
Abstract
Essential tremor (ET) and migraine headache are considered comorbid diseases on the basis of uncontrolled studies. We investigated the frequency of migraine in patients with ET by enrolling 110 patients with ET and 110 age- and sex-matched healthy controls in a case-control study. We found no significant differences in the frequency of lifetime and current migraine between patients and controls, even in patients stratified for age. Tremor had similar clinical features in patients with ET with and without migraine except that females predominated in patients with ET and migraine. Migraine also had similar characteristics in both patients with ET and migraine and in controls with migraine. Our study excludes a comorbid association between ET and migraine. When ET and migraine coexist their clinical phenotype and evolution remain almost unchanged.
Introduction
Studies performed in the early 1990s disclosed a bidirectional association between ET and migraine, suggesting that the two diseases share some pathophysiological mechanisms. In a cross-sectional study, Biary et al. reported that one in three patients with ET, mainly younger patients, have migraine, whereas one out of six migraineurs have ET (1). In a study on patients with hereditary ET, Bain et al. reported that 26% suffered from classic migraine and that classic migraine and ET are inherited together (2). Hence, ET has hitherto been considered comorbid with migraine (3). All these studies based their conclusions, however, on data obtained without comparing patients’ features with those of age-matched control groups.
To find out more about the association between ET and migraine, we designed this case-control study to investigate the frequency of migraine in a large sample of consecutive outpatients with ET. To diagnose migraine we used the latest diagnostic criteria published by the International Headache Society (IHS) (4).
Patients and methods
A case-control study was conducted to compare the frequency of migraine in 110 patients with ET consecutively recruited from 1 June to 31 December 2008 at the Department of Neurosciences, Sapienza University of Rome, and at the Department of Neurological, Motor and Sensorial Sciences (IRCCS) San Raffaele Pisana, Rome, and in 110 healthy controls paired for sex and age (±2 years), consecutively recruited in the same period from non-consanguineous relatives of outpatients attending our neurological units. All patients and controls signed informed consent after full disclosure of the purposes of the study.
All participants underwent a complete physical and neurological examination and were screened for concomitant diseases (including arterial hypertension, diabetes, liver and kidney insufficiency) and medications.
ET was diagnosed according to the Criteria of the Movement Disorder Society (5). Tremor was classified as resting, postural or kinetic. Severity of tremor was rated according to the Fahn-Tolosa-Marin Tremor Rating Scale (TRS) (6). Tremor in the arms, legs, head and voice was rated with a clinical scale ranging from 0 to 4 (0 = no tremor; 1 = mild [barely detectable or voice tremor only when anxious]; 2 = moderate [oscillations <2 cm or voice tremor most of the time]; 3 = severe [oscillations between 2 and 4 cm or constant voice tremor]; 4 = very severe [oscillations >4 cm or difficulties in understanding most words]). Tremor was also scored on a scale ranging from 0 to 4 during the execution of standard motor tasks (writing a sentence, drawing an Archimede spiral, drawing a parallel and sinusoidal line and pouring water from a full glass to an empty one) and during functional activities (speaking, drinking, eating, writing, body care, dressing, working, fine movements). Of the 110 patients enrolled, 43 (39%) were receiving medications for the treatment of tremor: 12 were receiving treatment with propranolol (mean dose 58.3 ± 49.3 mg), 12 with primidone (mean dose 276 ± 230 mg), 11 with clonazepam (mean dose 1.7 ± 1.4 mg), three with topiramate (mean dose 166.7 ± 57.7 mg), one with propranolol (40 mg) plus primidone (125 mg), and four with propranolol (80 mg) plus clonazepam (mean dose 0.98 ± 0.4 mg).
Migraine was diagnosed according to the IHS criteria (4). Patients with ET were asked to describe any change in the migraine course after the onset of ET or the beginning of therapy with propranolol or topiramate. Migraine improvement was defined as a reduction of >50% in the frequency of attacks.
Detailed information on ET (age at onset, site of onset, spread to other body sites) and migraine (current/lifetime, type, family history of migraine, disease duration, frequency and duration of attacks, location and intensity of pain) was obtained through structured questionnaires (7) in a face-to-face interview.
All variables are expressed as means ± SD. Chi-square test and paired t-test were used as appropriate to compare the frequency of lifetime and current migraine in case and control subjects and the clinical characteristics in subjects with or without migraine.
Results
The participation rate was 100% among case and control subjects. In the 110 patients with ET, the mean age at tremor onset was 52.2 ± 12.4 years and tremor duration was 16.2 ± 14.8 years. Tremor started in the upper limbs in 89 patients (81%), in the head in 13 (12%) and in the voice in eight (7%). In 68 patients (61.8%) tremor spread to other body parts. Mean tremor severity was 1.64 ± 0.84 in the upper limbs, 0.70 ± 0.87 in the head, and 0.48 ± 0.82 in the voice. Of the 110 patients with ET, 52 (47.3%) had a family history of tremor. There were no significant differences in demographic characteristics, tremor severity and duration and concomitant diseases between ET patients receiving medications for ET and those who did not.
The 110 patients with ET and the 110 healthy control subjects had similar demographic features (men/women: 49/61 vs. 49/61; mean age: 70 ± 11 years vs. 69 ± 12 years) and frequency of concomitant diseases. Lifetime migraine was reported by 28/110 (25.4%) patients with ET and 24/110 (21.8%) control subjects (p = 0.53). Case histories mentioned current migraine in 11/110 (10%) case patients and in 14/110 (12.7%) of the controls (p = .53). No difference was found in the frequency of lifetime and current migraine between patients and controls, even when patients’ data were stratified for age (data not shown).
Characteristics of migraine in subjects with essential tremor and in healthy controls
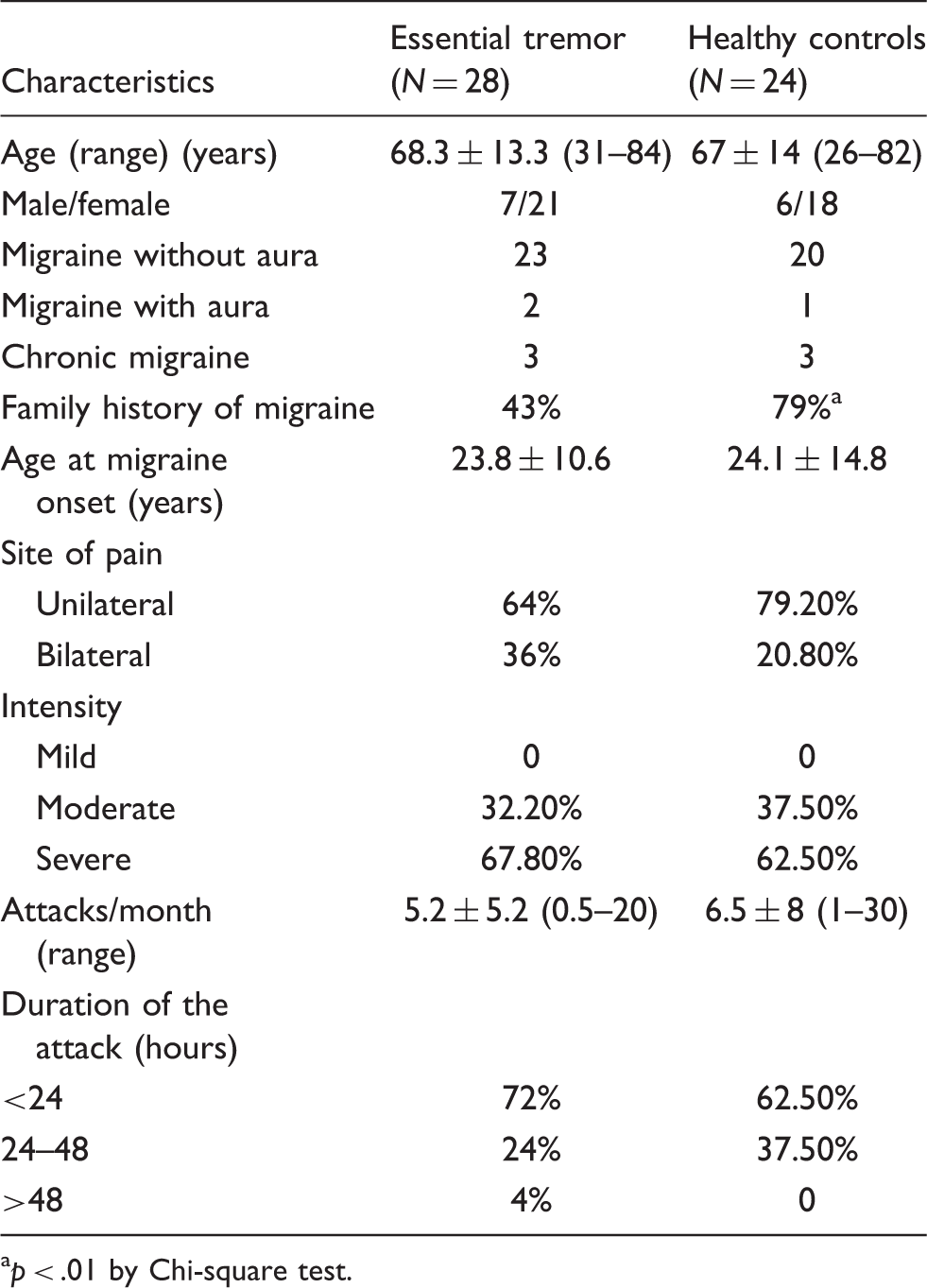
p < .01 by Chi-square test.
Characteristics of tremor in patients with essential tremor with and without migraine

p < .01 by Chi-square test.
p < .05 by paired t-test.
Discussion
In this case-control study enrolling a large population of patients with ET and healthy control subjects, we unexpectedly found a similar frequency of lifetime or current migraine in patients with ET and controls. When migraine and ET coexisted, neither condition influenced the other. The very small number of ET migraineurs (five patients) treated with propranolol or topiramate precludes us from speculating on why these drugs had no apparent action on migraine.
Overall, our results argue against prior uncontrolled studies suggesting an association between migraine and ET (1,2). Given the high prevalence of both conditions (8,9), ET and migraine may coexist merely by chance. Supporting our view, Duval et al. (2006) (10) found no differences in the characteristics of tremor in migraineurs and healthy controls.
Because we found no association between ET and migraine, our study provides no information on whether the movement disorder ET and migraine headache arise from similar pathophysiological mechanisms. Given the possible role of the extrapyramidal system in the processing and modulation of pain and in nociceptive sensorimotor integration, migraine has been widely investigated also in other movement disorders (11). In comparison to healthy controls, migraine prevalence has been reported to be reduced in Parkinson's disease (12), similar in cranial and cervical dystonia (7) and increased in Sydenham’s chorea (13) and in Tourette’s syndrome (14).
This study has several strengths: it enrolled a large number of patients, used a case-control design, assessed the possible influence of ET on migraine and vice versa, and used the latest IHS diagnostic criteria for migraine. Nevertheless, our study has limitations. First, because we recruited patients with ET in a tertiary-referral centre, this is not a population-based study. The demographic and clinical features of our case series were nonetheless similar to those of the general population of patients with ET. Second, we cannot rule out possible artefacts due to recall bias. Third, we cannot exclude in our ET sample some potential risk factors for migraine such as middle-low social level, self-reported poor health or both. Finally, the retrospective assessment made it difficult to establish whether the onset of ET altered the course of migraine.
In summary, our study provides definitive information excluding a comorbid association between migraine and ET. When migraine headache and ET coexist, their clinical phenotype and evolution remain substantially unchanged.