
Abstract
Preoperative assessment of functional capacity with the six-minute walk test (6MWT) allows for estimation of surgical risk and targeted triage to prehabilitation services. Patient with abdominal and pelvic cancers have worse preoperative function compared with the general population. However, six-minute walk distance (6MWD) reference values from cancer patients are unknown, which limits the interpretation of 6MWT in this population. This study aimed to establish an explanatory reference value model for preoperative 6MWD in patients with abdominal or pelvic cancers undergoing elective surgery. Adult patients undergoing surgery for abdominal or pelvic cancers at major international hospitals were included. The 6MWT was assessed before surgery using a standardised protocol. Anthropometric data including age, sex, height, weight and body mass index (BMI) were collected and included in multiple linear regression analysis to model preoperative 6MWD. A total of 742 patients were included. Age, height and BMI were correlated with 6MWD. Six regression models were estimated, including two from the entire cohort, two from the subset of males and two from the subset of females. A sex-neutral model was the most representative, explaining 15% of the variance in 6MWD (6MWD = 761.00–3.00 * Age (years) –2.86 * BMI (kg/m2) – 48.09 * Sex (M1, F2)). The explored regression models, using anthropometric variables, poorly explained the variance between measured and modelled 6MWD, which suggests that these models have no clinical utility in the cancer population. Consideration of additional, non-anthropometric variables may improve regression modelling of preoperative 6MWD in patients in abdominal and pelvic cancers.
Introduction
Preoperative assessment of functional capacity allows for estimation of surgical risk and targeted triage to prehabilitation services. The six-minute walk test (6MWT) is a performance-based measurement of functional capacity and reflects capacity to undertake activities of daily living.1 –3 6MWT is a metric of six-minute walk distance (6MWD) that can be useful for predicting perioperative outcome in the preoperative setting. The 6MWT is advantageous compared with cardiopulmonary exercise testing with cycle ergometry, as it is inexpensive, less time-consuming, requires minimal equipment and may better reflect the ability to undertake activities of daily living.1,3,4 It is also useful in elderly and frail populations, and in patients with debilitating chronic diseases who are unable to perform higher intensity tests such as maximal cycle ergometry. The utility of the 6MWT in measuring functional capacity has been demonstrated in patients with cancer in recent studies.5,6 Furthermore, these studies present evidence for association between preoperative performance in the 6MWT and postoperative outcomes.5 –7
Several studies have developed reference value models for 6MWD based only on anthropometric variables such as age, sex, height, weight, body mass index (BMI) and patient-reported outcomes.1,4,8 –13 These studies included healthy patients of different demographic subsets and patients with illnesses such as heart failure and respiratory disease. Reference value models have been used to determine normative values for 6MWD.5,6,14 Furthermore, in patients with chronic obstructive pulmonary disease, Andrianopoulos et al compared measured 6MWD against modelled 6MWD derived from several regression-based equations to determine the closest representative model for the population. 15 However, studies that propose a similar model in the cancer population are scarce.
Studies have shown that patients with abdominal or pelvic cancers perform worse on baseline 6MWT compared with the healthy population.5,6 Establishing a mathematical model of 6MWD that is representative of the cancer population is advantageous, because it enables comparison of 6MWD measured from the 6MWT against a population-based benchmark value to identify patients who may have suboptimal preoperative function and thus be at higher risk of complications and poorer postoperative outcomes. Identifying high-risk cancer patients based on modelled preoperative function prior to surgery may improve preoperative risk assessment, guide prehabilitation strategies and support perioperative clinical decision-making. Resources dedicated to preoperative optimisation strategies and postoperative destination planning can be better allocated towards patients who are deemed at high risk, which includes those with impaired functional capacity. For example, if an individual’s measured preoperative 6MWD lies below the 6MWD calculated from a population-based anthropometric model (based on the individual’s anthropometric characteristics), they can be appropriately triaged as at high perioperative risk requiring preoperative optimisation.
The aim of this international prospective cross-sectional study was to develop a population-based mathematical model of 6MWD utilising only anthropometric variables, in patients with abdominal or pelvic malignancies. Crucially, this was a modelling study only and does not evaluate accuracy of the modelled 6MWD for predicting postoperative outcomes.
Methods
Study design and ethics statement
This is an international prospective cross-sectional study of patients presenting with abdominal or pelvic malignancies who underwent the 6MWT before surgery at major referral centres. Data for this study were obtained from three separate research groups: Surgical Outcomes Research Centre (SOuRCe) at Royal Prince Alfred Hospital (Sydney, Australia), Peter MacCallum Cancer Centre (Melbourne, Australia) and an international consortium involved in the Measurement of Exercise Tolerance before Surgery (METS) study 16 that included 25 research centres across Australia, Canada, New Zealand and the United Kingdom that was coordinated at St Michael’s Hospital (Toronto, Canada). Ethics approval was obtained from the Sydney Local Health District Human Ethics Committee (2021/ETH01345). Ethics approval for the original METS study was obtained prior and included a clause for use of patient data in further substudies. 16 A Data Sharing Agreement was established between participating organisations (ID 21-0953-RPA). This study was designed in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.
Study population and variables
This study involved patients who were planned for surgical management for abdominal or pelvic malignancies and were assessed preoperatively with the 6MWT. Anthropometric variables including age (years), sex (male/female), height (metres), weight (kilograms) and BMI (kilograms per height in metres squared) were also collected from this population.
The population recruited at Royal Prince Alfred Hospital included 324 patients between the ages of 19 and 85 years who underwent either pelvic exenteration or cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (CRS-HIPEC) between 2017 and 2021.
The population recruited at Peter MacCallum Cancer Centre included 264 patients between the ages of 29 and 89 years who underwent pelvic exenteration, CRS-HIPEC or other surgeries for management of abdominal and pelvic malignancies, between 2019 and 2022.
The METS study 16 recruited 1723 participants aged 40 years or older who were scheduled for non-cardiac surgery. For this study, a subset of these patients who underwent the 6MWT preoperatively were included. This population consisted of a heterogeneous group of abdominal/pelvic, head and neck, thoracic, breast and plastic surgeries, and included both cancer and non-cancer populations. Of this population, 154 patients underwent abdominal and pelvic surgeries between 2013 and 2016 and were included in this study.
6MWT
Preoperative functional capacity was assessed using the 6MWT, which was conducted in accordance with the protocol published conjointly by the European Respiratory Society and the American Thoracic Society. 17 In brief, patients were instructed to walk as far as possible for 6 min up and down a 30 m straight, indoor corridor. Standard phrases were used for encouragement every 60 s. The total distance walked (measured in metres) and patient vital signs (blood pressure, heart rate and oxygen saturation) were recorded. A higher 6MWD indicated better functional capacity.
Statistical analysis
All statistical analyses were performed using GraphPad Prism (Version 9). Categorical data are expressed as frequency (percentage) and continuous data as median (interquartile range (IQR)). Multiple linear regression (least squares) analysis was performed with preoperative measured 6MWD as the dependent variable, and age, sex, height, weight and BMI as the independent variables. Being a binary variable, sex was coded as 1 representing males, and 2 representing females. In addition to sex being an independent variable in the model, separate regression analyses were performed in subgroups defined by sex (i.e. males versus females). The Pearson’s correlation coefficient (r) (or Point-Biserial Correlation) was used to determine the correlation between variables. Only independent variables that showed moderate or strong correlation with 6MWD were included in the multiple regression analysis. Furthermore, independent variables that showed a moderate to strong correlation between each other and thus failed to show independence were not included in the same model. Weakly correlated variables were still included in the regression modelling and were further assessed for multicollinearity. Since height and weight are components of BMI, they were not included in the same regression model. An r value >0 and ≤0.3 (or ≥–0.3 and <0) indicates a weak correlation, between >0.3 and ≤0.7 (or between <–0.3 and ≥–0.7) indicates a moderate correlation, and between >0.7 and ≤1 (or between <–0.7 and ≥–1) indicates a strong correlation. 18 Multicollinearity in the regression models was determined using the variance inflation factor (VIF), with a VIF less than 1.5 indicating homoscedasticity (or homogeneity of variances).
Results
Characteristics of the study sample
A total of 782 patients completed the 6MWT preoperatively, of whom 742 (94.88%) patients were scheduled for abdominal or pelvic surgeries. Patient characteristics are described in Table 1. Of this patient cohort, 324 (43.67%) patients were recruited from RPA Hospital, 264 (35.58%) patients from Peter MacCallum Cancer Centre and 154 (20.75%) patients from the METS collaboration. Within this cohort, 163 (21.97%) patients underwent pelvic extenteration surgery, 279 (37.60%) patients underwent CRS-HIPEC, and 300 (40.43%) patients underwent other abdominal or pelvic cancer surgeries. There was no statistically significant difference in the median preoperative 6MWD between the three centres (RPA Hospital (499 m (IQR, 145.00 m)), Peter MacCallum Cancer Centre (495 m (IQR 161.70 m)) and METS study (494 m (IQR 144.20 m)) (P = 0.22)). However, preoperative 6MWD was significantly higher in males compared with females (Table 1).
Patient characteristics.
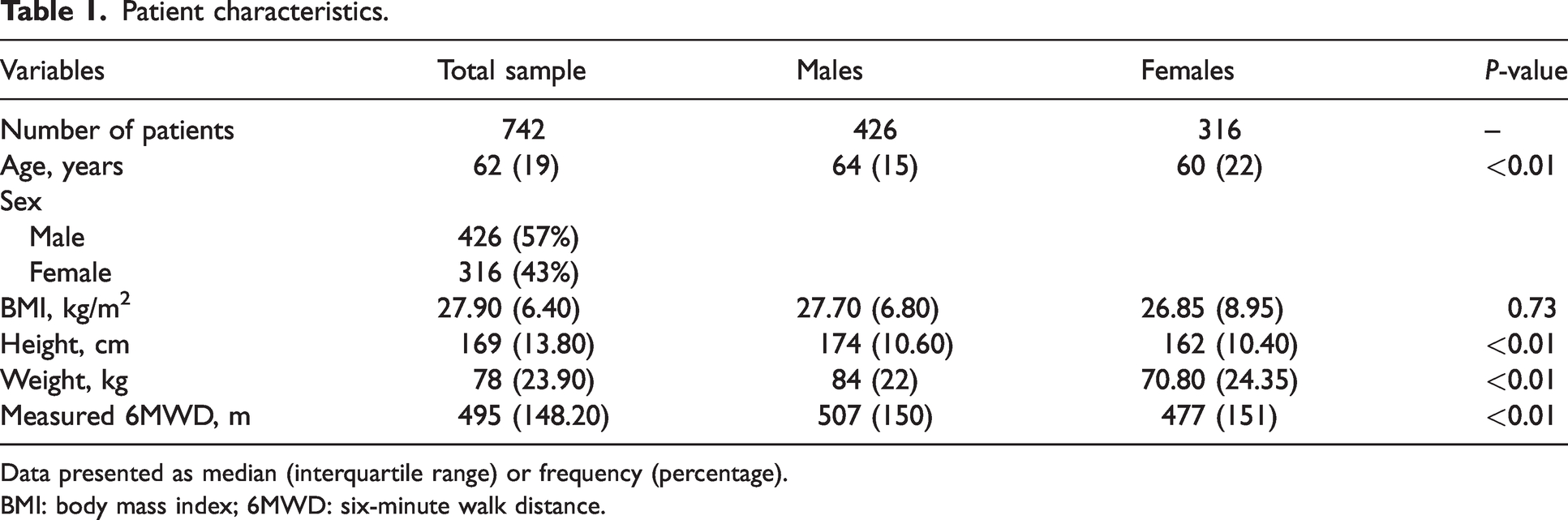
Data presented as median (interquartile range) or frequency (percentage).
BMI: body mass index; 6MWD: six-minute walk distance.
Correlation of variables
Correlation between the independent variables and preoperative measured 6MWD are presented in Supplementary material Table 1 (available on-line). Age (–0.29 (95% confidence interval (CI) −0.35 to −0.22)), sex (−0.15 (95% CI −0.22 to −0.08)), BMI (−0.15 (95% CI −0.22 to −0.08)) and height (0.19 (95% CI 0.12 to 0.26)) demonstrated weak correlations with preoperative measured 6MWD. Comparisons between anthropometric (independent) variables showed that male sex was weakly correlated with greater age (−0.18 (95% CI −0.24 to −0.11)) and weight (−0.29 (95% CI 0.35 to −0.22)) and moderately correlated with greater height (−0.63 (95% CI −0.67 to −0.58)).
The dataset was further subdivided based on sex for correlation analysis (Supplementary Table 2, available on-line). In males and females, preoperative measured 6MWD was moderately correlated with age (males: −0.34 (95% CI −0.42 to −0.26); females: −0.31 (95% CI −0.42 to −0.20)) and weakly correlated with BMI (males: −0.10 (95% CI −0.19 to −0.01); females: −0.21 (95% CI −0.31 to −0.10)), height (males: 0.12 (95% CI 0.02 to 0.21); females: 0.16 (95% CI 0.05 to 0.27)) and weight (males: −0.04 95% CI −0.14 to 0.05); females: −0.15 (95% CI −0.26 to −0.04)).
Multivariable linear regression models
In the entire dataset (i.e. including both males and females), independent variables sex and height showed moderate correlation (−0.63 (95% CI −0.67 to −0.58)) and failed to demonstrate independence. Therefore, these variables were not included in the same regression model. Weight was excluded from the regression analysis since it failed to show statistically significant correlation with preoperative measured 6MWD (−0.04 (95% CI −0.12 to 0.02)). Since height is a component of BMI, it was not included in the same regression model.
Given the outcomes of the correlation analyses, two multivariable linear regression models were estimated with the following independent variables: 1) age, sex and BMI, 2) age and height. The beta-coefficients, standard errors, 95% CI and VIF for the models are detailed in Table 2, and the summary of models is provided in Table 3. The independent variables accounted for 15% and 12% of the variance in the outcome 6MWD in models 1 and 2, respectively. The two models each demonstrated a VIF score of less than 1.50, suggesting that the assumption of homoscedasticity is valid across the models.
Regression coefficients, 95% confidence intervals, variance inflation factor and p-value of the linear regression model for the outcome preoperative six-minute walk distance.
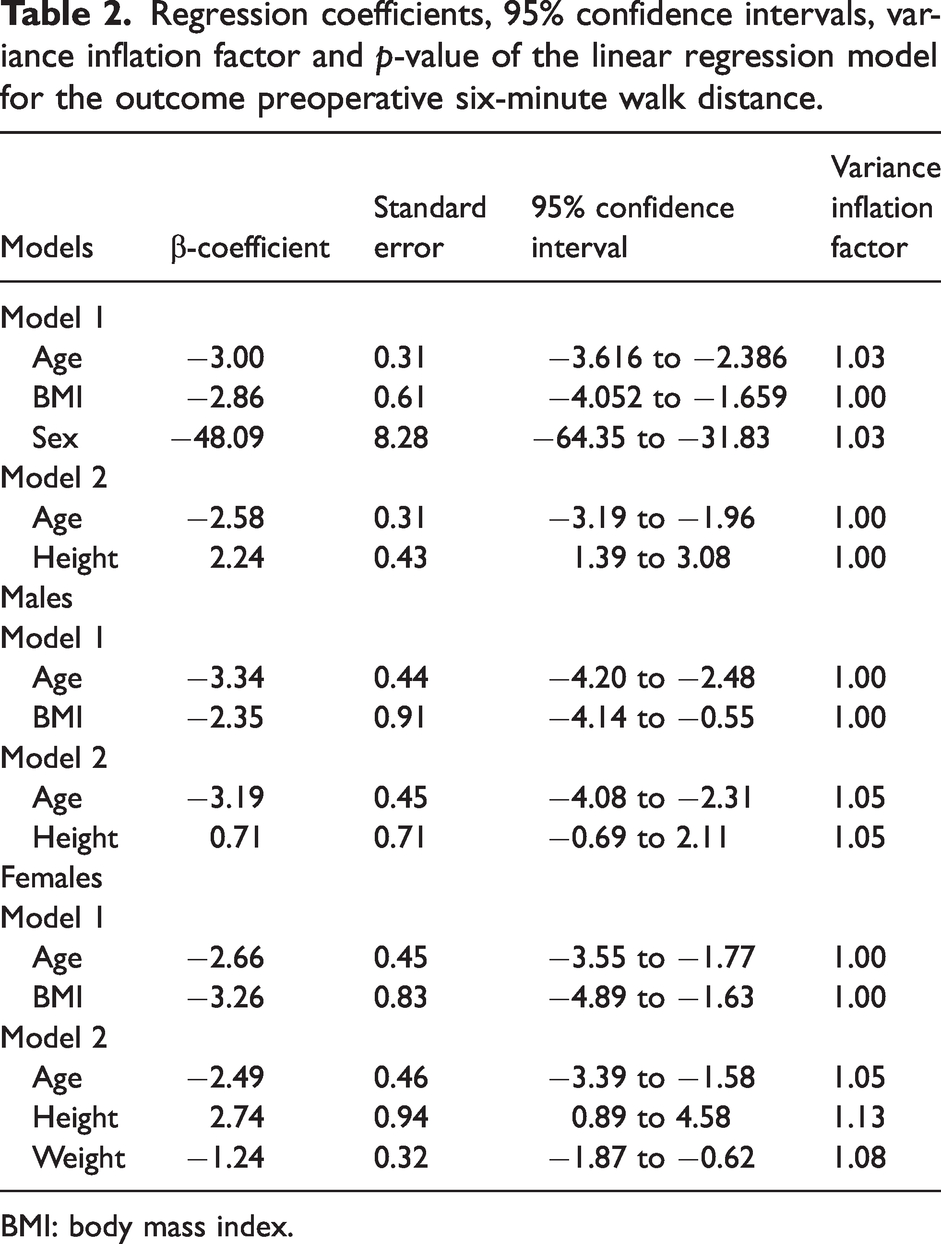
BMI: body mass index.
Summary of regression models.
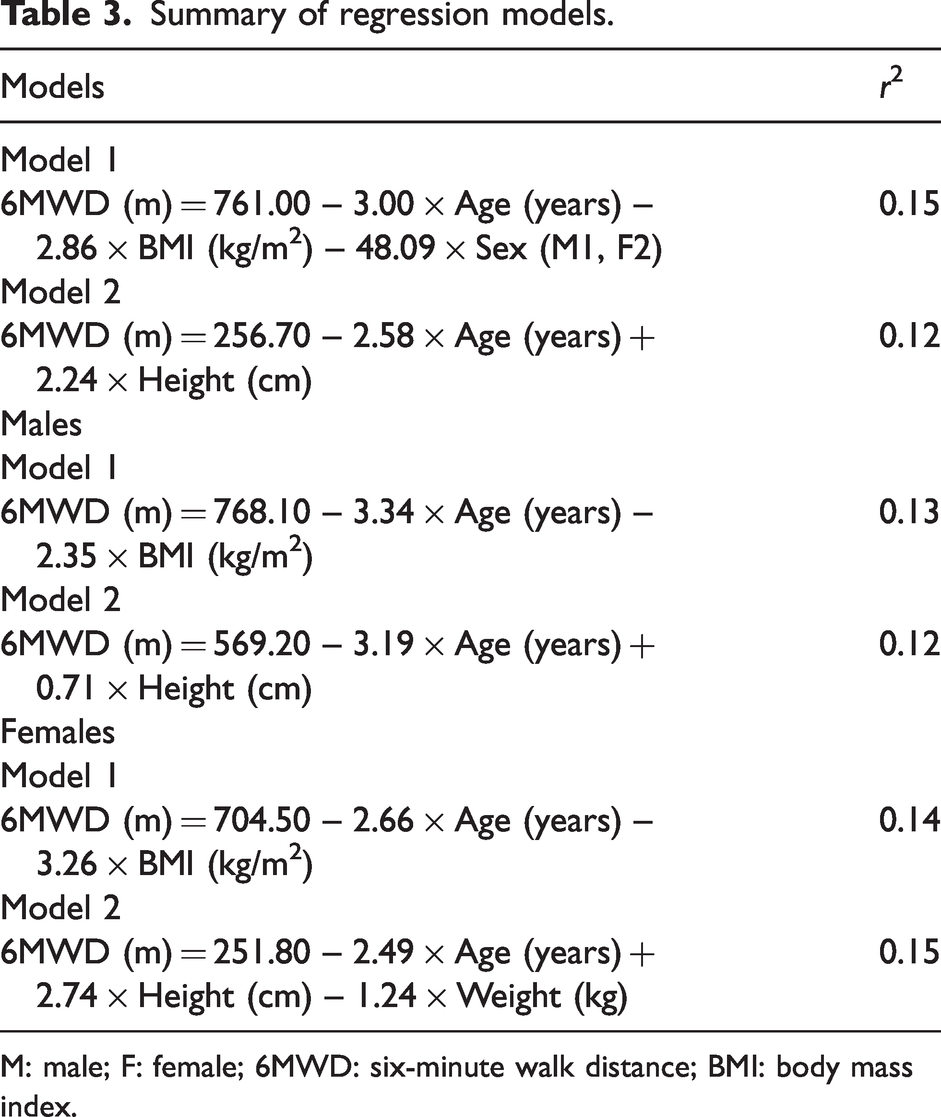
M: male; F: female; 6MWD: six-minute walk distance; BMI: body mass index.
In the sex stratified data, height and weight showed a moderately significant correlation in males (0.41 (95% CI 0.33 to 0.49)) and therefore were not included in the same regression models. Two models were trialled in multiple linear regression for males (model 1: age and BMI; model 2: age and height) and two models for females (model 1: age and BMI; model 2: age, height and weight) (Table 3). VIF in each model was less than 1.5, which was indicative of homoscedasticity (Table 2).
The independent variables accounted for 13% and 12% of the variation in male models 1 and 2, respectively, and 14% and 15% in female models 1 and 2, respectively (Table 3).
Comparisons of measured 6MWD and modelled 6MWD rendered from the regression equations are graphically shown in Figure 1. Whilst the median measured and modelled 6MWD are comparable, the range of the measured dataset is significantly greater than the model dataset.
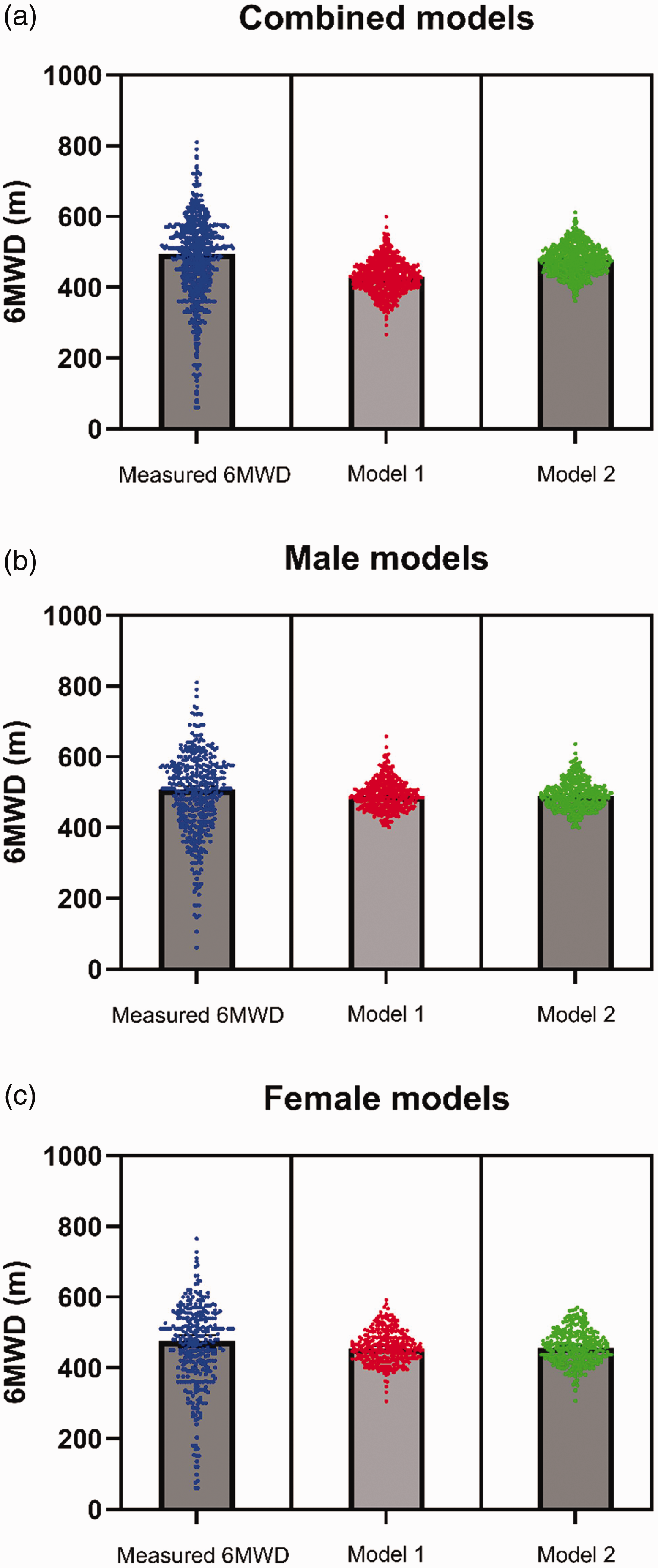
Comparison of measured six-minute walk distance (6MWD) and modelled 6MWD. Panel (a) shows a comparison between the measured 6MWD and modelled 6MWD derived from combined (sex-neutral) models 1 and 2 and 3. Panel (b) shows a comparison between measured 6MWD in males and modelled 6MWD from male-specific models 1 and 2 and Panel (c) compares measured 6MWD in females and modelled 6MWD from female models 1 and 2. Mathematical description of the individual models can be found in Table 3. Graphs show individual values superimposed on bar graphs depicting median.
Discussion
This international, multicentre, prospective cross-sectional study explored various reference value models based on anthropometric variables that are representative of preoperative 6MWD in patients with abdominal and pelvic malignancies. Based on regression modelling that best fit the available data, two models were proposed irrespective of sex, of which the model incorporating patient age, BMI and sex was better than the model based on age and height, accounting for 15% and 12% of the variance in 6MWD, respectively. Sex-based models were also trialled and found a model for female patients incorporating age, height and weight to be comparable to a sex-neutral model, and slightly better than the model incorporating age and BMI, accounting for 15% and 14% of the variance in preoperative 6MWD, respectively. However, male-specific models incorporating age and BMI, and age and height were inferior to female-specific and sex-neutral models. Given that the proposed models poorly explain the variance in 6MWD within the population, they are unlikely to offer clinical benefit and are inferior to other reported 6MWD anthropometric models.8 –11 Furthermore, the models presented in this study were not validated against postoperative outcomes, hence why this study does not propose thresholds for optimal 6MWD.
Notably in the sex-neutral model 1, an increase in age by one year accounted for a 3-m reduction in modelled 6MWD. With each additional 1 kg/m2 BMI, there was a reduction in modelled 6MWD by 2.86 m. In the female model involving age, height and weight, an additional 1 kg in weight contributed to a reduction in modelled 6MWD by 1.24 m, a reduction in height by 1 cm reduced the modelled 6MWD by 2.74 m, and for every one-year increase in age, the modelled 6MWD was reduced by 2.49 m. There are strong biological rationales for why age, height and BMI are correlated with 6MWD. Older populations have reduced skeletal mass and strength, which, combined with declining cardiorespiratory function, can result in lower functional capacity. A greater height is associated with a longer stride length and increased vital capacity, which offers a biomechanical advantage and contributes to better performance in the 6MWD. 19 Despite evidence suggesting that increased weight reduced 6MWD by increasing the workload of walking, 20 this study found a significant correlation between weight and measured 6MWD only in females. Rather, BMI and height were found to be a more consistent correlate of 6MWD. The reason for this is unclear; however, it may suggest that increased stride length conferred by taller height may have a greater contribution to 6MWD than weight. Furthermore, other measures of body size such as body surface area or fat percentage may better correlate with 6MWD than BMI or height and could be investigated in future studies.
Significant variability in modelled 6MWD exists across normative reference value studies,9 –11,21 –26 which is commonly explained by demographic and anthropometric differences in the sampled population as well as the variables included in the reference value model across various studies. One of the strengths of this study lies in the sample size, which is one of the largest reported in this study type spanning multiple recruitment centres and countries, reducing the likelihood of selection bias. This study also proposes multiple sex-neutral and sex-specific models using different variables, enabling clinicians and researchers to apply a specific reference value model based on the available anthropometric data. However, the variables included in the models could only account for 12% to 15% of the variance in 6MWD. This is further demonstrated in Figure 1, where the regression models, whilst being able to adequately represent the median, appear to under-represent the variability in the data, which suggests that anthropometric variables do not adequately account for the variability in the measured data from the cancer population.
Several other factors, such as type and stage of cancer, neoadjuvant treatment, specific timing of preoperative measurement, concurrent comorbidities, preoperative health and functional status (measured using American Society of Anesthesiologists physical status or Eastern Cooperative Oncology Group scores) and malnutrition, can impact preoperative 6MWD and may account for the variance in preoperative 6MWD. Inclusion of patient-reported outcomes of physical health may also improve modelling of preoperative 6MWD.
In the current population, males were significantly older and taller, which risks introducing bias into the sex-neutral regression models. In sex-specific regression modelling, the male model was proved inferior in that it accounted for only 12% to 13% of the variance in 6MWD. Indeed, sex-specific factors relating to malignancy and preoperative functional status may also contribute to the variance in 6MWD and these were not explored in the current modelling.
The variances of the regression models for preoperative 6MWD in the cancer population are relatively inferior to other models of preoperative 6MWD that report variances between 30% and 66%—albeit these are models of healthy individuals.11,13,20,23,26 This may reflect a skew in the measured data in the cancer population compared with the healthy population, which may complicate regression modelling based solely on anthropometric variables. Further validation is certainly needed against measured data in the abdominal and pelvic cancer population.
Owing to heterogeneity of the postoperative dataset, evaluating the association between measured and modelled preoperative 6MWD, and postoperative outcomes, and determining a population-based threshold for 6MWD was outside the scope of this study. However, this is certainly of interest for future studies. Therefore, the proposed models are not predictive of postoperative morbidity and serve as an adjunct to measured 6MWD. Given that the best anthropometric model accounts for only 15% of the variance in 6MWD, anthropometric models of preoperative 6WMD offer no clinical utility in the abdominal and pelvic cancer population.
Conclusion
In conclusion, this study suggests that, unlike in the healthy population, a mathematical model for 6MWD based on anthropometric values has no clinical utility in the abdominal and pelvic cancer population. As establishing normative preoperative 6MWD values in cancer patients may improve the evaluation of preoperative functional status prior to surgery and allow for targeted prehabilitation strategies to minimise postoperative morbidity, future studies should aim to improve the regression modelling with additional variables and assess diagnostic accuracy for adverse postoperative outcomes.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X241267907 - Supplemental material for Reference value models for predicting preoperative six-minute walk test in patients scheduled for abdominal and pelvic cancer surgery
Supplemental material, sj-pdf-1-aic-10.1177_0310057X241267907 for Reference value models for predicting preoperative six-minute walk test in patients scheduled for abdominal and pelvic cancer surgery by Preet GS Makker, Cherry Koh, Michael J Solomon, Nabila Ansari, Neil Pillinger, Linda Denehy, Bernhard Riedel, Lara Edbrooke, Jess Crowe, Duminda N Wijeysundera, Brian H Cuthbertson and Daniel Steffens in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.