
Abstract
The clinical and functional characteristics of patients with severe obesity who present for non-bariatric surgery have rarely been described. For this study, 293 such patients (mean body mass index 42 kg/m2) were investigated using their medical records, a 6-minute walk test, N-terminal pro B-type natriuretic peptide measurement, and the World Health Organization Disability Assessment Schedule 2.0 measure of disability. Cardiorespiratory disease and diabetes were common, with blood tests revealing a high probability of additional unexpected and undiagnosed renal and cardiac disease in a significant proportion of patients. One-third of patients had natriuretic peptide values that identify early left ventricular dysfunction in the community, with 16% above a value described as useful in predicting adverse outcomes for elective surgical patients. Only 10% of patients walked a distance within 10% of that predicted in six minutes, and 22% did not complete the test. Over one-third of patients (34%) had a clinically significant level of disability, with those unable to walk for six minutes describing higher levels of disability. Functional capacity as measured by the 6-minute walk test was significantly lower than would be expected from age, gender, and weight alone, and was related to age and degree of disability but not body mass index. We describe a severely obese population presenting for non-bariatric surgery who had significant levels of comorbid disease, functional impairment, and disability that were not apparent on routine preoperative assessment.
Introduction
Severe obesity, defined as a body mass index (BMI) greater than or equal to 35 kg/m2 with or without comorbidities, is becoming more common in Western society.1–3 Some 28% of Australian adults are obese, with the rate of severe obesity almost doubling from 4.9% to 9.4% over the last two decades.1,4 Patients with obesity regularly present for surgery. Local data from Wollongong, Australia, showed that 35% of our general surgical population was obese, with figures up to 55% for certain operations such as laparoscopic cholecystectomy. 5
Most patients with severe obesity will journey through a surgical episode with only minor problems, but some will experience serious events due to the severity of their obesity and underlying systemic diseases. While bariatric surgery patients have been well studied, the clinical characteristics of severely obese patients presenting for non-bariatric surgery have not been previously described.6–9
Traditional preoperative assessment considers the number of medical risk factors, assessment of functional capacity, and the degree of surgical insult.10,11 Functional capacity can be estimated in a number of ways. Although conventionally asked by anaesthetists, patient self-reported metabolic equivalents (METS) are not associated with objective measures of physical fitness and do not predict postoperative morbidity or mortality.12,13 Measures of exercise and activity are more useful. 12 The 6-minute walk test (6MWT) is a simple sub-maximal exercise test for evaluation of cardiorespiratory function that correlates well with cardiopulmonary exercise testing and functional capacity in healthy adults.14–16 Its performance in non-bariatric surgical patients with severe obesity has not been previously evaluated.
Recent work on preoperative assessment has highlighted the importance of biomarkers such as N-terminal pro B-type natriuretic peptide (NT-proBNP).12,17 Patient-centred measures such as level of disability are also becoming more prominent and can be reliably used to evaluate perioperative outcomes.18,19 The aim of this paper was to describe the characteristics of a cohort of patients with severe obesity presenting for non-bariatric surgery. Clinical characteristics (comorbidities, laboratory testing and plasma biomarkers), functional capacity, and disability were investigated.
Methods
We performed a prospective single-centre cohort study in Wollongong Hospital, New South Wales, Australia, in 2016–2018 to investigate the ability of the 6MWT to predict postoperative disability in surgical patients with severe obesity. Ethical approval was granted by the local regulatory body (HE15/379) and the trial was registered with the Australian New Zealand Clinical Trial Registry (ACTRN 12615001264572). This current paper presents the preoperative data. Wollongong Hospital is an outer metropolitan general tertiary hospital with 350 beds and 15 operating theatres, and performs approximately 13,000 operations per year of all types excluding cardiothoracic and complex paediatric procedures.
We recruited patients aged 18 years and older, undergoing any type of booked elective surgery, with a BMI of 35 kg/m2 and above as recorded at the pre-admission clinic (PAC). Exclusion criteria included inadequate time to complete the 6MWT, the presence of medical contraindications to the 6MWT, inability to understand study instructions because of language or any other cause, and individuals who were pregnant or undergoing only endoscopic procedures. All patients provided written informed consent prior to enrolment.
Background demographic and comorbidity data were obtained from the patient and the electronic health record. Height, weight, waist and hip circumference using hospital scales, a stadiometer and tape measure were measured on the day of PAC presentation. Routine biochemistry and haematology tests including serum bicarbonate and glucose (assumed to be a random glucose measurement) as well as NT-proBNP levels were collected by the pathology service at rest prior to exercise testing. Surgical severity scores were calculated using the Portsmouth – Physiological and Operative Severity Score for the enUmeration of Morbidity and mortality (P-POSSUM) definitions. 20
The 6MWT was performed in the PAC following standard guidelines. 21 A walking course with cones placed 30 m apart was set in a quiet corridor with markings every metre. Patients were accompanied as they performed the test and standard phrases of support were given. Patients were instructed to walk as fast as comfortably possible and were able to rest and to use walking aids if desired. The total distance walked at the end of six minutes, or earlier if the patient could not complete the time, was recorded as the final value. The distance predicted for the 6MWT was calculated using a published formula derived for an obese population that includes the variables of age, gender and BMI. 22
Patients completed the World Health Organization Disability Assessment Schedule 2.0 (WHODAS) in the PAC. 23 This questionnaire has been reported to provide highly acceptable, valid, and reliable measurement of disability-free survival after surgery and has also been used to measure disability in obese populations.18,24,25 The WHODAS consists of 12 items covering limitations over the previous 30 days in six major life domains: cognition, mobility, self-care, interpersonal relationships, work and household roles, and participation in society. Each item is scored from 0 (no difficulty) to 4 (extreme difficulty). The raw score out of 48 was converted to a percentage. A WHODAS score of greater than or equal to 25% is defined as clinically significant disability. 18
Continuous data were analysed using t-tests, analysis of variance, or Mann–Whitney U tests as appropriate. Proportions were compared using chi-square statistics or exact tests when the minimum cell frequency assumption was violated. Statistical analysis was conducted using SPSS (V 23 IBM Corp, Armonk, NY, USA). As this analysis was exploratory, power and sample size calculations were not performed.
Results
Participants
In total, 406 eligible individuals were approached for recruitment. Approximately 25% (111) declined and two patients were excluded after recruitment due to their booking for endoscopies. Therefore a total of 293 patients enrolled in the study over an 18-month period. Demographic data are shown in Table 1. Fifty-eight percent of the population were female. Most patients were classified as American Society of Anesthesiologists physical status 2 or 3 by the PAC anaesthetist: only 2% were in each of categories 1 and 4. Males were significantly heavier (P < 0.001) with a larger waist circumference (P < 0.001), whereas females had a higher mean hip circumference (P < 0.001). Some 21% of operations were classified as minor, 38% as moderate, 41% as major and one operation as complex major.
Demographic data of patients with body mass index ≥35 kg/m2 booked for elective non-bariatric surgery. Values are mean (standard deviation).

The range of surgery types included 31% orthopaedic surgery, 19% urology, 16% gynaecology, 15% general, 6% ear, nose and throat and maxillofacial, with smaller numbers of neurosurgery, vascular, colorectal, plastics, and other surgeries. The genders were roughly equally distributed except in urology and gynaecology procedures.
Comorbidities
The prevalence of recorded comorbid disease is described in Table 2. The most commonly recorded conditions were hypertension, diabetes, and obstructive airway disease.
Comorbidities. Percentages relate to the total cohort of 293 patients.
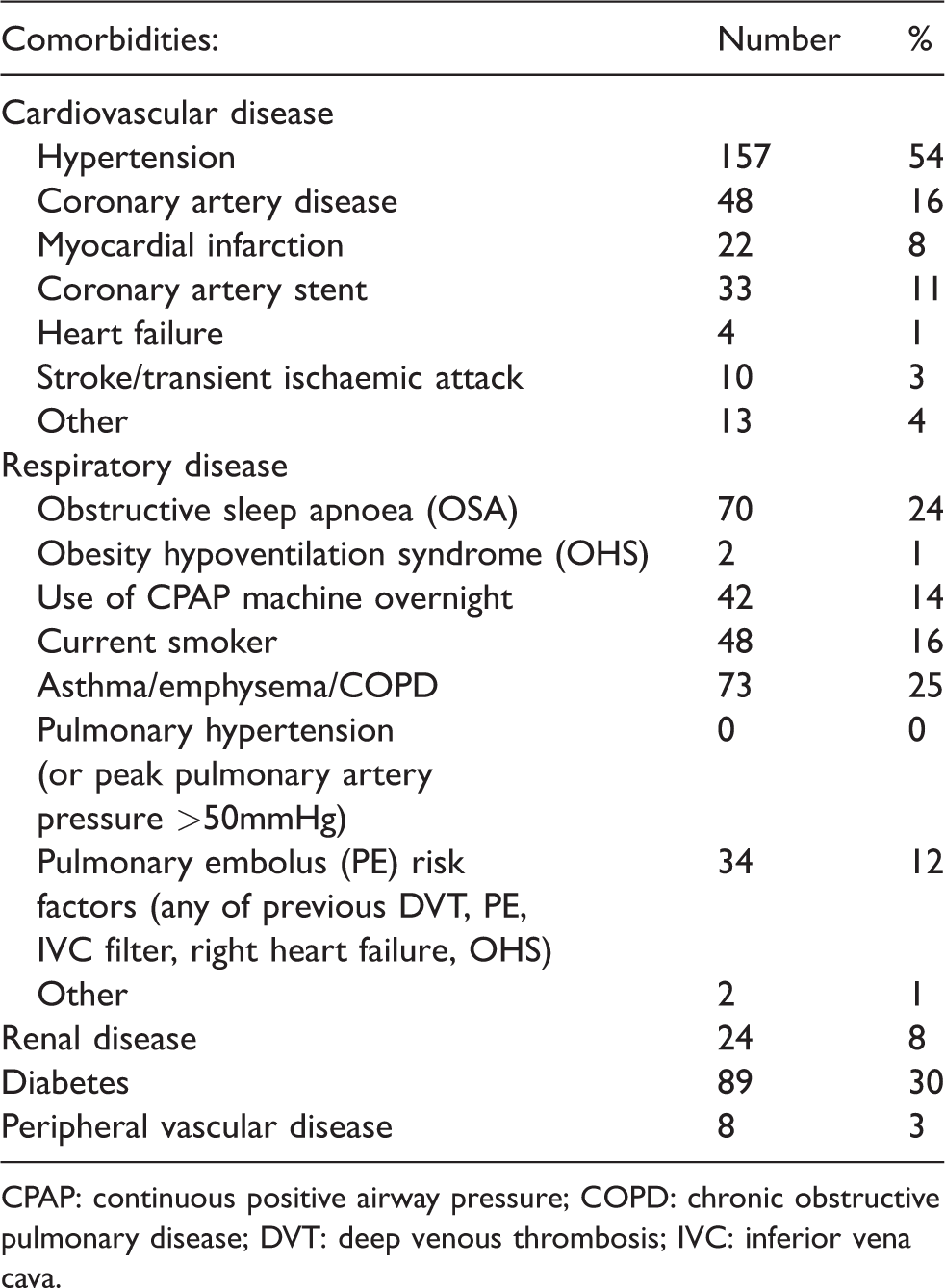
CPAP: continuous positive airway pressure; COPD: chronic obstructive pulmonary disease; DVT: deep venous thrombosis; IVC: inferior vena cava.
Functional capacity
A summary of the 6MWT results is shown in Table 3. The mean distance walked was shorter only in the highest BMI group (256 m compared with 332 m, P = 0.054 for distance between the highest and lowest BMI group, respectively) and was only significantly shorter in the over-70--year age group compared with those 70 years and under (226 m compared with 348 m, P < 0.001). However, a number of patients were unable to walk for the required six minutes. Nine patients were unable to walk even one lap (30 m) of the course and 55 completed more than one lap but stopped before six minutes. Therefore only 229 patients (78%) completed the full six minutes. Those who stopped early were significantly older than those who completed the test (mean age 66 y compared with 56 y, P < 0.001) but had similar BMIs (43 and 42 kg/m2, P = 0.5) (Tables 3 and 4). Patients who were unable to complete the 6MWT had higher levels of disability compared with those who completed the test (mean 31% compared with 16%, P < 0.001, Table 5). Only 10% of patients who completed the walking test (22/229) achieved a distance that was at least 90% of that predicted by the Capodaglio formula: the overall mean distance walked was 152 m lower than the predicted mean (380 m compared with 532 m, P < 0.001, Table 4). No adverse events occurred during this assessment.
Six-minute walk test summary results.
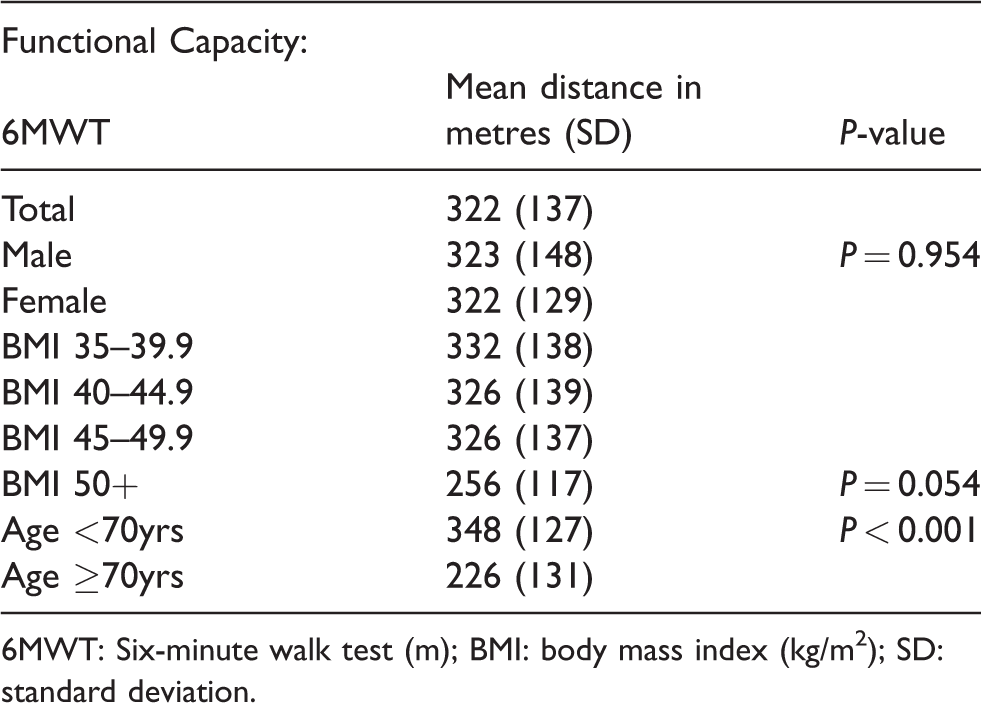
6MWT: Six-minute walk test (m); BMI: body mass index (kg/m2); SD: standard deviation.
Six-minute walk test distance by completion groups

6MWT: Six-minute walk test (m); BMI: body mass index.
World Health Organization Disability Assessment Schedule 2.0 scores.
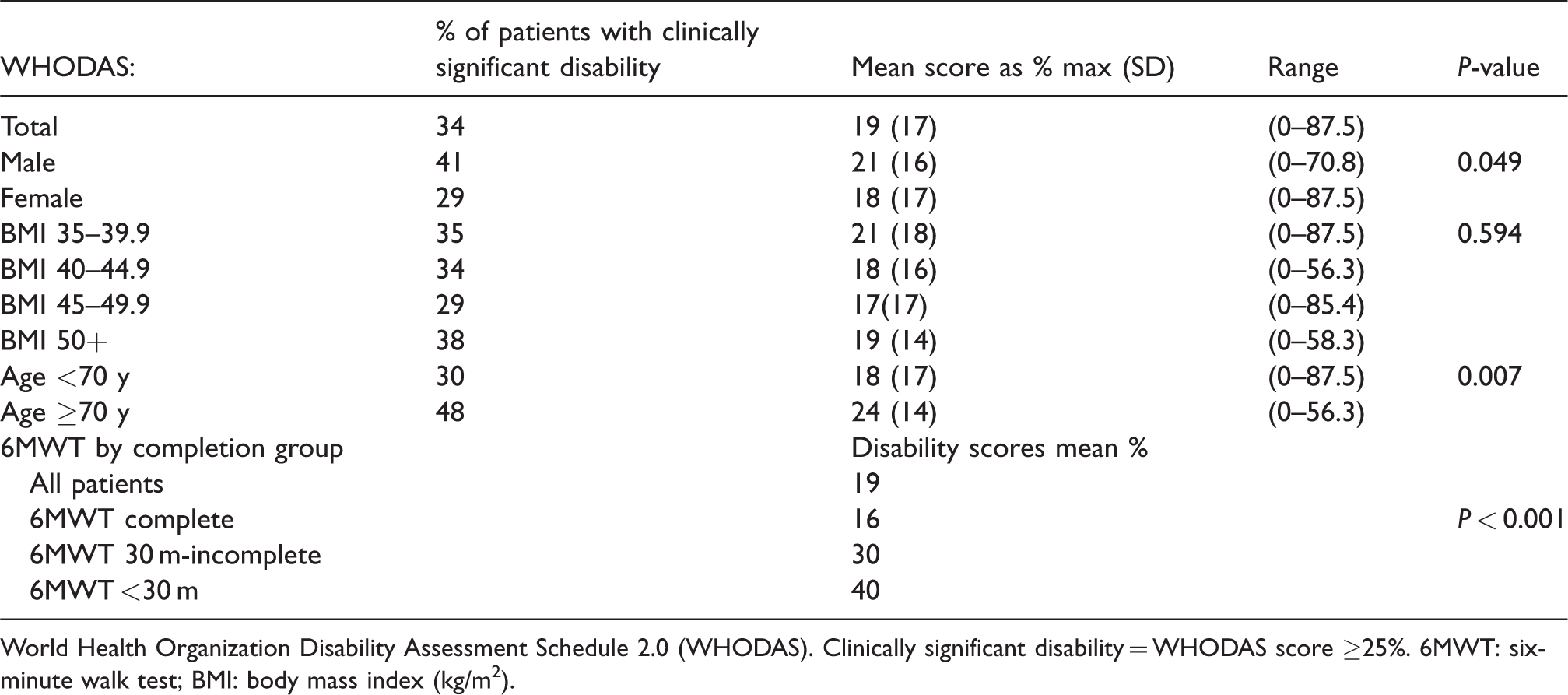
World Health Organization Disability Assessment Schedule 2.0 (WHODAS). Clinically significant disability = WHODAS score ≥25%. 6MWT: six-minute walk test; BMI: body mass index (kg/m2).
Most orthopaedic surgery patients in the study were booked for lower limb procedures. As mechanical and pain issues rather than cardiorespiratory function may have influenced their ability to walk for six minutes, results for this group were considered separately and compared with all other patients having non--lower limb orthopaedic surgery. The 79 patients booked for lower limb orthopaedic surgery were significantly older (mean age 64 y compared with 56 y: P < 0.001) than but had similar BMIs (mean BMI of 42 kg/m2 in both groups) to all other patients. More of the lower limb orthopaedic surgery patients stopped the test early (43% compared with 14%: P < 0.001), giving a lower overall mean distance walked of 244 m compared with 351 m (P < 0.001). Of those who completed the six minutes, the distance walked was similar (mean 344 m and mean 389 m, P = 0.423).
Disability
Of the patients, 99 (34%) had a clinically significant level of disability of ≥25% (Table 5). Their BMIs ranged from 35 to 63 kg/m2. Of these, 42% did not complete the 6MWT, a higher proportion than the overall sample figure of 22%. The patients who did complete the test from this higher disability group walked a similar mean distance to the overall sample who completed the test (326 compared with 322 m). Fourteen patients (5%) had a moderate or severe level of disability of ≥50%.
The mean sample score in the WHODAS of 19% fell in the range defined as mild disability (Table 5). Significant differences were seen in males compared with females but not between BMI groups. Increasing age was associated with a higher level of baseline disability (correlation r 0.256 P < 0.001). The range of scores overall and for each subgroup was large, from no to severe disability within each BMI range.
Biomarkers
Routine haematology and biochemistry were performed in approximately 95% of patients, with glucose levels recorded in 84% and NT-proBNP in 86%. Measures of renal function were most frequently abnormal (Table 6). An estimated glomerular filtration rate (eGFR) was documented for 278 patients, of whom 11% had a value of less than 60 and 8% less than 45 ml/min/1.73 m2. In 19 of these 33 patients, renal disease was not documented as present in the perioperative records. Seventeen percent of patients with abnormally high random blood glucose levels did not have a recorded diagnosis of diabetes. Only five patients in the whole cohort had a recorded HbA1C level, representing 6% of the 89 patients with known diabetes. Serum bicarbonate levels (HCO3), although not outside the normal laboratory range, were above a value of 27 mmol/l in 45 patients (16%).
Blood sample results.
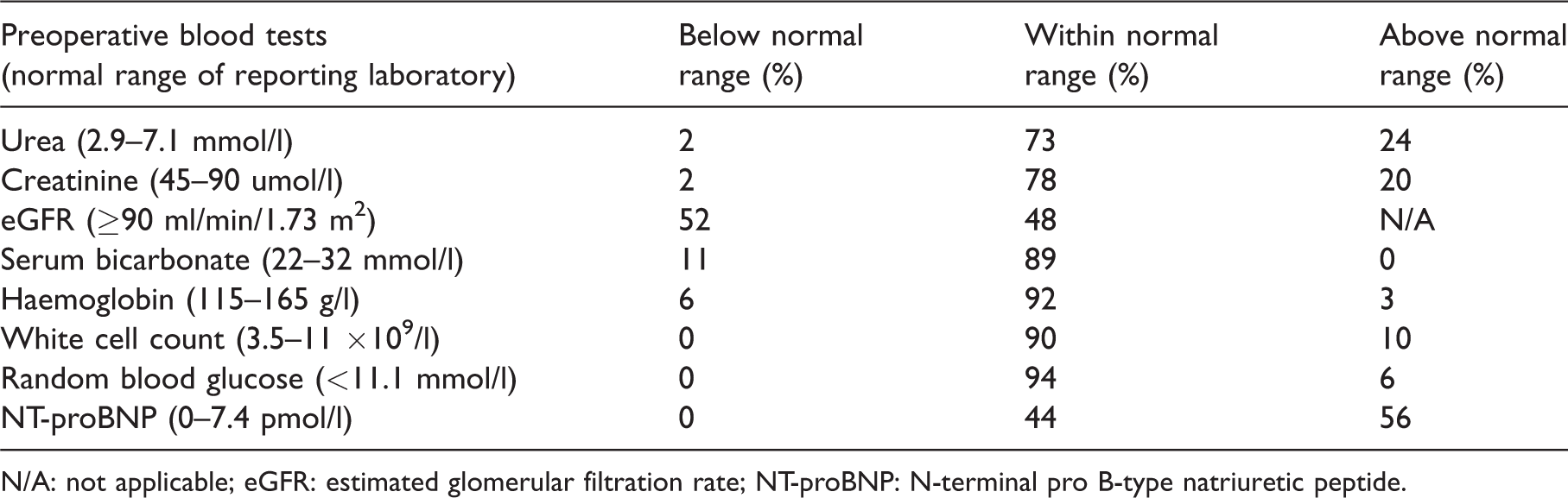
N/A: not applicable; eGFR: estimated glomerular filtration rate; NT-proBNP: N-terminal pro B-type natriuretic peptide.
There was a wide range of values for NT-proBNP (0.6–886 pmol/l, n=229). Patients with known cardiovascular disease had significantly higher mean levels than those without (37.3 vs. 12.8 pmol/l, P = 0.032) but no significant difference was found between BMI ranges. Seventy-four patients (32%) had a measurement above 14.8 pmol/l and 38 (16%) had a level above 36 pmol/l. Patients with clinically significant abnormalities in NT-proBNP, eGFR, and HCO3 had the same mean BMIs as those within the normal ranges for each parameter (all mean BMIs 42 or 43 kg/m2).
Discussion
This study provides a comprehensive description of the functional, clinical and biochemical characteristics of a group of patients with severe obesity presenting for routine, elective, non-bariatric surgery. Cardiorespiratory disease and diabetes were common, with biochemical tests revealing a high probability of additional undiagnosed renal and cardiac disease in a significant proportion of patients. Only 10% of patients walked a 6MWT distance within 10% of that predicted, and almost one-quarter did not complete the test. Functional capacity, measured by the 6MWT as an estimate of cardiorespiratory fitness, was significantly lower than would be expected from age, gender, and weight alone, and was related to age and degree of disability but not BMI. One-third of patients had a clinically significant level of disability, with those unable to walk for six minutes describing higher levels of disability.
Our patients displayed severe obesity. In addition to a mean BMI of 41 kg/m2 in men and 43 kg/m2 in women, all patients had significantly high waist circumference measurements. Waist circumferences greater than 102 cm in men and 88 cm in women have been shown to be associated with cardiovascular risk factors, health impairment, and reduced quality of life.26–28 All of our patients had measurements above these values, with the mean measurement in males being 30% above this upper limit, and 40% above in females. Our study cohort also represented a wide range of surgical practice, with 79% booked for moderate or major surgery.
Comorbidities
These 293 patients with severe obesity presented for elective non-bariatric surgery with a high burden of comorbid disease. Hypertension, obstructive airway disease, and diabetes were documented as present in up to a half of our patients (54%, 25%, and 30%, respectively). Few groups have reported the background prevalence of comorbidities in severely obese patients undergoing non-bariatric surgery. Our patients had higher rates of hypertension, pathological lung disease and diabetes than have been reported in one perioperative study of patients with mild obesity. 29 Our rates were closer to those in several studies in bariatric surgery populations that included patients with higher mean BMIs.7,30
Almost one-fifth of our patients with random blood glucose levels that met the criteria for diabetes were not formally diagnosed as having diabetes. Fasting blood sugars and HbA1C levels were rarely performed in our patients so we are unable to comment on the likely true underlying incidence of diabetes. One previous study of preoperative HbA1C screening in surgical patients found a rate of undiagnosed diabetes of 4%, with a further 23% considered to be at very high risk. 31 The mean BMIs in these patients ranged from 29 to 34 kg/m2. Our data also suggest that underlying undiagnosed diabetes may be more common than realised in surgical populations.
Despite only 8% of our patients presenting to PAC with a documented diagnosis of renal impairment, elevated urea and creatinine levels were present in more than twice this proportion and 52% had an eGFR below the normal limit. Kidney Health Australia notes that a single eGFR value of less than 60 ml/min/1.73 m2 identifies a degree of renal dysfunction described as Stage 3 clinically significant chronic kidney disease (https://kidney.org.au/your-kidneys/detect/kidney-disease/stages-of-chronic-kidney-disease); 11% of our population met this criterion, and 60% of these did not have renal disease documented in the preoperative records, including five of the nine patients with stage 4 and 5 kidney disease as defined by eGFR level. It is recommended that kidney health checks should be offered to individuals with the following high-risk indications: obesity, diabetes, hypertension, established cardiovascular disease, and smokers (https://kidney.org.au/health-professionals/detect/kidney-health-check). Our study sample met the first indication by definition, and at least one of these other risk factors was also present in 71%. Some individuals may have had known, diagnosed renal disease that was not recorded or mentioned to their anaesthetists. Other patients may not have been specifically investigated or diagnosed.
Obesity hypoventilation syndrome (OHS) is defined by the presence of obesity and daytime hypoventilation in the absence of a known cause. 32 Postoperative complications including respiratory and cardiac failure, intensive care unit (ICU) transfer, prolonged intubation, and prolonged ICU and hospital lengths of stay, are up to ten times more likely to occur in patients with OHS than in patients with obstructive sleep apnoea alone, who are already at increased risk. 33 In the absence of formal arterial blood gas analysis, a HCO3 level of above 27 mmol/l has been described as a surrogate measure of daytime hypoventilation in the diagnosis of OHS.32,34 Some 16% of the patients in our study met this criterion and all were obese, suggesting a potential diagnosis of OHS in this number despite it only being formally diagnosed in two patients. An increased awareness of potential OHS may allow anaesthetists to modify patient management plans to minimise the severe adverse postoperative outcomes.
An autopsy study found that obese people were 1.65 times more likely to have a major clinically unsuspected diagnosis that was related to death than normal or underweight individuals. 35 Our study supports the finding that patients with severe obesity may have a significant incidence of undiagnosed pathology such as diabetes, renal dysfunction, respiratory disease and early heart failure. The resource implications of specialist referral and ongoing management are likely to be outweighed by the potential savings of decreased postoperative adverse events and improved longer term health.
Function and disability
Our patients displayed a generally low level of functional capacity. In the 6MWT, only 10% walked a distance within 10% of that predicted by a standard formula that incorporated BMI, and could therefore be considered to have displayed a reasonable level of cardiorespiratory fitness. The mean distance walked by those who completed the test was 380 m. Examples of previously reported mean values include 475 m in females with an average BMI of 42 kg/m2, and 455 m in a mixed gender group with an average BMI of 37 kg/m2.8,36 Distances of around 600 m for individuals aged 20–50 years who were healthy and normal weight have been described. 37
We found that 22% of patients who consented to participate in this study were unable to walk for six minutes. All were booked to have elective surgery. Previous studies of the 6MWT in a variety of patient groups have not reported such a high level of non-completion. In most studies, all enrolled patients completed six minutes, even with medical conditions such as pulmonary hypertension, obesity and severe heart failure.8,22,36,38–40 Others note non-completion rates mainly around 5%.14,41,42 One study that considered both 6MWT and disability in non-surgical patients with BMIs of over 40 kg/m2 found non-completion rates of 17% in men and 30% in women. 43 Our relatively high non-completion rate may reflect the patients undergoing lower limb orthopaedic procedures or the number of patients aged over 70 years. The most likely explanations for the low 6MWT distance in our patients who did complete the test include the impact of severe obesity, significant disability, or the presence of a surgical condition on functional capacity.
Overall, only 7.5% of patients who enrolled in our study demonstrated a reasonable level of walking ability as measured by the 6MWT. Objective assessment of physical fitness is known to be more reliable than patients’ self-report.12,13 Inability to sustain exercise is important, as low levels of physical fitness are associated with higher rates of cardiovascular disease and cancer-related and all-cause mortality in the general population as well as postoperative complications in obese patients.44–49 Obesity independently impacts on cardiopulmonary dynamics and oxygen uptake. 50 Gait speed tends to decline with chronic disease, and is a strong independent predictor of disability, healthcare utilisation, nursing home admission and mortality. 51 The capacity to walk effectively and independently has been described as a central requirement for independent living. 52
Over one-third of our population (34%) met the criteria for clinically significant disability prior to surgery. This is higher than that reported in a general non-obese surgical population (27%) that included patients having cardiac, thoracic and emergency surgery. 18 Just over half of our patients were booked for minor or moderate surgery and would be expected to have a lower degree of disability than those undergoing the aforementioned procedures. Further data from a large cohort study of over 4000 patients from our group demonstrated that only 21% of surgical patients, with a mean BMI of 30 kg/m2, had clinically significant disability prior to surgery (unpublished data). Previous work has shown that patients with high BMI and waist circumference have impaired quality of life.24,28 Increasing BMI was not related to the degree of disability in our patients, as the range was wide and included no to severe disability within each BMI level. Disability may encompass attributes not due to physical size alone. Factors such as age, cardiorespiratory fitness, burden of comorbid disease, and social supports may be more important.
The 6MWT and preoperative WHODAS were strongly related to each other. Patients who were unable to complete the 6MWT had higher levels of disability as measured by the WHODAS than those who completed six minutes. The level of disability in those who walked for six minutes was mild and increased with decreasing walking ability. Donini et al. explored the relationship between obesity, 6MWT, and disability, and also found disability to be a strong predictor of 6MWT non-completion. 43 Functional capacity and disability are different constructs but may be related. Neither was associated with BMI, but both were associated with older age. Performing a 6MWT may be a feasible method to estimate disability in a preoperative setting. Conversely, if a 6MWT is not logistically possible, completing a WHODAS assessment may provide some degree of insight to underlying functional capacity.
Biomarkers
Over half of the NT-proBNP levels in these study patients were above the normal limit. Patients with cardiovascular disease had higher mean levels than those without, confirming the validity of the measure in this population. NT-proBNP levels were not associated with BMI, 6MWT, or WHODAS values. These data suggest that disability, lack of fitness or orthopaedic problems were more strongly associated with limitations in the 6MWT than cardiovascular disease in this cohort of patients. The data also support other literature suggesting that NT-proBNP may represent a different underlying construct than that measured by other tools, and that its addition may add value to combined risk models. 12
NT-proBNP has been described as ‘a useful screening tool in the nonacute and primary care settings for identification of incipient heart failure and asymptomatic left ventricular dysfunction’. 53 However, establishing a level that gives a high specificity and sensitivity for diagnosing cardiac disease is not straightforward. NT-proBNP is influenced by a number of factors including weight and renal function, and these may have been relevant in our patients.53,54 In cardiovascularly asymptomatic patients in the community, whom our study patients closely resembled, a cut-off value equivalent to 14.8 pmol/l is often used to identify the presence of mild or early left ventricular dysfunction.53,55 One-third of our study patients were above this threshold despite only 2% having a recorded diagnosis of heart failure. Other groups have found a cut-off value of around 36 pmol/l to be useful in predicting adverse outcomes for elective surgical patients.56,57 Some 16% of our study patients had levels above this figure. While none of these reports are specific to perioperative patients with severe obesity, our results suggest that an elevated NT-proBNP is commonly found in this population to a degree that is likely to be clinically significant.
Limitations
Twenty-five percent of eligible patients did not consent to participate in the study. This proportion is reasonable when compared with another recently reported study investigating measures of preoperative fitness that had a 25% enrolment rate. 12 It is also not unexpected that some patients with severe obesity may have declined to participate in a trial involving performance of an exercise measure. While several non-consenting patients had a BMI higher than the highest BMI in our cohort, the mean BMIs in our cohort and the non-consenting group were similar (42 and 43 kg/m2, respectively).
The single biochemical measurements made in this study were not able to definitively confirm disease diagnoses and we were not able to trace any follow-up of abnormal blood results. Our findings suggest only that further investigation would be recommended in many of our patients to meet the standards of a number of published guidelines.
This initial descriptive paper does not refer to the postoperative course of our patients, which will be reported in future stages of this study. Further work to elucidate the background incidence of undiagnosed comorbidities and appropriate investigation and management of functional limitations would allow for better preoperative optimisation in this population of high-risk patients.
Conclusion
To our knowledge, this is the most comprehensive report of the health status of patients with severe obesity presenting for a wide range of elective non-bariatric surgeries. Patients had a number of serious occult comorbidities that were not apparent on routine preoperative assessment. In particular, impaired left ventricular function, renal impairment, and OHS may be more prevalent than recognised.
The 6MWT and the WHODAS provided objective information about underlying physiology and function that was not directly related to either weight or BMI. Functional capacity was significantly lower than would be expected from age, gender, and weight alone, even considering a mechanical cause of impairment in some patients. Furthermore, patients had a higher rate of clinically significant disability than that described in non-obese populations.
Patients with severe obesity presenting for surgery require careful preoperative evaluation, as relying only on patient self-report and written records means that anaesthetists could miss medical conditions of perioperative importance. A more detailed laboratory analysis with appropriate referral as well as consideration of functional capacity and disability may yield useful information that is not usually assessed. Our ongoing programme of research focuses on the ability of clinical and functional assessments to predict adverse clinical outcomes in the severely obese population.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by a project grant from the Australian and New Zealand College of Anaesthetists (16/018). The authors do not have any other interests to declare.