
Abstract
Healthcare’s environmental sustainability is increasingly an area of research and advocacy focus. The Australian and New Zealand College of Anaesthetists (ANZCA) has produced a professional document, PS64, Statement on Environmental Sustainability in Anaesthesia and Pain Medicine Practice, and a background paper, PS64 BP. The purpose of the statement is to affirm ANZCA’s commitment to environmental sustainability and support anaesthetists in promoting environmentally sustainable work practices. This article presents the main features of PS64 and its background paper, and the associated supporting evidence. The healthcare sector is highly interconnected with activities that emit pollution to air, water and soils, considerably adding to humanity’s collective ecological footprint. As anaesthetists, we are uniquely high-carbon doctors due to our work anaesthetising with greenhouse gases (particularly desflurane and nitrous oxide) and our exposure and contribution to large amounts of resource and energy use and waste generation in operating theatres. Discussion is made of the improving research base of anaesthetic life-cycle assessments—that is, cradle-to-grave studies of how much energy, water and so on a product or process requires throughout its entire life. Thereafter, reducing, reusing and recycling as well as water use are examined. Ongoing research efforts within environmentally sustainable anaesthesia are highlighted. Environmentally sustainable anaesthesia requires scholarship, health advocacy, leadership, communication and collaboration. The focus is placed on practical initiatives within PS64 and the background paper that can be achieved by all anaesthetists striving towards more sustainable healthcare practices that reduce waste, reap financial benefits and improve health.
Introduction
The Australian and New Zealand College of Anaesthetists (ANZCA) promotes high standards of safety and quality for patient care through the development of professional documents. The development of professional documents aims to be objective, informed, transparent and based on best available evidence. 1 After almost two years of development and piloting, the final PS64 Statement on Environmental Sustainability in Anaesthesia and Pain Medicine 2 and its accompanying background paper, PS64 BP, 3 were released in July 2019.
ANZCA PS64 exists to: (a) affirm ANZCA’s commitment to environmental sustainability, (b) aid clinicians and healthcare facilities to promote and embed environmentally sustainable workplace practices into patient care and (c) assist healthcare facilities in embedding sustainable practices in the delivery of safe patient care. 4 This article presents the key features of PS64 and the background paper, as well as associated supporting evidence. We recognise that there can be accord as well as conflict between individual patient health and public health commitments. Such commitments will require careful judgement by anaesthetists to ensure safety and quality for patient and population care.
PS64 is similar to statements regarding environmental sustainability issued by the American Society of Anesthesiologists, 5 the Association of Anaesthetists 6 and the Société Française d’Anesthésie et Réanimation. 7 Accordingly, anaesthetic journal interest in environmental sustainability is evident with editorials in the BJA, 8 Anesthesia and Analgesia 9 and Anaesthesia. 10 Environmental sustainability within medicine is a nascent field, which demands that we engage with the challenge of incorporating this evidence-based field into our specialty, continually asking research questions as we do so. 11
ANZCA PS64 is significant, as (a) climate change and biodiversity loss are defining and challenging health issues relevant to all anaesthetists,12,13 (b) anaesthetists are a unique group of doctors who administer greenhouse gases that are subsequently delivered into the atmosphere, (c) anaesthetists witness large amounts of physical waste associated with operating-room activities, and (d) we wish to do no harm to patients or the environment, yet many anaesthetists experience cognitive dissonance, 14 as every day they are exposed to wasteful medical work practices, although the majority of anaesthetists are interested in ‘reducing, reusing and recycling’. 15
Climate change and health
ANZCA does not purport to have expertise in climate science, and neither PS64 nor its accompanying BP are repositories of evidence for climate change. Climate science sources can be found via the Australian Bureau of Meteorology and CSIRO, 16 the NZ National Institute of Water and Atmospheric Research, 17 the US National Oceanic and Atmospheric Administration 18 and the UN Intergovernmental Panel on Climate Change. 19
The health implications associated with climate change are already widespread and predicted to increase.12,20 The World Health Organization estimates that between 2030 and 2050, climate change will lead to approximately 250,000 additional deaths per year globally. 21
Climate change impacts social and environmental determinants of health: clean air, safe water, sufficient food, freedom from disease, and secure shelter. 12 It amplifies extreme weather events such as heatwaves, droughts, floods and storms. Climate change’s impacts will be particularly significant for the vulnerable (children, the elderly, the infirm, indigenous populations, etc.). 12 In 2015, the Rockefeller Foundation–Lancet Commission on planetary health published Safeguarding Human Health in the Anthropocene Epoch, 13 which noted that ‘the health impacts from environmental changes are driven by unsustainable patterns of resource consumption, technological development and population growth, 13 and pose enormous challenges to the global health gains of recent decades’.
Healthcare pollution
In Australia, more than 7% of national carbon emissions arise from the healthcare sector 22 —midway that between the UK and the USA (4% and 10%, respectively, of their national carbon dioxide equivalent (CO2e) emissions stem from healthcare).23,24 The US healthcare system accounts for the equivalent CO2e emissions of the entire UK. 24 In Australia, healthcare CO2e emissions are dominated by those arising from acute hospital care (44% in total) and pharmaceuticals (19%), with all general practice, for example, contributing only 4%. 22 Although we have not quantified the effects of anaesthetic agents in Australia, the UK estimates are that 5% of acute hospital CO2e emissions are a direct result of all anaesthetic gases (volatiles and nitrous oxide (N2O)). 25
The healthcare sector is highly interconnected with activities that emit pollution to air, water and soils, making a significant contribution to our collective ecological footprint.4,12,13 Sustainable healthcare practices can reduce costs and waste and improve health. 12 Anaesthetists are high-carbon doctors. We work (a) by anaesthetising with greenhouse gases, (b) in operating theatres which are high-end users of hospital resources, and (c) in hospitals that are intensive users of energy, equipment and resources. Providing guidance through documents such as ANZCA PS64 will assist anaesthetists, surgeons, nurses and other colleagues towards more environmentally sustainable practices.
Anaesthetic agents
Of particular interest to anaesthetists in any discussion about sustainable healthcare are the atmospheric impacts of using inhaled general anaesthetic agents (halogenated organic compounds and N2O). Global warming potential (GWP) is one metric used to compare warming impacts of different agents relative to the same mass of CO2 over a specific time frame. The GWP is calculated by multiplying the atmospheric lifetime of an agent with its radiative forcing capacity. Despite being present in the atmosphere at a concentration around 100,000 times lower than CO2, halogenated organic compounds have high GWPs.26,27 The global warming effect of all halogenated compounds is approximately 11% of total anthropogenic radiative forcing (global warming). 26 Halogenated organic compounds include hydrofluorocarbons used in refrigeration, but also volatile anaesthetic agents. As a proportion of total CO2 emissions, volatile anaesthetic agents are responsible for 0.01%–0.1% of global warming.28,29
N2O is responsible for a further 6% of anthropogenic global warming. 26 N2O breaks down atmospheric ozone, and its ongoing release is now the main worldwide contributor to ozone depletion. 30 The vast majority of N2O arises from burning forests, fertiliser use, industrial processes and transport. Worldwide anaesthetic use of N2O is estimated to contribute between 1% 31 and 3% 32 of global N2O emissions.
The global warming effects of anaesthetic agents vary markedly and have been researched over the past 30 years.29,32–36 The most recent and comprehensive work (in 2011) by Sulbaek Andersen et al.29,36 calculated that over 100 years, the GWP of desflurane was 2540 (1 g of desflurane has the same GWP as 2540 g CO2), sevoflurane was 130,29,36 isoflurane was 510 and N2O was approximately 300. 27 Thus, per mass, desflurane has a GWP approximately 19 times that of sevoflurane, four times that of isoflurane, and eight times that of N2O.
Atmospheric lifetimes of anaesthetic volatile agents are determined by their structure, and they range from 1.1 year for sevoflurane to 3.2 years for isoflurane, 14 years for desflurane 36 and 114 years for N2O. 27 The greater GWP of desflurane is mainly due to its atmospheric persistence more than its slightly higher intrinsic radiative forcing. Where inhalational agents are being measured in the atmosphere, desflurane’s concentration is rising, sevoflurane’s is relatively static and halothane’s and isoflurane’s levels are falling. 37
A further consideration for anaesthesia is the amount of the agent required for clinical use. Given that desflurane has a minimum alveolar concentration (MAC) of 6.6%, sevoflurane of 1.8% and isoflurane of 1.2%, we need at least three times as much desflurane (by mass) to achieve the same degree of anaesthesia as sevoflurane and five times that of isoflurane. 38 Taking into account the GWPs, for the same fresh gas flow (FGF), the greenhouse gas emissions (CO2e) for desflurane are approximately 50 times (19 GWP×3 potency) that of sevoflurane and 20 times (4 GWP×5 potency) of isoflurane. N2O has a GWP of approximately 300 (one-eighth of desflurane), but we deliver 50% FiN2O, approximately eight times the inspired concentration of desflurane. Hence, the greenhouse gas effect of N2O and desflurane are similar per MAC-hour, though at 50% FiN2O, approximately half a MAC is delivered.
In common parlance, delivering 50% N2O or 7% desflurane at a total FGF of 1 L/min for six hours is equivalent to driving an average car over 500 km (for 50% N2O) or 1000 km (for 7% desflurane).39–41 For 3.5% Fi sevoflurane or 2% Fi isoflurane at 1 L/min FGF for six hours (a day of anaesthesia), we have driven our average car less than the equivalent of 50 and 100 km, respectively. 41
Any considerations for the choice of anaesthetic agent must be in the context of achieving the best patient outcomes. As noted previously, environmental pollution is one of several factors to consider when determining the best technique for an individual patient. Nevertheless, the most important measures anaesthetists can take individually to reduce their carbon footprint are to (a) avoid desflurane and N2O, (b) practice low-flow anaesthesia and (c) embrace techniques to minimise the requirement for inhalational agents, such as regional anaesthesia and total intravenous anaesthesia. Furthermore, there is ongoing research and development of devices to capture and either destroy or reclaim waste anaesthetic gases,42–46 though no such devices are in common use as yet.
A life-cycle assessment (LCA) estimated that the carbon footprint of propofol was several orders of magnitude lower than inhalational anaesthetics. 47 Sherman et al.’s study 47 estimated the environmental effects of propofol manufacture, and included the environmental burden of syringes and pumps associated with drug delivery, assuming 50% propofol drug wastage. 48 Importantly, discarding of unused propofol to the environment may have other deleterious effects upon aquatic and terrestrial ecosystems. 48
Life-cycle assessments
An LCA includes a cradle-to-grave analysis of the environmental footprints arising from the extraction, manufacture, transport, use and recycling/waste disposal/reuse of equipment or processes.49,50 Environmental footprints can be determined for energy, carbon emissions (climate change), water, pollutants (aquatic and terrestrial) and ozone depletion, amongst others. A general introduction to LCA for the anaesthetist is available in the medical literature. 51 Fortunately, large, established databases and software 52 now exist to assist researchers with LCAs of the relative environmental impacts associated with products/procedures, reducing the time and expense of undertaking LCAs and hopefully leading to more examples of this research in healthcare.
To date, life-cycle studies indicate that using reusable anaesthesia items consistently saves money when compared to single-use equipment, but that the environmental impacts depend very much upon the source of electricity for reprocessing reusable items. Further, in all considerations between using reusable versus single-use devices, there are safety and quality concerns in addition to potential regulatory restrictions and local jurisdictional factors.53,54
A review of five studies comparing reusable versus single-use surgical gowns concluded that using reusable gowns had at least a 50% lower environmental footprint than using single-use gowns. 55 In a study of anaesthetic drug trays and central venous catheter insertion kits, it was found that using reusable equipment had significant financial advantages over the single-use items, though the carbon emissions depend on the hospital energy sources, including the presence of co-generation facilities and grid electricity energy source (higher CO2 emissions for reusable equipment processing compared to single use if present in locations using coal-based electricity).56,57 In 2012, Eckelman et al. found that the carbon footprint of using reusable laryngeal mask airways (LMAs) was two-thirds that of the single-use LMAs. 58
The environmental footprint of reusable versus single-use commonly used anaesthetic items such as facemasks, direct and videolaryngoscope handles and blades and breathing circuits have been compared in Australia through LCA studies. 59 It was found that using reusable anaesthetic equipment saved approximately $5000 per operating room per annum, though the carbon footprint was slightly higher. However, if the LCAs had been performed in New Zealand, Europe or the USA, the carbon footprint would have been considerably lower for the reusable anaesthetic equipment due to different energy sources; Australian electricity is heavily reliant upon coal. 59 Internationally, the environmental impacts for different surgical procedures have also been analysed, including caesareans, 60 cataracts 61 and hysterectomies, 62 with a hysterectomy generating approximately 500 kg of emissions in the USA—equivalent to driving an average Australian car 2800 km. 63
Further LCA analysis will enable a more accurate understanding of where efforts can be made to minimise healthcare’s environmental footprint, already known to be overwhelmingly hospital-centric, rather than from community practice, public health or ambulance transport.24,64
Waste: reduce, reuse, recycle
Reducing: rational use of diagnostics, prescriptions and procedures
The environmental impact of diagnostic tests and prescriptions is large. Reducing unnecessary investigations and medications can significantly reduce the environmental footprint of healthcare. 65 Programmes such as Choosing Wisely may improve clinical care while promoting rational resource use. 66 The same principles apply to avoiding ineffective operations, or the routine practice of opening consumables in case of an emergency. Interventions and protocols can be evidence- based and work towards preventing escalation of care whilst considering patient expectations.
Reducing: equipment, pharmaceuticals and consumables
In the UK, the National Health Service (NHS) Sustainable Development Unit (SDU) has identified the procurement chain involved in maintaining stock levels, equipment and pharmaceuticals as a substantial source of waste and carbon footprint. 64 Anaesthetists can participate in hospital product evaluation committees and introduce LCA considerations into the procurement chain. 11 Clinicians and healthcare facilities can encourage manufacturers and suppliers to provide more environmentally friendly products. 11 Management of stock volumes to allow for less wastage of expired and outdated stock could occur. 11 Unused stock and equipment may be collected and donated to developing nations after careful consideration of its eventual use. 67
Operating suites produce a quarter of all hospital waste, 68 and up to 25% of this can be derived from anaesthetic services. 69 Further, approximately one quarter of operating room waste could be recycled in Australia. 70 Simple, correct waste segregation between general and clinical waste is often poorly practised. Yet, no new waste streams need to be set up, and it can have significant financial and environmental benefits.
Reducing: through reusing
Simple measures of reducing by reusing are available throughout the operating suite. For example, use of reusable surgical gowns, dedicated operating theatre footwear and laundered hats will reduce the volume of single-use gowns, caps and overshoes whilst maintaining infection control standards. Using reusable anaesthetic equipment reduces waste and saves money.54,56,58,59,71 The net environmental effect of reusable versus single-use equipment is a complex calculation, and the carbon footprint depends upon the local energy source, mainland Australia (predominantly coal) being very different to New Zealand (predominantly renewable). 51
Anaesthesia breathing circuits can be used for variable periods of time in different countries. ANZCA’s PS28 Guidelines on Infection Control in Anaesthesia do not comment upon the duration of use of anaesthesia breathing circuits provided that each patient receives a separate single-use filter. 72 Several studies have indicated that it is safe from a microbiological standpoint to reuse circuits and to change/wash anaesthesia circuits weekly versus daily.54,71
Recycling
The anaesthetist with a focus on sustainability may consider recycling after exhausting the possibility of reducing and reusing equipment. 73 Polyvinyl chloride recycling of intravenous fluid bags and oxygen masks/tubing is a large-scale programme of reducing operating room waste which began in Australia. 74 Several local studies have shown either large 75 or moderate 70 reductions in waste disposal costs for operating theatres when recycling programmes have begun. ANZCA PS64BP and the ANZCA Australasian Anaesthesia (the Blue Book) 76 detail the efforts required for successful operating room recycling.
Water
In many areas, water availability is becoming scarcer and may have an increasing monetary value attached to it, particularly if desalination is being utilised. 77 Hence, water consumption and recycling are likely to become increasingly important. 11
Incorrect drug disposal can contribute to water-table contamination and toxicity.48,78 Of particular relevance to anaesthetists is propofol waste disposal, as it is poorly biodegradable, accumulates in fat and is toxic to aquatic life and should therefore be disposed of in clinical or pharmaceutical waste receptacles. 48
Infrastructure
Infrastructure planning should recognise that economic, social and environmental benefits are interdependent,79,80 and new infrastructure should be built with consideration of expected changing weather patterns. Workplace efficiency inherently reduces waste, energy demand and costs. Hence, new and existing facilities could be designed or retrofitted with measures to reduce usage and wastage of natural resources. Interaction between hospital engineers and anaesthetists could assist in improving operating room engineering efficiencies and innovation.81,82 Hospital use of renewable energy sources would considerably reduce greenhouse gas production and local air pollution.
The NHS SDU has worked with components of the health system at all scales to pursue a sustainable health system. The SDU has three main purposes: (a) rating the progress towards a healthier environment by the health and social care system, (b) preparing communities for resilience in changing times and climates, and (c) using an approach similar to the accounting framework term ‘triple bottom line’ where every decision should contribute to healthy lives, communities and environments. In 2016, compared to a baseline of 2009, the SDU achieved a carbon reduction of 11% during a period of growth in activity of 18% with associated cost savings for the NHS estimated at £90 million annually. 83 Ambitious targets are for a 50% reduction by 2025. 25
Beyond energy- and resource-efficient buildings, there is evidence-based architectural healthcare design that can improve patient wellbeing and staff satisfaction. Quiet surroundings, natural lighting and views or contact with nature improve patient recovery. 80 The costs of constructing a quality indoor healthcare environment may also be offset by increased productivity from happier, healthier staff. 79
Travel
Considerable direct and indirect health benefits arise from less travel.84,85 Fewer ‘carbon miles’ due to reduced air and road travel will reduce the global burden of climate change and the health impacts of air pollution. 86 Greater active and public transport has health co-benefits through greater physical activity and the associated health advantages in relation to lowering rates of obesity, cardiovascular disease and diabetes. Some preadmission appointments, for example, could be run remotely. Furthermore, all health professionals should be mindful of the benefits of teleconferencing on the environment and health, 87 although individual considerations should always be prioritised, as remote access can be challenging and problematic for some conditions and patients.
Research
Although research into environmental sustainability within healthcare is expanding, more evidence-based research and LCAs are required to assist clinicians and healthcare workers to make informed decisions about the environmental effects of their daily work. Unlike medicine, research in the field of environmental sustainability, and its underpinning foundations in the physical, chemical and biological sciences, are not (and cannot be) contingent upon large, randomised clinical trials (RCTs). Like medical RCTs, however, such environmental research requires robust and scientific aims and methods. For example, LCAs require specific data on the amounts and types of equipment and processes used, with inputs from large-scale life-cycle inventories. Studies of the atmospheric effects of anaesthetic agents or of aquatic pollution by drugs require informed, clearly reproducible methods. Translation of this rapidly evolving evidence into practice in the near future lends itself to an area of increasing priority and demonstration of leadership.
An example of LCA research that may lead to changes in processes/packaging is a recent study of morphine’s life cycle. 88 The entire life cycle of producing and packaging 100 mg of intravenous morphine was found to have a CO2 emission equivalent to driving an average car only 1 km. 88 The sterilising and packaging of intravenous morphine added significantly to the final CO2 emissions, with 50% of the total carbon footprint from the packaging and only 10% from producing the morphine compound (perhaps because morphine is plant based).
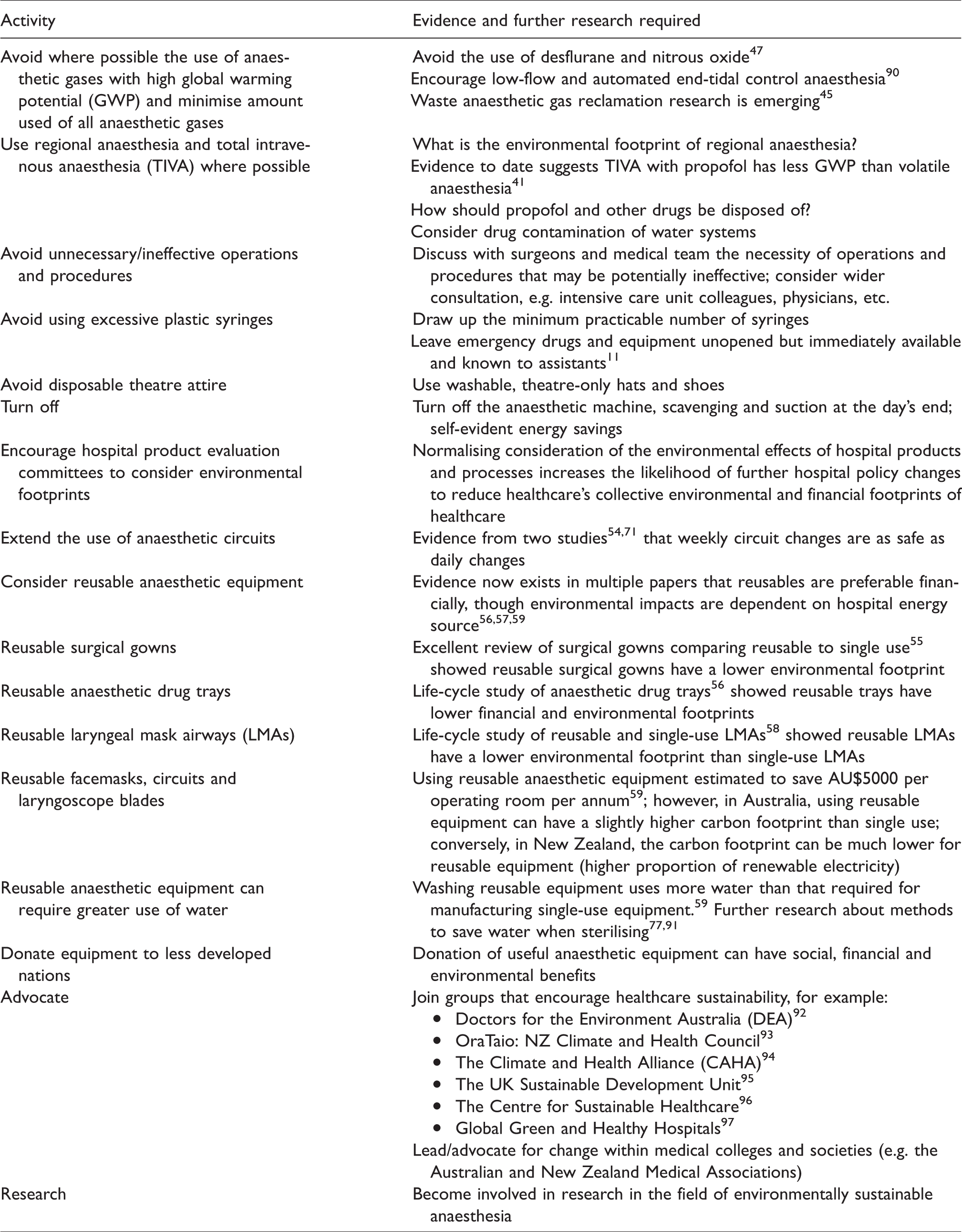
Currently, there are little published LCA data available about the environmental footprint of other pharmaceutical products, including the relative environmental footprints for any drug’s oral versus intravenous preparations, though oral preparations do not require sterilisation. 88 Further research and analysis will create more opportunities for practitioners to instigate informed meaningful change and continually re-evaluate their practice in relation to environmental sustainability. Table 1 gives an abbreviated view of current research and advocacy within the field of environmental anaesthesia.
Improving the environmental impact of anaesthesia.
Conclusion
ANZCA’s PS64 and associated background paper offer an opportunity for anaesthetists to make increasingly well-informed environmental choices in their routine practice. Such environmental choices can be considered alongside individual patient factors, safety, regional versus general anaesthesia, financial and even societal factors when choosing medicines, devices and techniques for individual patients.
Environmentally sustainable anaesthesia requires scholarship, health advocacy, leadership, communication and collaboration. Considerable progress has been made in improving the research, awareness of and advocacy for environmentally sustainable healthcare. Such considerations do not usurp patient-centred or fiscally prudent care, but rather complement such goals by protecting patients, our healthcare system and the environment. 89
Footnotes
Acknowledgements
We thank Kate Davis and Delwyn Lawson, Policy Officers, ANZCA, for coordination and preparation of the ANZCA PS64 and BP documents. Thanks also to Dr. Rod Mitchell (ANZCA President) for reviewing this manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: F.McG. has received grant funding from ANZCA (ANZCA Grant 2018/011) examining methods to capture waste anaesthetic gases.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.