
Abstract
At teaching hospitals, consultants must provide effective supervision, including appropriate selection of teaching cases, such that the outcomes achieved by trainees are similar to that of consultants. Numerous studies in the surgical literature have compared patient outcomes when surgery is performed by consultant surgeons or surgical trainees but, to our knowledge, none exist in the field of anaesthesia. We aimed to compare analgesia outcomes of regional anaesthesia when performed by supervised trainees versus consultants. We designed a retrospective observational study using registry data. The primary outcome was inadequate analgesia, defined as a numerical rating scale (NRS) for pain >5 reported at any time in the post-anaesthesia care unit (PACU). Secondary outcomes included the maximum pain NRS, pain experienced in the PACU, and the requirement for systemic opioid analgesia in the PACU. Of the 1814 patients analysed, the primary proceduralist was a consultant for 514 (28.3%) patients and a trainee for 1300 (71.7%) patients. All trainees were supervised by an on-site consultant. There were no statistically significant differences between consultants and supervised trainees in terms of the primary outcome (NRS >5 in 24.9% and 24.5% of patients, respectively; P = 0.84) and secondary outcomes. Compared to trainees, consultants had a slightly higher rate of patients with a body mass index >30 kg/m2, an American Society of Anesthesiologists Physical Status Classification of 3 or 4, nerve blocks performed under general anaesthesia, paravertebral/neuraxial blocks and blocks with perineural catheter placement. Regional anaesthesia performed by supervised trainees can achieve similar analgesia outcomes to consultant-performed procedures.
Introduction
Consultant doctors have a professional duty to practise medicine safely and effectively. 1 This is enshrined in the concept of the ‘primacy of patient welfare’ 2 that places the interests of patients before that of clinicians. A competing obligation of the consultant is to teach the next generation of doctors. 3 This includes supervising procedures performed by trainees with varying degrees of experience. Inexperience, however, is associated with poorer outcomes, as illustrated by the existence of learning curves for medical procedures. 4 If one accepts that consultants are generally more proficient at performing procedures than trainees, an ethical dilemma arises. 3 The principle of nonmaleficence (potential for poorer outcomes in the current patient) compels the consultant to perform the procedure independently. Conversely, beneficence (trainee education, improved future patient outcomes) strengthens the argument that the trainee should perform a supervised procedure.
In the field of regional anaesthesia, there are procedural errors known to be common amongst trainees. 5 Consultant anaesthetists must therefore judge the proficiency of trainees, the complexity of patients and the context of the case before making the decision that the trainee should conduct the procedure as the ‘primary proceduralist’. After appropriate case selection, consultants must then provide the correct level of supervision to trainees during the procedure. If consultants are successful in doing these tasks (i.e. if they demonstrate effective supervision), the outcomes achieved by trainees should be similar to that of consultants.
Despite calls to develop a system that supports effective clinical supervision, 6 we are not aware of any studies in clinical anaesthesia that directly compare patient outcomes for procedures performed by consultants or supervised trainees. The surgical literature, however, has studied this extensively. Numerous studies have compared patient outcomes when surgery is performed by consultant surgeons versus surgical trainees.7–15
This study aimed to employ concepts similar to that used in the surgical literature but in the field of regional anaesthesia. We aimed to compare analgesia outcomes of regional anaesthesia procedures performed by consultant anaesthetists versus supervised trainees on the patient cases they were assigned. Supervised trainees were those who had an on-site consultant present. The primary outcome was inadequate analgesia in the post-anaesthesia care unit (PACU). We also evaluated opioid consumption in the PACU. The null hypothesis was that patient regional anaesthesia outcomes would be similar between the two groups; the alternate hypothesis was that one group would outperform the other.
Methods
This single-centre retrospective observational study was undertaken at the Royal Brisbane and Women’s Hospital (RBWH). The checklist for Strengthening the Reporting of Observational Studies in Epidemiology 16 was utilised. The RBWH is a tertiary university-affiliated teaching hospital with a dedicated Regional Anaesthesia Service that employs a ‘block room’ or ‘block team’ model. 17 The regional anaesthesia service is a consultant-led, in-hours (Monday to Friday, 0730–1800) service with a rostered consultant and registrar. The service utilises an electronic point-of-care data entry system to maintain a registry for all procedures performed. Data from consecutive patients are entered into the registry by treating clinicians on completion of the regional technique. Ethical approval was obtained from the RBWH Human Research Ethics Committee (LNR/2018/QRBW/47004) and waiver of consent approved.
Registry data included the type of regional anaesthesia procedure, patient details and clinician details. Consultant and trainee presence was documented. The registry included a specific question regarding which clinician was the ‘primary proceduralist’. Data were recorded after the regional anaesthesia procedure but before the patients’ surgery and before the primary outcome of this study was known. Nursing staff independently gathered PACU data that included numerical rating scale (NRS) for pain and the requirement for opioid analgesia.
If a trainee was the primary proceduralist, the level of supervision was at the discretion of the consultant. This may have ranged from remote supervision to verbal advice or ‘hands-on’ assistance. The Australian and New Zealand College of Anaesthetists (ANZCA) training handbook 18 recognises four levels of supervision (level 1: the ability to intervene immediately; level 2: the ability to intervene quickly; level 3: on-site availability; level 4: off-site availability) and recommends that all clinical work as part of ANZCA training be supervised at an appropriate level. All trainees in our regional anaesthesia service have consultant supervision. Our institutional culture aims for the majority of our trainees to have direct supervision such that the supervisor could intervene immediately, similar to ANZCA level 1 supervision. If a consultant does not directly supervise a trainee but is available in accordance with ANZCA level 3 supervision, this is recorded in our data entry system as ‘remote supervision’.
The primary outcome was inadequate analgesia, defined as an NRS >5 reported at any time in the PACU. This outcome has been previously used as an indicator of quality of regional anaesthesia.17,19 Secondary outcomes included the maximum NRS in the PACU, the presence of pain at any time in the PACU, and the requirement for systemic opioid analgesia in the PACU. Primary and secondary outcomes and statistical analyses were determined a priori.
Inclusion criteria included all patients entered into the block service registry. Patients were excluded for the following reasons: patients who did not receive a regional anaesthesia procedure (the Regional Anaesthesia Service also provides a vascular access service); patients who did not go to the PACU (e.g. patients who were cared for in the intensive care unit or emergency department and thus did not have PACU data recorded); patients who received multiple regional anaesthesia procedures for a single surgery where the primary proceduralist changed between a consultant anaesthetist and supervised trainee; postoperative or ‘rescue’ regional anaesthesia procedures; procedures where the timing of the block was not clearly documented; and patients where it was unclear who performed the procedure. Patients who received multiple regional anaesthesia procedures for a single surgical operation were considered only once with regard to outcome data.
This was a sample of convenience. The dedicated Regional Anaesthesia Service point-of-care registry was established in 2015, and the sample size at the time of study design was based on data availability. As no estimates of the proportion of consultant or trainee procedures resulting in an NRS > 5 at any time in PACU (primary outcome) were available at the time of study design, we chose a conservative proportion of 0.5 for consultant procedures with an NRS > 5. To have >90% power to detect a clinically significant difference in the proportion of 0.1, based on a two-sided test of proportions, a type I error of 0.05 and an estimated ratio of procedures performed by trainees compared to consultants of 2.5:1, a minimum sample size of 1271 was required.
Data were summarised using number (percent), mean (standard deviation) or median (interquartile range) as appropriate. Chi-square or Fisher’s exact test (for small expected counts) were used to assess associations of categorical variables with the principal proceduralist. Associations between non-normally distributed continuous variables and the principal proceduralist were assessed using a Mann–Whitney U test, whilst a Student’s t-test was implemented for normally distributed continuous variables. Statistical significance was predefined at α < 0.05 (two-sided). STATA v15 was used for all statistical analyses (StataCorp LLC, College Station, TX, USA).
Results
During the study period (17 February 2015 to 1 August 2018), the regional anaesthesia service performed procedures on 2163 patients. After 349 patients were excluded, 1814 patients remained. Reasons for exclusion are detailed in Figure 1. Of the 1814 patients analysed, the primary proceduralist was a consultant for 514 (28.3%) patients and a trainee for 1300 (71.7%) patients.
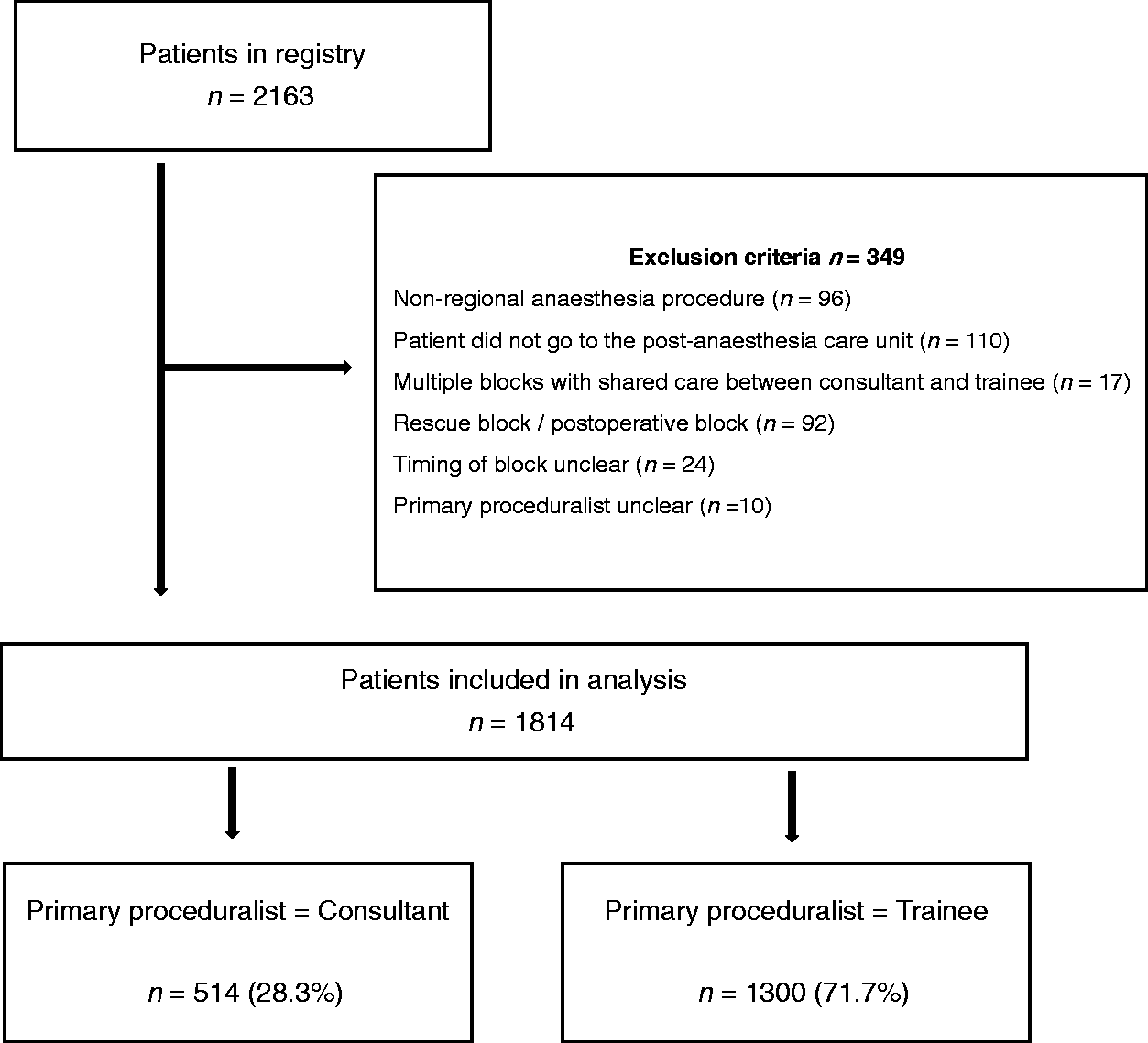
Study flow diagram.
Trainees were present for 1646 (90.7%) patients, and information regarding the experience of a trainee was available in 1571 cases. A total of 1274 trainees were in advanced anaesthesia training, and 297 trainees were either basic anaesthesia trainees or in another group (e.g. intensive care or emergency medicine trainees). Of the 1300 patients with a trainee as the primary proceduralist, there was either level 1 or 2 consultant supervision in 1230 (94.6%) and level 3 supervision in 41 (3.2%). The level of supervision was not documented in 29 (2.2%). No cases had level 4 supervision, as all cases were performed with on-site consultant supervision. Although the culture of our service is that level 1 supervision is routine, our data did not differentiate between level 1 and 2 supervisions.
The characteristics of the patients and procedures are shown in Table 1. Consultants had a higher rate of performing blocks on patients with a body mass index (BMI) >30 kg/m2 (43.2% versus 34.8%; P < 0.001) and a higher American Society of Anesthesiologists Physical Status Classification (ASA PS; P = 0.006). Consultants also had a higher rate of nerve blocks performed under general anaesthesia (14.6% versus 10.0%; P = 0.010), paravertebral/neuraxial blocks (12.6% versus 8.8%; P < 0.001) and blocks with perineural catheter placement (33.1% versus 19.9%; P < 0.001). Consultants were less likely to be the primary proceduralist if the trainee was an advanced trainee (62.1% versus 86.0%; P < 0.001).
Patient demographics and procedure characteristics of 1814 patients receiving regional anaesthesia procedures, stratified by primary proceduralist.
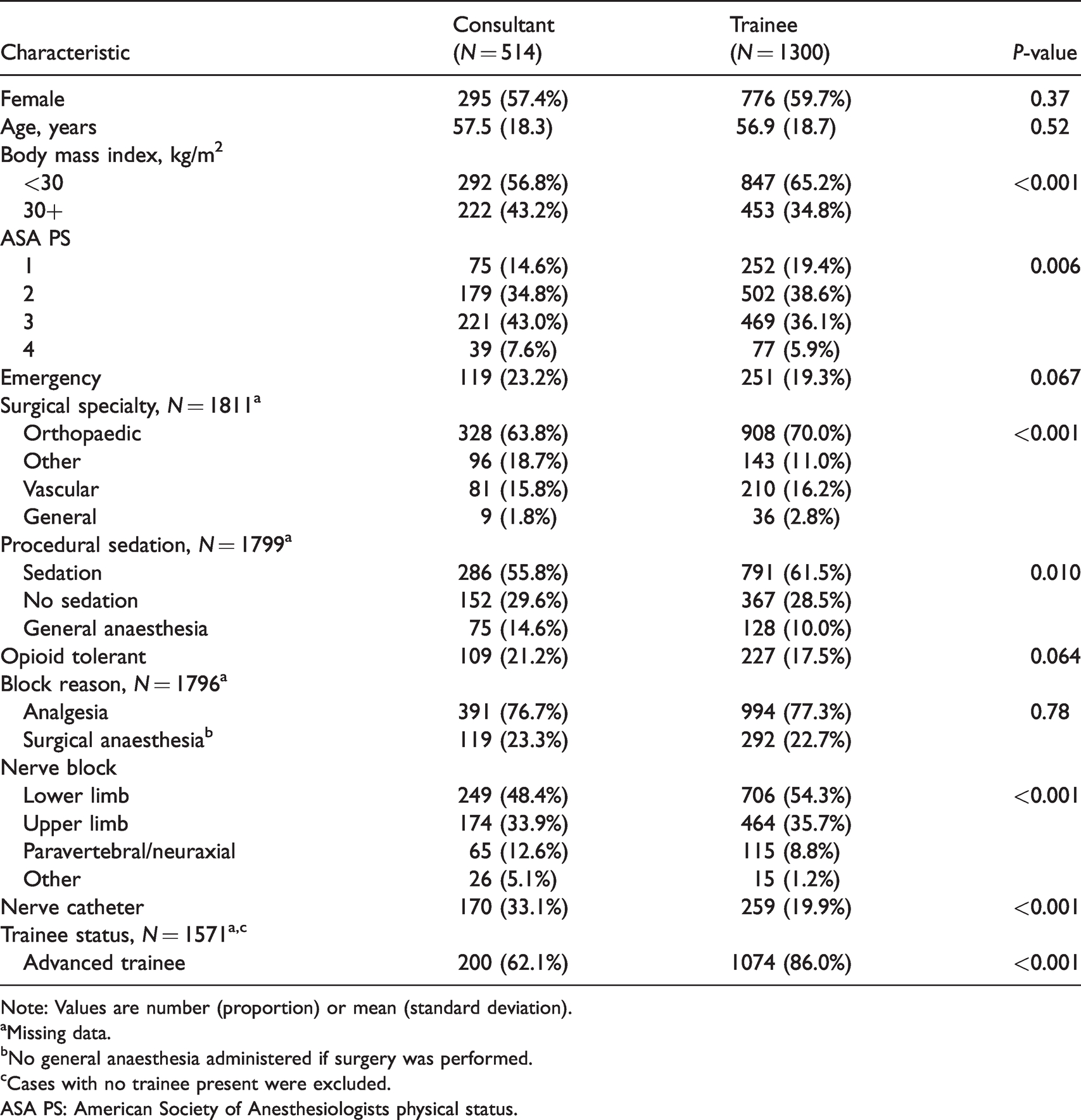
Note: Values are number (proportion) or mean (standard deviation).
aMissing data.
bNo general anaesthesia administered if surgery was performed.
cCases with no trainee present were excluded.
ASA PS: American Society of Anesthesiologists physical status.
Regarding the primary outcome of inadequate analgesia (NRS > 5 at any time in PACU), there was no statistically significant difference when consultants and trainees were compared (24.9% and 24.5%, respectively; P = 0.84). Similarly, there were no statistically significant differences between consultants and trainees when secondary outcomes were analysed (Table 2).
Primary and secondary outcomes (pain and systemic opioid requirement in the post-anaesthesia care unit) of 1814 patients receiving regional anaesthesia procedures, stratified by primary proceduralist.
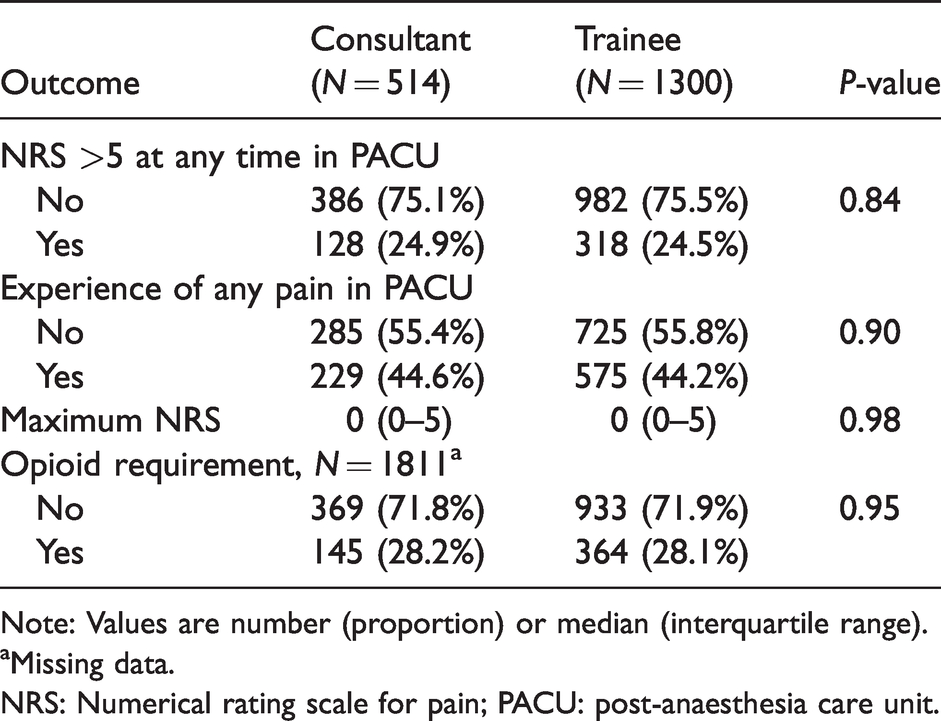
Note: Values are number (proportion) or median (interquartile range).
aMissing data.
NRS: Numerical rating scale for pain; PACU: post-anaesthesia care unit.
Discussion
There was no statistical difference in the rate of inadequate analgesia between consultant-performed procedures and supervised trainee procedures. This suggests that consultants at our institution, as a group, undertook appropriate decision-making regarding the case selection and supervision of trainees.
While there is extensive literature comparing surgical trainees and consultants, we believe this to be the first study to compare the clinical performance of supervised trainees and consultant anaesthetists in the field of anaesthesia directly. Consistent with our findings, both meta-analyses11,13,15 and single-centre studies7,8,12,14 evaluating a range of operations have demonstrated no statistical difference when consultant surgeon and supervised trainee outcomes were compared. Conflicting evidence was provided in an analysis of laparoscopic anti-reflux surgery which suggested that consultants performed better than trainees. 9 A meta-analysis of patients undergoing colorectal resection 10 found surgical trainees performed better than consultants—a finding the authors attributed to case selection.
Interestingly, a number of studies showed that surgical trainees, despite having longer operating times, had no worse postoperative outcomes than consultants, implying that supervision may impede efficiency but not safety.10,11,14,15 It has been suggested that effective supervision may improve patient outcomes due to greater attention to detail compared to independent expert practice.10,20 Unfortunately, our data did not measure the time taken to perform regional anaesthesia. However, a benefit of a block team model of care is that parallel processing means the time to perform a block is less relevant to theatre efficiency.
Clinical supervision at teaching hospitals can benefit both trainees and patients. Trainees gain experience and confidence from improved performance, 6 while patients may experience better outcomes. 21 Our results have demonstrated that within a block team model of care, supervised trainees can perform the practical aspects of regional anaesthesia without compromising patient outcomes. Supervision involves an assessment of trainee proficiency, matching that proficiency to the predicted difficulty of the procedure and provision of the right amount of supervision. If this occurs, the trainee gains experience without decreasing the effectiveness or safety of the procedure.
Providing the right amount of supervision is challenging because assessing trainee proficiency is not straightforward. Although tools designed to assess regional anaesthesia skills have been shown to be reliable and feasible, 22 there are a wide variety of tools available 23 without a clear gold standard. Indeed, a gold standard tool would require trainees to perform procedures on actual patients.24,25 Variability in the steepness of ultrasound learning curves26,27 makes predicting trainee proficiency prior to performing a procedure difficult. In our study, consultants were less likely to assume the role of primary proceduralist if the trainee was an advanced trainee, suggesting consultants allow experienced trainees more independence.
Predicting which procedures are likely to be troublesome is also problematic. A small but statistically significant finding in our study was that consultants were more likely to be the primary proceduralist for blocks performed on patients with a higher BMI and ASA PS. The evidence to support the use of patient characteristics to predict failed regional anaesthesia is conflicting.28–30 However, the importance of achieving success in such patients may influence decisions regarding the primary proceduralist. In our study, consultants were more likely to be the primary proceduralist for blocks performed under general anaesthesia (where time pressure, a surgical audience and the inability of the patient to report paraesthesiae add to the level of difficulty) and for patients requiring a peripheral nerve catheter (technically more challenging than a single-shot block).
A strength of our study is that the service is in-hours with a rostered consultant and registrar. Therefore, decisions about assigning the role of primary proceduralist are less likely to be due to consultant availability as might occur afterhours.
The non-randomised retrospective nature of this study is a limitation. However, assessing this study question in a randomised fashion is problematic. By its nature, effective clinical supervision is not random but tailored to the situation. Therefore, one might expect differences in baseline characteristics, as we found in our study. Prospectively allocating patients to trainees when the clinical scenario suggests a procedure should be consultant-led would be ethically questionable. Another limitation of this study is that although it assessed whether supervision benefited patients, it did not assess the quality of trainee learning. These results may reflect over-supervision of trainees, which is an under-appreciated phenomenon. 31 Our study is limited in that it is unable to provide granular detail about the level of direct supervision provided. A further limitation is that sensory block, though routinely assessed as part of clinical care, is not recorded in our registry. Though this would be useful additional information, it represents a surrogate marker; the primary goal of regional anaesthesia is to provide pain relief. Patients were not blinded to the seniority of the doctor performing the procedure and may have been aware that teaching was occurring. This may have introduced a bias in favour of consultants. Finally, our study does not identify how effective clinical supervision was achieved. The team model of a dedicated service may in itself improve outcomes, 17 particularly when part of a well-structured training programme. 11
Clinicians at teaching hospitals face the daily dilemma of how much independence to give trainees. We have demonstrated that trainee-performed regional anaesthesia procedures did not compromise patient pain relief when undertaken within a supervised (levels 1–3) block team model of care in our institution. Further research comparing trainee and consultant performance in the field of anaesthesia is needed, with a focus on patient outcomes and levels of supervision.
Footnotes
Author contributions
Acknowledgements
The authors wish to thank Dr Katherine Hames for assistance with data acquisition.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.