
Abstract
To advance scientific knowledge on workplace compassion, we need to know ‘where we are now’ to identify ‘where to go next’. This article provides a systematic review of workplace compassion research, spanning almost 30 years and 1433 articles across the social sciences. We employ bibliometric techniques to (1) identify and map the literature’s intellectual foundations with a co-citation map revealing 595 key journals, (2) provide an interactive topic map showing 267 key research topics, (3) reveal the most frequent, trending, and most-cited article topics, and (4) provide an empirically derived taxonomy of two primary topic clusters: Compassionate Labour (e.g. research in healthcare settings, where compassion is relevant to the work being done), and Mental Health (e.g. research on burnout, compassion fatigue/empathic distress, compassion satisfaction, stress, interventions). We review key research themes in these clusters and identify promising future research directions to advance the field.
1. Introduction
Compassion has been defined as ‘being moved by another’s suffering and wanting to help’ (Lazarus, 1991: 289) and has a long tradition as a topic of interest in religion, philosophy, and sociology. In the management literature, research on workplace compassion has a relatively short history (Frost et al., 2006; Lilius et al., 2008). However, there is growing recognition that workplaces are emotionally charged arenas (Fineman, 2000) and that encountering suffering is common in organisational life – be it the spillover of suffering from life to work (e.g. trauma, loss, or illness) or suffering that occurs at work (e.g. difficult and/or stressful work or working conditions, working with clients or patients who are suffering, workplace experiences such as workplace conflict/bullying, or organisational change that dislocates employees [Lilius et al., 2008]). In recent decades, there has been increasing interest among scholars in investigating the predictors, consequences, and complexities of compassion as a response to suffering encountered at work.
For many employees, particularly frontline employees, the provision of compassion is (at least implicitly, if not explicitly) an important part of their job. For example, healthcare professionals’ compassion has been found to be critical for patient satisfaction (Vogus and McClelland, 2016). Employee compassion has also been linked to the quality of the customers’ experience in retail banking (Wasan, 2018), as well as corporate customers’ satisfaction (Andaleeb et al., 2016). The compassion that judges show in managing their courtrooms has even been linked to the instillation of public faith in the justice system (Levitt and Dunnavant, 2015).
However, jobs that involve managing or responding to other people’s suffering have been argued to take a substantial toll on mental health, which has been referred to in parts of the literature as ‘compassion fatigue’ (although researchers have argued that this phenomenon should be labelled ‘empathic distress fatigue’: Dowling, 2018; Sinclair et al., 2017). For example, nurses are at risk of compassion fatigue and secondary trauma (Lin et al., 2021) and lawyers exposed to traumatic material in their cases may experience both compassion for victims and suffer from that exposure (Weir et al., 2021). Compassion fatigue also impacts those who work with animals (e.g. veterinary personnel [Schlanser et al., 2021], those who work in animal shelters [Levitt and Gezinski, 2020] and in animal research facilities [Murray et al., 2020]). In recognition of this, numerous interventions have been developed with the aim of cultivating sustainable compassion towards oneself and others in a range of workplace contexts (see Kirby, 2017).
Because of the increasing recognition of the importance of compassion in the workplace, and its consequences for those who give and receive it, the social science literature on workplace compassion has grown dramatically over the last few decades (Figure 1). For example, our systematic search of social science scholarship finds that, in recent years, over 200 research articles are being published on this topic each year. Moreover, workplace compassion is being studied across a number of fields, including the fields of mental health/clinical psychology research, healthcare research, and organizational research (e.g. social psychology research, management research, and public administration research). In light of this breadth and volume of research, in this article, we aim to advance the field by providing a much-needed integrative overview of workplace compassion scholarship.
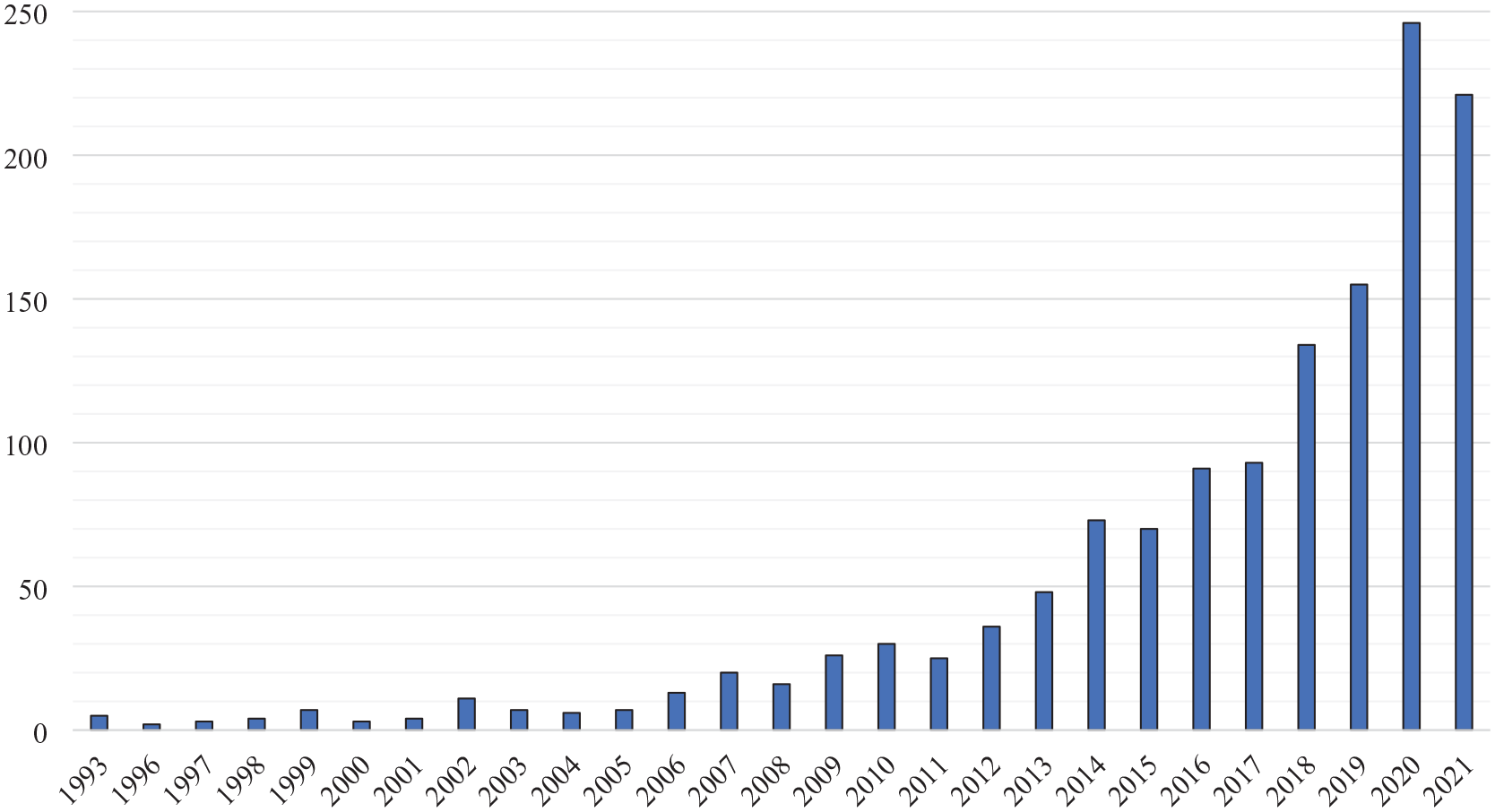
Number of social science research articles on workplace compassion per year.
Using bibliometric techniques, we offer a systematic analysis and review of this vast and rapidly growing literature. In doing so, this article makes a number of important contributions. First, to our knowledge, this article offers the most comprehensive analysis of workplace compassion research to date, covering almost 30 years of scholarship from across the social sciences. Unlike prior reviews (see Table 1) that have tended to focus on a subset of the workplace compassion literature from a more narrow topic or disciplinary perspective (e.g. Swami et al. [2021] review of self-compassion research; Sweileh’s [2020] review of compassion research in the healthcare sector), our review summarizes workplace compassion research from across the social sciences, covering 1433 articles. As such, we are able to provide an integrative overview of this large social science literature.
Prior reviews and meta-analyses of workplace compassion research.

Second, while there have been a number of insightful reviews of compassion research, they typically employ the traditional approach of authors describing the literature based on their intuitive impressions and schemas (see Table 1). As such, key topics, articles, and research themes in the literature may have been overlooked, and/or the intellectual structure of the field may have been misrepresented by prior reviews (Markoulli et al., 2017). In contrast, this article draws on bibliometric methods to systematically analyse and map the topic contents of articles, and identify the literature’s key empirical features and structure as the basis of our review. In doing so, we provide what we believe is the first systematic review of workplace compassion scholarship.
Third, we offer new, empirically grounded descriptive frameworks for describing the literature. This is accomplished by using bibliometric science mapping to rigorously analyse and map the literature’s disciplinary foundations as well as the literature’s topic contents (respectively), and by using systematic article coding to identify 13 key subthemes in this literature which we discuss in our review (Strauss and Corbin, 1990). Such frameworks have been described as an important type of conceptual contribution for advancing a field (Klein and Potosky, 2019).
In providing a highly comprehensive and systematic review of workplace compassion research across the social sciences, we aim to provide an overview of this broad literature, integrative framework for understanding the field’s contents, and offer a detailed, interactive topic map that allows researchers to explore its topic contents. That is, enabling researchers and practitioner to ‘see the forests’ (in terms of what the major topic clusters are) and ‘the trees’ (in terms of the specific topics in this literature, how closely specific topics are associated with one another within the literature, the number of articles on each topic, the ‘trendingness’ of each topic, citation rates associated with articles on each topic, and the degree of association between particular topics), as well as ‘the groves’ by reviewing key themes in the articles associated with the major topic clusters within this literature.
We believe that the view of the literature provided by this review, which is both broad and detailed, is an especially valuable contribution as it can provide a foundation for future scholarship. For example, our interactive topic map allows scholars to more easily see the topics that are (and are not) studied in workplace compassion research across the social sciences. Thus, scholars can more easily detect what is ‘missing’ from workplace compassion research as a whole as topics for future scholarship. Moreover, the topic map reveals which topics in workplace compassion scholarship tend to be studied together (and which topics are not) as indicated by the distance between topics on the map. Thus, the topic map can help researchers to identify topics that may have yet to be examined together, and could be investigated together in future scholarship. Furthermore, our bibliometric topic map and systematic review of key themes in the literature can be used by scholars to identify opportunities to import insights across disciplinary divides. Such importation may yield helpful, practical, and generalisable insights for how organisations can support their employees. Thus, beyond providing a rigorous description of what currently exists in workplace compassion scholarship, our topic map of the literature, overview of key research themes across the social sciences, and review of the scholarship on those themes aims to provide scholars with a foundation for identifying new directions for workplace compassion scholarship.
As a final contribution, we aim to provide several novel critiques of the literature as a whole, and outline a research agenda to address those critiques. For example, our first critique, informed by our science mapping analysis, suggests that there are disciplinary divides in the literature (Figure 2), and highlights the challenge of overcoming siloing in workplace compassion research as a key issue that can be addressed by a stronger emphasis on integrative research efforts to build on insights from across disciplines. Second, based on our map of the topic contents of the field, the number of articles on each topic, the degree of association between topics, the ‘trendingness’ of specific topics (i.e. Figures 3 and 4), as well as our refined definition of compassion and integrative model of the literature, we highlight key topics for future study that have been underexplored. This includes a call for research examining workplace compassion in a wider range of work contexts, occupations, professions, and sectors, and particularly the need for research examining workplace compassion dynamics among lower status employees and employees in stigmatised roles that are often overlooked and underrepresented in mainstream research.
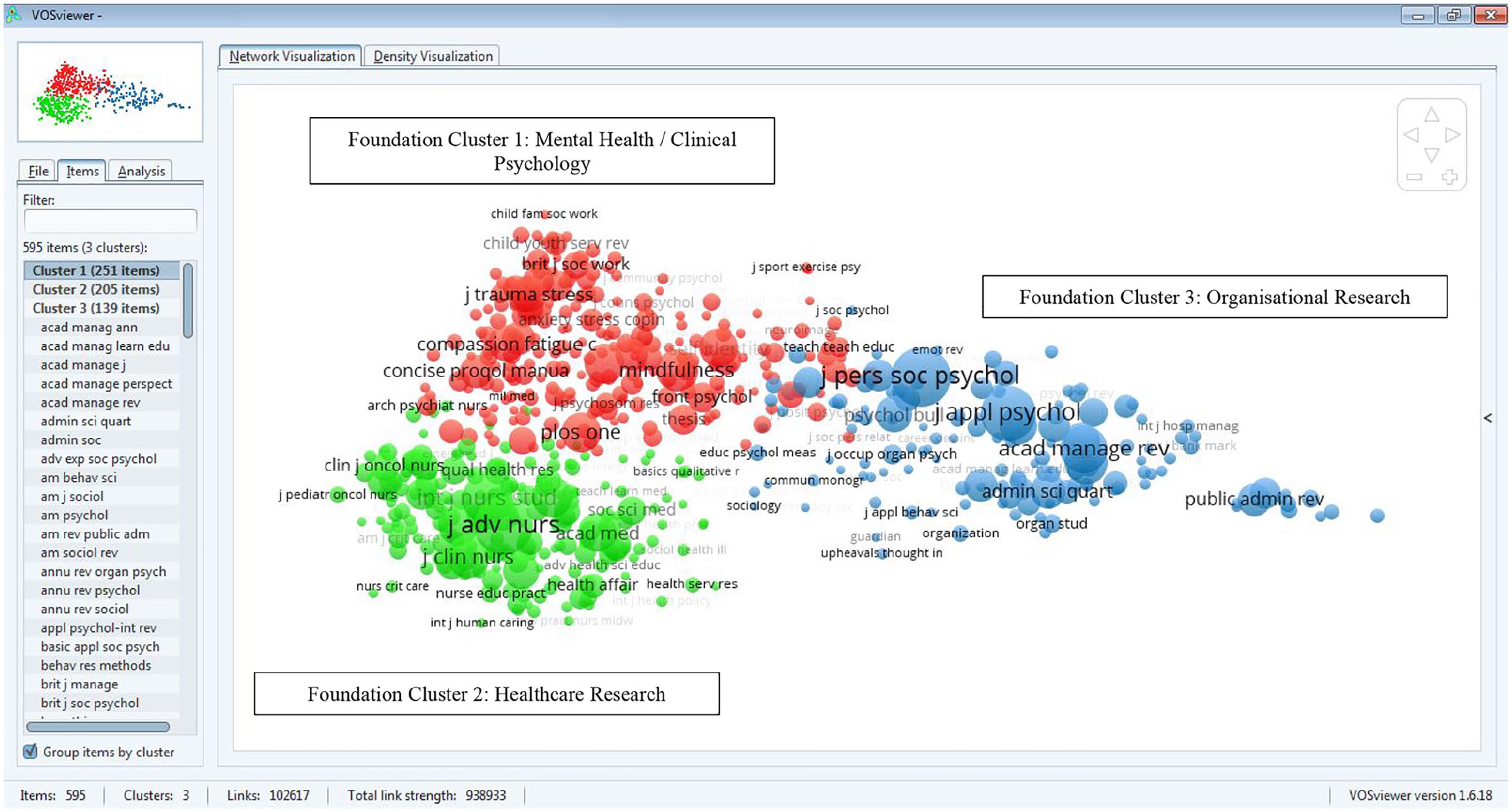
Foundations map: static image of the interactive co-citation map of journals cited by this literature.
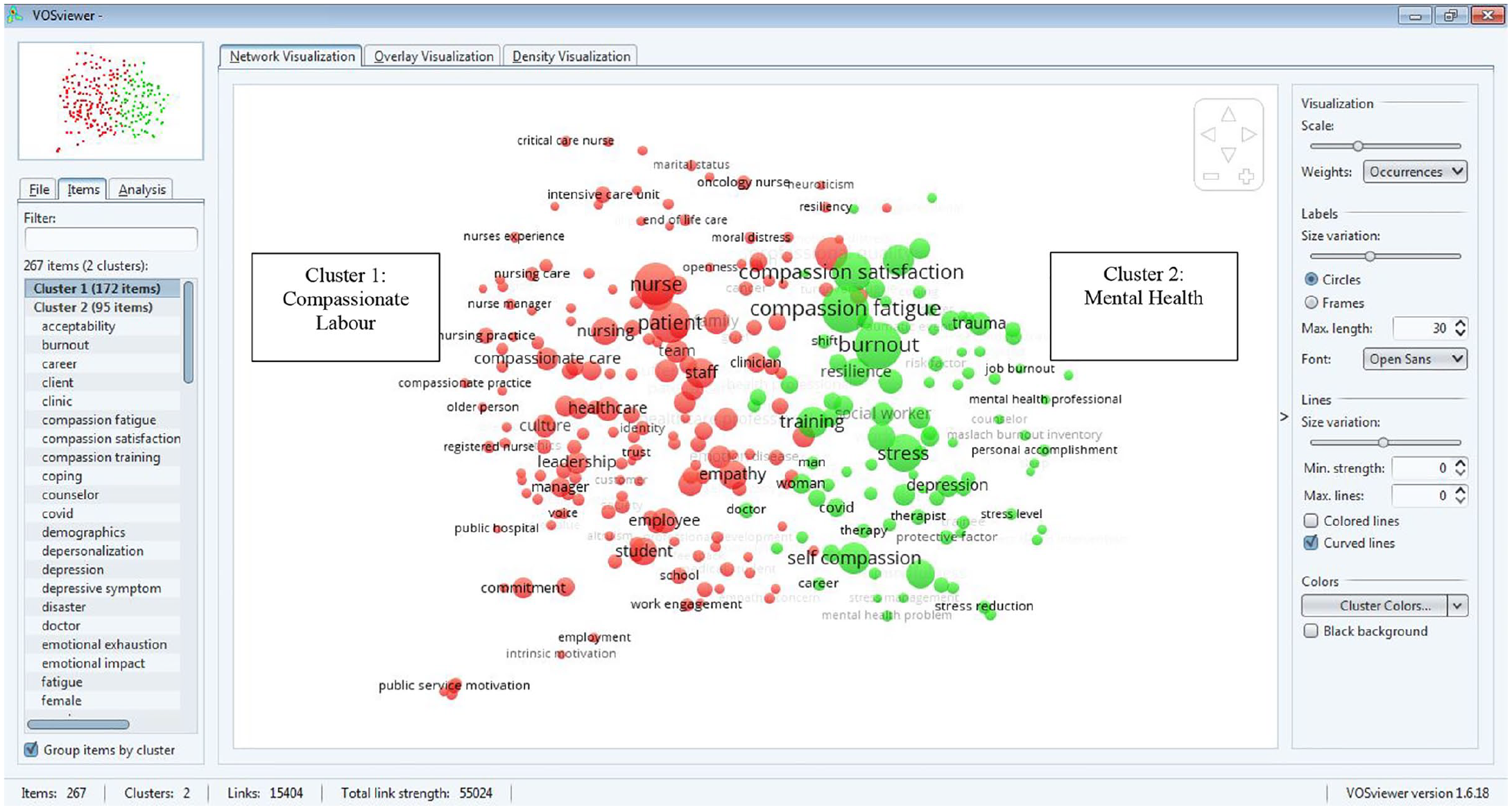
Topic map: static image of the workplace compassion topic map.
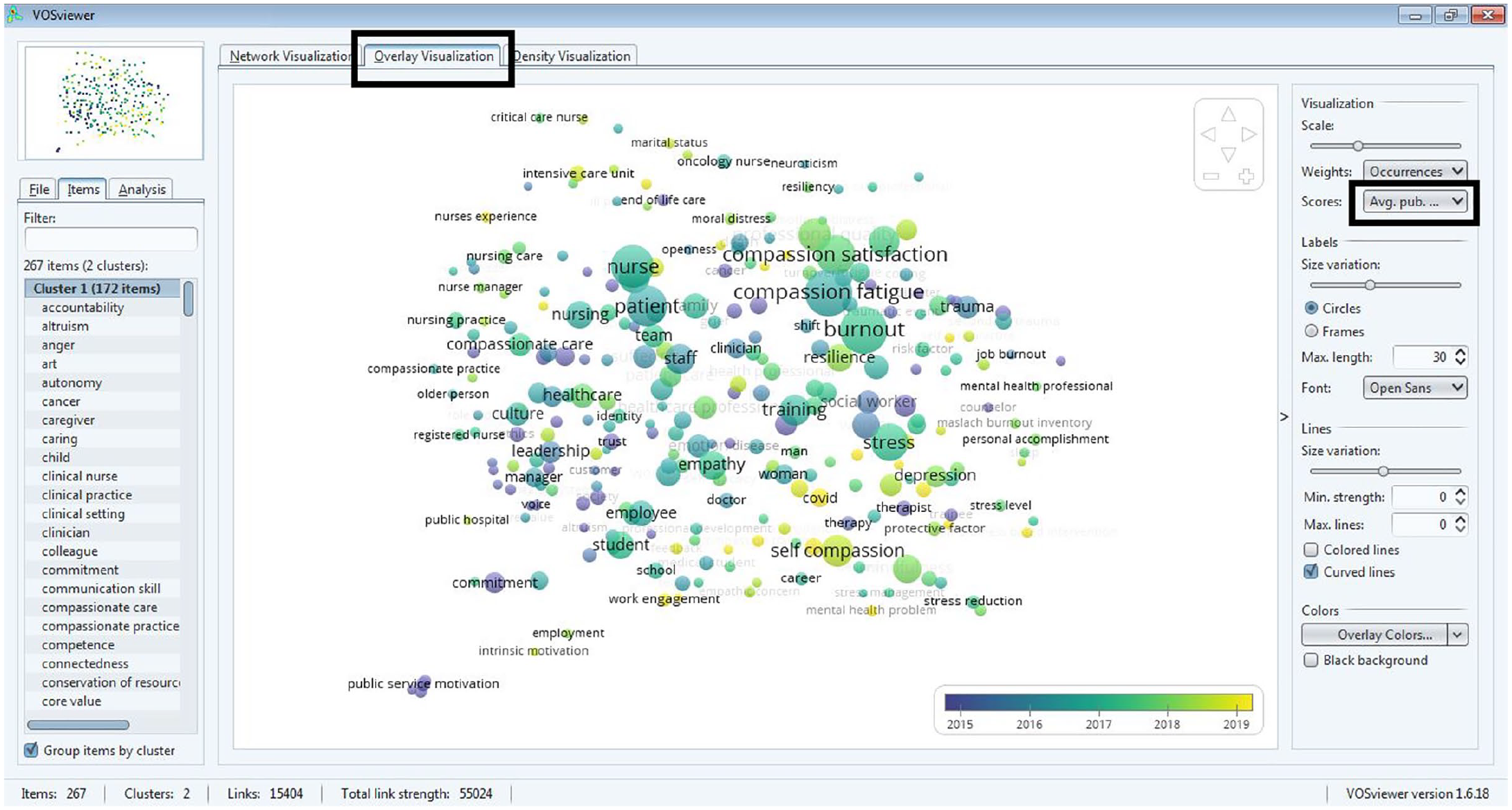
Static image of trending topic map.
2. Bibliometric analysis and review methods
To systematically analyse the intellectual structure of workplace compassion research across the social sciences, we employed VOSviewer’s bibliometric mapping techniques (Van Eck and Waltman, 2014). This allows us (1) to provide readers a visual, interactive map of the literature’s contents, and (2) to ground our review in the empirical features of the literature’s contents and structure. Reviews that employ VOSviewer are becoming increasingly common in management (e.g. Byington et al., 2019, 2021; Carpini et al., 2017; Lee et al., 2014; Markoulli et al., 2017; Verma and Gustafsson, 2020), and visual, bibliometric mapping techniques have been suggested to play an important role in taking stock of existing knowledge and guiding future scholarship (Linnenluecke et al., 2020).
2.1. Sample
To identify research on workplace compassion across the social sciences, we employed a five-step process. First, we collected all article records for journal “articles” and “review articles” in the Web of Science Social Science Citation Index (WoS-SSCI) with “compassion” + [“work*”, or “leader*”, or “employee*”, or “employer*, or “manage*, or “organisation*”, or “organisation*”] in their title, abstract, author generated keywords, or in the keywords generated for the article by the Web of Science based on the articles’ references. The article search period was 1993 (when electronic copies of articles began being systematically indexed in WoS) through December 25, 2021 (and including early indexed articles/reviews). Second, we collected all Management journal articles and review articles in the WoS-SSCI with “compassion” in their title, abstract, author generated keywords, or in the keywords generated for the article by the Web of Science. Third, we manually removed all duplicate articles. This yielded 3394 potentially relevant articles. Fourth, any article that did not mention “compassion*” in their title or abstract was removed from our database, as research article titles and abstracts typically reflect an academic article’s primary topic contents (Justeson and Katz, 1995). This yielded 2540 potentially relevant articles. Fifth, articles were manually reviewed to ensure their relevance for the proposed review.
In manually reviewing the articles to ensure relevance, the inclusion criteria used was: The article is ‘about’ compassion or very closely related constructs (e.g. ‘self-compassion’, ‘compassion fatigue’, ‘compassionate leadership’) in organisations. More specifically, the article (1) measures or discusses compassion as a focus of the article (i.e. not just mentions ‘compassion’), (2) in organisations, and (3) among adults. In making these assessments, the authors also considered bibliometric features of each article (i.e. whether and how many times the articles cited or was cited by any other article in the database of potentially relevant articles, contents of titles/abstracts, author keywords used). This coding process yielded a final database of 1433 relevant articles on workplace compassion. This process is displayed visually in Figure 5.
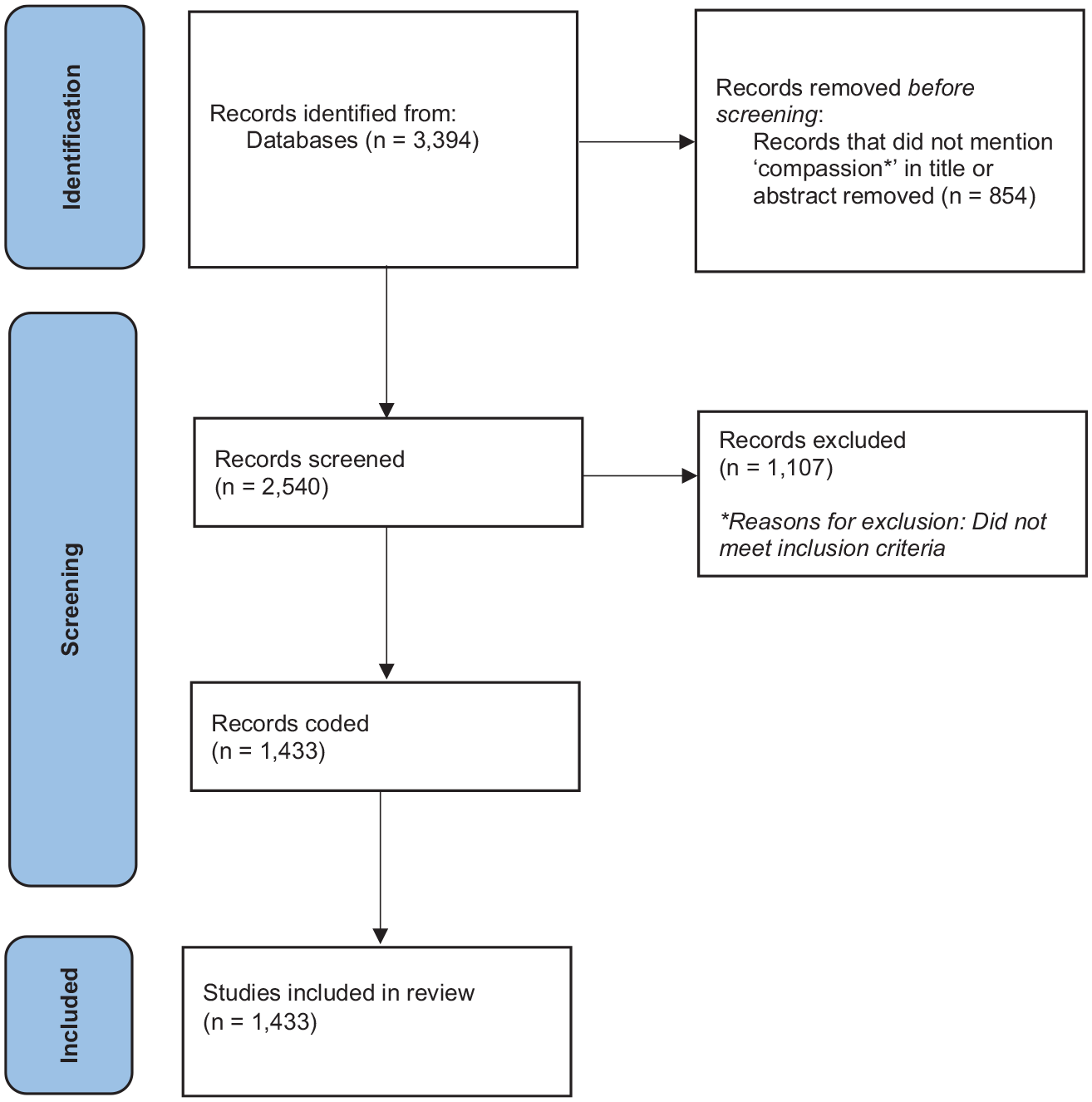
Prisma flow diagram of the studies included in the meta-analysis.
2.2. Analysis
For the ‘Foundations Map’ of key journals cited by this literature, we used VOSviewer co-citation analysis to identify key journals/sources cited by the corpus of 1433 articles on workplace compassion. We applied VOSviewer’s default minimum criteria for the number of times a source needed to be cited by the articles in our database for that journal to appear in the map (i.e. a journal needed to be cited at least 20 times by the 1433 articles in our database to be included in the map). This threshold helps ensure (1) that the journals reflected in the results were referenced at least to a moderate degree to be considered part of the ‘foundation’ that workplace compassion research builds on and (2) that the co-citation results of the map are robust (i.e. there were enough citations to the journals that their relations to one another could be reliably mapped. The application of this criteria resulted in 595 sources being identified and included in this co-citation analysis. Next, to ensure a reliable mapping solution, 100 random starts and 100 random seeds were used. To help ensure a robust clustering solution, we also used 100 random starts, 100 random seeds, and 100 iterations. A clustering resolution of 1 and a minimum cluster size of 50 yielded the three cluster solution revealed in Figure 2. In this map, the size of the circle behind each source indicates the number of times that source is cited in the 1433 article database. The colour of the node indicates which cluster a source most strongly ‘belongs’ to, and the distance between sources indicates the relative degree to which these journals appeared together in the reference lists of the 1433 articles in our database. The results of this analysis are discussed below and presented in an interactive journal map that readers can download by clicking this link: https://bit.ly/3qPNDtB. 1
For the topic map, VOSviewer was used to identify noun-phrases in the titles and abstracts of the 1433 articles. To ensure a reliable map of the associations between terms, and to ensure that a topic was a bonafide topic of research, we applied the default occurrence criteria of 10. That is, in order to be included in the map, a topic needed to appear in the title/abstract of at least 10 of the 1433 articles in our database. Candidate terms were manually reviewed to ensure that only meaningful noun phrases/topics of research were ultimately included in the map (e.g. concepts, actors, work contexts), and non-meaningful/non-substantive terms were excluded (e.g. ‘research’, ‘study’ ‘data’, ‘issue’, ‘importance’, ‘analysis’, ‘article’) to help ensure that the map reflects the substantive research topics in the literature. Highly generic terms (e.g. ‘compassion’, which appeared in the title and abstract of every article) were also excluded, as they can visually obscure the map and the substantive structure between topics. To help ensure reliable article counts, plural and singularized spellings of the same term and spelling variations (e.g. health care professional and healthcare professional) were merged, and abbreviations were converted and merged with the full spelling of a term (e.g. proqol professional quality of life scale). This yielded 267 research topics for inclusion in the topic map.
Once the article topics were systematically identified, the degree to which topics tend to co-occur in workplace compassion research title/abstracts (i.e. the association strength between topics) was then calculated in VOSviewer (van Eck and Waltman, 2009). The relations between topics were then spatially mapped, such that the distance between topics in the map indicates the degree to which they were likely to co-occur in the titles/abstracts of the 1433 articles in our sample (Waltman et al., 2010). We then applied VOSviewer cluster analysis to systematically and empirically identify distinct clusters of topics based on their pattern of co-occurrence. To help ensure a robust clustering solution, 100 random starts, 100 random seeds, and 100 iterations were used. A minimum cluster size threshold of 50 was applied to ensure that the topic clusters represented ‘major’ domains of the literature and were associated with a large enough number of articles to warrant review. A clustering resolution parameter of .90 was applied. This analysis yielded an empirically grounded taxonomy of major topic areas in workplace compassion research, based on the pattern of topic co-occurrence in our article database. The results of this analysis are discussed below, and are presented in an interactive topic map that readers can download by clicking this link: https://bit.ly/3ISPUu6 (see Note 1).
Once downloaded and opened, in the interactive topic map, readers can see the number of articles on each topic (indicated by topic node size, with the exact number of articles appearing when you hover your cursor over a node), the degree to which topics tend to co-occur in articles (as indicated by the spatial distance between topics in the map), as well as the cluster each topic is most strongly associated with (indicated by node colour). The ‘trendingness’ of each topic (i.e. average publication year of articles on each topic) can be seen by clicking the ‘Overlay Visualization’ tab, and then selecting ‘avg. pub. yr’. from the ‘Scores’: from the menu on the right-hand side of the map image (see Figure 4). The average number of citations articles on each topic receive (adjusting for publication year), can be seen by selecting ‘avg. norm. cites’ from that same drop-down menu on the right-hand menu.
3. Bibliometric results
3.1. Foundations map
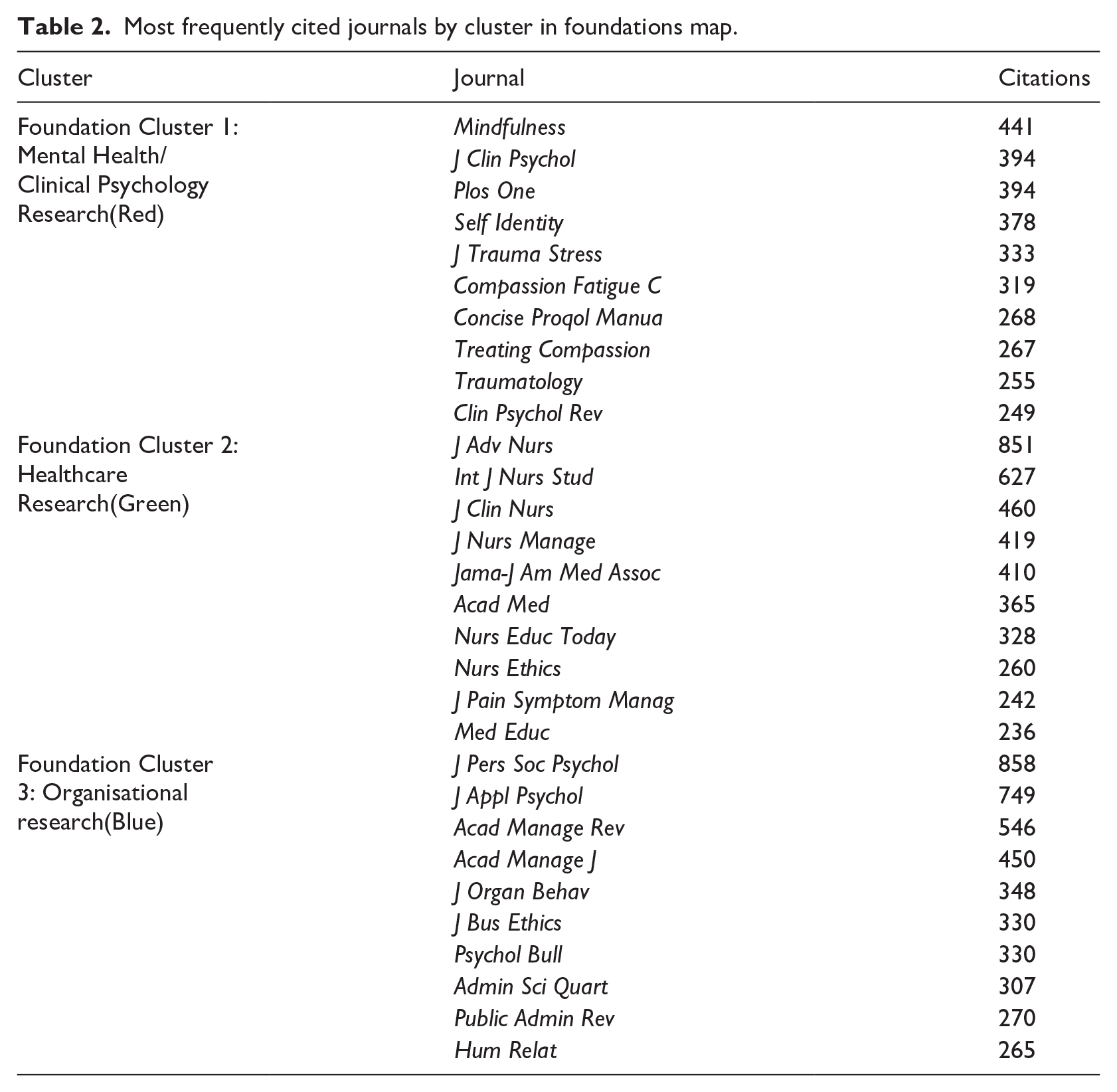
As shown in Figure 2, a co-citation analysis of the journals cited by the articles in our sample yields three clearly distinct and interpretable journal clusters that adhere to social science disciplinary areas. The three distinct journal clusters are (1) Mental Health/Clinical Psychology (Cluster 1, Red in the map, e.g. journals focused on trauma, stress, mindfulness research), (2) Healthcare research (Cluster 2, Green, e.g. journals focused on clinical and advanced nursing and healthcare), and (3) Organisational research (Cluster 3, Blue, e.g. journals on management, social psychology, and public administration). As such, this map reveals (1) evidence that workplace compassion is studied across multiple social science disciplines, and (2) clear evidence of disciplinary boundaries in the referencing patterns of workplace compassion articles. For example, the foundation map reveals that Organisational journals are far less likely to be cited alongside Healthcare or Mental Health/Clinical Psychology journals in the reference lists of workplace compassion research – as indicated by the distance between the Blue Organisational journal cluster and the other two clusters in the map. Similarly, Healthcare journals are much more likely to be cited alongside other Healthcare journals in workplace compassion research reference lists than Mental Health/Clinical Psychology sources, and vice versa, as indicated by their separate clusters in the map. This suggests that workplace compassion articles tend to build on/reference insights within their disciplines, rather than across the disciplines where workplace compassion is studied. Table 2 presents the most frequently cited journals in each cluster, and the different disciplinary orientations of each cluster can be seen by the names of the journals that belong to each cluster.
Most frequently cited journals by cluster in foundations map.
3.2. Topic map
The topic map analysis presents the first empirically derived taxonomy of workplace compassion scholarship in the social sciences, and reveals the key topic contents of this literature. As shown in Figure 3, the results of the analysis reveal two major topic clusters in workplace compassion scholarship. As described in the section above, readers can also explore an interactive version of the map to examine the intellectual structure of the literature in detail (e.g. the specific topics associated with each cluster, the degree of co-occurrence of topics in articles, the number of articles on each topic, the rate of citations associated with articles on each topic, the ‘trendingness’ of each topic). Given the topics and articles associated with each cluster, we labelled the two topic clusters: (1) Compassionate Labour research and (2) Mental Health research.
The Compassionate Labour topic cluster (Topic Cluster 1, red, Figure 3) contains 172 article topics. The topics and articles associated with this cluster predominantly focus on compassion as it occurs in workplace contexts (e.g. research in healthcare settings, where compassion is relevant to the work being done). Table 3 reveals (1) the 20 ‘concept’ topics associated with the most articles in this cluster (including: ‘professional quality of life’, ‘empathy’, ‘culture’, ‘compassionate caring’ and ‘job satisfaction’), (2) the top 20 trending topics (i.e. topics with the most recent average article publication date), and (3) the ‘highest impact’ article topics – i.e. the topics whose articles have the highest average citation rates, correcting for year of article publication.
Most frequent, trending, and highest cited article topics by topic cluster.
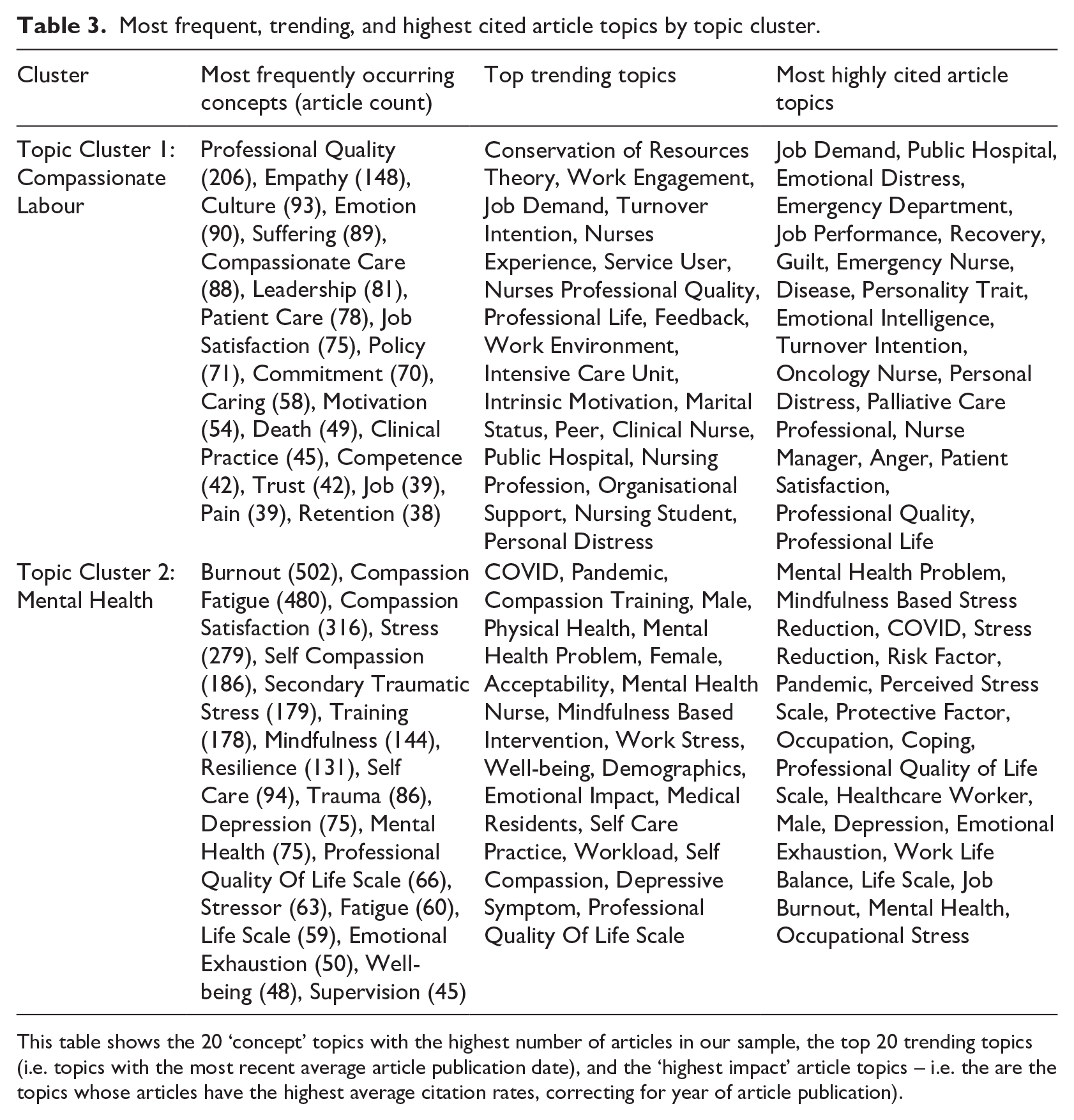
This table shows the 20 ‘concept’ topics with the highest number of articles in our sample, the top 20 trending topics (i.e. topics with the most recent average article publication date), and the ‘highest impact’ article topics – i.e. the are the topics whose articles have the highest average citation rates, correcting for year of article publication).
The Mental Health topic cluster (Topic Cluster 2, green), contains 95 article topics. The topics in this cluster predominantly deal with the consequences of exposure to suffering, and includes research on burnout, stress, compassion fatigue, compassion satisfaction, and intervention approaches. The focus is on employees who especially need mental health support due to the stressful or even traumatising nature of their work – such as healthcare, military and veterinary professionals, and employees who provide support to others – such as social workers and psychologists. Table 3 provides an overview of the top 20 ‘concept’ topics associated with the largest number of articles this cluster (including: ‘burnout’, ‘compassion fatigue’, ‘stress’, ‘traumatic stress’ and ‘mindfulness’), the top 20 trending topics, and the ‘highest impact’ article topics.
3.3. Systematic reviews
In this section, we review the literatures associated with the two major topic clusters identified in workplace compassion research, revealing key article themes and findings. Following previous research (e.g. Byington et al., 2019, 2021; Markoulli et al., 2017), articles were assigned to a topic cluster if (1) the articles contained at least two topics in their title/abstract and (2) more than 50% of the topics ‘belonged’ to a single cluster.
Next, to systematically identify major themes, the articles belonging to each topic cluster were coded using an open coding, axial coding, and selective coding process (Strauss and Corbin, 1990). The articles were fully coded by the first author, with a subsample of 15% of the articles also independently coded by the last author, and with discrepancies resolved by collectively reviewing the relevant articles to reach consensus. Once coding was completed, an independent researcher completed a final review of the axial and selective codes with 100% agreement. The open, axial, and selective codes and number of articles associated with each code are presented in Table 4 for Topic Cluster 1, and Table 5 for Topic Cluster 2. These tables offer readers an overview of a) key themes in the workplace compassion research across the social sciences, and b) the structure of this review. Figure 6 provides a visual overview of the open and axial codes. Below, we discuss key concepts, relationships and findings associated with the selective and axial codes. We chose to discuss articles that are either (1) the most-heavily referenced, and/or that are (2) exemplary of the main concept(s), relationship(s) or outcome(s) discussed in that section.
Open, axial and selective codes in topic cluster 1: compassionate labour.
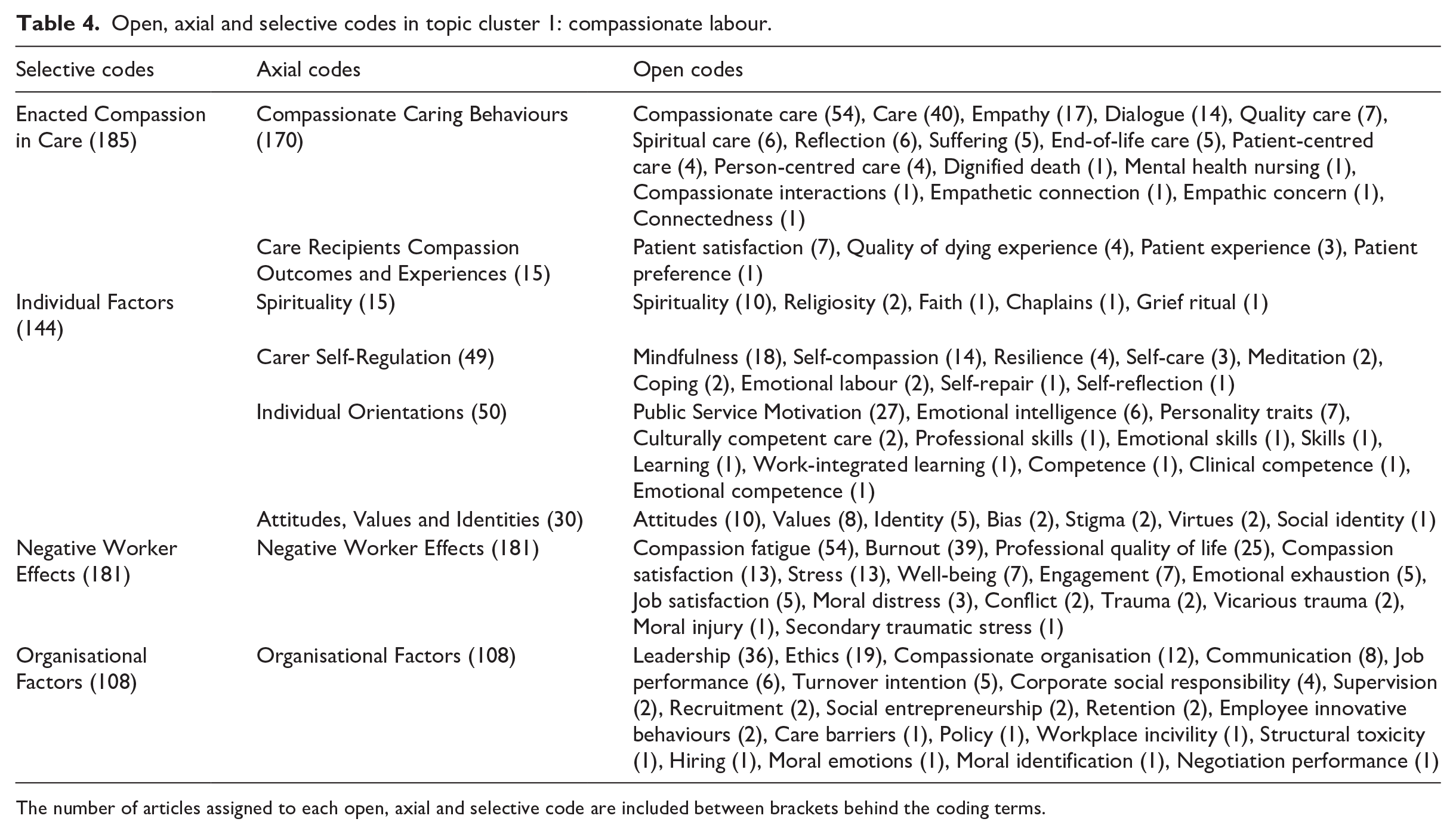
The number of articles assigned to each open, axial and selective code are included between brackets behind the coding terms.
Open, axial and selective codes in topic cluster 2: mental health.
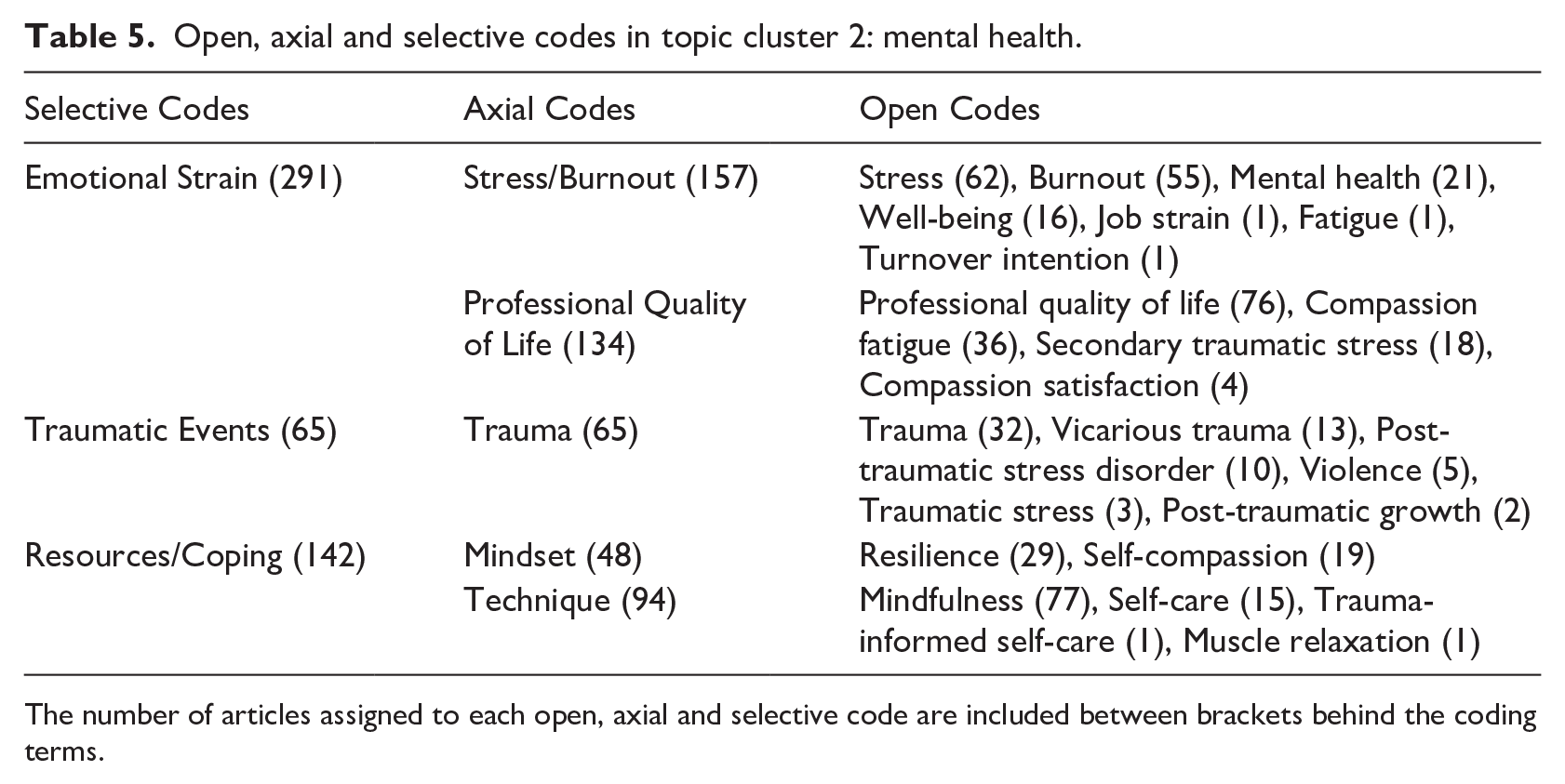
The number of articles assigned to each open, axial and selective code are included between brackets behind the coding terms.

Visual representation of selective and axial codes.
3.3.1. Topic cluster 1: compassionate labour
The process of open, axial, and selective coding of articles associated with Topic Cluster 1 revealed four major themes in this literature, namely: (1) enacted compassion in care (i.e. the phenomenon of compassionate care in organisations), (2) individual factors (i.e. worker qualities linked to the provision of compassion), (3) negative effects on workers (i.e. consequences of compassionate care delivery for workers) and (4) organisational factors. Table 4 provides a summary of the open, axial and selective codes associated with Topic Cluster 1. We discuss key articles associated with these Topic Cluster 1 themes and their subthemes in more detail below.
3.3.1.1 Enacted compassion in care
A large number of articles associated with Topic Cluster 1: Compassionate Labour focus on the provision of compassion as a feature of high quality care for others (usually patients, clients, consumers) in organisations, and most often in healthcare settings. Terms in the map related to this theme can be split into two subthemes, those related to compassionate caring behaviours of healthcare professionals (e.g. ‘care’, ‘compassionate care’, ‘empathy’, ‘dialogue’), and those related to the compassion outcomes and experiences of care recipients (e.g. ‘patient satisfaction’, ‘patient preference’, ‘patient experience’, ‘quality of dying experience’).
3.3.1.1.1. Compassionate caring behaviours
‘Compassionate care’ is associated with the highest number of articles in the ‘enacted compassion in care’ theme (e.g. from Adam and Taylor, 2014; Brown et al., 2014; up to Zamanzadeh et al., 2018), and in this literature, compassion is often presented as a fundamental element of healthcare work. Compassionate care has been defined as a process, where attention, empathy, and understanding is provided (Tehranineshat et al., 2019) to respond to another’s need and to ameliorate their suffering (Sinclair et al., 2018). Importantly, the ‘care’ element is reflected in the individual’s motivation and action to improve the situation (for example through patient-nurse communication) as a ‘professional choice’ (Tehranineshat et al., 2019). Articles on this theme consider what defines care as ‘compassionate’ (e.g. Durkin et al., 2019; Papadopoulos et al., 2016), how healthcare employees incorporate compassion into their caring practice (e.g. Lin et al., 2021; McGinnis et al., 2016), and what impairs healthcare professionals’ capacity to offer compassionate care (e.g. Valizadeh et al., 2018).
Fundamental to this subtheme is that the provision of compassionate care requires the observation or noticing of others’ suffering and experiencing empathy (or ‘empathetic connection’ or ‘empathic concern’) for others. This leads to healthcare professionals’ engaging in compassionate caring behaviours to decrease or relieve the pain or suffering of patients (Tehranineshat et al., 2019). The motivation to relieve patient suffering is also critical for enhancing the capacity for compassionate care, and this capacity is further influenced by individuals’ values and beliefs (having altruistic motives, aligning compassionate care with faith, belief, or one’s upbringing), engaging with positive role models of compassion (as it is both an innate and learned clinical competence), and having personal experience being a patient or having had a family member who has suffered (which helps healthcare professionals to be compassionate; Zamanzadeh et al., 2018).
As providing compassionate care is partly an acquired competence, various articles have examined how educators can best equip nursing students with this skill, and how a culture of compassion in healthcare is best promoted. Education that focuses on students’ self-reflection on their experience during work placements has been found to help students to identify which skills they need to develop to be more effective in delivering compassionate care, and to develop a ‘toolkit’ to help them meet these needs (Adam and Taylor, 2014). Similarly, various compassionate care programmes have been found to help nurses engage in reflection, master challenging situations, and develop confidence to deliver compassionate care (Coffey et al., 2019). Beyond the early healthcare placement stages and education, various articles have investigated how healthcare leaders encourage healthcare professionals’ compassion, or enlarge or enable more compassionate care (e.g. Dewar and Cook, 2014; Lown et al., 2019). Interventions that focus on compassionate care often involve engaging in conversation and reflection, for example with the help of Schwartz rounds (Adamson et al., 2018; Farr and Barker, 2017), reflective debrief (Schmidt and Haglund, 2017), or narrative-based interventions (Swordy et al., 2020) – with the aim of developing a greater understanding of and empathy for others’ suffering, experiences, and views. However, the number of publications on evidence-based clinical or educational interventions remains limited, and is an important avenue for future research efforts (Malenfant et al., 2022).
In addition, various barriers that prohibit the delivery of compassionate care are also identified in this literature. For example, Roze des Ordons et al. (2020) outlined that ‘gaps’ in compassion provision can be a) individual (due to inattention or insufficient personal capacity to be compassionate, and a lack of patients’ perception of healthcare professionals’ intention to be compassionate), b) relational (due to conflict, fragmented care, lack of shared understanding), or c) reflective of the organisational/hospital context (e.g. situational pressures such as lack of time, workload, the clinical environment, physical layout, poor organisational culture, a lack of education). Organisational constraints such as staffing shortages, activities that detract from patient contact (e.g. record-keeping and internal processes of quality control), and a lack of support are frequently highlighted obstacles (e.g. Brown et al., 2014; Crawford et al., 2014; Horsburgh and Ross, 2013). Other challenges can be the provision of compassionate care in the digital age, where care is mediated through technology (Wiljer et al., 2019), as well as the variety of stresses related to, for example, providing end-of-life care – which can lead to clinician burnout (Kearney et al., 2009). However, many articles highlight that when compassionate care is provided, it is powerful and can have positive consequences both for the care provider (such as positive worker experiences) and patient experiences. The latter is described in the following theme.
3.3.1.1.2. Care recipients’ compassion outcomes and experiences
A smaller subsection of articles in the ‘enacted compassion in care’ subtheme examine the link between the provision of compassionate healthcare and the experiences of patients and patients’ family members (e.g. patient experience after total shoulder arthroplasty: Menendez et al., 2019; childbirth experience: Gregory et al., 2019, and family members’ experience of hospice care: York et al., 2012). A recurrent finding in these articles is that when patients and family members perceive healthcare professionals and their care to be compassionate, they report a more positive experience and are more satisfied with the overall care (Gregory et al., 2019; Menendez et al., 2019; York et al., 2012). In addition, compassion benefits the patient-caregiver relationship. Interviews with patients with breast cancer, Lyme disease, and mental illness finds that attentiveness, eye contact, being friendly, truthful, non-judgmental, reassuring, respectful and sensitive (often summarised as compassionate) were crucial elements that helped foster trust in healthcare providers (Mechanic and Meyer, 2000). Similarly, in an experimental paradigm, breast cancer patients observed either a ‘standard’ videotape based on real-life breast cancer diagnosis consultations (where the physician described treatment risk and benefits, survival probabilities, and side effects) or a ‘compassionate’ tape (with two additional segments, including the expression of support, empathy, and compassion for the patient’s difficult situation). Patients who viewed the compassionate tape reported lower post-test anxiety, and believed the doctor cared about the patient more than patients who viewed the standard tape (Fogarty et al., 1999). On the other hand, healthcare providers who were perceived by patients to be inattentive, who were unable to address emotional distress (Menendez et al., 2019), who did not have time for questions (Gregory et al., 2019), or who showed a lack of empathy and support provision (York et al., 2012) were strongly associated with negative patient comments about their care and experiences. Overall, these articles highlight the importance of providers’ compassionate care. Factors that relate to the capacity and opportunity to be compassionate at an individual level are discussed in the following theme.
3.3.1.2. Individual factors
A second group of articles associated with Topic Cluster 1: Compassionate Labour focus on individual traits and factors that allow, enable, or predict individuals being compassionate at work, as well as individual factors that contribute to creating compassionate organisations. This group of articles is further divided into four main ‘subthemes’ of individual factors, namely: 1) spirituality, 2) carer self-regulation, 3) individual orientations, and 4) attitudes, values and identities.
3.3.1.2.1. Spirituality
A subset of articles (Table 4) in this literature focus on the importance of spiritual care, and religiosity or spirituality in medicine and organisations. Terms in the map related to this theme include ‘spirituality’, ‘religiosity’, ‘faith’ and ‘chaplains’. In these articles, spirituality is often likened to values and attitudes (such as caring and respect for others, creating a corporate culture with universal human values). For example, interviews with managers in organisations in Turkey highlighted that leaders often look for spirituality in their work, and it is related to building high quality connections with others, developing empathy and rapport, and ‘reaching hearts’ (Karakas, 2010). Workplace spirituality is found to relate to positive outcomes for employees, with survey research on 250 healthcare professionals suggesting that when employees have a spiritual orientation, and serve the organisation as a spiritual and professional duty, they experience higher job satisfaction and have lower turnover intentions (Zaidi et al., 2019). Similar results were observed following a spiritual care training for palliative care professionals. Specifically, when healthcare professionals reflect on their own fear of death, learned techniques of active and compassionate listening in ways that recognised and addressed suffering, they reported higher well-being, greater compassion for the dying, and compassion for themselves six months later (Wasner et al., 2005).
3.3.1.2.2. Carer self-regulation
The second group of articles focuses on individual behaviours that enable employees to be a compassionate carer, leader, or labourer in a sustainable way. Terms associated with this subtheme include ‘mindfulness’, ‘meditation’, ‘self-compassion’, ‘self-care’, ‘self-repair’, ‘resilience’, ‘emotion regulation’, ‘coping’ and ‘emotional labour’. These behaviours are overarchingly related to being in the moment and mindful (Hägglund et al., 2022), practicing self-compassion (Shepherd and Cardon, 2009), practicing self-care (Mills et al., 2018), resilience (Grauerholz et al., 2020), and effectively regulating emotions (Barnett et al., 2020) when experiencing hardship or stress. Importantly, many of these ‘self-regulation’ behaviours are suggested to be crucial for supporting sustainable work engagement (Cao and Chen, 2021), compassionate care delivery (Aycock and Boyle, 2009), and well-being (Lefebvre et al., 2021; Micklitz et al., 2021) in challenging work environments such as healthcare.
3.3.1.2.3. Individual orientations
The third group of articles deals with the individual orientations that motivate individuals to engage in compassionate labour, to help build compassionate workplace cultures, and to be effective in their jobs. The frequent article topics in the map associated with this subtheme are ‘public service motivation’, ‘personality’, ‘traits’, and ‘emotional intelligence’. Public service motivation – defined as ‘an individual’s predisposition to respond to motives grounded primarily or uniquely in public institutions and organisations’ (DeHart-Davis et al., 2006: 873) – captures commitment to public interest, civic duty, social justice, self-sacrifice, and compassion, and has been found to relate to job satisfaction (Belrhiti et al., 2019), as well as presenteeism and performance (Gross et al., 2019). Similarly to public service motivation, greater intercultural sensitivity (which includes having respect for other cultures, enjoying interactions with individuals from different cultures, and being attentive during these interactions; Arli and Bakan, 2018) and higher ability and trait emotional intelligence (Nightingale et al., 2018) are associated with compassion in nurses. In addition, the personality traits agreeableness, extraversion and conscientiousness are also associated with the compassion satisfaction of paediatric nurses (Chen et al., 2018) as well as neonatal nurses (Barr, 2018). These findings highlight that individuals’ orientations are important contributors to individuals’ compassion capacity.
3.3.1.2.4. Attitudes, values, and identities
The fourth group of articles identifies individuals’ attitudes, values and identities that are important in encouraging (or impair) the experience of compassion towards others at work. Examples of barriers include bias and stigma (e.g. bias against patients of a certain race or with low socio-economic status: Hirsh et al., 2019; patients with disabilities: Sahin and Akyol, 2010; or against patients who suffer from opioid use disorder: Cernasev et al., 2021). On the other hand, individuals’ values, attitudes, and identity (such as a sense of responsibility, accountability, and being ‘an advocate for patients’) can lead them to be compassionate towards others, and support patient-centeredness and alignment with organisational values of compassion (Groothuizen et al., 2019), or prompt one to enter a certain profession in the first place (such as nursing: Van Der Cingel and Brouwer, 2021).
3.3.1.3. Negative worker effects
A third key theme in Topic Cluster 1 articles is the potential negative effects for employees working in professions where they are frequently exposed to emotional and physical suffering in their work (e.g. Delgado et al., 2021; Pérez-García et al., 2021; Richardson and Greenle, 2020; Sullivan and Germain, 2020). Such demanding and high-stress work environments can, over time, lead to work-related stress and traumatisation for employees (Van Mol et al., 2015), and in the long run, negative work outcomes such as lower professional quality of life (Sinclair et al., 2017), burnout (Hooper et al., 2010), lower well-being and job satisfaction, post-traumatic stress, and moral distress and injury. Importantly, what sets this theme in Topic Cluster 1 apart from themes in Topic Cluster 2 (‘mental health’), is that in this theme, the negative worker effects are examined in light of how cumulative stress relates to work (of predominantly healthcare professionals), and how these negative cumulative effects a) can impact the delivery of care in organisations, b) are considered a ‘cost of caring’, and c) are a key contributor to the lack of compassion in organisations (Sinclair et al., 2017).
3.3.1.4. Organisational factors
A final major theme in Topic Cluster 1 articles focuses on organisation-level compassion (rather than individual level). Within this theme, articles focus on how collective compassion (e.g. compassionate culture) is developed in organisations (e.g. Dutton et al., 2006; Kanov et al., 2004), and what the ‘outcomes’ are of having compassionate organisations (e.g. Hur et al., 2016; Ko and Choi, 2019) or lack thereof (Bolton and Laaser, 2021). The most often occurring map terms associated with this group of articles include: ‘organisational ethics’, ‘compassionate organisation’, ‘corporate irresponsibility’, ‘leadership’, and ‘turnover’.
In this literature, there is a major focus on how compassionate organisations come to be. This includes a) how organisations can be structured (systems, policies, processes) to be more compassionate (for example through a more compassionate hiring processes or by allocating resources to help alleviate pain or suffering; Dutton et al., 2006) and b) the role organisational citizens play in developing compassionate organisations (for example, compassionate leadership, compassionate culture). This acknowledges that individual and organisational compassion influence and build one another. Developing compassionate organisations starts with the identification of pain or suffering of individuals (such as patients, employees, clients) by employees. Once there is individual awareness of suffering, employees may engage in ‘activation’ in organisations to alleviate this suffering (Kanov et al., 2004).
An example of the link between compassion at the individual and organisational levels from Dutton et al. (2006) is of two international university students losing their belongings in a fire. A faculty member driving past the scene observes the students’ suffering and notifies student services and the dean’s assistant. This leads to a sequence of compassionate actions and resource allocation by the university, including the provision of temporary laptops, new accommodation, and clothing donations. These actions are positively perceived by students and employees, affirming their belief that the university is a compassionate organisation. Through this process, an organisation creates shared values that in turn define how employees act (Dutton et al., 2006). In the example above, there is an emergent norm that employees and students show kindness and help those in need, which helps to create a more compassionate organisation.
The top-down link between organisational practices and employee-level compassion has also been investigated. For example, Guzzo et al. (2022) found that when organisations engage in corporate social responsibility practices, employees report feeling more grateful and compassionate at work, and in turn engage in more organisational citizenship behaviours. In this example, corporate social responsibility practices act as an ‘ethical stimuli’ to promote a compassionate workplace culture.
Organisational leaders can also play a key role in impacting employee behaviours and the culture of their organisation. For example, compassionate leadership (including empathy, integrity, authenticity, dignity and accountability) has been found to improve employee engagement, psychological well-being, lowers intention to leave (Shuck et al., 2019), and relates to improved nurse well-being (Adams et al., 2019). As compassionate leadership skills have been found to be effectively developed or improved through coaching (Boyatzis et al., 2006) and mindful leadership courses (Vreeling et al., 2019), developing compassionate leaders is a way through which organisations can develop a compassionate workplace culture.
There is also a growing emphasis on embedding compassionate behaviours as part of professional training and accreditation (Whitehead et al., 2014), and by ‘demanding’ compassionate behaviours and actions through policy and codes of ethics and conduct. For example, the International Council of Nursing identified compassion as one of the five core nursing values (Younas and Maddigan, 2019), programmes such as ‘Compassion in Practice Vision and Strategy’ were launched to promote compassionate care in the United Kingdom following the Frances Report (2013), and the United Kingdom implemented a nursing code of ethics and conduct where the absence of kindness and compassion is identified as contrary to ‘The Code’ (Snelling, 2016).
Researchers have also identified an absence of discourse on compassionate care in medical education (Whitehead et al., 2014). To address this, proposals for policy frameworks have been put forward that involve programmes and strategies promoting the cultivation of compassionate care in nursing education. Such proposals include 1) the explicit promotion of professional values (such as compassion) in medical education (Whitehead et al., 2014), 2) the inclusion of affective learning in the curriculum, 3) the use of reflection to grow, and 4) assessing students’ understanding and expression of compassion (Younas and Maddigan, 2019). At the same time, initiatives such as the ‘Compassion in Practice Vision and Strategy’ and the inclusion of compassion in organisational policy has also been met with critique. Rather than improving compassionate care, nurses have reported less self-confidence in their care and perceive the changes as a blow to morale (Whitehead et al., 2014). Crawford and Brown (2011) warn that individual practitioners are blamed for failing to be compassionate at work, rather than addressing contextual factors in healthcare that undermine the delivery of compassionate care, such as high work intensity, low staff levels and resources, and working under time pressure (Crawford et al., 2014). Compassion is argued to ‘require a facilitative environment to flourish’ (Tierney, 2018: 5) and individually focused compassion-related policies may overlook much bigger, broader, and more systemic challenges.
3.3.2. Topic cluster 2: mental health
The articles associated with Cluster 2 in the topic map focus on the consequences of working in professions where frequent exposure to suffering or potentially traumatic events or material is common. The topics in the map associated with these articles include outcomes for these individuals (such as ‘stress’, ‘burnout’ and ‘trauma’) as well as intervention techniques or available routes to enhance resilience (most frequently involving ‘mindfulness’ interventions).
The process of open, axial, and selective coding of articles associated with Topic Cluster 2 revealed three major themes in this literature, namely: (1) emotional strain, (2) traumatic events, and (3) resources/coping. Table 5 provides a summary of the open, axial and selective codes associated with Topic Cluster 2. We will discuss notable articles related to each of these key themes below.
3.3.2.1. Emotional Strain
Per Table 5, a large number of articles associated with Topic Cluster 2 focus on the mental health-related consequences of dealing with suffering. The majority of these articles focus on healthcare professionals, with a smaller number focusing on veterans, teachers, psychologists/psychotherapists, and veterinarians. The articles in this theme can be further split into two subgroups; ‘stress/burnout’ and ‘professional quality of life’.
3.3.2.1.1. Stress/burnout
Articles in the ‘stress/burnout’ group include the terms ‘stress’, ‘burnout’, ‘job strain’, ‘fatigue’, ‘well-being’ and ‘mental health’. Overarchingly, articles in this subtheme focus on employees who are at high risk of developing poor mental health (for example front-line providers; Jawa et al., 2022, veterinary nurses; Lloyd and Campion, 2017, paediatric nurses; Khatatbeh et al., 2021, child protection social workers; Conrad and Kellar-Guenther, 2006; McFadden et al., 2015 oncologists; Kleiner and Wallace, 2017). The most frequent negative mental health outcomes examined within this theme are symptoms of burnout (e.g. Kemper et al., 2020; Montero-Marin et al., 2016), psychological distress (e.g. Higuchi et al., 2016; Page and Robertson, 2022), and depression and anxiety (e.g. Dosil et al., 2020; Magnavita et al., 2021). Predictors of poor mental health identified in this literature include perceived time pressure and heavy workload (Kleiner and Wallace, 2017), work-related stress (Mota Vargas et al., 2016), sleepiness/exhaustion and dissatisfaction with work-life balance (Kemper et al., 2020), and frequently experiencing burden and traumatic events at work (Inbar and Shiri, 2021).
3.3.2.1.2. Professional quality of life
Articles in this subtheme focus specifically on the ‘cost of caring’ and commonly include terms such as ‘professional quality of life’, ‘secondary traumatic stress’, ‘compassion fatigue’, and ‘compassion satisfaction’. Within this subtheme, ‘professional quality of life’ is examined most often (see Table 5).
A particular challenge within this literature is the lack of conceptual clarity between constructs (Beck, 2011). Namely, in this literature, the ‘cost’ of caring is often measured using the Professional Quality of Life Scale (ProQoL; Stamm, 1995). While there are differences between versions of this scale, the most frequent subscales used include compassion fatigue, compassion satisfaction, secondary traumatic stress, and burnout. However, while these are closely related constructs, and are often measured and discussed in the same articles (e.g. Avieli et al., 2016; Chia-Yun et al., 2021; Scott et al., 2021), they are not conceptually synonymous. There is empirical evidence that some of the ‘cost of caring’ constructs may strongly overlap. Specifically, while psychometric property analysis has been found to be satisfactory for the ‘compassion satisfaction’ construct, there are concerns around the ‘compassion fatigue’, ‘burnout’, and ‘secondary traumatic stress’ scales (Hemsworth et al., 2018). In addition, many scholars contest the term ‘compassion fatigue’, and suggest that what the ProQol measures is more aptly labelled ‘empathic distress’ or ‘personal distress’ (e.g. Hofmeyer et al., 2020), and that: ‘the ProQOL . . . does not assess any of the elements of compassion’ (Sinclair et al., 2017: 9). As the extent to which the ProQol is a valid and reliable instrument is debated, we will outline how the constructs differ or relate.
‘Compassion fatigue’ is a major focus in this group of articles (see Table 5). Figley (2002) outlines that compassion fatigue arises because: ‘the very act of being compassionate and empathic extracts a cost’ and ‘in our effort to view the world from the perspective of the suffering, we suffer’ (p. 1434). Compassion fatigue is argued to reduce individuals’ capacity or interest in ‘bearing the suffering’ of others and is described by Figley (2002) as a function or consequence of ‘secondary traumatic stress’. Secondary traumatic stress (see Table 5) is in turn described as ‘the natural consequent behaviours and emotions resulting from knowing about a traumatizing event experienced by a significant other – the stress resulting from helping or wanting to help a traumatized or suffering person’ (p. 1435). Beck (2011) describes secondary traumatic stress as an ‘occupational hazard for persons who provide direct patient care to traumatized victims’ (p. 2).
Interestingly, the burnout items of the ProQOL are not focused on exhaustion symptoms (unlike other job burnout scales, such as the Maslach Burnout Inventory [MBI; Maslach et al., 1997] which appears in articles on the stress/burnout subtheme), but rather focus on negative work attitudes, feeling ‘overloaded’ with work, and lacking well-being (Cieslak et al., 2014). Notably, Figley argues that ‘compassion fatigue’ is a narrower construct. Where burnout involves physical, emotional and mental exhaustion, compassion fatigue is argued to be caused specifically by the provision of compassionate care, and related exposure to the trauma or suffering of clients/individuals. The relationship with secondary traumatic stress and burnout is complex. A meta-analysis (Cieslak et al., 2014) examined the relationship between secondary traumatic stress and job burnout and found a large and positive association (weighted r = .69). When burnout was measured with the MBI, the relationship between secondary traumatic stress was the strongest with the emotional exhaustion subscale (weighted r = .55), then depersonalization (r = .51), and finally with the subscale that captures feelings of a lack of accomplishment (r = .35), suggesting more conceptual distinction (Cieslak et al., 2014). ProQoL burnout and secondary traumatic stress may share as much as 48% of variance (Cieslak et al., 2014) – highlighting that how these constructs are operationalised and measured is important as these constructs are not necessarily distinct.
A number of articles in this subtheme describe the factors related to the experience of low professional quality of life. These factors include negative co-worker relationships, high number of hours worked per shift (Hinderer et al., 2014), years in service and reported levels of depression (Jacobson et al., 2013), lower empathy and higher use of maladaptive coping strategies (Raynor and Hicks, 2018), understaffing, poor relationship with supervisors, and lack of training in managing work-related distress (Randall et al., 2021).
Furthermore, in case study research associated with the subtheme, Figley (2002) outlines how compassion fatigue develops among psychotherapists who work with chronic illness, and what therapists can do to avoid compassion fatigue or to ameliorate their situation. Specifically, Figley recommends a) familiarising individuals working with the suffering of others with the concept and the symptoms of compassion fatigue (Coetzee and Klopper, 2010), b) desensitising therapists to traumatic stressors, c) combining exposure to traumatic stressors with relaxation, and d) assessing and enhancing social support (Figley, 2002). Recommendations to protect employees from secondary traumatic stress are similar. For example, Beck (2011) suggests that workers need to be educated about the symptoms of secondary traumatic stress, need to get enough sleep, exercise, enjoy activities outside of work, spend time with family and friends, diversify the types of patients they see, focus on positive components of one’s work, and share the experience with other workers who may experience the same.
As noted above, while compassion fatigue has been a major topic of interest in this literature, many compassion scholars critique the label ‘compassion fatigue’, and argue that it is a misnomer (Dowling, 2018; Sinclair et al., 2017). For example, Hofmeyer et al. (2020) provide neuroscientific evidence (i.e. functional magnetic resonance imaging [fMRI] study results) that highlights that excessive empathy causes fatigue, rather than compassion. Many compassion scholars strongly argue that ‘compassion fatigue’ should be called ‘empathic distress fatigue’, because the distress and fatigue arise from the inability to disconnect from the other person who is suffering (for example, patients), and an inability to protect oneself from excessive negative feelings. This is an important distinction, as fMRI studies show that empathic distress fatigue can be ameliorated by turning empathy into compassion (for example through compassion training; Klimecki and Singer, 2011). Importantly, the proliferation of research on ‘compassion fatigue’ has implications for our understanding of cause and effect and can have downstream consequences for prevention and intervention initiatives for healthcare professionals. For example, it could be used as the rationale for not investing resources to support compassion-based initiatives. Thus, there is a need to focus on conceptualising and operationalising empathic distress and empathic distress fatigue in research (DeDecker, 2020).
3.3.2.2. Traumatic events
In addition to the exploration of the high risk of poor mental health outcomes due to working with suffering, a subtheme in the literature associated with Topic Cluster 2: Mental Health focuses on the trauma outcomes of specific events. This theme includes articles on ‘trauma’, with a small subsection focusing on ‘violence’ as a trauma-inducing event. Topic map terms associated with this subtheme include ‘post-traumatic stress disorder’, ‘post-traumatic growth’, ‘trauma’, ‘traumatic stress’ and ‘vicarious trauma’, as well as ‘violence’ and ‘victim services’.
A distinction can be made here between vicarious trauma, which is the experience of secondary or ‘indirect’ trauma and distress when working with traumatised patients, clients or individuals, and traumatic stress and post-traumatic stress disorder, which is distress and trauma following firsthand experience of traumatic events or material. Of note is that ‘secondary traumatic stress’ is a sub-scale of the Professional Quality of Life Scale (ProQoL; Stamm, 1995), and the term ‘vicarious trauma’ is often used synonymously with compassion fatigue, secondary traumatic stress, and burnout. Trauma as discussed in this theme (rather than secondary traumatic stress as included in the sub-scale of the ProQoL) involves a) cognitive changes in beliefs and attitudes as effects of trauma (Sabin-Farrell and Turpin, 2003), as well as b) neurobiological changes that can lead to flawed decision making (Tyler, 2012). Experiencing violence at work is an example of a firsthand experience that can lead to traumatic stress or the development of post-traumatic stress disorder, with Hilton et al. (2022), for example, finding that events such as assault, cumulative exposure and aggression experienced by psychiatric nurses are implicated in the development of post-traumatic stress disorder.
When working with clients who have or are experiencing trauma (vicarious trauma for the worker), it is important for workers to reflect on and work through the trauma themselves. For example, one study conducted by Ifrach and Miller (2016) found that art therapy-based interventions for counsellors working in domestic violence and sexual assault services were helpful in reducing the counsellors’ stress. Similarly, trauma therapists who work with torture survivors were found to have higher burnout and distress when they did not work through the discussed traumatic events themselves (Deighton et al., 2007).
3.3.2.3. Resources/coping
The final theme in Topic Cluster 2: Mental Health articles focuses on investigating resources and coping skills that are helpful in building resilience and minimising or ameliorating the detrimental effects of working in taxing environments. This theme can be subdivided into articles that focus on ‘mindsets’, and those that focus on ‘techniques’.
3.3.2.3.1. Mindsets
Key terms associated with the mind-set subtheme articles include ‘resilience’ and ‘self-compassion’. Both resilience and self-compassion have been identified as crucial skills for healthcare professionals, as well as for other professionals who deal with suffering. Resilience has been defined as ‘the ability to practice professionally utilizing empathy, optimism, stability, honesty and self-awareness . . . it can be considered as an umbrella term encompassing internal resources and behaviours, helping people cope with adversity and develop themselves from such experiences’ (Kotera et al., 2020: 3). Self-compassion, on the other hand, has been defined as the ‘nonjudgmental awareness of one’s own suffering and failures, and the recognition of these as an inherent part of being human’ (Medvedev et al., 2021: 636). Although the two are distinct concepts, resilience and self-compassion are often examined in tandem, or self-compassion is seen as part of the mind-set that helps create resilient workers.
Several studies examine the effect of self-compassion training or interventions. For example, Finlay-Jones et al. (2017) found that a 6 week online, self-guided self-compassion cultivation programme for psychology trainees helped promote self-compassion, happiness, and helped lower distress. It is argued that self-compassion promotes adaptive coping and emotion regulation following stressful events (Finlay-Jones et al., 2017). Similarly, Scarlet et al. (2017) found that Compassion Cultivation Training (CCT) for healthcare professionals enhanced self-compassion, reduced interpersonal conflict, and improved self-reported job satisfaction following an 8 week course.
Articles within this subtheme have also examined what makes an employee resilient, and what the consequences can be of having resilience in terms of well-being outcomes. A study conducted by Lakioti et al. (2020) found that a variety of well-being factors, such as finding meaning in the job, self-efficacy, empathy, workplace characteristics, and experiencing positive emotion at work help therapists maintain resilience to work stressors. However, there are also factors outside of individuals that can lower resilience. For example, non-clinical issues in the workplace were found to be a critical factor that reduced resilience in doctors in the United Kingdom (McCain et al., 2018) – in these cases, improving personal resilience may not be enough to remain happy and healthy in one’s job.
3.3.2.3.2. Techniques
The final article subtheme under the theme of Resources/Coping focuses on techniques individuals can use to maintain well-being. The terms include ‘mindfulness’, ‘self-care’, ‘trauma-informed self-care’ and ‘muscle relaxation’. The difference between articles included in the ‘techniques’ versus the ‘mindsets’ subthemes is largely due to the focus of the latter on interventions or skills. Where resilience and self-compassion focus on positive psychology and self-view, coping and self-talk, the articles included in this subtheme focus on techniques that can be practised and refined to help ameliorate or improve mental health in the face of challenging work environments. Within this subliterature, mindfulness is by far the most often-coded term. Notably, many of these articles examine mindfulness interventions through pilot studies/programmes (e.g. Moody et al., 2013; Rimes and Wingrove, 2011), controlled clinical trials (e.g. Pérula-de Torres et al., 2019), and randomised controlled trials (e.g. Trombka et al., 2021; Verweij et al., 2018). Given the sheer volume of articles on mindfulness-based interventions (77 articles, see Table 5), it is no surprise that several meta-analyses have examined the influence of mindfulness-based interventions on outcomes. For example, meta-analyses on mindfulness-based interventions indicated that these interventions improve self-compassion in healthcare professionals (Wasson et al., 2020), reduce stress, ruminative thinking, and anxiety (Chiesa and Serretti, 2009), reduce depression and burnout, and improve health and job performance (Lomas et al., 2019). This accumulating evidence of the benefits of mindfulness-based interventions is encouraging, as it offers an easy and accessible route to prevent or ameliorate some of the negative consequences of working in challenging environments and occupations. However, as mentioned previously in this review, the focus on the worker to ‘heal themselves’ can also be problematic (Crawford et al., 2014), and place additional burdens on workers.
4. Discussion
Overall, this article makes several important contributions. First, we used science mapping and primitive grounded theory to provide a summary of the workplace compassion literature from across the social sciences that is more comprehensive, systematic, and integrative than prior reviews. Our topic map can aid scholars in exploring the topic contents of this vast literature more conveniently, to see what is studied, what may be missing, and assist in identifying opportunities for concept importation across disciplines. Second, in identifying topic clusters and article themes, we have provided new, integrative frameworks for understanding workplace compassion scholarship and its contents (e.g. Figures 3 and 6). Furthermore, in identifying and reviewing key themes and subthemes in the articles associated with each topic cluster, we have provided an integrative review of this large literature, and highlighted a few critiques and ongoing debates (e.g. issues of conceptual clarity and empirical overlap depending on the specific measures employed). Here, we aim to highlight both key takeaway conclusions from the new organising framework that this article provides, acknowledge limitations, and note promising future research directions for the field broadly – which we derived from this new, overarching view of workplace compassion scholarship.
The summary of the workplace compassion literature presented in the topic map analysis offers an empirically derived taxonomy of two major topic clusters in the workplace compassion literature. The topics and articles associated with these topic clusters indicate two primary conversations on workplace compassion in the social sciences, namely Compassionate Labour research and Mental Health research. The Compassionate Labour articles predominantly focus on compassion as it occurs in workplace contexts, whereas the Mental Health articles focus on employees who especially need mental health support due to the stressful or even traumatising nature of their work (e.g. healthcare, military, and veterinary professionals), and for employees who provide support to others (e.g. social workers and psychologists). Articles in both topic clusters highlight that compassion is a critical part of many types of work, and yet working in a role where compassion is integral to being effective at work may come at a cost. Documenting harm, developing solutions, and the value of cultivating compassion both for individuals and organisations have been key areas of interest. And indeed, enabling compassion at work and protecting those employees who provide it may prove to not only prevent harm, but may also improve capacity, motivation, and self-confidence, and the social climate for employees.
5. Limitations
Although we cover nearly 30 years of research, our search was limited to workplace compassion research in the Web of Science Social Science Citation Index, and does not reflect compassion research in other non-work contexts, nor research outside the WoS-SSCI. The advantage of our approach is the relevance of this review for management scholars and practitioners specifically. However, we recognise that future reviews that provide an even broader view of compassion beyond the work domain, as well as targeted reviews (e.g. compassion in politics, geopolitical social domains, the environment, etc.) could yield potentially interesting and relevant insights about the phenomena of compassion in organisations.
6. Research agenda
First, as noted above, the results of our co-citation journal map (Figure 2) suggest disciplinary divides in the citation patterns of workplace compassion research. This highlights a key challenge for scholars, as our analysis suggests that while workplace compassion has roots in Mental Health/Clinical Psychology research, Healthcare research, and Organisational scholarship, these literatures appear to be building on knowledge within their respective discipline rather than across disciplines. This can slow the advancement of workplace compassion scholarship as a whole and creates the possibility of duplication of efforts when literatures are disconnected from one another. To help address this issue, this article (1) provides a topic map so that researchers can more easily see the topics being studied by workplace compassion scholars across the social sciences to help identify topics of study for importation across disciplinary lines, and (2) reviews major themes in workplace compassion scholarship across the social sciences, rather than within a discipline. While reading this review can be a first step towards greater understanding of insights being produced across disciplines, the frameworks provided here can aid the identification of relevant insights from other fields to achieve greater integration. One way to do this is to look for complementary or especially relevant themes indicated in the results of our coding analysis (Figure 6) and investigating those literatures further, perhaps starting with the articles on those themes discussed in the review above. For example, one area where we see particular opportunities for such integration is between the ‘Negative worker effects’ research subtheme being studied by Compassionate Labour researchers and the ‘Resources and coping’ literature in the Mental Health literature. Applied organisational scholars may be able to build on the insights produced by mental health scholars on successful coping strategies and techniques by examining the effects of field interventions in organisations aimed at supporting employees who encounter suffering at work, and who are at risk of experiencing burnout. Our co-citation analysis seems to suggest that Organisational research on workplace compassion may be the most insular and disconnected from the insights being produced by Healthcare and Mental Health/Clinical Psychology research when it comes to referencing (as indicated by the relatively large disconnect between the former and the later depicted in Figure 2). As such, we would suggest that organisational scholars may particularly benefit from broader reading into those social science literatures indicated to build on knowledge from those fields in order to contribute to greater cumulative advancements in workplace compassion scholarship as a whole, and to help avoid the possibility of duplication of research efforts and insights.
Second, given the overarching focus across both major workplace compassion literatures on frontline employees primarily in healthcare, we suggest there is a need for more research examining workplace compassion in a wider range of contexts, occupations, professions, and sectors. For example, as discussed above, much of the current literature focuses on educated, knowledge workers (e.g. healthcare professionals, therapists, social workers, etc.). We suggest a need to go beyond knowledge or white-collar workers to investigate workplace compassion dynamics among blue-collar workers (e.g. construction, agricultural, mining), and particularly for workers in stigmatised roles that are often overlooked and underrepresented in mainstream research. Indeed, in emerging economies and impoverished work contexts, many workers occupy low status roles, have insecure/precarious and stressful positions, including roles that may involve high risk of exposure to injury, trauma, and secondary traumas for themselves and their coworkers. Importantly, these employees may also benefit from interventions developed specifically to assist them in dealing with the stressors they face – that is, solutions that are feasible to implement given the particular organisational contexts they inhabit and the specific challenges they face – and where current interventions such as multi-week online self-compassion training interventions may not be feasible.
Third, our review reveals a dominant but narrow focus on the alleviation of negative mental health outcomes associated with compassion delivery, particularly the ill-health end of the mental health spectrum. Fewer studies capture positive employee well-being outcomes of compassion, such as thriving and flourishing at work. This represents a further interesting avenue for future exploration.
Fourth, methodologically, in reviewing this literature, we found that self-reported work outcomes dominate the literature generally, with far fewer studies linking workplace compassion with objective bottom-line outcomes such as turnover, absenteeism, safety/errors, performance, and productivity. Aside from George’s (2014) editorial on the apparent contradiction in the tenets of corporate capitalism (which prioritises self-interest, profit/loss, and efficiency) and compassionate organisations, the literature has been largely mute on the organisational compassion-profitability paradox. Furthermore, research linking compassion to work-related outcomes, including organisational and team effectiveness/performance outcomes is limited, and presents another promising avenue for future scholarship.
Fifth, our review finds scholarship focused on individual and organisational factors respectively, yet the field has only scratched the surface in trying to understand and unpack the multilevel nature of workplace compassion. At all levels of compassion – micro, meso, and macro – there are opportunities for more research. For example, at the individual and dyadic level, the field would continue to benefit from further studies providing in-depth investigations of the psychological mechanisms underpinning the giving and receiving of compassion. There are also opportunities to better understand the role of appraisals (e.g. self/goal relevance, deservingness, and the availability of coping/self-efficacy resources) and work motives in facilitating compassionate acts towards others. We also need more theoretical focus to better understand the reciprocal role of the compassion receiver. At the meso/team and group level, more research is warranted on the role of team leadership, norms and climate for compassion in enabling sustainable, reliable compassionate acts. Social network research offers a particularly promising opportunities to investigate compassionate networks and the ripple effects of compassion through meso-levels, such as in teams and work groups.
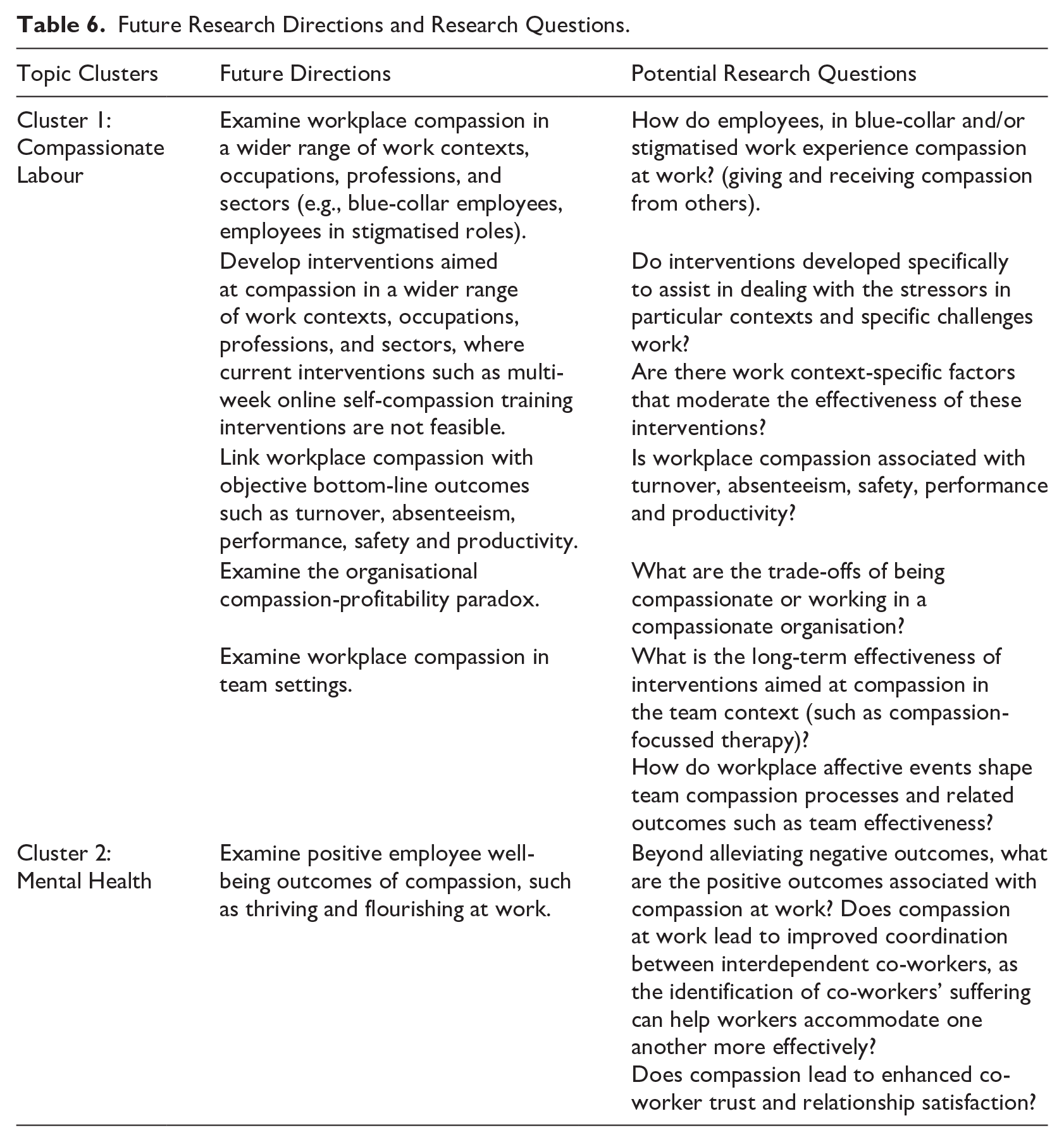
At the organisation level, a modest number of studies have examined compassion as an organisational-level socio-emotional capital that is not a given and cannot be bought (unlike other organisational resources). A lot more research is needed to identify the organisational contextual factors such as the role of work schedules, demands and interruptions in acting as contextual impediments to the ability to engage in compassionate actions. Indeed, the practice of having regular team meetings where members are encouraged to talk about their emotions and concerns can be easily disrupted by high work demands and work pressures. Again, leadership as a contextual factor plays a critical role in signalling and modelling care and compassion through actions and expressed values, publicly endorsing and legitimatising compassionate acts. For example, when leaders demonstrate compassion, they promote compassionate values, which in turn can encourage frontline health professionals to deliver compassionate care. Our future research directions and potential research questions that could advance the field are summarised in Table 6.
Future Research Directions and Research Questions.
To summarise, workplace compassion is a growing literature that has garnered significant interest across the social sciences. This review highlights that while substantial progress has been made in understanding workplace compassion over the past three decades, several foundational issues remain unresolved. We are still only beginning to explore the depths of this phenomenon, and numerous exciting opportunities for further research and practical application to enhance organisational well-being and effectiveness are waiting to be explored.
Key Contributions and Future Research Directions
There is a clear need to
While much of the existing research focuses on
See Table 6 for a detailed summary of future research directions and research questions.
Footnotes
Final transcript accepted 8 February 2025 by Lynne Reeder (AE Special Issue)
Data availability statement
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.