
Abstract
Previous studies have established that bullying is a pervasive problem in healthcare. However, most investigations of bullying in anaesthesia use self-labelled survey questions in which respondents’ subjective perceptions of bullying are central in defining prevalence. This study applied the validated revised Negative Acts Questionnaire (NAQ-r) for a more objective assessment of bullying prevalence and types of negative behaviours experienced by anaesthesia trainees in Australia and New Zealand.
An online questionnaire was distributed by the Australian and New Zealand College of Anaesthetists (ANZCA) Clinical Trials Network to 990 randomly selected ANZCA trainees. Bullying prevalence was assessed using both a self-labelled survey tool and the NAQ-r, which requires respondents to select from a list of negative acts, with validated cut-offs that define bullying. Sources of bullying, impact on recipients and barriers to reporting were also examined. This design allowed comparison of the two methods for evaluating bullying prevalence.
Twenty-six percent of trainees surveyed completed both bullying survey instruments. Thirty percent of these respondents self-labelled as having experienced bullying in the previous six months, with 8% reporting bullying at least monthly. With the NAQ-r, most respondents (96%) reported experiencing at least one negative act in the prior six months, with 54% reporting these on a monthly basis. The most frequent behaviours described were humiliation and intimidation. Using NAQ-r cut-offs, 36% of respondents experienced occasional bullying and 10% were victims of severe workplace bullying.
The NAQ-r provides a more nuanced and objective insight into bullying faced by ANZCA trainees than do self-labelled surveys. The results of the present study provide a valuable baseline for ongoing assessment.
Introduction
In 2015, the Australian Broadcasting Corporation Four Corners television programme ‘At their mercy’ made public the high level of bullying in surgery, shining a light on what is described as an ‘entrenched culture’ within medicine that fosters unreasonable and unacceptable behaviours. 1 The response from the Royal Australasian College of Surgeons led to the Operating with Respect initiative targeting bullying through education and diversity initiatives, with the aim of widespread cultural change. 2
Bullying is a global problem, not just in surgery, and not just in medicine, but across all health disciplines and systems. Consequences are experienced at individual, team and organisational levels. 3 Such behaviours create a risk for patient safety. All specialist medical colleges represented on the Council of Presidents of Medical Colleges have responded with increased resourcing to understand and address this issue. 4 In 2017, an Australian and New Zealand College of Anaesthetists (ANZCA) working group convened to address bullying, discrimination and sexual harassment (BDSH) delivered its final report. 5 This stated the College’s zero tolerance for such behaviours and defined 13 actions to prevent BDSH, protect trainees and respond to inappropriate behaviours.
A central tenet for monitoring the impact of interventions to address BDSH is ensuring clarity on prevalence. Reported bullying prevalence varies widely across medical specialties and experience levels.6,7 For Australian and New Zealand specialist anaesthetists and anaesthesia trainees, published rates vary from 13% to 45%, with the 2017 ANZCA report identifying a rate of 34% in trainees and recent trainees.5,6,8,9
This prevalence variability is multifactorial. A significant influence may be the methods used to measure it, including different time frames (from any time during training to a specified recent period). Most studies rely on so-called ‘self-labelled’ surveys, usually developed by the surveying organisation. Participants are presented with a definition of bullying and asked to indicate whether they have been exposed or not. In some studies participants are asked whether they have experienced bullying, without a definition being provided. 9 Whether or not a definition is provided, reliance on individual understanding of what specific behaviours constitute bullying, particularly within a culture where such behaviours may be tolerated, potentially confounds reported rates.
The purpose of this study was to compare a more rigorous and detailed bullying measure, the revised Negative Acts Questionnaire (NAQ-r), with self-labelled questions in ANZCA trainees. The NAQ-r does not rely on individual understanding of the term ‘bullying’, but, rather, asks about exposure within the prior six months to a series of behaviours, which constitute bullying at thresholds with validated cut-off scores.10,11 This may prove a more reliable measure for longitudinal monitoring of prevalence, including the impact of interventions for prevention and management. In comparison with the binary outcomes of most self-labelled surveys, the NAQ-r also provides detail on the nature of the negative behaviours experienced.
Methods
Approval for this study was obtained from the Royal Perth Hospital Human Research Ethics Committee (EC00270 reference number RGS0000001454). Approval was also granted by the ANZCA Clinical Trials Network, which distributed the survey to a randomly selected sample of 990 from the total of 1602 ANZCA trainees in Australia and New Zealand at the time. Trainees were invited to participate via email and non-identifiable data were collected using SurveyMonkey online software available from www.surveymonkey.com. The survey was open for six weeks from August 2019, with two reminder emails sent. Trainees were informed that the entire survey would take appropriately five minutes to complete. The survey was anonymous and confidential, with potentially identifying data such as IP addresses not collected.
The 18-question survey was presented in three sections. The first section requested demographic data including sex, training stage and training location. The second section, the NAQ-r, was presented prior to any reference to the term ‘bullying’. Following the NAQ-r, the third section included self-labelled bullying questions. The overall survey was titled ‘Working Conditions Survey’ to avoid reference to the term ‘bullying’ prior to NAQ-r completion. Recognising the potential risks associated with asking questions about experiences with negative behaviours, links to trainee wellbeing support resources were included. A copy of the survey is available as Supplementary material online.
The revised Negative Acts Questionnaire
The NAQ-r was designed by Einarsen and colleagues in 2001 to measure bullying prevalence by assessing exposure to an inventory of 22 negative acts that are considered to constitute bullying, without reference to the term. 10 This is a shorter version of the Negative Acts Questionnaire, published by the same research group in 1997. 12 Reported acts are in three categories: ‘work-related’, ‘person-related’ and ‘physically intimidating’ (Table 1). The first category includes work tasks and workload, the second interpersonal behaviours, and the third physically abusive acts. Participants are asked to indicate how often they have experienced each of these 22 behaviours in the prior six months using a modified Likert-like scale: ‘never’, ‘now and then’, ‘monthly’, ‘weekly’ or ‘daily’. Response scores are derived from the number and frequency of negative acts experienced.
Revised Negative Acts Questionnaire (NAQ-r) categories and behaviours.
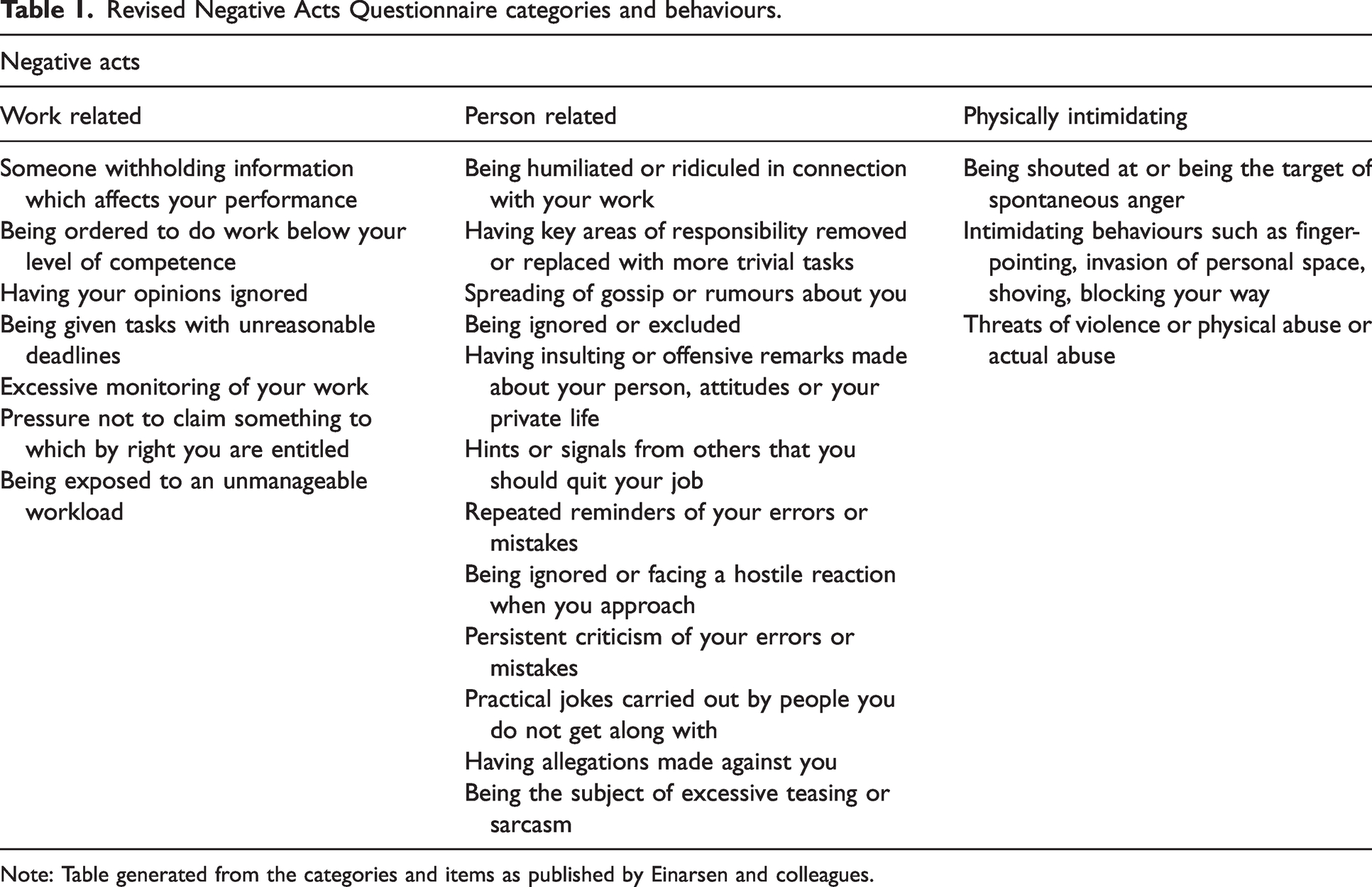
Note: Table generated from the categories and items of the NAQ-r as published by Einarsen and colleagues. 10
The NAQ-r has demonstrated excellent validity, correlating with known impacts of bullying such as increased health complaints and absenteeism. 10 It has high internal reliability. 10
Revised Negative Acts Questionnaire section
Respondents were asked about their exposure to each behaviour and its frequency, as per the NAQ-r methodology. In addition, they were asked to indicate the main perpetrators of these negative behaviours. We applied cut-off scores validated by Einarsen and colleagues, defining their exposures as ‘not bullied’, ‘bullied occasionally’ and ‘victim of workplace bullying’ (also termed ‘severe exposure’). 11
Self-labelled bullying section
The self-labelled questions used in this study were developed using the ANZCA definition of bullying, ‘repeated unreasonable behaviour directed towards a person or group that creates a risk to health and safety’.5,13 Trainees were asked to indicate whether they had been bullied or not. To allow comparison with the NAQ-r, the same Likert-like response categories and time frame (the prior six months) were used.
Participants who reported experiencing bullying in the self-labelled section were asked for details on the role of the alleged perpetrator, the behaviours experienced (exclusion, intimidation, humiliation, threatening, indirect behaviour such as being given the majority of unpleasant tasks or inadequate information to perform their role, and physical behaviours, derived from the ANZCA BDSH policy 13 ), the impact of the bullying, whether the behaviours were reported, and the outcome of reporting, where relevant. Respondents who experienced but did not report bullying were asked why they did not report the behaviours. (This section of the survey was piloted at the institution of the primary author, with 14 of 34 trainees responding. This found that the self-labelled questions were short and unambiguous, with only minor changes to question wording made.)
Analysis
Responses were entered into Microsoft® Excel version 16.65 for analysis of descriptive statistics. ANZCA provided a summary of overall demographic data for all current trainees. Stata Statistical Software (2019, version 16.1, StataCorp LLC, College Station, TX, USA) was used for Fisher’s exact test calculations to compare the sample with the demographics of all ANZCA trainees, and to compare bullying prevalence measured by the NAQ-r and the self-labelled questions. Prevalence results from both the NAQ-r and the self-labelled sections were cross-tabulated to determine whether the same responders were identified by each tool. Demographic results for partial responders were included in the analysis. No missing data imputation was undertaken. Results are reported in accordance with the 2019 Story and Tait Toolbox. 14
Results
Of the 990 ANZCA trainees invited to participate, 274 (28%) opened the survey and provided demographic information. Two hundred and fifty-five respondents (26%) fully completed the NAQ-r section and nine partially completed it. The same 255 trainees who fully completed the NAQ-r also completed the self-labelled section, with no partial completions.
Demographics
Fifty-four percent of respondents identified as female and 45% as male. A majority of respondents were in advanced training (55%), followed by provisional fellowship training (32%), with the remainder being in introductory or basic training (13% combined). Sixty-three percent were under 35 years of age. The Australian states of New South Wales, Queensland and Victoria had the most respondents (26%, 23%, 20%, respectively), with 16% from New Zealand. The sex and geographical distribution of respondents was similar to that of all ANZCA trainees at the time of the survey (Table 2).
Demographics of Bullying in Anaesthesia Registrars Survey respondents compared with all Australian and New Zealand College of Anaesthetists trainees.
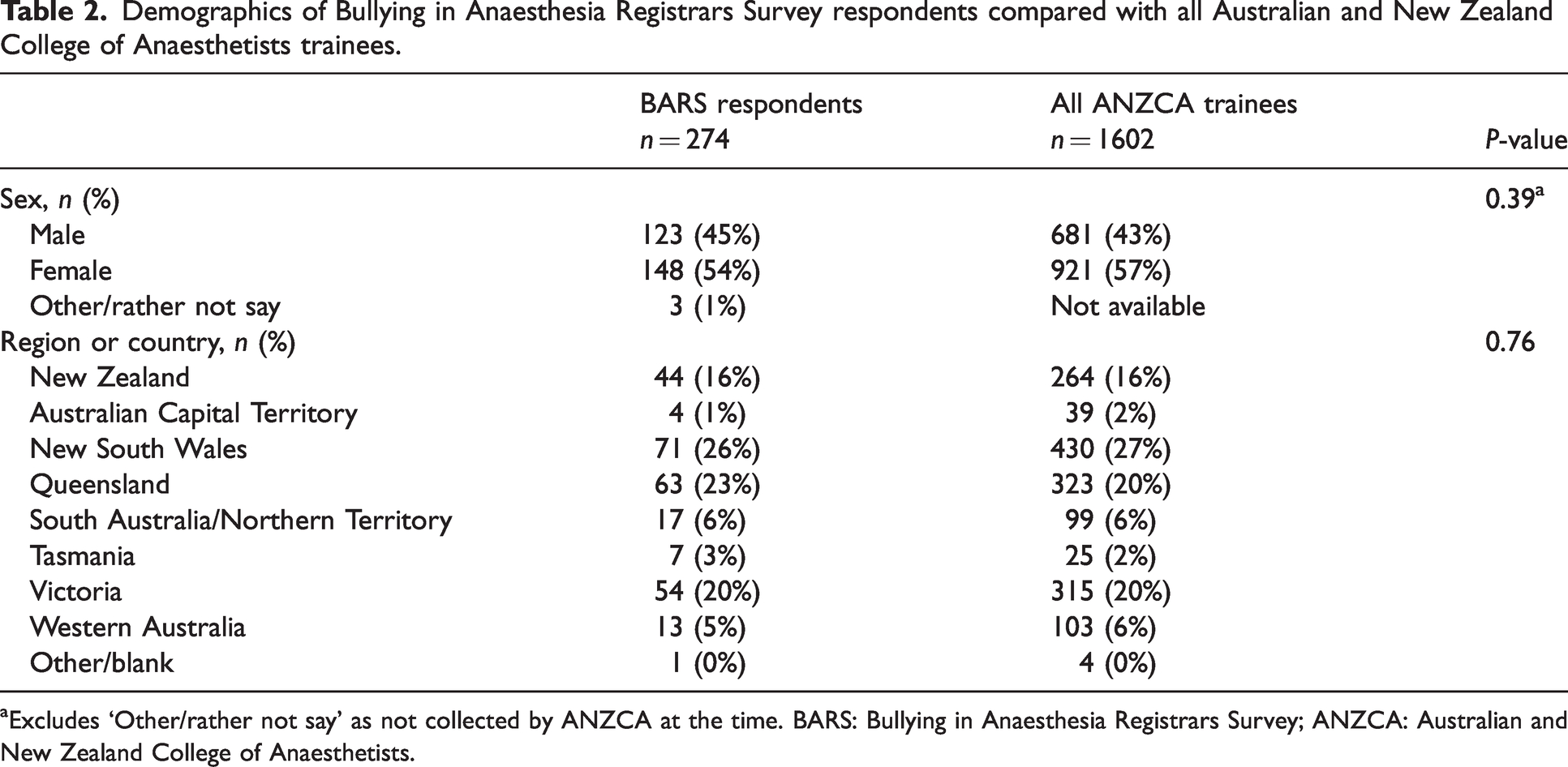
aExcludes ‘Other/rather not say’ as not collected by ANZCA at the time. BARS: Bullying in Anaesthesia Registrars Survey; ANZCA: Australian and New Zealand College of Anaesthetists.
Revised Negative Acts Questionnaire
Ninety-six percent of respondents reported experiencing at least one negative act in the preceding six months, with 35% reporting at least one act on a weekly or daily basis. Thirty-six percent of respondents met the validated cut-off scores for ‘experiencing bullying’, with 26% ‘occasionally bullied’ and 10% meeting criteria for ‘severe workplace bullying’. Table 3 shows the distribution of negative acts by NAQ-r category. Notably, whilst behaviours in all three categories were experienced occasionally, physically intimidating behaviour was less frequently experienced than acts in the work-related and person-related categories. Also, whilst there was a minor decline in the number of trainees who completed the first compared with the third section of the questionnaire, most respondents who started the NAQ-r completed it.
Bullying in Anaesthesia Registrars Survey respondents’ personal experience of negative acts in each category of the revised Negative Acts Questionnaire in the prior six months.a
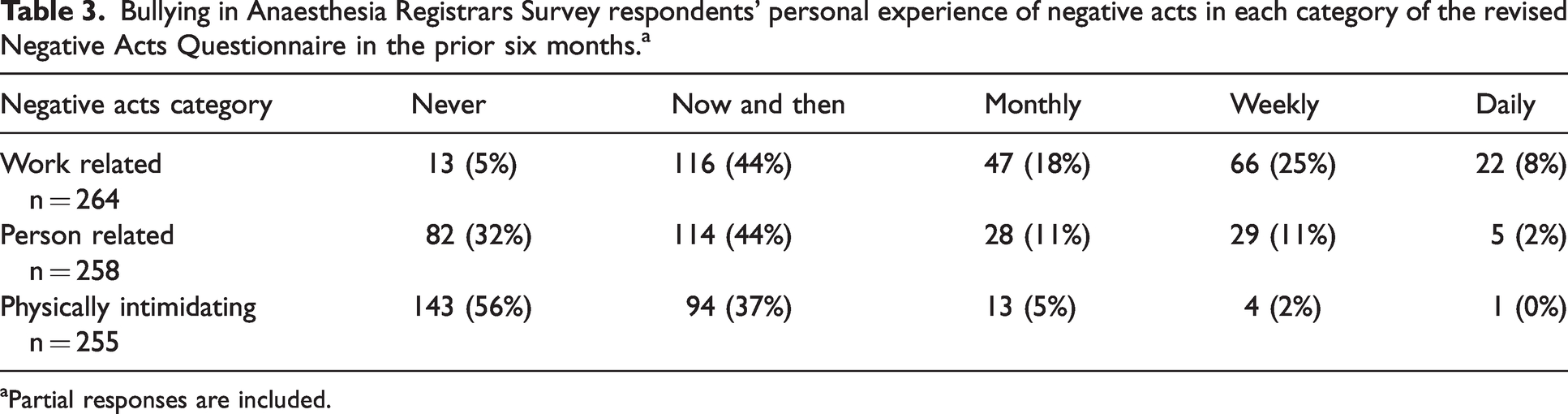
aPartial responses are included.
Self-labelled section
On being provided with the ANZCA definition of bullying, 13 72% of respondents indicated that they had witnessed workplace bullying of others in the prior six months, 18% on at least a monthly basis. During the same time period, 30% reported personally experiencing bullying, with 8% reporting that it occurred at least monthly. Of those self-reporting bullying, 56% identified humiliation, 48% intimidation, 48% indirect behaviours, such as being given the majority of unpleasant tasks, and 32% exclusion. Threatening behaviour was reported by 11% and racism by one respondent, in free text.
Of those reporting personally experiencing bullying in the self-labelled section, common effects cited were increased stress and anxiety, disrupted sleep and decreased confidence. Two respondents indicated that they sought psychological support, three reported considering leaving the training programme, and one stated that they had quit training because of bullying.
In the group who self-labelled as having experienced bullying, more than three-quarters (77%) indicated that they had not reported this within their workplaces. Of those who formally reported bullying, only 24% said the issue was resolved and the behaviour stopped. Twenty-nine percent indicated that the issue was addressed but not resolved and the behaviour continued. Eighteen percent said the issue was not addressed and the behaviour continued. The most common reasons for trainees not reporting bullying were concern about the impact on their careers (25%) or of exacerbating the situation (16%).
Revised Negative Acts Questionnaire compared with self-labelled bullying
The measured prevalence of bullying experienced in the prior six months using the NAQ-r (36%) was not significantly different from that reported in the self-labelled question (30%, P = 0.221). However, the populations identified by each approach were different, as shown in Table 4. Fourteen percent of those who self-labelled as bullied did not meet the NAQ-r cut-off score and 42% of those who met NAQ-r bullying criteria self-labelled as ‘not bullied’.
Comparison of bullying measured by self-labelling and the revised Negative Acts Questionnaire (NAQ-r) in Bullying in Anaesthesia Registrars Survey respondents.

aOne participant selected ‘rather not say’ in the self-labelled section.
Both tools identified a similar ranking of perpetrators of negative behaviours and self-labelled bullying—most commonly anaesthesia consultants (43% of negative acts versus 66% of self-labelled bullying), followed by surgeons (27% versus 34%) and then nurses (22% versus 34%), noting that these are not exclusive categories as respondents could choose all that applied.
Discussion
Approximately one in three ANZCA trainee respondents reported being personally bullied in their workplaces, with similar overall prevalence measured by the NAQ-r and the self-labelled questionnaire. The NAQ-r further elucidated the severity and nature of these bullying experiences, with one-quarter of respondents meeting criteria for ‘occasional bullying’ and one in ten ‘severe bullying’. Furthermore, the negative acts experienced were most often work-related (work tasks and workload) and person-related (interpersonal behaviours), with far fewer trainees experiencing physically intimidating acts. The NAQ-r was completed by most survey respondents, suggesting that it is feasible for use in this population.
Other studies using the Revised Negative Acts Questionnaire in health settings
The NAQ-r was developed and initially validated in employees in a range of non-health industries across the private, public and volunteer sectors in Great Britain, 10 and has also been used in the health sector.15,16 A 2012 study of 370 Australian surgical trainees and consultants found bullying rates of 47% with self-labelled methodology and 38% with at least one negative behaviour daily or weekly, as measured by the NAQ-r. 16 These investigators used different cut-off scores to determine bullying rates from the NAQ-r data. Therefore, direct comparison with our results is difficult. A study of senior salaried doctors and dentists in New Zealand found similar overall bullying prevalence using the NAQ-r and a self-labelled method. 15
In a survey of vascular surgery trainees in the United States of America, the NAQ-r had reported sensitivity of 0.76, specificity of 0.91, positive predictive value of 0.80 and negative predictive value of 0.89, although it is not clear exactly how these values were derived. 17 A study of a range of National Health Service workers (N = 2950) in the United Kingdom used both the NAQ-r and a self-labelled tool. 18 This showed high rates of witnessed and personally experienced negative behaviours, most commonly from a supervisor or manager. There was no direct comparison of bullying rates measured by the self-reported tool and the NAQ-r.
We were unable to identify other research on the NAQ-r in anaesthesia trainees. Consequently, there are no studies in this population for comparison with our findings.
Validation of the Revised Negative Acts Questionnaire in the health setting
Outside the medical workplace there is a significant body of work validating the use of the NAQ-r in a variety of environments and languages. A seminal study of 2539 Norwegian workers was based on the widely accepted premise that bullying significance is primarily manifested in psychological impacts on the recipient of the behaviours. Using combined results from the Hopkins Symptoms Check List-25, a measure of mental health, and self-labelled bullying they developed a standard against which the NAQ-r cut-off scores were derived using Receiver Operating Curves. 11
A small number of studies validate NAQ-r use within health workplaces. Samsudin and colleagues examined the psychometric properties of the NAQ-r in Malaysian junior doctors and found high internal consistency and excellent test–retest reliability. 19 A systematic review and meta-analysis identified 31 studies of the NAQ-r in nurses, although no studies were from Australia or New Zealand. 20 It determined that the NAQ-r is a reliable tool for measuring bullying among nurses, but noted significant methodological heterogeneity. Whilst all studies collected data in a similar fashion, interpretation varied significantly.
Bullying detected by the Revised Negative Acts Questionnaire compared with self-labelling
The trainees identified by the NAQ-r and the self-labelled sections in our study were overlapping but not identical groups. The reasons for this are unknown. Self-labelling relies on respondents recognising and understanding bullying, including that it is a pattern of behaviour that is repeated over time, rather than a single incident. The NAQ-r removes the need for such understanding by asking for reporting of primary behaviours that constitute bullying and their frequency. Those trainees who self-labelled as bullied but did not meet NAQ-r criteria may represent vulnerable trainees nonetheless, as they may be experiencing inappropriate workplace interactions. Those who met NAQ-r criteria but did not self-label as bullied may not understand what bullying is, or bullying behaviours may be so enculturated within their workplaces that they are not recognised as such.
Limitations
The response rate to this survey, whilst similar to that of other ANZCA Clinical Trials Network–distributed surveys, is low. This means there was potential responder bias, with those who have experienced bullying more likely to complete the survey. Alternatively, those who have experienced bullying may be triggered by the topic and less likely to respond. Using the title ‘Working Conditions Survey’ may have mitigated such response bias. Whilst our responders had similar demographic characteristics to the population of all ANZCA trainees, we cannot know whether results are generalisable.
As in most studies of bullying in healthcare, our findings are limited by the cross-sectional design of this study. However, use of a validated tool like the NAQ-r facilitates more robust repeated measurement and future comparisons. 21 Whilst the NAQ-r is not validated in ANZCA trainees, it has been validated in health workplaces and extensively in other sectors.
Implications
Whilst the NAQ-r and self-labelled questionnaires showed similar bullying prevalence, the former provided additional information on both bullying severity and the types of behaviours experienced. These data help quantify the impacts of bullying. The additional information on the negative behaviours experienced may guide interventions to increase awareness of common bullying behaviours and decrease their prevalence.
This study identified higher rates of work- and person-related negative behaviours which align closely with what ANZCA defines as ‘indirect’ bullying behaviours. 13 This suggests that interventions targeting awareness and prevention of indirect rather than direct bullying behaviours may be more necessary and effective. As these doctors are both College trainees and healthcare employees, solutions must be collaborative. As there is cross-disciplinary bullying, interventions must target all health service employees.
While our study provides cross-sectional data on bullying prevalence and characteristics, the NAQ-r has shown excellent test–retest reliability in other medical workplaces, suggesting its value for development of longitudinal data on bullying experienced by anaesthesia trainees. It could be used to evaluate the impact of interventions on the rates and types of behaviours experienced. Validation studies in this population would be useful.
The NAQ-r does not consider race and gender, which are important factors in harassment and bullying.22,23 Smith-Han and colleagues at the University of Otago, New Zealand, addressed this in a study in health profession students. 24 They revised the NAQ-r to incorporate these two additional factors, developing a new instrument, ‘The Clinical Workplace Learning NAQ-r’. Their investigation showed good construct validity and reliability. It may be that this also has better utility for doctors in specialist training.
Conclusions
The NAQ-r provided more information on bullying faced by ANZCA trainees than did self-labelled survey questions. It may also be a more robust tool for repeated measurement. The present study may therefore act as a baseline for the ongoing assessment of negative behaviours and bullying in the workplaces of ANZCA trainees, supporting the creation of valuable longitudinal data.
Our findings provide a reminder that bullying is experienced by ANZCA trainees at unacceptable rates. Such behaviours can have profound negative impacts on recipients and barriers to reporting remain. It is important that all those involved in the training and employment of trainees actively work to reduce negative behaviours, create safe reporting pathways, act appropriately when formal reports are made, and support systems improvements for cultural change.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X221138584 - Supplemental material for The Bullying in Anaesthesia Registrars Survey (BARS): Does a validated questionnaire improve our understanding of bullying in Australian and New Zealand anaesthesia trainees?
Supplemental material, sj-pdf-1-aic-10.1177_0310057X221138584 for The Bullying in Anaesthesia Registrars Survey (BARS): Does a validated questionnaire improve our understanding of bullying in Australian and New Zealand anaesthesia trainees? by Peter BJ Garnett, Scott G Douglas, Richard H Riley, Lindy J Roberts in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Acknowledgements
The authors wish to acknowledge the assistance of Professor Staale Einarsen from the University of Bergen, Norway, for provision of the NAQ-r survey, the ANZCA Clinical Trials Network for survey distribution, and Dr Chang-Yang Yew for statistical analysis.
Declaration of conflicting interests
The authors declared no conflicts of interest in respect to the research, authorship and/or publication.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.