
Abstract
Elective cardiac surgery accounts for a significant proportion of perioperative resource allocation in Australasia. Preoperative pulmonary function testing (PFT) is routinely undertaken in some centres to identify patients who may require prolonged ventilation and intensive care unit (ICU) stay, although there are currently no data supporting this practice. Routine PFT places a burden on respiratory diagnostic laboratories, is inconvenient to patients and may delay surgery. We aimed to identify whether PFT parameters identify patients requiring prolonged mechanical ventilation after elective cardiac surgery. Adult patients admitted to the Royal Adelaide Hospital ICU following elective cardiac surgery between July 2013 and December 2017 were identified retrospectively from the local ICU database. Preoperative PFT and operative and postoperative outcome data were retrieved from local databases, and multivariable logistic regression was undertaken to identify which PFT variables were associated with prolonged mechanical ventilation. PFT data were available for 835/1139 (73%) elective cardiac surgical cases. The best independent predictors of prolonged mechanical ventilation were post-bronchodilator forced vital capacity (FVC) and single-breath diffusing capacity for carbon monoxide (DLCO). Patients with FVC <80% predicted and DLCO <60% predicted had an odds ratio for prolonged postoperative ventilation of 7.5 (95% confidence intervals 3.6–15.6; P < 0.001). The area under the receiver operating characteristic curve derived from this model was 0.68. Abnormal PFT results were associated with prolonged postoperative mechanical ventilation. A PFT-based prediction tool does not accurately predict individual patient outcome but identifies a cohort of patients at higher risk of requiring prolonged ventilation, potentially informing ICU resource allocation and surgical planning.
Keywords
Introduction
Between 2013 and 2017, approximately 32,000 patients underwent elective cardiac surgery in Australia, most of whom required postoperative intensive care unit (ICU) support. 1 Cardiac surgery exerts considerable occupancy pressure on ICUs. Equally, a lack of ICU bed availability may lead to cancellation of elective surgery and a waste of valuable theatre, surgical and anaesthetic resources. Successful theatre planning requires consideration of available data that might assist with predicting ICU length of stay (LOS) and bed occupancy. Prolonged ICU LOS can result from postoperative respiratory failure and a requirement for extended ventilation which occurs more frequently in patients with pre-existing lung disease.2–4 Cardiovascular risk factors and respiratory disease coexist, such that a large proportion of patients undergoing cardiac surgery will have underlying compromised pulmonary function. The importance of the association between pulmonary function and cardiac surgical outcomes is underscored by the prognostic value of chronic lung disease evaluation in the Society of Thoracic Surgeons (STS) and EuroSCORE II operative mortality prediction tools.5–9 Reduced diffusing capacity for carbon monoxide (DLCO) has also been associated with poor outcome following cardiac surgery. 10 In addition, population studies have identified an independent association between the presence and severity of chronic obstructive pulmonary disease (COPD) and arrhythmia. 11 Arrhythmias are common after cardiac surgery, promoting haemodynamic compromise and sometimes eliciting the need for anticoagulation. Data regarding the association between COPD and the risk of arrhythmia after cardiac surgery are inconsistent.
Some centres, including our institution, routinely undertake pulmonary function testing (PFT) for elective cardiac surgical patients to identify and quantify lung disease that might complicate anaesthesia and postoperative recovery. Evaluation of PFT results has identified that spirometry evidence of an obstructive ventilatory pattern may predict duration of mechanical ventilation and ICU LOS following elective cardiac surgery.12–14 Nevertheless, performing PFT commands resources, may involve the discomfort of arterial blood sampling and is inconvenient for patients. We undertook a retrospective study to test the hypotheses that in a contemporary Australian context, PFT could identify patients likely to require prolonged ventilation following elective cardiac surgery and identify which parameters were most closely associated with prolonged mechanical ventilation.
Methods
A retrospective, observational, single-centre study was undertaken investigating adult patients admitted to the Royal Adelaide Hospital ICU between July 2013 and December 2017 following elective cardiac surgery. Patients undergoing elective coronary artery bypass graft and/or valvular surgery who had undergone PFT (spirometry plus single breath DLCO and/or arterial blood gas analysis) within the six months prior to surgery were identified by cross-referencing the local Australian and New Zealand Intensive Care Society (ANZICS) Adult Patient Database and hospital PFT laboratory database. Surgical procedure and complication data were extracted from the Australian and New Zealand Society of Cardiac and Thoracic Surgeons (ANZSCTS) Cardiac Surgery Database. Spirometry, flow–volume curves and arterial blood gas analysis were undertaken in all patients using conventional methods.
Ethical approval was granted from the Royal Adelaide Hospital Research Ethics Committee (RAH HREC Approval no. R20180401).
The primary outcome was to determine which PFT parameters (spirometry, DLCO and/or arterial blood gas) best predicted the need for prolonged postoperative mechanical ventilation (defined as the fifth quintile of duration of ventilation, ≥18 hours) following elective cardiac surgery. Planned secondary outcomes included whether PFTs identify those patients requiring prolonged ICU or hospital LOS, and whether those with a diagnosis of COPD (diagnosed as post-bronchodilator forced expiratory volume in one second (FEV1) <80% of the predicted value in combination with an FEV1/forced vital capacity (FVC) <70% 15 as per Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria) or those with FEV1/FVC less than the lower limit of normal (according to the Australian and New Zealand Society of Respiratory Science using Global Lung Initiative (GLI) criteria 16 ) are at higher risk of developing postoperative arrhythmia or hospital-acquired pneumonia (defined by ANZSCTS criteria).
Discrete variables are summarised as number (%), and continuous variables as median (interquartile range (IQR)) or mean (standard deviation (SD)), with between group comparisons performed by chi-square, rank-sum or Student’s t-test as indicated. Logistic regression was conducted to identify covariates associated with prolonged ventilation. Covariates significant at P < 0.20 univariate were entered into a fixed-effects multivariable logistic regression model with ventilation hours as the dependent variable and retained at the 0.05 level to identify which variables are most predictive of the primary outcome. Collinearity was assessed by variance inflation factor and model fit by Akaike and Bayesian information criteria. Point estimates are presented as either odds ratios (OR) and corresponding 95% confidence intervals (95% CI), or as the population predicted probability as percentage (95% CI). A receiver operating characteristic curve was generated from these data, and area under the curve (AUROC) calculated. A two-tailed P-value of <0.05 was considered significant. Adjustment for multiple comparisons was not undertaken, as this was an exploratory study with preplanned outcomes. All analyses were performed using Stata v15.1 (StataCorp, College Station, TX, USA).
Results
Of the 1139 patients undergoing elective cardiac surgery identified from the local ANZICS database, 835 (73.3%) had undergone preoperative PFT; 746 spirometry, DLCO and blood gas analysis; 59 spirometry and DLCO; 28 spirometry and blood gas analysis; and two spirometry only. Baseline demographic and clinical data, subdivided by prolonged ventilation, are shown in Table 1. Overall median (IQR) duration of invasive mechanical ventilation was 9.1 hours (5.75–16.75 hours), and median (IQR) ICU LOS was 52 hours (30–96 hours). Mean PFT parameters for patients requiring ≥18 hours invasive ventilation are compared to those requiring ≤18 hours invasive mechanical ventilation (Table 2).
Demographic and clinical characteristics by duration of mechanical ventilation.
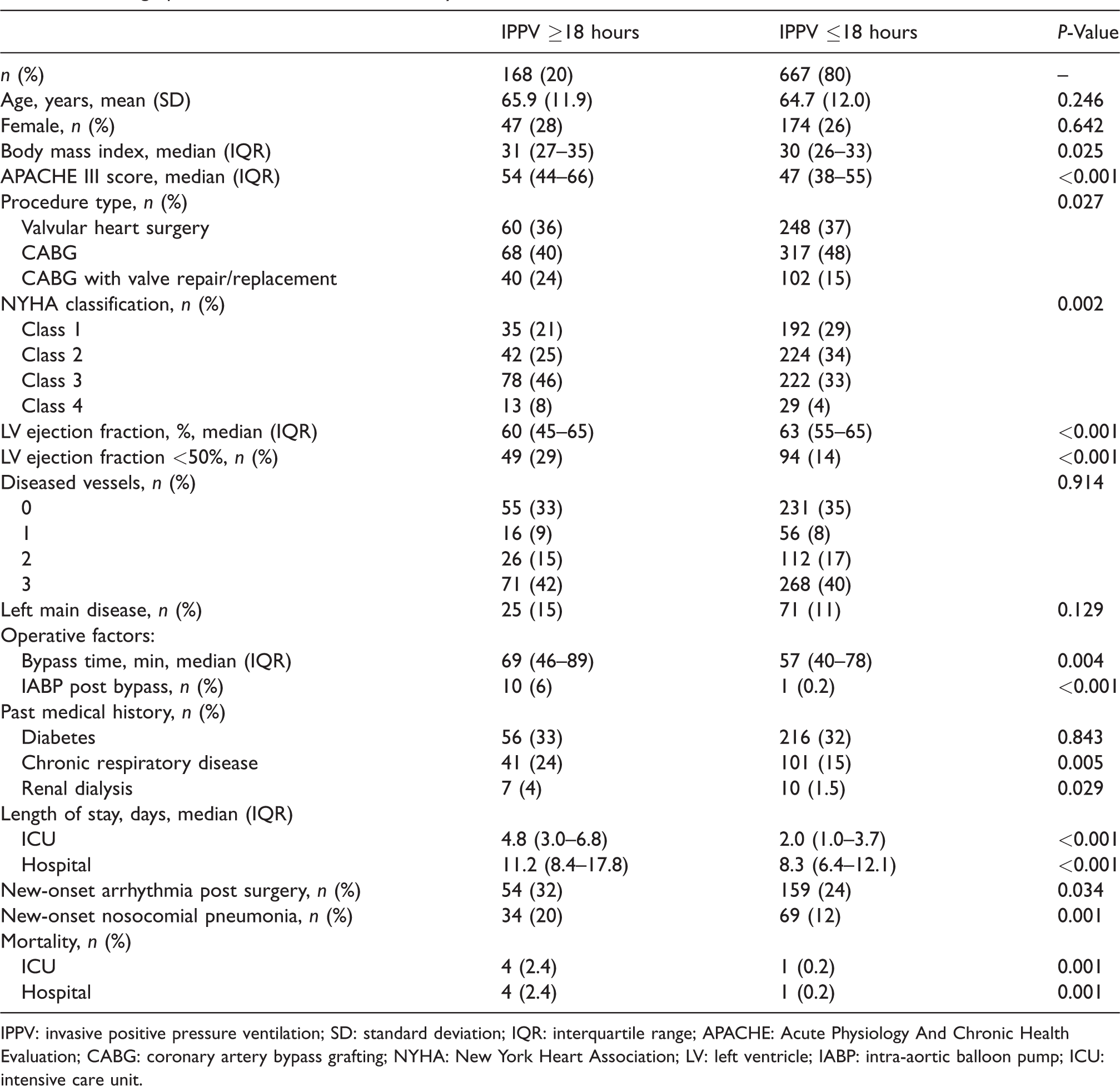
IPPV: invasive positive pressure ventilation; SD: standard deviation; IQR: interquartile range; APACHE: Acute Physiology And Chronic Health Evaluation; CABG: coronary artery bypass grafting; NYHA: New York Heart Association; LV: left ventricle; IABP: intra-aortic balloon pump; ICU: intensive care unit.
Pulmonary function test parameters according to patient group <18 hours versus ≥18 hours invasive positive pressure ventilation.
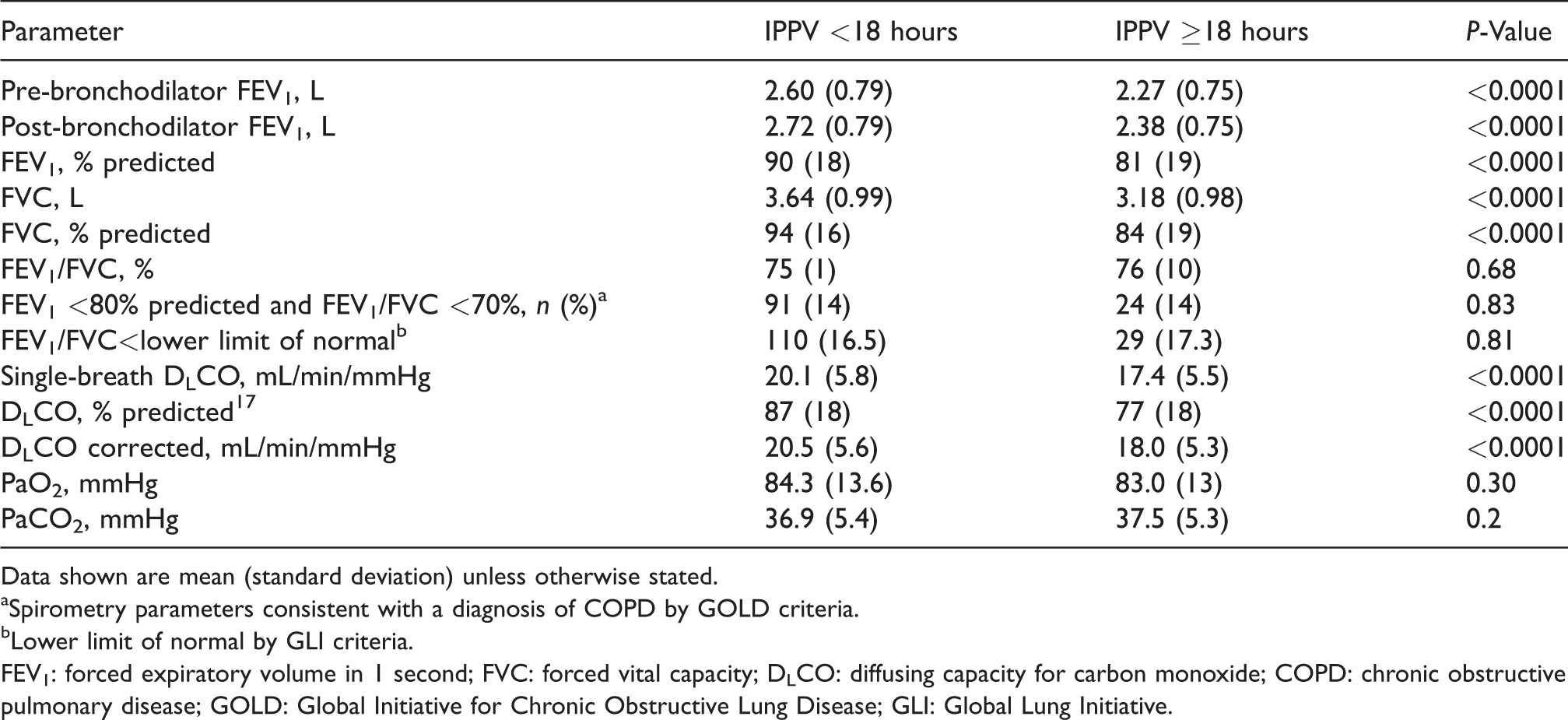
Data shown are mean (standard deviation) unless otherwise stated.
aSpirometry parameters consistent with a diagnosis of COPD by GOLD criteria.
bLower limit of normal by GLI criteria.
FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; DLCO: diffusing capacity for carbon monoxide; COPD: chronic obstructive pulmonary disease; GOLD: Global Initiative for Chronic Obstructive Lung Disease; GLI: Global Lung Initiative.
When undertaking regression analysis of PFT parameters a high level of collinearity was identified. The strongest independent predictors of prolonged postoperative ventilation (identified following the stepwise exchange process described above) are shown in Table 3. Patients with spirometry parameters consistent with a diagnosis of COPD were not more likely to develop hospital-acquired pneumonia or require prolonged ventilation or longer ICU admission.
Independent predictors of prolonged postoperative ventilation.
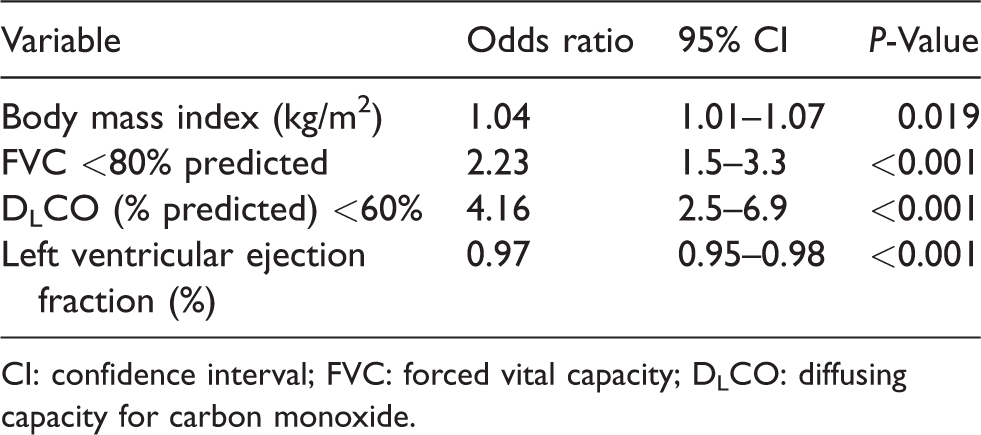
CI: confidence interval; FVC: forced vital capacity; DLCO: diffusing capacity for carbon monoxide.
Those patients with single-breath DLCO <60% predicted and FVC <80% predicted had an OR of 7.5 (IQR 3.6–15.6) for prolonged postoperative ventilation; 57% of these patients required prolonged postoperative ventilation compared to 19% for patients without both of these parameters (P < 0.001). The AUROC derived from this model was 0.68.
Patients with both FVC <80% predicted and DLCO <60% predicted were also more likely to require >48 hours in ICU (OR 2.73; IQR 1.2–6.2; P = 0.001). Seventy-five percent of this group needed >48 hours of ICU care compared to 57% for patients without both of these parameters (P < 0.001). Patients with both FVC <80% predicted and DLCO <60% predicted were not more likely to have longer hospital LOS.
Patients with spirometry parameters consistent with a diagnosis of COPD were more likely to develop postoperative arrhythmia. This association was significant for COPD defined by GOLD criteria (OR 1.86; IQR 1.23–2.82; P = 0.004) but not GLI criteria (OR 1.39; IQR 0.93–2.07; P = 0.1). Severity of expiratory flow obstruction, as measured by the forced expiratory ratio (FER) of the percent predicted FEV1 and FVC, was independently associated with the occurrence of postoperative arrhythmia with an OR of 0.80 (IQR 0.68–0.94; P = 0.007) for every 10% increase in FER. The observed proportion of patients experiencing an arrhythmia as FER% varied is shown in Figure 1.
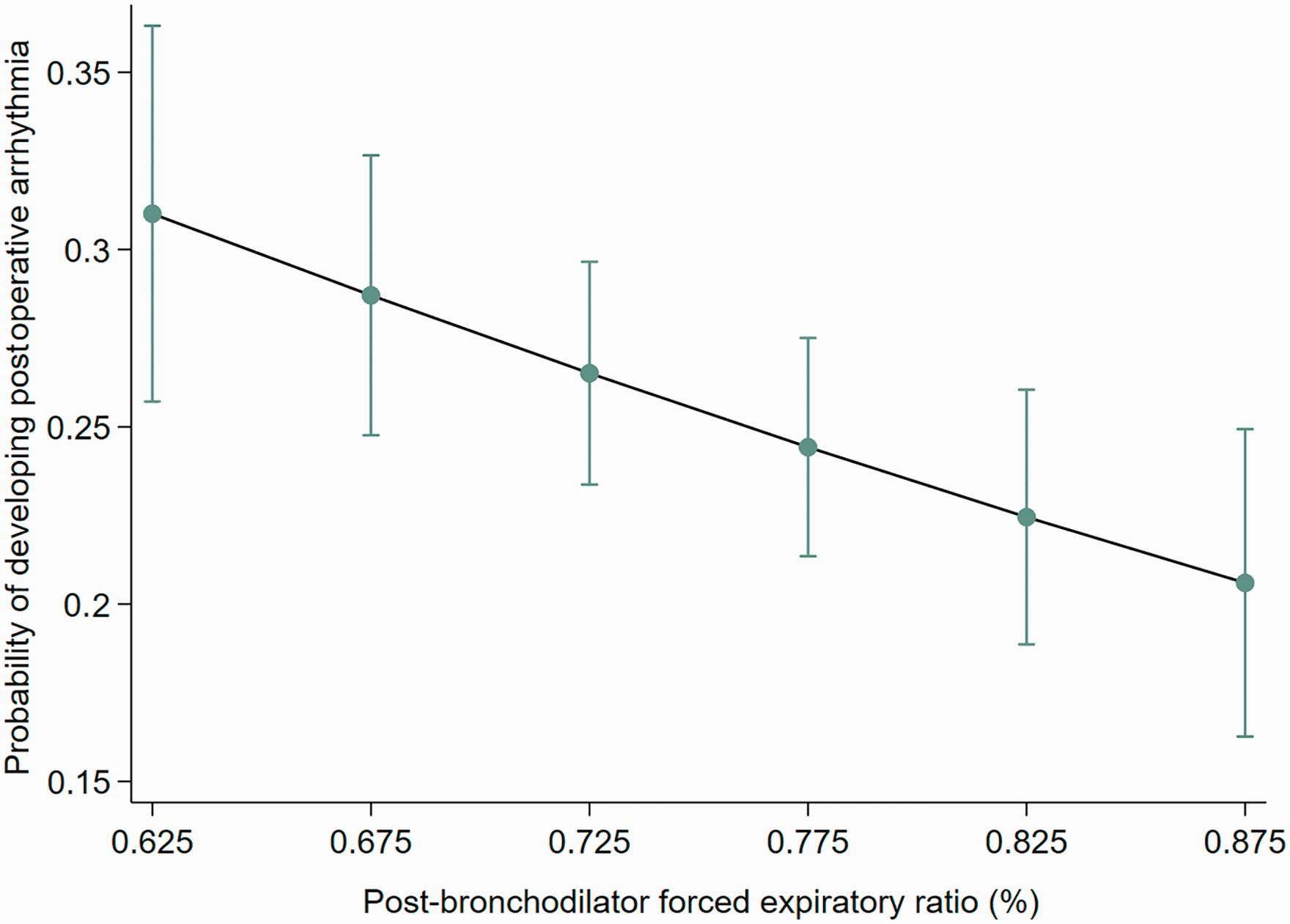
Plot of the predicted probability of postoperative arrhythmia, with 95% confidence intervals, versus forced expiratory ratio (%; range 10th–90th percentile).
Discussion
Of the PFT measures studied, percent predicted DLCO and FVC were most strongly associated with prolonged postoperative ventilation and ICU LOS. We defined prolonged ventilation as extending beyond 18 hours, the upper quintile for ventilation hours in our population. This cut-off also represented twice the median duration of ventilation and the threshold duration of ventilation below which patients were able to be discharged on day 1 post surgery. Patient-level discrimination was poor, however. Patients with high-risk PFT parameters had only a slightly greater than 50% probability of requiring prolonged ventilation.
Elective cardiac surgery is a common intervention with a considerable impact on both surgical and intensive care resources. Since 25% of patients are ≥75 years old and the majority of patients have at least one chronic comorbidity, 18 cardiac surgery requires intensive perioperative care. A requirement for prolonged invasive ventilation can impact the efficiency of cardiac surgical services unless anticipated and planned for. It is conceivable that PFT parameters might usefully predict the risk of postoperative complications and ICU utilisation, thus facilitating perioperative planning. However, PFT requires specialised equipment and skilled technical personnel servicing a broad range of disciplines, and access can be challenging. Furthermore, as well as presenting both direct and opportunity cost to the healthcare system, inappropriate use of PFT is of considerable inconvenience to patients. Moreover, although the presence of chronic lung disease is important to identify, as it influences validated risk-stratification scores such as the EuroSCORE 2 and STS scores, this information is often available without repeating formal PFTs, and indeed adding PFT does not appear to improve model discrimination. 19 We found that although patients with FVC <80% predicted plus DLCO <60% predicted had an OR of 7.5 for requiring prolonged ventilation, only 57% of this cohort of patients actually required prolonged ventilation, and the proportion of these patients requiring >48 hours in ICU was only 14%. In keeping with the existing literature supporting the idea that continuous probability predictions are not useful for individual patient prediction, the extent to which variability in duration of ventilation, ICU LOS and frequency of postoperative complications was explained by our PFT-based model was limited. Our data thus support the assertion of the US STS that PFT is unnecessary before cardiac surgery in patients without respiratory symptoms. The observation that ICU LOS and not hospital LOS is predicted by PFT indicates that other important variables influence overall hospital course. Nevertheless, our data provide useful population-level information regarding predictors of prolonged ventilation and ICU utilisation which may guide system-wide resource planning. It is noteworthy that spirometry parameters consistent with a diagnosis of COPD did not identify patients more likely to require prolonged ventilation or ICU LOS. This makes it less likely that the association of FVC and DLCO with prolonged ventilation was primarily driven by COPD with gas trapping.
The risk of postoperative arrhythmia was higher for those patients with spirometry parameters consistent with a diagnosis of COPD. Furthermore, the risk of postoperative arrhythmia was inversely related to FER. Mechanisms by which chronic lung disease may promote arrhythmia include atrial remodelling and beta-adrenergic agonist therapy.20,21 Atrial fibrillation after cardiac surgery is associated with increased stroke risk, need for anticoagulation and worse long-term survival.22,23
Our study has several limitations. Whilst our large study cohort and institutional practice is broadly representative of the Australian and New Zealand elective cardiac surgical population and healthcare service, our data are derived retrospectively from a single centre where PFT is routinely requested prior to elective cardiac surgery, and the application of our findings should be considered accordingly. Furthermore, 26.5% of elective cardiac surgical patients did not have PFT. These may have been healthier patients not referred for PFT, or frail or non-metropolitan patients less able to attend for PFT. Such baseline disparity might influence generalisability of the data. Since PFT is actually a ‘suite’ of investigations with a high degree of collinearity, it is unavoidable that multiple comparisons must be made to identify candidate variables. Accordingly, our findings should be considered exploratory. Finally, whilst most postoperative arrhythmias are atrial fibrillation, the ANZSCTS database does not record subtypes of postoperative arrhythmia, and we cannot fully evaluate the association of subtypes of arrhythmias with COPD. 24
In conclusion, deranged PFT parameters are associated with a requirement for prolonged postoperative ventilation and the duration of ICU LOS. These findings may inform the resource implications associated with performing cardiac surgery on the elective adult cardiac surgical population in South Australia. PFT also identifies those patients at highest risk of arrhythmia, and future interventional trials might focus on this high-risk subgroup.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.