. ITNmn was often misdiagnosed as trigeminal neurinoma before surgery (7–9). Compared to ITNmn, trigeminal neurinoma often accompanied motor function impairment (29–86% vs 29% in ITNmn), absent corneal reflex (79% vs 17%) and impairment of the other cranial nerves (22–43% vs 14%) (23–25). Particularly, lower cranial nerves were occasionally impaired in neurinoma, whereas there have been no such reports for ITMmn. Myxoid cystic degeneration and haemorrhage were also notable findings in neurinoma (10,23,25). However, appearance of these findings depends on tumour size and location (10), so it seems difficult to distinguish between ITNmn and small neurinoma without mass effect. Not only neurinoma but also other tumours including malignant lymphoma, meningioma, skull base tumour and non-tumorous lesions including sarcoidosis, amyloidosis and multiple sclerosis show mass-like enlargement of the trigeminal nerve (10–15). These many differential diagnoses and non-specific MRI findings of ITNmn make it difficult to distinguish ITNmn from other lesions especially neurinoma before surgery (7–9). However, spontaneous regression should be a noteworthy finding, although other lesions such as malignant lymphoma may occasionally show spontaneous regression (26).
Our review is limited by the lack of pathological diagnosis in three cases including our two. There has been no evidence of recurrence for 9 months and more than 2 years in our two cases. Rorick et al. (6) reported a case which did not show recurrence after 4 months from onset. On the other hand, most malignant lymphomas recurred within 2 months (26). Considering the short duration until recurrence of lymphoma, it is unlikely that our cases were malignant lymphoma.
Conclusions
ITNmn should be added in the differential diagnosis of non-specific mass-like lesions in trigeminal neuropathy. Although biopsy is generally recommended for a trigeminal nerve mass with no clear aetiology, careful observation including MRI follow-up at intervals of 4–8 weeks may be an alternative strategy in patients presenting with stable trigeminal neuropathy and a trigeminal mass-like lesion without malignant features, unless clinical progression beyond the trigeminal sensory symptoms is documented.