
Abstract
Abstract
P2/N95 respirators or filtering facepiece respirators may not have the same pass rate on quantitative fit testing. The aim of this study was to investigate the pass rate of four commonly used filtering facepiece respirators in Australian healthcare providers. The secondary objectives included assessing the ease of donning, doffing and comfort of wearing these four filtering facepiece respirators for more than 30 minutes. A multivariable analysis was also conducted to assess if certain variables (e.g. age, sex, body mass index, ethnicity, facial width and length) were associated with passing or failing fit testing. We conducted a prospective observational study of 150 hospital staff who presented for fit testing in a metropolitan hospital in Victoria, Australia. The order of the four filtering facepiece respirators being tested was randomised. A Cochran’s Q test was used to test the global null hypothesis that all four filtering facepiece respirators being tested have the same pass rate. A difference in pass rate was found between the four filtering facepiece respirators that were tested (P < 0.001). The 3M™ Aura 1870+ (3M Australia Pty Ltd, North Ryde, NSW) had the highest pass rate (83%) followed by the 3M™ 1860 (3M Australia Pty Ltd, North Ryde, NSW) (61%), BSN ProShield™ N95 (BSN Medical, Mulgrave, Victoria) (55%) and the BYD DE2322 N95 (BYD Care, Los Angeles, CA, USA) (44%). There was also a difference in the ease of donning, doffing and comfort. Therefore, healthcare facilities that perform fit testing should take these factors into consideration when designing an effective respiratory protection programme.
Keywords
Introduction
Fit testing is the process of ensuring that an N95/P2 respirator or filtering facepiece respirator (FFR) can form an adequate seal to protect healthcare workers from airborne diseases such as SARS-CoV-2, which causes COVID-19. Previous studies have demonstrated that certain FFRs have a higher chance of passing fit testing than others.1–5 However, there are few quantitative fit testing studies with a strict testing methodology comparing different FFRs in an Australian healthcare setting. Comparing different FFRs is important because health services could purchase large quantities that do not fit a substantial proportion of their healthcare workers. Therefore, we sought to determine the pass rate of four different styles of FFRs in a metropolitan teaching hospital in Victoria, Australia. Other factors that affect compliance with wearing FFRs such as ease of donning, doffing and comfort were also assessed. Demographic and anthropometric data were also collected to assess whether these factors correlated with passing fit testing.
Methods
This was a prospective, single-centre, observational study of participants who presented for fit testing at a metropolitan hospital in Victoria, Australia. Participants were requested not to smoke within 30 minutes of testing. Men were asked to be clean-shaven or to have shaved within 24 hours prior to testing. The recruitment period was from 2 July to 7 September 2021. The follow-up was completed on 7 October 2021.
Four FFRs were investigated in our study: 3M™ Aura™ 1870+ (3M Australia Pty Ltd, North Ryde, NSW), 3M™ 1860 (3M Australia Pty Ltd), BYD DE2322 N95 (BYD Care, Los Angeles, CA, USA) and BSN ProShield®: Size M (BSN Medical, Mulgrave, Victoria). These four were chosen because they represent four different styles, were tested in previous studies,2,6,7 or were used extensively in public hospitals in Victoria prior to the COVID-19 pandemic. All four FFRs are currently registered in the Australian Register of Therapeutic Goods.
Our testing protocol was different from routine quantitative fit testing in several respects: all four FFRs were tested; the order of the four FFRs being tested was randomised, and a strict testing protocol was used to reduce the risk of bias introduced by different fit testers.
The fit test was conducted by trained fit testers using the AccuFIT 9000® PRO (AccuTec-IHS, Tulsa, OK, USA) with the ‘N95 mode’ enabled. The AccuFIT 9000 PRO uses a condensation nuclei counter technique to assess the number of particles in ambient air and compares it to the particles within the breathing zone of the FFR. A fit factor of ≥100 is required for an FFR to pass fit testing as per Australian Standards. 8 This fit factor is derived from the harmonic mean of the four pre-specified modified Occupational Safety and Health Administration (OSHA, Washington, DC, USA) exercises. These exercises consist of bending at the waist, talking, turning head side to side and looking up and down. 9 Testers were trained by an external provider performing fit testing at the hospital or had completed a training course.
Daily ‘validation checks’ were performed to ensure that the machine was functioning correctly and that adequate particle counts were present for testing. A particle generator was also used to increase the ambient particle count. All four pre-specified exercises were completed for each test regardless of the fit factors obtained—that is, the test was not allowed to terminate early.
After obtaining informed consent, participants were asked to don the FFR in front of the mirror. The testing protocol was then explained to the participant, and testing commenced. The fit tester was allowed to remind the participants how to don the FFR and perform a fit check. At the time of this study, a hospital-wide training programme had not yet been implemented. Care was taken to ensure that the breathing tubes were supported by hand by the participants so that the FFR seal was not affected. We did not use a lanyard to hold the breathing tubes. If the fit factor for the test was ≥100, it was recorded as a pass. If the fit factor was <100, then the test was recorded as a fail. If the test failed, real-time mode was used, which allowed the participants to adjust the FFR while looking at the fit factor in real time. This mode teaches the participant how to don the FFR correctly to achieve a good seal. If the participant could consistently achieve a fit factor of ≥100 during the real-time mode, the participant was allowed a second test after doffing and redonning the FFR. This ensured that the participant could pass the fit test without assistance. If the second test also failed, the FFR was recorded as a fail, and no other tests were allowed for that FFR. The participants then continued to test the next FFR in the randomisation sequence.
Randomisation of the order of the four FFRs was performed using a web-based research randomiser programme (https://www.randomizer.org/). The purpose of randomisation was to reduce the potential bias from repeated donning, doffing and testing, which may lead to better outcomes for FFRs that are tested later in the sequence.
As there is no validated questionnaire to assess the ease of donning, doffing and comfort of wearing the FFR, we constructed a 10-point Likert scale, with 1 being ‘very difficult to don/doff or very uncomfortable to wear’ and 10 being ‘very easy to don/doff or very comfortable to wear’. The participants were requested to assess the ease of donning and doffing immediately after the testing session. They were then asked to wear the FFR for at least 30 minutes in a non-clinical setting for a comfort assessment. A plug was used to seal the probed FFR in order to simulate similar breathing resistance.
Demographic and anthropometric data (age, weight, height, sex, ethnicity, face width and face length) were also collected to determine whether these factors correlated with the likelihood of passing fit testing. The ethnicity categories were derived from the Australian Standard Classification of Cultural and Ethnic Groups by the Australian Bureau of Statistics, 10 except for the category of ‘mixed descent’. The Menton–Sellion length (face length) and bizygomatic breadth (face width) were also measured using Martin breadth callipers and sliding bone callipers.
Based on previous reports,10,12 a sample size of 116 participants would have an 80% power to detect a 25% absolute difference in pass rates between the worst FFR (56%) and the best FFR (81%). We inflated the recruitment to 150 participants to account for dropouts. For the primary outcome, a Cochran’s Q test was used to test the global null hypothesis that there was no difference among the four FFRs. If a difference was found, a pairwise McNemar’s test was used to test the statistical significance between pairs of FFRs. A Bonferroni correction was applied where multiple comparisons were made by dividing the calculated P-value by the number of pairwise comparisons. Therefore, the cut-off for statistical significance remained at P < 0.05.
Secondary outcomes were compared using analysis of variance, and the Bonferroni correction was again applied for multiple comparisons. Univariate and multivariate analysis were conducted to assess which variables (age, sex, body mass index, ethnicity, Menton–Sellion length and bizygomatic breadth) were associated with the categorical outcome of passing or failing fit testing. Multivariable analysis of ethnicity only included categories with more than five participants. Given the vast number of variables and multiple testing in the relatively small number of subjects, the results of the multivariate analysis were considered exploratory only, that is, to generate hypotheses that may warrant future testing. Data are presented as mean (standard deviation), rate and proportion, as appropriate.
Written informed consent was obtained from all the participants. This study was approved by the Eastern Health Human Research Ethics Committee and followed the guidelines stipulated in the National Statement on Ethical Conduct in Human Research. This study was also prospectively registered in the Australian and New Zealand Clinical Trials Registry (ACTRN12621000388819).
Results
In total, 150 participants were recruited. Five participants dropped out after signing the consent form but prior to commencing testing because of a lack of time. A total of 145 participants completed fit testing, which was randomised, for all four FFRs.
Participants’ characteristics are presented in Table 1. Of the four FFRs, the 3M Aura had the highest pass rate (121/145; 83%), followed by the 3M 1860 (89/145; 61%), the BSN ProShield (M) (80/145; 55%) and then the BYD DE2322 N95 (64/145; 44%). The differences in the pass rate between the four FFRs were statistically significant (P < 0.001). A pairwise McNemar’s test found that all the pairs that were tested were statistically significantly different, except for the difference between the 3M 1860 and the BSN ProShield. Detailed statistical analysis with individual comparisons and P-values are included in the online Supplemental Material.
Characteristics of participants.
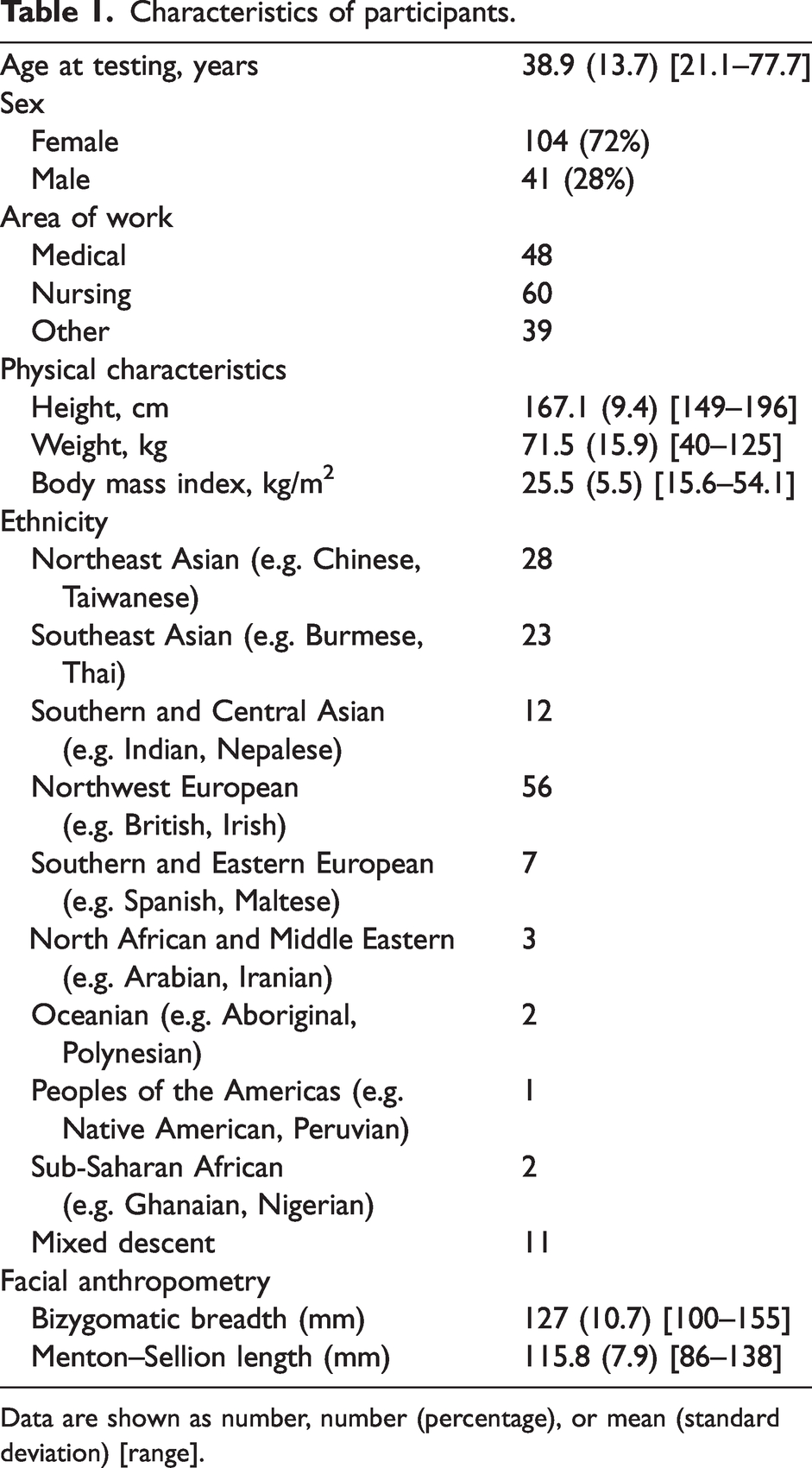
Data are shown as number, number (percentage), or mean (standard deviation) [range].
Most FFRs that passed the fit testing passed on the first test; the 3M Aura and 3M 1860 had more fit factors of >200 (see Table 2). A fit factor of >200 signifies that the FFR had a very good fit at the time of testing.
Pass rates of filtering facepiece respirators on quantitative fit testing.
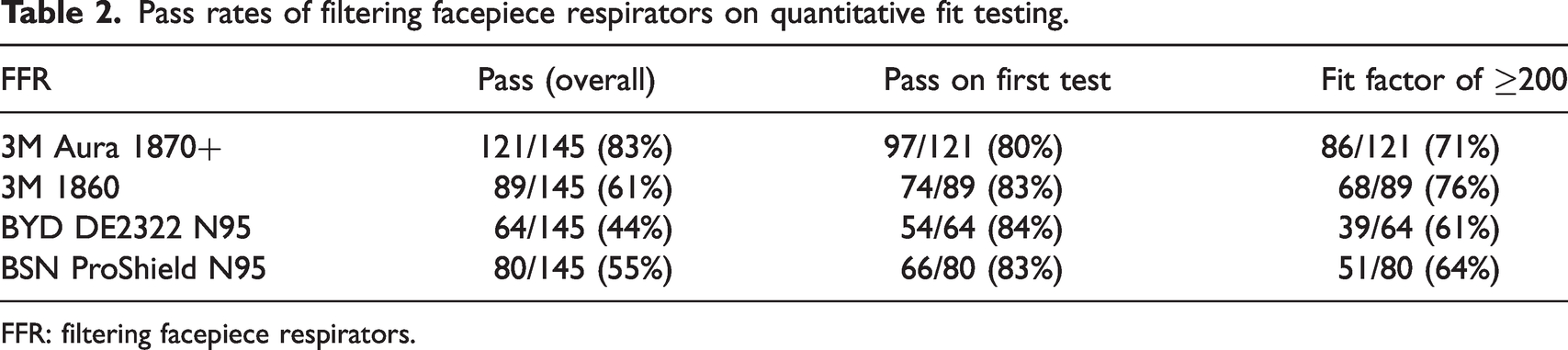
FFR: filtering facepiece respirators.
For the secondary outcomes, 142 participants answered the questionnaire on the ease of donning and doffing, and 88 participants returned their comfort assessment. There was a small difference in the ease of donning and doffing among the four FFRs (see Table 3). The 3M 1860 was the most difficult to don compared to all the other FFRs (P ≤ 0.002). There was also a small difference in doffing between the 3M 1860 and 3M Aura (P = 0.005). For comfort, a larger difference was found, with the 3M Aura being the most comfortable (with a mean comfort score of 7.8), whereas the 3M 1860 was rated as the most uncomfortable FFR to wear for more than 30 minutes (mean comfort score of 3.8; P < 0.001) (See Figure 1).
Ease of donning, doffing and comfort of filtering facepiece respirators.a,b
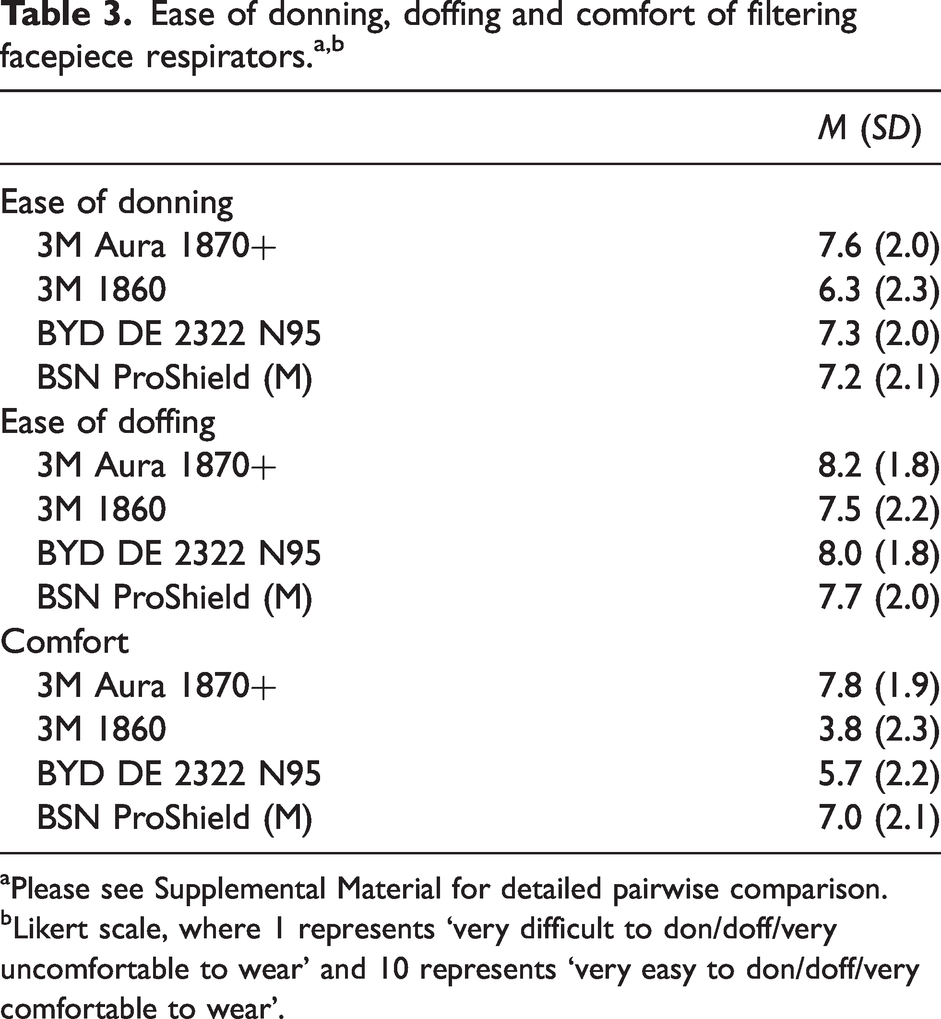
aPlease see Supplemental Material for detailed pairwise comparison.
bLikert scale, where 1 represents ‘very difficult to don/doff/very uncomfortable to wear’ and 10 represents ‘very easy to don/doff/very comfortable to wear’.
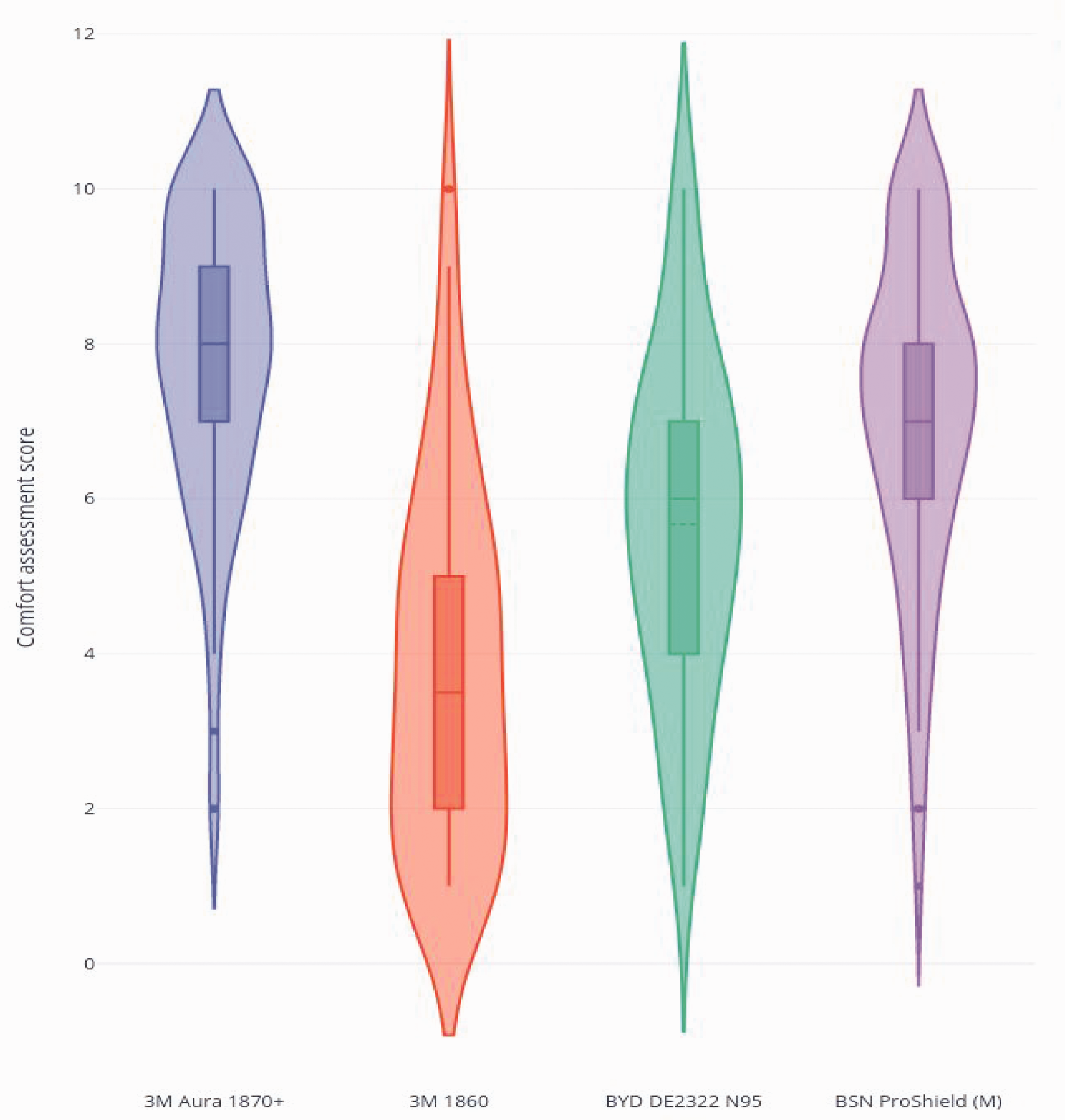
Subjective assessment of comfort for four different filtering facepiece respirators.a
Multivariable logistic regression analysis was conducted to investigate variables that may be associated with passing fit testing. The variables that were tested included age, sex, body mass index, ethnicity group, facial width and facial length. For the 3M Aura and BYD N95, no variables were statistically significant in predicting passing fit testing. For the 3M 1860, the categories of Southern and Eastern European (P = 0.048, odds ratio (OR) 0.07, Southeast Asian (P = 0.041, OR 0.09) and Northeast Asian (P = 0.016, OR 0.06) achieved statistical significance for being associated with failing fit testing compared to the mixed-descent ethnicity, but the effect was very small. For the BSN ProShield, a wider face (P = 0.027, OR 1.04) was associated with a greater chance of passing the fit test, but again the effect was very small. A more detailed analysis is provided in the Supplemental Material.
Discussion
In this study, the 3M Aura had the highest pass rate among the four FFR tested. It was also rated the easiest to don and doff and the most comfortable to wear for at least 30 minutes. Our pass rate finding is similar to previous studies that have found the 3M Aura to be most likely to pass fit testing of the four FFRs tested.1,5,13
Although the 3M 1860 had the next highest pass rate at 61%, it was rated as the most uncomfortable to wear for more than 30 minutes. This is relevant because staff who work in COVID-19 wards or intensive care units must wear an FFR continuously for several hours. There was also a small difference in the ease of donning between the 3M 1860 and the other FFRs. Many participants remarked that the rigid metal nosepiece was difficult to mould. Although the difference was found to be statistically significant, the difference is small, and the clinical significance is unclear.
A key strength of our study is that it was conducted in an Australian hospital with a diverse, multicultural cohort. Our participants included a variety of hospital personnel such as doctors, nurses, allied health personnel, engineers, translators and cleaners. Some of our participants were very experienced at wearing FFRs, whereas others had no experience. Therefore, our results are likely to be generalisable to other Australian metropolitan hospitals. Furthermore, this cross-disciplinary study included occupational hygienists at our hospital.
Our study has several limitations. First, we did not test all FFR sizes. The 3M 1860 and the BSN ProShield N95 are available in size ‘S’ as well as the sizes tested. We decided not to include additional sizes because the supply of the BSN ProShield (S) was limited at the time of testing, and there were no instructions from the manufacturer as to who should be fitted with size ‘S’. Therefore, if we had included the size ‘S’, all the participants would have needed to be tested on both sizes, and it would have prolonged the testing time, potentially making it too onerous. Second, the participants were not blinded to the outcome of the fit testing, which could bias their rating of the secondary outcomes. As the purpose of fit testing was to determine the FFR fit, we thought it would be unethical to withhold this information. Furthermore, our study also did not evaluate the change in fit when an FFR was worn over a prolonged period. Third, we acknowledge that the Likert scales used to assess the ease of donning, doffing and comfort are not validated scales, and the results should be interpreted accordingly. Finally, we recognise that our multivariable analysis was most likely underpowered to identify or exclude real effects of the demographic variables on passing fit testing.
In conclusion, the results of this study showed that different FFRs have different pass rates, ease of use and comfort. This could affect compliance and safety. Healthcare facilities that stock and perform fit testing of FFRs should consider these differences when developing a respiratory protection programme.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X231154017 - Supplemental material for Pass rates of four P2/N95 respirators or filtering facepiece respirators in Australian healthcare providers: A prospective observational study
Supplemental material, sj-pdf-1-aic-10.1177_0310057X231154017 for Pass rates of four P2/N95 respirators or filtering facepiece respirators in Australian healthcare providers: A prospective observational study by Low Caitlin SR Conceptualization Data curation Funding acquisition Investigation Methodology Project administration Writing – original draft Writing – review & editing Ngui Sean Z Data curation Methodology Project administration Writing – review & editing Casey Matthew J Conceptualization Methodology Project administration Resources Writing – review & editing Vuong Chloe Data curation Methodology Project administration Writing – review & editing Afroz Afsana Formal analysis Methodology Writing – review & editing Sengupta Shomik Funding acquisition Methodology Writing – review & editing Weinberg Laurence Conceptualization Methodology Supervision Writing – review & editing in Anaesthesia and Intensive Care
Supplemental Material
sj-pdf-2-aic-10.1177_0310057X231154017 - Supplemental material for Pass rates of four P2/N95 respirators or filtering facepiece respirators in Australian healthcare providers: A prospective observational study
Supplemental material, sj-pdf-2-aic-10.1177_0310057X231154017 for Pass rates of four P2/N95 respirators or filtering facepiece respirators in Australian healthcare providers: A prospective observational study by Low Caitlin SR Conceptualization Data curation Funding acquisition Investigation Methodology Project administration Writing – original draft Writing – review & editing Ngui Sean Z Data curation Methodology Project administration Writing – review & editing Casey Matthew J Conceptualization Methodology Project administration Resources Writing – review & editing Vuong Chloe Data curation Methodology Project administration Writing – review & editing Afroz Afsana Formal analysis Methodology Writing – review & editing Sengupta Shomik Funding acquisition Methodology Writing – review & editing Weinberg Laurence Conceptualization Methodology Supervision Writing – review & editing in Anaesthesia and Intensive Care
Footnotes
Acknowledgements
The authors would like to thank the fit testers who participated in this research project.
Author Contributions
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Caitlin Low received funding from the Australian and New Zealand College of Anaesthetists (Novice Investigator’s Grant N22/008).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.