
Abstract
This survey was designed to investigate levels of stress, anxiety and depression, and to identify factors exacerbating or relieving stress in anaesthesia trainees within the Australian and New Zealand College of Anaesthetists training scheme. In addition, the survey investigated levels of personal healthcare, some working conditions, and reports of bullying and reported discrimination along with stigmatisation of mental health issues in this cohort. Psychological distress was assessed using the Kessler psychological distress scale (K10). An electronic survey was sent to 1310 randomly selected registrars, and 417 (32%) responses were received. The majority of respondents (67%) reported being satisfied or very satisfied with their job and training. However, 31% had K10 scores indicating high or very high levels of distress. Eleven percent reported being currently on treatment for anxiety and/or depression. Major stressors were examinations, job prospects, critical incidents and fear of making errors. Forty-five percent of respondents reported having experienced bullying during anaesthesia training, 25% discrimination and 7% sexual harassment. Twenty-six percent reported an excessive workload and 21% reported that they felt their workload compromised patient safety. Forty-two percent reported that they would avoid seeking help for anxiety or depression and 50% reported that they thought revealing mental health problems would jeopardise their careers. The results of this survey demonstrate a high incidence of psychological distress, and high levels of bullying and discrimination, as well as stigmatisation of mental ill health among respondents. Appropriate education, a review of assessment tools, effective management of bullying and discrimination, a review of working conditions, and destigmatisation of mental illness appear to be indicated.
Keywords
Introduction
Doctors interested in gaining specialty qualifications are attracted to anaesthesia for many reasons, including a high rate of job satisfaction, a perceived high standard of practice, collegiality, personal fulfilment and autonomy.1–4 Specialty training programmes can be challenging and consequently stressful, particularly for junior trainees. Challenges such as the high workload, dealing with life-threatening critical incidents and living with the fear of making errors can contribute to significant levels of work-related stress. 5 This stress is often amplified in trainees who invariably, irrespective of their chosen specialty, face regular examinations, work-based assessments and concerns about future job prospects.5–7
McDonnell et al., in a previous survey of 500 Australian anaesthetists, found a 7% incidence of ‘high distress’ or ‘very high distress’ using the Kessler psychological distress scale (K10),8–10 a 13% incidence of diagnosed mental illness with 26% of respondents reporting significant mental health issues during their career. Similarly, the prevalence of depression in physicians is over 28% compared to the lifelong incidence of depression in the general population of 14%.11–13
In the previous welfare of anaesthesia trainees survey conducted in 2015 and published in 2017, 28% of Australian and New Zealand College of Anaesthetists (ANZCA) trainees were identified as having high or very high distress scores using the K10. 5 This level of distress was concerning, but not surprising, given previous findings from the Beyond Blue report on the mental health of Australian medical students and doctors. 14 The Beyond Blue report identified doctors as having a higher rate of anxiety and depression than the general population and identified anaesthetists as second among doctors for suicidal thoughts.
Recently, there have been a number of programmes implemented to improve anaesthesia welfare. These include publication by ANZCA of the bullying, discrimination and sexual harassment (BDSH) working group report and the Doctors’ Support Program, and promotion of mentoring for trainees.15,16
The present study was conducted four years after our 2015 study (published in 2017). It adds to, and compares the findings with the results of the 2017 publication by reassessing the levels of stress, the current stressors, coping mechanisms and factors associated with reduced stress among ANZCA trainees. 5 In addition, limited questions were asked about aspects of personal healthcare, working conditions, bullying and discrimination, and stigmatisation of mental health issues in this cohort. The length of the survey was intentionally short to encourage a high response rate. As a result, additional data were not collected on the nature, timing or resolution of bullying and discrimination, nor on all details regarding adverse events or all aspects of working conditions.
Methods
An anonymous, confidential and voluntary survey was distributed by the ANZCA Clinical Trials Network to Australian and New Zealand ANZCA trainees via email using SurveyMonkey software. A total of 1310 trainees were invited to complete the survey.
The survey questions were based on those used in our 2015 survey, with changes made in the present study to obtain greater detail in identified areas of concern such as self-prescribing of medications, bullying, discrimination and sexual harassment, and negative coping strategies such as excessive alcohol consumption. The questions included demographics, personal health, treatment for anxiety or depression, perceptions about notification of mental ill health, factors which may exacerbate stress such as bullying, and coping strategies (see Supplementary material). Participants were asked to rate their exposure to a number of training and workplace stressors as minimal, moderate, or severe and select options from a number of coping strategies they used. Finally, psychological distress was assessed using the K10. The K10 has been used to assess the psychological wellbeing of anaesthesia trainees in a number of similar studies,5,10 also in broader medical staff 14 and the general population. 17 The K10 asks respondents to rate each of ten questions related to their psychological state in the previous four weeks using a five-point Likert scale from ‘none of the time’ to ‘all of the time’. A total score is given between 10 and 50. A score of 10–15 indicates low distress, 16–21 moderate distress, 22–29 high distress and 30 or above very high distress. 17 Those with a high distress score may be experiencing levels of distress consistent with a diagnosis of a moderate depressive or anxiety disorder. Those with a very high distress score may be experiencing levels of distress consistent with a diagnosis of a severe depressive or anxiety disorder. 18
All fully completed surveys were included in the study. Participants who had only partially completed the survey had all fully completed sections included in the analysis. A total of 417 surveys were included in the study, of which 400 were fully completed.
Ethical approval for the survey was obtained from Western Sydney local health district, human research ethics committee (HREC) (reference no. LNR/18/WMEAD/445). In addition, approval to conduct the study was given by the ANZCA Clinical Trials Network, who distributed the survey via email. The survey was conducted between 5 April 2019 and 17 May 2019. Only non-identifiable data were obtained and the confidentiality of the survey was guaranteed using SurveyMonkey.
A total of 1310 surveys were distributed out of a total of 1589 active ANZCA trainees. To obtain an alpha level of 0.05 with a margin of error of 5%, it was calculated that 310 responses were required for the given population studied. 19
Statistical analysis was conducted using a chi-squared goodness of fit test on the statistical computing program R. 20
Results
A total of 417 survey responses were received from 1310 trainees, giving a response rate of 32%. Forty-nine percent of respondents were men (which is the same as the gender split for the entire ANZCA trainee population of 1589). A total of 142 responses were from basic trainees (34%), 144 from advanced trainees (34%), 95 from provisional Fellows (23%) and 34 from Fellows in their first year (8%). Only two responses (0.5%) were from introductory trainees. The number of respondents in a committed relationship was 347 (83%): men 181, women 166. A total of 145 respondents (34%) had children (the same as in our previous study: men 89, women 56).
A total of 268 respondents (65%) had visited their general practitioner (GP) in the previous 12 months (men 111, women 157) (a slight increase from our previous study, 59%). A total of 105 respondents (25%) reported not having a regular GP; 149 respondents (36%) reported they had self-prescribed medication in the past year: antibiotics were the most commonly self-prescribed medication (12%), followed by oral contraceptives (10%), proton pump inhibitors (10%) and non-opioid analgesics (5%) (this pattern mirrored our previous study). Three respondents reported self-prescription of opioid analgesics. Several respondents self-prescribed anxiolytics (n = 4) or antidepressants (n = 14); 46 respondents (11%) reported self-referring for tests or to specialists.
Sixty-seven percent of respondents reported being satisfied or very satisfied with their job and training and 24% were neutral. This leaves only 9% of respondents who reported being unsatisfied or very unsatisfied (down from 13% in the previous survey).
A total of 173 respondents (42%) were planning on sitting either the Primary or Fellowship examination in the next six months. Eighty-four (34%) of these had at least one previous attempt.
A total of 123 (31%) respondents were identified as having a K10 score consistent with high or very high distress (>22) (which is similar to the 28% reported in our 2017 publication). Very high K10 scores (>30) were identified in 10% of respondents (up from 8% in the 2017 publication).
High and very high K10 scores were associated with being on treatment for anxiety and/or depression (χ2 (1, n = 123) = 6.74, P < 0.01), often working unsafe hours (χ2 (1, n = 123) = 6.48, P < 0.05), being unsatisfied with their job (χ2 (1, n = 123) = 33.088, P < 0.001), and sitting the examinations (χ2 (1, n = 123) = 8.9905, P < 0.005).
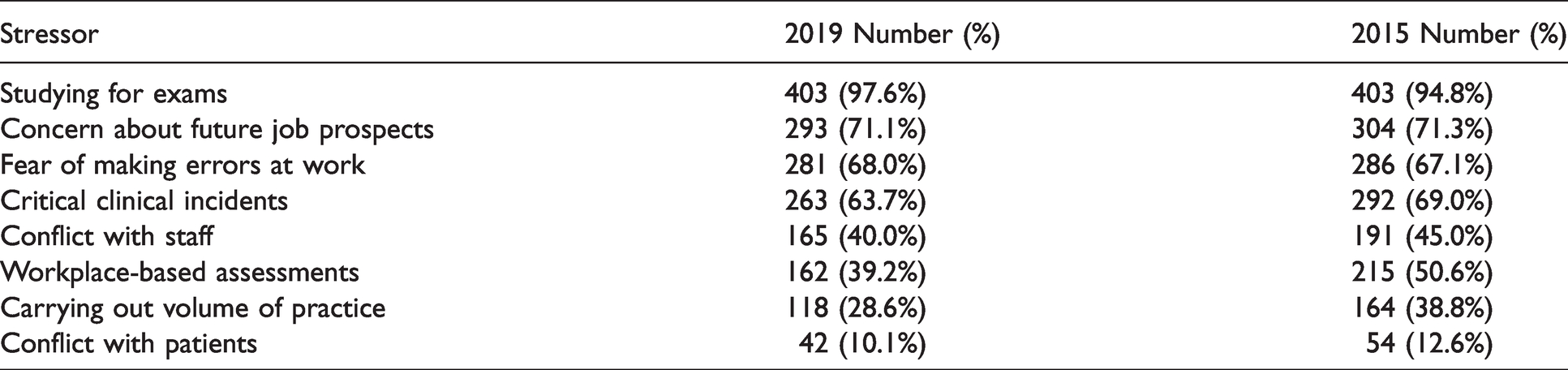
The most common stressors were studying for examinations and future job prospects (see Table 1).
Causes of moderate or severe stress 2019 and 2015.
Forty-five respondents (11%) reported currently being under treatment for anxiety or depression (the same percentage as in our previous study). One hundred and five (26%) had received treatment in the past. Half of the respondents (207) reported that they thought revealing a potential diagnosis of depression or anxiety to their department would jeopardise their career and 42% of respondents stated that they would avoid seeking help for anxiety or depression due to privacy issues.
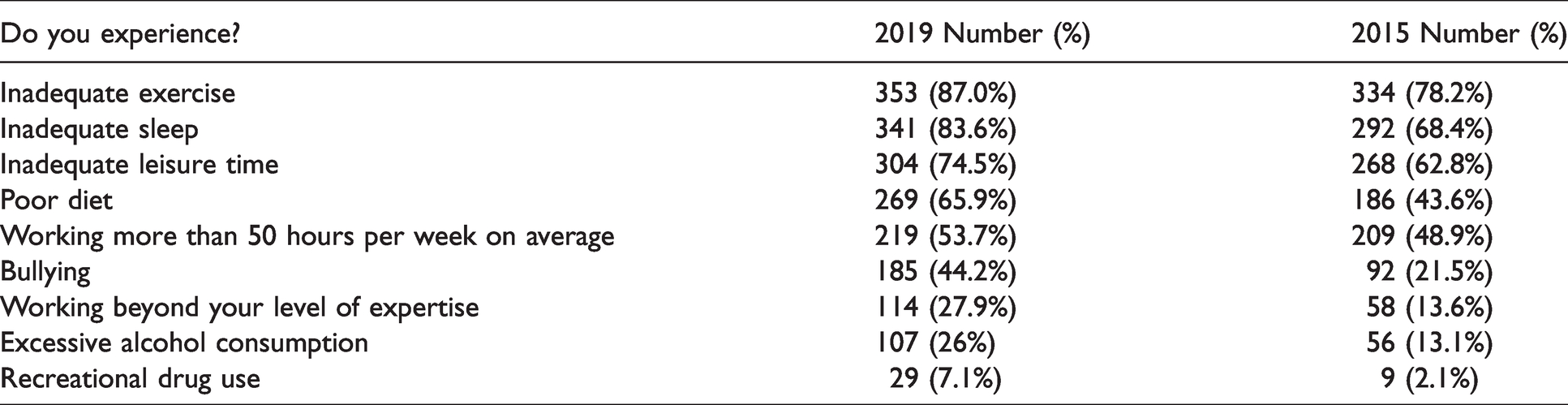
Eighty-four percent of respondents reported inadequate sleep, with only 6% having enough sleep on six or more nights of the week. Forty-six percent reported only obtaining enough sleep on two or fewer nights per week.
In their past year, 87% of respondents reported inadequate exercise, 75% reported inadequate leisure time and 66% reported a poor diet. Fifty-four percent worked more than 50 hours per week on average, with 28% reporting they have worked beyond their level of experience. Excessive alcohol consumption was revealed in 26% or respondents, with 7% (29 respondents) admitting to recreational drug use in the last 12 months (see Table 2). (It should be noted that the survey did not distinguish between single instances and ongoing practices. Also some respondents may have interpreted ‘in the past year’ as ‘year to date’ as opposed to 12 months. It should not be interpreted that these issues were present all the time.)
Personal health in the workplace 2019 and 2015.
A total of 179 respondents (44%) were involved in an adverse patient event causing iatrogenic injury or near miss in the past year. Eighty-five percent of these events were reported. Of the 179 respondents who did report an adverse event, 65% reported being given appropriate institutional support subsequently. Seventy-nine respondents (44% of those experiencing an event) reported ongoing anxiety or guilt due to the event.
Workplace bullying was reported by 45% of respondents (significantly increased from our last study, 22%). Discrimination was reported in 25% of respondents and almost 7% reported sexual harassment. (These data relate to all of the period of anaesthesia training for each individual as opposed to a particular time frame and, in addition, did not stipulate single or persistent events or severity and resolution.)
Leave was reported as difficult to access by 35% of respondents, with only 54% of respondents accessing four weeks or more leave in the past year. Seven percent of respondents accessed less than two weeks annual leave in the past year, improved from our last survey (15%). (It should be noted that data were not collected about the reasons for difficulty accessing leave such as department workload, inconvenient timing or trainee choice.) Twenty-six percent of respondents reported that they felt that their workload was excessive (increased from 19% in the last survey) and 20% felt their workload compromised patient safety (increased from 15% in the last survey). Unsafe hours, defined as working hours putting staff at risk of fatigue, were reported by 27% of respondents.
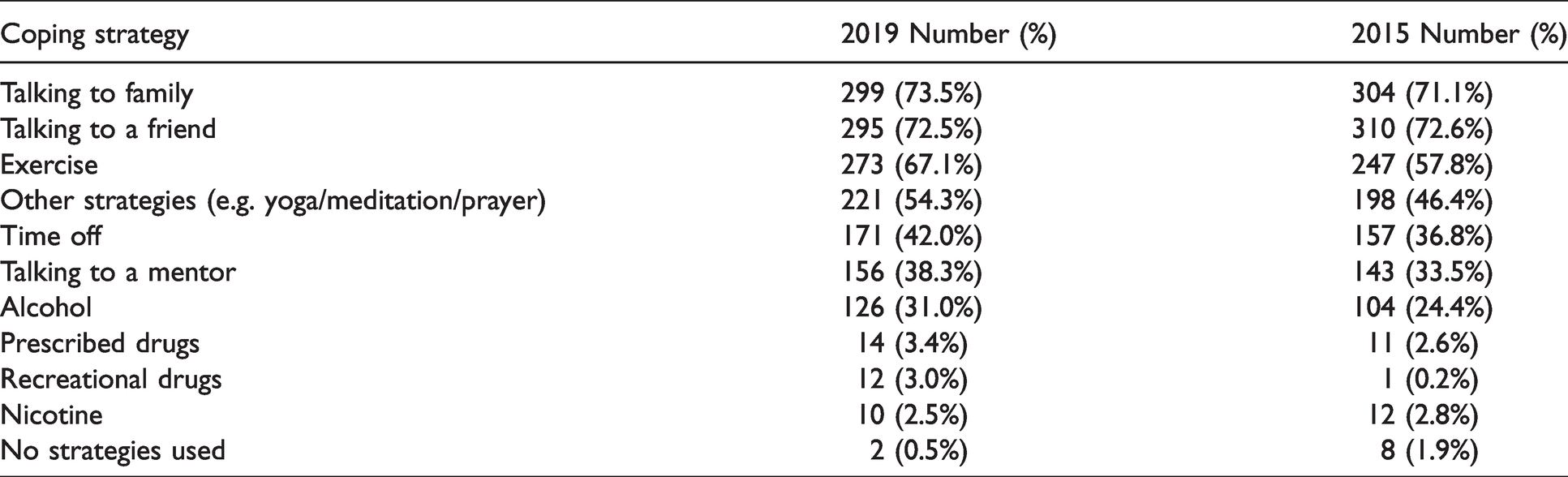
Coping strategies used to handle stress were similar to our previous study. Talking to family or a friend were the most common, with 74% and 73% of respondents utilising these strategies, respectively. Alcohol was used by 31% of respondents; 3.4% used prescribed drugs and 3% used recreational drugs (see Table 3).
Coping strategies used to handle stress 2019 and 2015.
Discussion
In this survey of ANZCA trainees, almost a third of respondents reported high (21%) or very high (10%) distress according to the K10 instrument, with a 1:1 male to female incidence. This is similar to the incidence in our 2015 survey, 5 but far outweighs the reported incidence in other surveys assessing anaesthesia consultants and trainees combined.10,14 McDonnell et al. reported high or very high scores in only 7% of anaesthetists and anaesthesia trainees combined. 10 The Beyond Blue survey of doctors’ mental health found very high K10 scores in 4.8% of all doctors and medical students aged 18–40 years, 5.6% in all trainees, 3.8% in anaesthetists (the second highest after oncologists). 14 The Australian Health Survey of 2018 revealed that 3.4% of the general population in the 25–34 year age group had very high K10 scores. 21 This compares to 10% in the present study. On a more positive note, it was pleasing that two-thirds of respondents reported being satisfied with their job and training and only 9% of respondents reported being unsatisfied. This was reflected also in the Medical Board’s Training Survey 2019. 22
The 31% incidence of high or very high K10 scores in the present study would indicate a high incidence of anxiety and affective disorders according to the World Health Organization (WHO) Composite International Diagnostic Interview (CIDI). 23 This indicates that a significant number of trainees are at risk of the consequences of mental ill health, including isolation, alcohol or substance abuse, relationship breakdown and suicide. This is a disturbing finding and raises a red flag to all of us who are involved with the teaching or mentoring of trainees.
In the present survey, 11% of respondents reported being currently treated for anxiety or depression and 26% reported having been treated previously for anxiety or depression. It should be noted, however, that we cannot exclude the possibility that respondents with anxiety would be more likely to respond, thereby providing a biased sample (responder bias).
It would be of interest to compare K10 scores of trainees as well as anxiety or depression scores in other training programmes to determine if they are at similar risk of mental health problems. Many of these issues may not be unique to anaesthesia trainees. Such data are unavailable at the time of publication. It would be beneficial to know whether the K10 scores reported in this survey are higher or lower than in other specialties or professions. Further research is indicated in this area.
Of the 100 respondents with high K10 scores, 77 reported that they were not under treatment for mental health issues. This discrepancy could indicate that a large proportion of trainees have untreated mental health problems. This is further compounded by 58% of respondents reporting that they would avoid seeking help for anxiety or depression. The potential reasons for avoiding seeking help are multiple and include stigmatisation (half of the respondents indicated that reporting a diagnosis of anxiety or depression would jeopardise their career), embarrassment, inability to recognise symptoms, a preference for self-reliance, 24 concern regarding Australian laws on mandatory reporting of mental health problems, and fear of jeopardising future insurance claims. 25 Of those with high or very high K10 scores, a number of factors were associated: low job satisfaction (13% of high K10 respondents), working unsafe hours (24% of high K10 respondents), sitting or re-sitting examinations (60% of high K10 respondents) and being on treatment for anxiety or depression (11% of high K10 respondents).
As in our 2015 survey (published in 2017), examinations (98% of respondents) and future job prospects (71% of respondents) were the most frequently reported causes of stress, followed by critical incidents and fear of making errors. The examination system is an arduous method of assessment, common to most medical fraternities, and with a significant failure rate. The prospect of failure may be foreign to the vast majority of trainees who may never have experienced academic failure previously. The stress of the examination process, particularly if associated with failure, may put many trainees at risk of mental ill health and its sequelae. A review of the examination process with a view to reducing this stress would appear beneficial. This could entail a greater focus on workplace assessment and commensurate reduction in the importance of examinations. Of course, any review of the examination process would have to ensure the same standard of competence for trainees in order to ensure patient safety. There are already extensive resources available to trainees and teachers on study technique, stress reduction and managing failure through ANZCA, the Australian Society of Anaesthetists (ASA) and other professional organisations.16,26
The problem of job prospects and workforce issues has been highlighted previously by the ASA and ANZCA.27,28 Respondents to the present survey have also indicated it remains a cause of stress in the vast majority. However, anaesthesia trainees are not alone in this regard. The 2019 Medical Training Survey showed that although 46% of all trainees were concerned about job prospects, it was of greater concern to physicians (70%), surgeons (63%) and anaesthetists (63%). 22
Forty-four percent of respondents reported they had been involved in an adverse patient event or near miss in the previous year. Of those, 85% of respondents reported them, and 71% reported being given institutional support. Nonetheless, of the respondents who had been involved in an adverse event or near miss, 44% reported that the adverse event had caused them ongoing anxiety or guilt. Care should be taken in interpreting these data as the survey did not determine either the duration or the severity of harm occurring as a result of the iatrogenic injury, and that this might explain the disparity in institutional support or ongoing anxiety or guilt. The practice of anaesthesia, as in other areas of medicine, may be associated with exposure to poor patient outcomes because of: the nature and severity of patient illness; limited resources and personnel in some hospitals; the timing of medical interventions; the potential for incorrect diagnoses; inappropriate medical management; and medical error or oversight. The term ‘second victim’ has been coined to describe those practitioners adversely affected by critical incidents and errors. 29 The management of the second victim requires adequate training in preparation for such events such as training in how to cope with adverse patient outcomes, a culture of support and transparency when investigating such adverse events, open access to debriefing after events, and ongoing monitoring of the second victim’s emotional state. The high percentage of respondents who reported ongoing anxiety or guilt following an adverse event or near miss would indicate that current training, management and monitoring of the second victim is deficient in at least some institutions.
A wide variety of strategies can be used for stress reduction.5,30–33 In this survey, the commonest coping strategies that respondents reported were talking to friends or family, exercise or taking leave. Over half of respondents used other techniques such as yoga, prayer, meditation, counselling, hobbies and unfortunately ‘crying’. It is of concern that alcohol was used for stress relief in 31% of respondents. A lack of availability and training of mentors may have partly contributed to this result. In addition, the high K10 scores reported in this study would tend to indicate an inadequacy of coping techniques employed by the majority of respondents. Whether this was a result of components of their job and training or was partly or wholly due to other factors was not determined by this survey. Similarly, whether these are present in other areas of the workforce was not determined.
This survey asked about lifestyle practices as an indicator of adequacy of response to, and management of, stress. It revealed poor lifestyle practices of poor diet (65% of respondents), inadequate exercise (85% of respondents), inadequate leisure time (73% of respondents), inadequate sleep (82% of respondents reported four nights or less per week of adequate sleep) and excessive alcohol intake (26% of respondents). The proportion of trainees experiencing these issues has increased since our 2015 survey. 5 It should be noted, however, that data about the causes of these lifestyle practices were not collected and may well be due to factors unrelated to anaesthesia training. In addition, 35% of respondents reported having difficulty accessing leave and 23% of respondents reported having two or fewer weeks of annual leave per year.
The results from this survey appear to indicate that, assuming the sample and respondent characteristics are similar, work practices have not improved in the four years since our 2015 survey. 5 Twenty-six percent of respondents reported their workload was excessive, 52% of respondents worked more than 50 hours per week, 25% reported working beyond their level of experience and 21% reported they felt that their workload compromised patient safety. It should be noted that in the Medical Board survey, working more than 50 hours a week occurred in 28% of anaesthesia trainees, 41% of physicians and 82% of surgeons. As was reported in our previous survey, it is well recognised that a heavy workload causes negative consequences due to fatigue. ANZCA’s professional document, ‘Guideline on fatigue risk management in anaesthesia practice PS43’, 34 highlights the need for departments to adhere to safe work practices. It also calls attention to the fact that safe patient care is jeopardised by anaesthetists who work while severely fatigued, stressed or unwell.
Bullying was reported by almost half of trainees during training (45%) with 25% reporting discrimination and 7% reporting sexual harassment. These high figures are unfortunately consistent with other studies, further underlining the endemic nature of these issues.5,35,36 Despite the publication of ANZCA’s BDSH report in 2017, 15 the continued high rates of bullying and discrimination could be at least partly responsible for the high K10 scores in this study. Unlike other stressors faced by trainees, such as exposure to adverse events and examination requirements, which are unavoidable, distress cause by bullying, discrimination and sexual harassment can be mitigated by reducing its presence in the workplace. However, the survey was not designed to differentiate whether these adverse experiences were isolated events or persistent practices. Similarly, the survey was not designed to assess their severity, whether they had been reported through appropriate channels, or the outcomes following reports and investigations if they occurred (i.e. the survey did not ask about the severity of these adverse experiences, whether they were reported, and if so whether there had been a satisfactory response to the report). Nevertheless, any such behaviour of any time scale or severity is unacceptable. Resources focused on reducing these rates at both a hospital and department level could therefore have a significant positive effect on trainee wellbeing.
Self-care, self-prescribing and self-referral are common practices among medical practitioners. Putting work before personal health (so-called ‘presenteeism’) 37 and the trivialisation of their own illnesses put doctors at considerable risk of poor outcomes for personal ill health.35,36 ANZCA professional document PS49 makes recommendations about finding and attending a GP, avoiding self-prescribing and appropriate referral to specialist care when required. 38 In the present study, 75% of respondents reported they have a GP and 65% reported they have seen their GP in the past year. It is pleasing to note that this is an increase compared to our 2017 study. It is also pleasing to note a reduction in self-prescribing (36% of respondents). However, although the commonly prescribed drugs were antibiotics, oral contraceptives, proton pump inhibitors and non-opioid analgesics, it is concerning that 18 respondents reported self-prescribing antidepressants or anxiolytics and four reported self-prescribing opioid analgesics.
It is self-evident that the time period of anaesthesia training will end with progress to consultant practice, with consequent cessation of stressors inherent in that training. However, the training period is not short, in most cases encompassing five years after junior residency. Trainees are predominately in their 20s or 30s during training, an age when they will be involved in establishing relationships, potentially marrying, having children and establishing a home. These activities have their own issues of stress, as well as happiness. These stressors can compound those involved in anaesthesia training and may in part be responsible for the high K10 scores reported here. The stress of this training period may result in serious adverse sequelae for some, including depression, anxiety, substance abuse, self-harm or even suicide. Moreover, despite the limited time period of anaesthesia training, these potential sequelae may persist into consultant practice and be exacerbated by poor job prospects, the need to establish a practice and stresses inherent in consultant practice.
It is relevant that this survey was undertaken in 2019 prior to the coronavirus disease 2019 (COVID-19) pandemic that has led to an unprecedented increase in workplace difficulties, interrupted training, delays in examinations, and the many social consequences of lockdowns and social distancing. Those consequences include increased future job insecurity, fear of exposure to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), shortages of appropriate personal protective equipment (PPE), and also disruption in ability to debrief with colleagues due to social distancing. The cancellation and delays in examinations, as well as alterations in their format might be anticipated to cause particular difficulties given that examinations are one of the major areas of stress. It is possible even more trainees than those in this survey are experiencing distress. Further studies are needed to assess the true impact of the present extraordinary circumstances.
This survey was a follow-up to the preceding Welfare of Anaesthesia Trainees study performed in 2015 and published in 2017. It is discouraging that potentially very little has changed in the four years since that survey. This survey acts as a reminder to organisations, hospitals, departments and to individuals, that work is still needed to improve trainee wellbeing.
Preventive strategies for stress management and resilience training have been suggested at an early stage in medical training. 30 Strategies that could be beneficial include mindfulness interventions,31,32 interpersonal communication, 31 reflection groups, promotion of self-care 38 and resilience training. 33 In addition, preventable stressors such as workplace bullying, if reduced, could result in a significant improvement in trainee stress.
ANZCA has formulated or adopted programmes designed to improve wellbeing of trainees and Fellows alike. The Doctors’ Health and Wellbeing Framework underpins a number of resources and initiatives including the Trainee Wellbeing Project Group, the Doctors’ Support Program and the Wellbeing Special Interest Group. 39 ANZCA’s policy on bullying, discrimination and harassment provides definitions, advice and resources to combat this ongoing problem. 40 The Long Lives Healthy Workplaces toolkit, an initiative of ANZCA’s Wellbeing Special Interest Group and Everymind and supported by the ASA is designed to improve wellbeing through targeted interventions. 26 The lack of any significant improvement in wellbeing among respondents between this survey and that conducted four years earlier would suggest that there has been either insufficient time for these programmes to have effect, that there is insufficient uptake by the anaesthesia community, and/or that there needs to be further changes in the assessment process, working conditions, management of the second victim, personal lifestyle practices and adherence to ANZCA guidelines on topics such as bullying and fatigue. On the other hand, 67% of respondents reported being satisfied or very satisfied with their job and training and 24% were neutral. Only 9% of respondents reported being unsatisfied or very unsatisfied, which was down from 13% in the previous survey.
This study has several limitations, some of which have been mentioned above. Surveys such as that used in the present study are inherently associated with sources of bias, specifically response bias. As mentioned, we cannot exclude the possibility that respondents with anxiety would be more likely to respond, thereby providing a biased sample. Questions on bullying, discrimination and sexual harassment encompassed all of anaesthesia training and were not restricted to a particular time frame. This could also bias the data. Care should be taken when comparing anaesthesia training to other specialties as data for these are not available. Given the low response rate to this survey, caution should be exercised when interpreting it. In particular, the findings do not necessarily apply to introductory trainees for whom there was a very low response rate. However, every effort was made to obtain an adequate and unbiased sample. Providing a snapshot of trainee welfare, the timing of the survey and its relationship to examinations and job applications could also be a source of bias. However, the timing of the study was carefully selected to be at a time with the least amount of examination interruption in consultation with ANZCA. Because of the gaps between examinations and vivas and the six–12-month period during which trainees study for examinations, this is likely to be a constant throughout every training period.
It is also important to note that the study does not test any hypotheses in relation to specific factors that might influence stress such as gender or level of training; any observations we have made in this regard should be interpreted with caution. The survey, as with any survey, relies on reliable responses from respondents and not formal diagnosis of conditions or observation and confirmation of trainee behaviour. These limitations indicate that the findings should be interpreted with caution.
Conclusion
This study has shown that high levels of psychological distress persist in this cohort of anaesthesia trainees, with high K10 scores in nearly one-third of respondents. Many respondents reported bullying or discrimination as well as poor lifestyle practices and excessive alcohol consumption. Stigmatisation of mental health problems and concerns about career prospects if reporting them were issues for many respondents. Despite this only a small minority were unsatisfied with their job and training.
Even though the response rate to this survey was low, the authors believe that the above results and conclusions are of relevance and pertinent to all ANZCA trainees.
Anaesthesia departments need to maintain awareness of the difficulties trainees may be experiencing, and their reticence to seek help. Constant vigilance is needed within departments to identify problems and modify work practices and workplace behaviours as much as possible. The trainees also need to take responsibility for their personal wellbeing by taking appropriate self-care. Most of our suggestions for reducing stress among anaesthesia trainees are already in place. Programmes are available within ANZCA to improve wellbeing, particularly the Doctors’ Health and Wellbeing Framework and the Long Lives Healthy Workplaces toolkit. In the light of our findings of continued high levels of stress, the anaesthesia community needs to be aware of these programmes, adopt them and diligently enact them.
Footnotes
Author Contribution(s)
Acknowledgements
The author(s) would like to acknowledge the assistance of the ANZCA trials group.
Declaration of conflicting interests
The author(s) have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
Supplementary material for this article is available online.