
Abstract
Emergence delirium, characterised by inconsolable crying, perceptual disturbances and thrashing, occurs in young children during the recovery phase from general anaesthesia. Our aim was to determine whether timing of laryngeal mask airway removal (deeply anaesthetised versus awake) influenced the incidence of emergence delirium in children after tonsillectomy. A single-centre, randomised controlled trial was conducted at Albury Wodonga Health, a regional hospital in Australia. Included patients were two to seven years old, American Society of Anesthesiologists physical status classification 1–2, undergoing elective tonsillectomy (with or without adenoidectomy or grommet insertion) under general anaesthesia. Patients were randomised to have their laryngeal mask removed whilst deeply anaesthetised (in the operating theatre) or after awakening (in the post-anaesthesia care unit (PACU)). Pediatric Anesthesia Emergence Delirium score was determined at 5 and 20 min after eye opening, and frequency of complications (cough, vomiting, excessive salivation, oxygen desaturation and laryngospasm) in the PACU were recorded. Sixty-two patients were randomised to deep laryngeal mask removal and 62 to awake. In the awake versus deep groups, 33 (53%) versus 40 (65%) participants had emergence delirium at 5 min (odds ratio (OR) 0.63, 95% confidence interval (CI) 0.30 to 1.29, P = 0.20). At 20 min, 18 (29%) vs. 19 (31%) participants had emergence delirium (OR 0.93, 95% CI 0.43 to 2.00, P = 0.88). A greater incidence of most PACU complications was observed in the awake versus deep group; cough (24% vs. 8%), vomiting (8% vs. 0%), excessive salivation (23% vs. 8%) and oxygen desaturation (16% vs. 0%). We found no significant difference between the two techniques in terms of preventing emergence delirium. However, other PACU complications were more frequent with awake removal.
Introduction
Emergence delirium is a common clinical condition that occurs in children during the recovery phase from general anaesthesia. It is associated with perceptual disturbances, inconsolable crying and hyperactive motor behaviour, manifesting as kicking, thrashing and distress.1 –8 The reported incidence of emergence delirium varies due to differing study designs and methods of defining emergence delirium; however, a reasonable estimate of its incidence is 20–30%.2,3,8,9 Further complicating estimates of the incidence of emergence delirium is the frequent interchangeable use of the terms ‘emergence delirium’ and ‘emergence agitation’. Emergence delirium implies a disturbance in cognition accompanying agitation in the post-anaesthesia period, whereas emergence agitation is an agitated state not necessarily associated with cognitive disturbance. 10 Repercussions of emergence delirium include possible interference with surgical wounds and unintentional removal of drains and intravenous catheters, and stress for post-anaesthesia care unit (PACU) staff and the child’s parents.1,7,8 Risk factors include younger age, male sex and inhalation anaesthesia, particularly with sevoflurane or desflurane.1,6,9,11,12 Specific types of surgery, specifically otolaryngological, have been associated with an increased risk of emergence delirium.1,5,6,9,13
Preventive strategies for emergence delirium have been widely investigated, although no single intervention can reliably prevent the syndrome. Studied behavioural strategies have included parental presence and distraction.
14
A number of pharmacological agents, including benzodiazepines,
15
propofol,
16
ketamine
17
and
The laryngeal mask and ETT are both commonly used during tonsillectomy. The laryngeal mask airway is preferred in our hospital 21 because of its many advantages over the ETT, including a lower incidence of pain, respiratory complications, sore throat and coughing postoperatively.22 –26
Given that emergence delirium has been suggested to be associated with a feeling of ‘suffocation’ upon awakening, 27 we hypothesised that an in situ supraglottic airway during awakening might contribute to this sensation and therefore increase the risk of emergence delirium. This study aimed to determine whether the timing of removing the laryngeal mask (deep versus awake) would affect the incidence of emergence delirium and secondarily whether various PACU complications were affected by this timing.
Materials and methods
This randomised, two-armed, parallel, controlled trial took place at Albury Wodonga Health Albury Campus from February 2021 to October 2021. The trial was approved by the Albury Wodonga Health Human Research Ethics Committee (project ID: 66918) and written, informed consent was obtained preoperatively in the paediatric ward from at least one caregiver of all participants. The study was registered with the Australian New Zealand Clinical Trials Registry (ACTRN12621000362897).
The study included patients who were American Society of Anesthesiologists physical status classification 1 or 2, between two and seven years of age and scheduled to undergo elective tonsillectomy with the successful placement of a laryngeal mask after induction of anaesthesia. Participants were excluded if the anaesthetist was concerned regarding deep removal of the laryngeal mask for any medical or anaesthetic reason, if the participant had a known or suspected difficult airway or required endotracheal intubation for tonsillectomy for any medical or anaesthetic indication, or if the parents were not able to speak English.
Demographic data such as age, sex, weight and indication for tonsillectomy, along with a baseline preoperative Pediatric Anesthesia Emergence Delirium (PAED) score were obtained and recorded by the researcher in the anaesthetic bay prior to the tonsillectomy commencing. Participants were randomised to deep or awake laryngeal mask removal in accordance with a pre-prepared randomisation schedule. Consecutively numbered envelopes containing ‘deep’ or ‘awake’ were opened by the researcher prior to the tonsillectomy and shown to the anaesthetist. Neither the anaesthetist nor the researcher were blinded to group allocation due to the nature of the intervention and the postoperative assessments.
To ensure buy-in from anaesthetists, and to maintain a real world perspective on anaesthesia options in this situation, specific methods of anaesthesia were left to individual treating anaesthetists, including premedication, induction, maintenance and analgesia. The child was induced according to the anaesthetist’s preference, but it was anticipated that this would most commonly be using inhalation anaesthesia (sevoflurane, with or without nitrous oxide). Opioids and other adjuncts administered during the surgery were at the discretion of the anaesthetist. Standard anaesthetic monitoring was applied. Emergency management of any intraoperative adverse events was at the discretion of the anaesthetist, and appropriate further management of the airway, as dictated by the clinical situation (e.g. endotracheal intubation), was allowed.
Upon completion of the tonsillectomy, after appropriate suctioning of the airway and regular respiration established, the child was placed in the left lateral position and the laryngeal mask removed in the operating theatre (in the deep group) or transported to the PACU with the laryngeal mask in situ (in the awake group). In the latter group, the laryngeal mask was removed by the PACU nurse upon meeting certain recovery criteria such as eye opening, facial grimace or purposeful arm movements. Any complications that occurred in the PACU, such as airway obstruction, were managed by the PACU nurse and/or anaesthetist. Medications administered, if any, by the PACU nurse for emergence delirium and/or pain relief were at the discretion of the anaesthetist and nurse in charge. PAED scores were obtained 5 and 20 min after eye-opening, with emergence delirium being defined as a PAED score ≥10 at either timepoint. 28 Surgical details, including tonsillectomy technique, were recorded.
For vomiting to be listed as a complication, a subject had to eject some substance or matter from the mouth following a gag reflex (simply gagging on the airway whilst awakening was not considered a complication). Excessive salivation required three or more instances of suctioning with each instance separated by at least 30 s. Desaturation was defined as any instance of an oxygen saturation under 92%.
Based on an estimated emergence delirium incidence of 30%, and an anticipated reduction to 10%, a randomised study with a type 1 error rate of 5% and a power of 80% required 62 subjects in each group. We aimed to recruit 124 subjects. Randomisation was in permuted blocks with block sizes of 2, 4 and 6. These allocations were placed into sealed opaque envelopes by a member of the research team not involved with recruitment of subjects. Analysis involved a chi-square test to assess the primary outcome while logistic regression and chi-square tests were used to determine the effect of other factors on emergence delirium and the incidence of complications in the PACU. Analysis was by intention-to-treat. Statistical analyses were performed using IBM SPSS Statistics 26 (IBM Corp., Armonk, NY, USA).
Results
One hundred and twenty-five children were identified for possible inclusion in the study (Figure 1). Parent(s) of 124 children consented on behalf of their child to participate in the study. Sixty-two subjects were randomised to each group. Baseline characteristics were similar between groups (Table 1). All participants had documented snoring, and it is therefore likely that sleep-disordered breathing was the primary indication for most subjects, although it is uncommon for children at our institution to have had formal sleep studies. Additionally, around two-thirds in each group had recurrent tonsillitis. Three subjects did not receive their allocated treatment: one in the deep group and two in the awake group. In all children, general anaesthesia was induced and maintained with sevoflurane. Paracetamol was the only medication administered preoperatively; medications administered intraoperatively for analgesia and/or emergence delirium prevention were largely consistent between groups (Table 2).
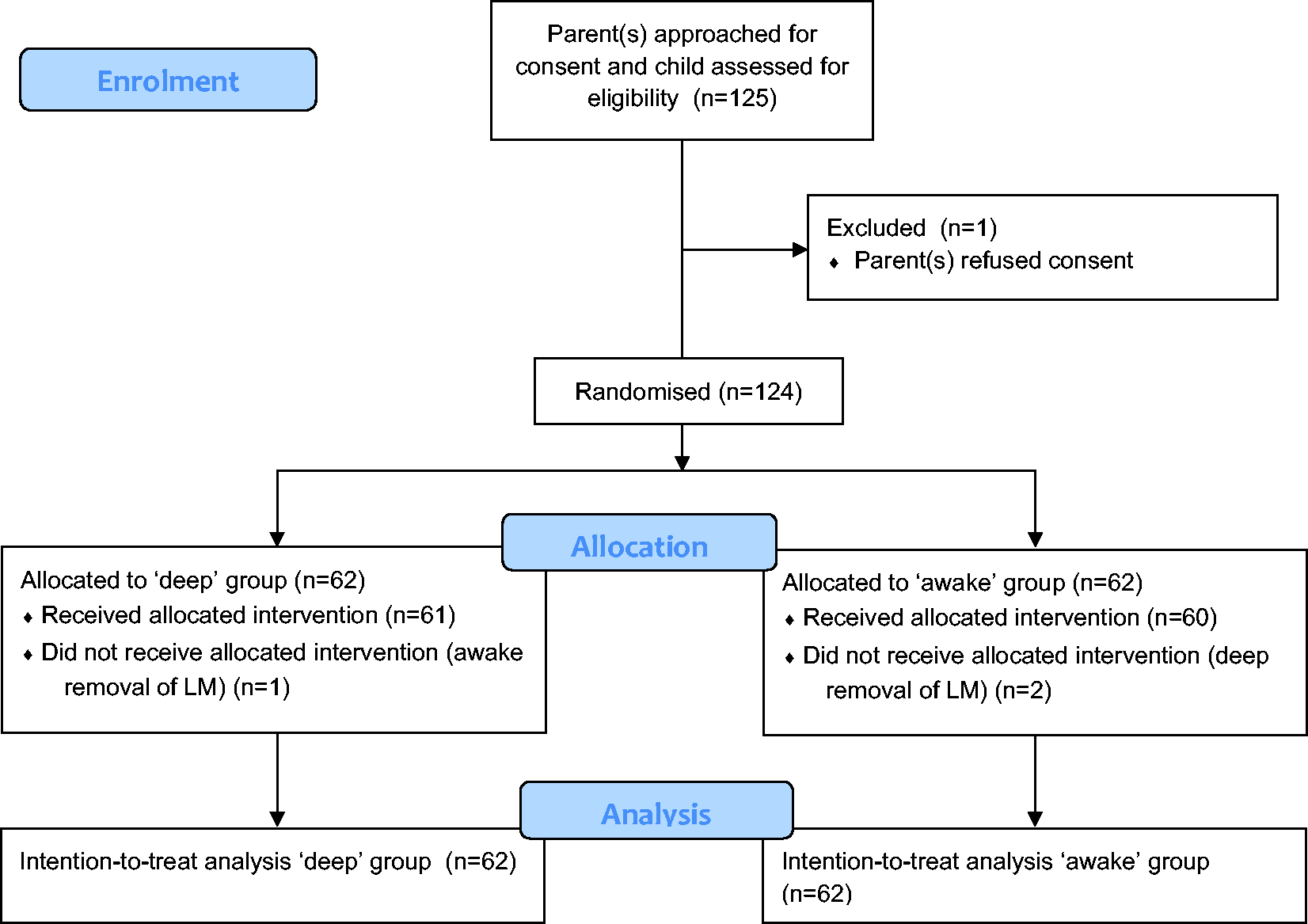
Flowchart depicting the randomisation process. An intention-to-treat principle was applied. LM: laryngeal mask.
Patient characteristics and surgical details.
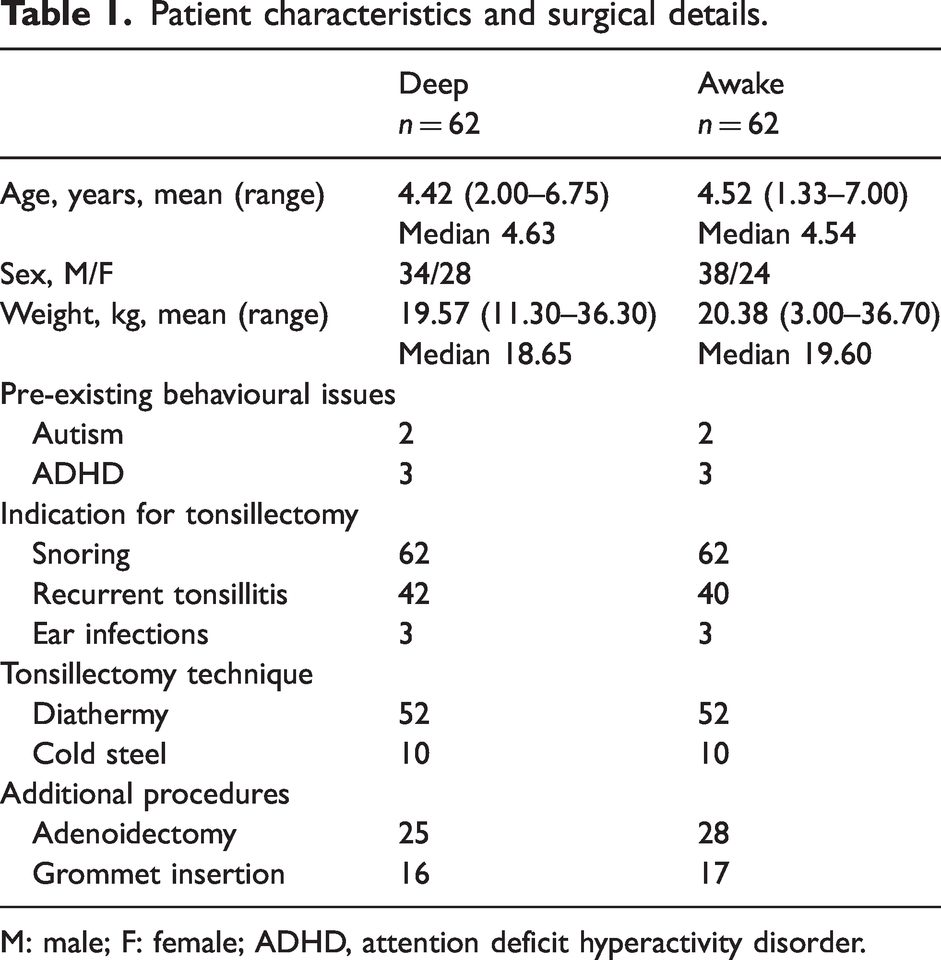
M: male; F: female; ADHD, attention deficit hyperactivity disorder.
Preoperative and intraoperative medications.
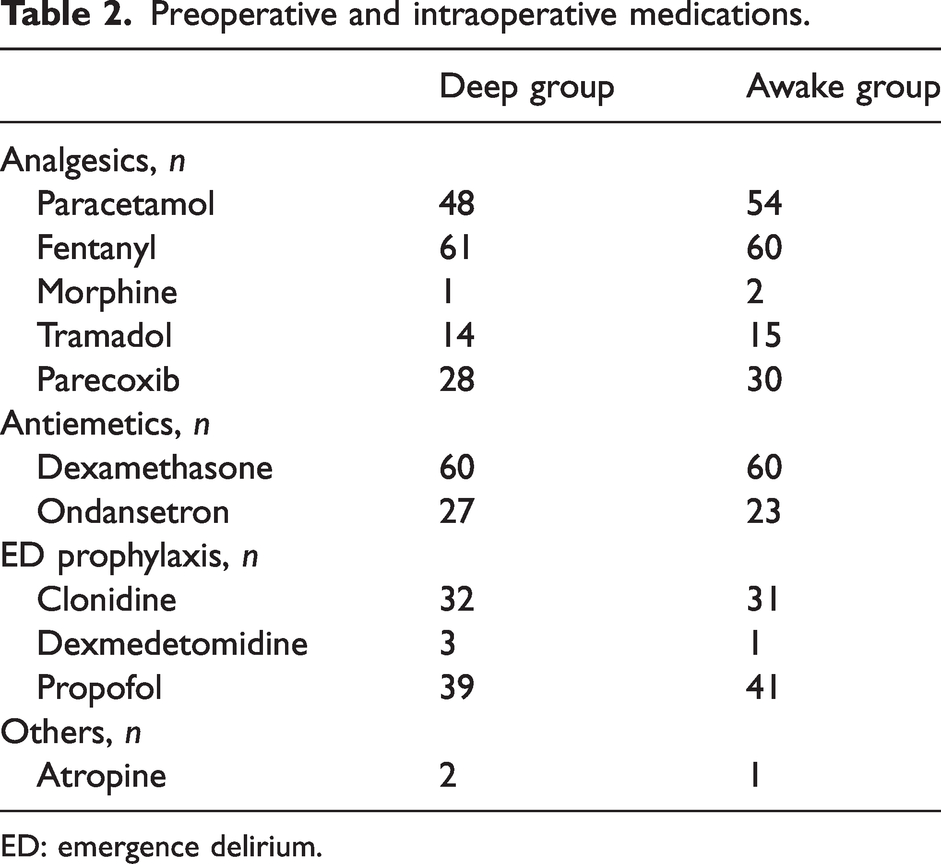
ED: emergence delirium.
Figure 2 depicts the proportion of patients experiencing emergence delirium at 5 and 20 min. At 5 min, deep (40/62 = 64.5%) versus awake (33/62 =53.2%) laryngeal mask removal had no statistically significant effect on the incidence of emergence delirium (chi-square statistic 1.63 (df: 1, P = 0.20), odds ratio (OR) 0.63 (95% confidence interval (CI) 0.30 to 1.29)). Similarly, at 20 min, no statistically significant difference in emergence delirium incidence was noted: deep 19/62 = 30.6%, awake 18/62 = 29.0% (chi-square statistic 0.39 (df: 1, P = 0.84), OR 0.93 (95% CI 0.43 to 2.00)). Thirty-two patients met the criteria for diagnosis of emergence delirium at both timepoints.
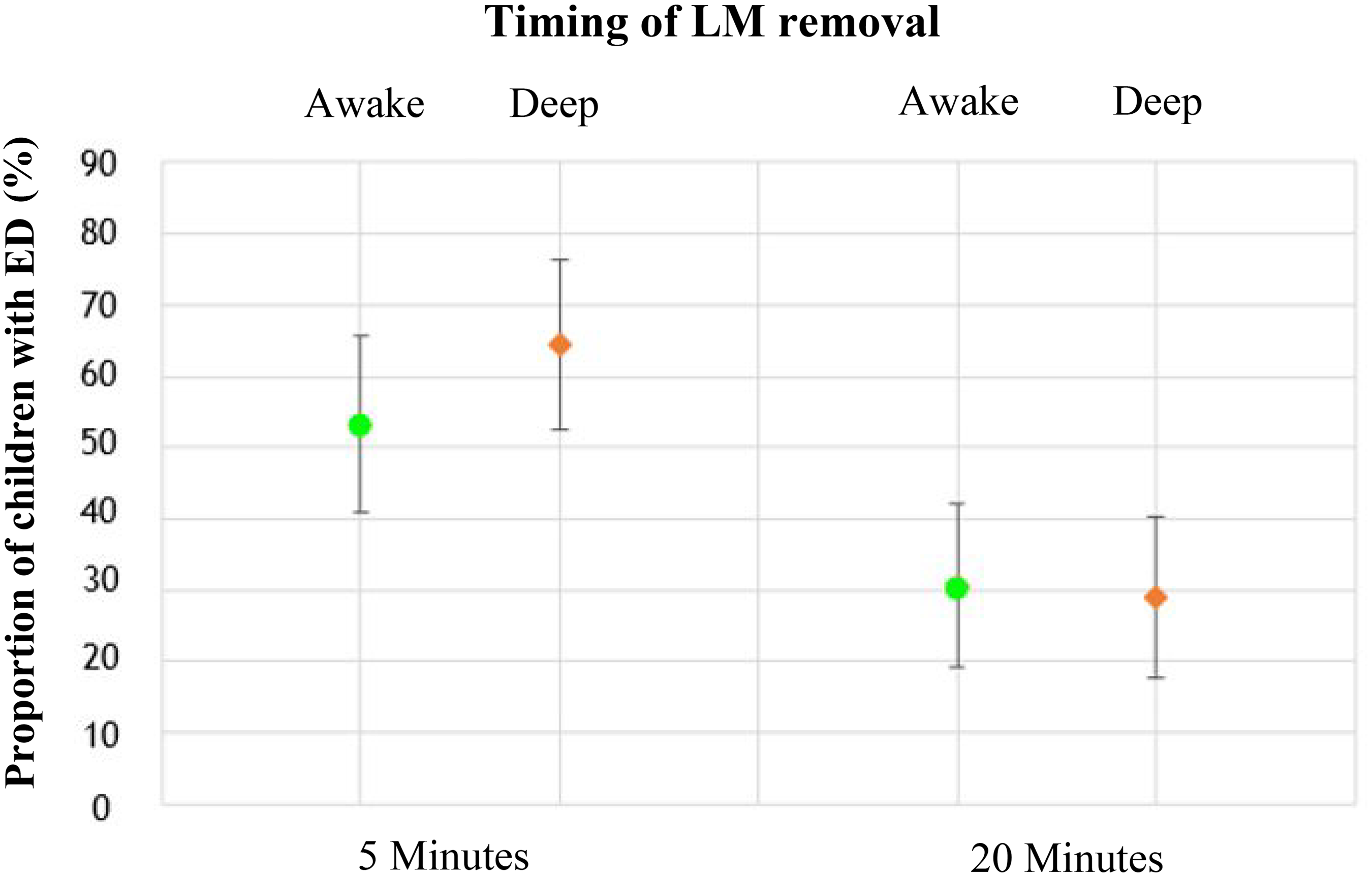
Proportion of subjects (and 95% confidence intervals) with emergence delirium at 5 and 20 min after eye-opening, by group. ED: emergence delirium; LM: laryngeal mask.
Postoperative complications are summarised in Table 3. Most complications were observed more frequently in children in the awake group: cough (24% awake vs. 8% deep), vomiting (8% awake vs. 0% deep), excessive salivation (23% awake vs. 8% deep) and oxygen desaturation (16% awake vs. 0% deep), although only oxygen desaturation was significantly different between groups after Bonferroni adjustment. There was no evidence of a difference in the incidence of laryngospasm between the groups, nor did any participants return to theatre from PACU for early haemorrhagic complications.
Post-anaesthesia care unit complications.
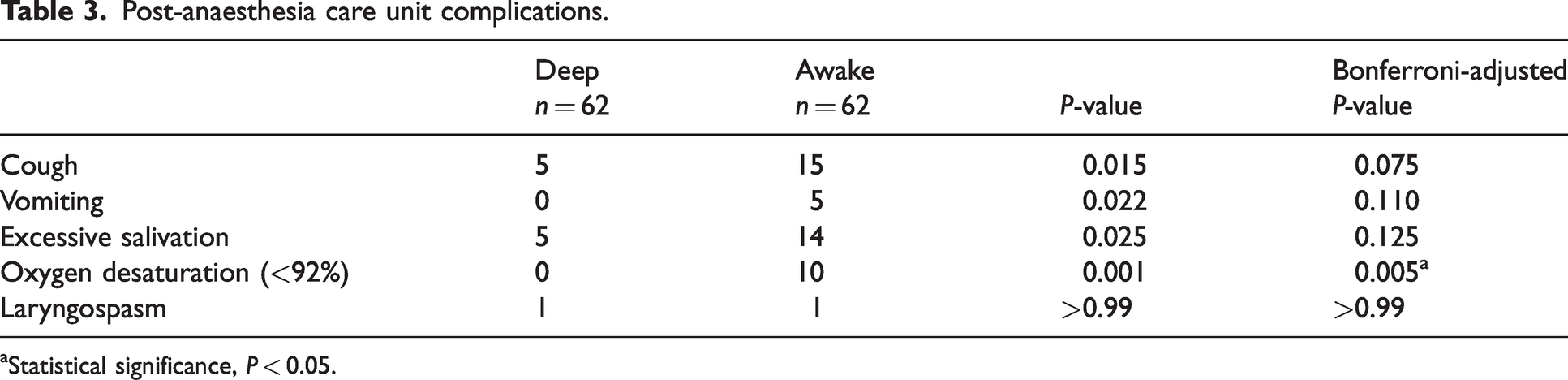
Statistical significance, P < 0.05.
No statistically significant relationship was observed between a specific medication and the incidence of emergence delirium at 5 or 20 min after eye opening after correcting for multiple testing (Table 4).
Effect of pre- and intraoperative medications on incidence of emergence delirium.
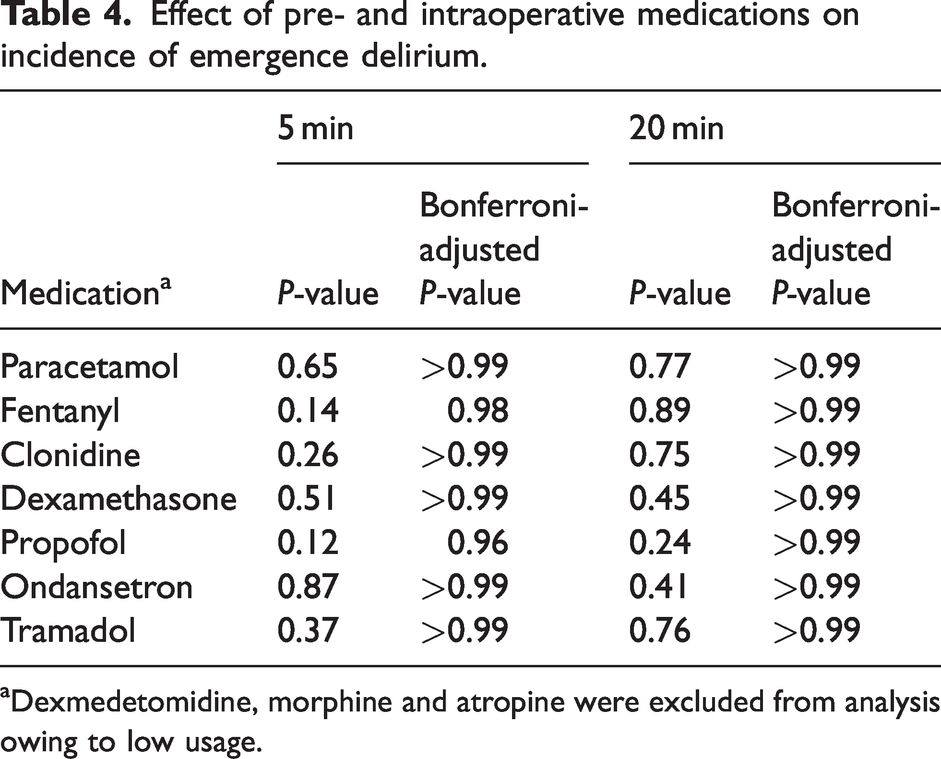
Dexmedetomidine, morphine and atropine were excluded from analysis owing to low usage.
A binary logistic regression analysis was performed to ascertain the effects of age, sex, weight and preoperative PAED score on the incidence of a child awakening with emergence delirium. At 5 min, there was no evidence for an effect of any of these variables on the incidence of emergence delirium, nor for sex and weight at 20 min. There was evidence for an effect of age, with an OR of 0.96 (95% CI 0.93 to 0.99) per month increase in age, and preoperative PAED score, with an OR of 1.19 (95% CI 1.01 to 1.40) per point increase in preoperative PAED score, on the incidence of emergence delirium at the 20 min timepoint (Table 5).
Odds ratios for the effect of variables on incidence of emergence delirium.
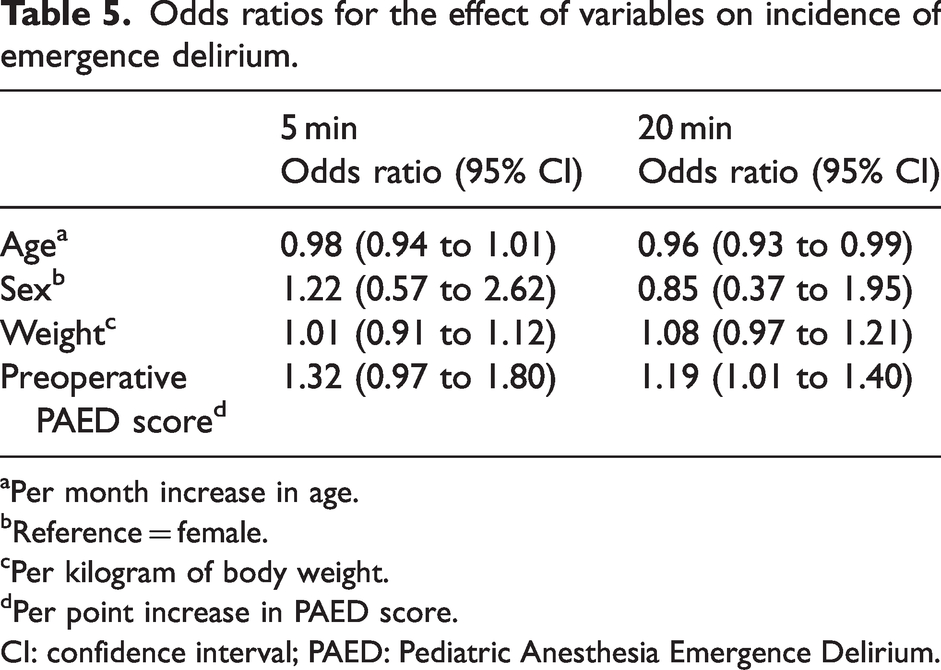
Per month increase in age.
Reference = female.
Per kilogram of body weight.
Per point increase in PAED score.
CI: confidence interval; PAED: Pediatric Anesthesia Emergence Delirium.
The only medication administered in PACU for distress in any child was fentanyl. Whether this was for postoperative pain or emergence delirium was not specifically recorded; 41 (66%) and 37 (60%) children were administered fentanyl in the deep and awake groups respectively. Average PACU doses of fentanyl were 0.46 µg/kg (deep) and 0.36 µg/kg (awake).
Discussion
This study demonstrated no significant difference in the incidence of emergence delirium in children after tonsillectomy whose laryngeal masks were removed deeply anaesthetised versus awake. At 20 min, the binary logistic regression model explained that increasing age was associated with a decline in the incidence of emergence delirium, which is consistent with established evidence that younger age is associated with a greater incidence of emergence delirium.5,28
Airway management has been studied previously with respect to emergence delirium incidence. Lee et al. 29 assessed whether deep removal of a laryngeal mask compared with awake or deep ETT extubation decreased the incidence of emergence agitation, noting that awake ETT extubation was associated with a higher risk. They did not, however, include an awake laryngeal mask removal group and noted this as a limitation of their study. Eshetie et al. 30 noted that in 153 patients aged two to nine years undergoing ophthalmic surgery, the incidence of emergence delirium was greater in children whose airway was managed with an ETT compared with those who had a laryngeal mask that was removed whilst deeply anaesthetised.
A greater incidence of complications was observed in our awake group relative to our deep group and this is akin to results from previous similar studies. One study reported an incidence of oxygen desaturation in their sevoflurane group of 15.9% upon removal of the laryngeal mask in an awake state. 31 This incidence is similar to that in our awake group, which demonstrated a 16% incidence of oxygen desaturation. In other studies of airway management in children undergoing general anaesthesia, complications such as cough, laryngospasm, oxygen desaturation and airway obstruction have been observed more often in awake airway removal groups, compared with deep airway removal groups, 32 although this has not been a universal finding.33,34 A meta-analysis of 17 studies noted that, in children, the timing of laryngeal mask removal made no difference to the incidence of cough, oxygen desaturation or laryngospasm. 35
There are several strengths and limitations in our study. In terms of strengths, our study assessed a population at high risk of developing emergence delirium, thus maximising case ascertainment. Particularly at 5 min, the incidence of emergence delirium was approximately 60%, which is higher than the incidence in many other studies and in previous work from our institution. 36 To measure emergence delirium in this study, we used the PAED scale, which is a well-recognised, validated instrument for diagnosing emergence delirium. Assigning a single member of our research team to score children on the scale will likely have decreased variability on this measure. Our higher-than-expected emergence delirium incidence could have been contributed to by the universal use of sevoflurane anaesthesia, 12 pain associated with tonsillectomy 10 or, indeed, other unexplained factors.
The lack of standardising anaesthetic technique in this study is an important limitation. While certain medications may increase or decrease the incidence of developing emergence delirium, this was not specifically controlled for. Of the medications administered in this study, no drug appeared to influence the incidence of emergence delirium. Nevertheless, the ‘real world’ approach of this study enhances its external validity. Another limitation occurred when our randomisation process was slightly compromised as one of the envelopes was misplaced from the envelope bundle but was eventually found and reintroduced into the study. Non-blinding of the data collector is a limitation although within the constraints of our departmental resources it was not possible to blind this role.
Observation of our study subjects was carried out only in the PACU, so it is possible that airway complications in the deep group could have occurred while subjects were under the care of the anaesthetist in the operating room prior to transfer to the PACU. Nevertheless, PACU complications are of greater clinical significance because the anaesthetist is likely to no longer be present, representing a greater risk to patients.
Time from sevoflurane discontinuation to eye-opening was not recorded in either group. Although we expect that this would have been similar between groups, we acknowledge that different sevoflurane washout times may have occurred between groups that could potentially have influenced occurrence of emergence delirium. Future research should consider including this measure.
Confounding clinical issues such as postoperative pain were also not specifically addressed in this study. It is well known that many of the reactions observed in children with emergence delirium are similar to those that might be observed in the setting of acute postoperative pain. We felt that using a single operation (tonsillectomy) should have limited the confounding effects of pain, although future studies should also consider assessing pain in postoperative subjects to allow differentiation of emergence delirium from pain, or utilising a clinical scenario that is unlikely to include pain as a confounder. 10
Conclusion
This study found no evidence that removing the laryngeal mask deep or awake yielded a clinically important difference in the incidence of emergence delirium after tonsillectomy in children. Although this provides reassurance that either technique is acceptable in the context of emergence delirium prevention, we did note an increase in the incidence of airway-related complications in the awake removal group. These secondary outcomes are exploratory and therefore not conclusive, but they are consistent with previous work exploring these complications in similar populations.
Footnotes
Author Contribution(s)
Acknowledgements
The authors would like to thank Dr Gordana Popovic for her guidance regarding statistical analysis, and Dr Barbara Robertson and the Albury Wodonga Health theatre staff for supporting this research.
Data sharing statement
Due to consent constraints, data sharing will not be available.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.