
Abstract
This paper reviews the natural and treated history of hepatitis C virus infection, the interactions between current therapies and anaesthesia medications, and the implications of occupational exposure and infection to anaesthetists in light of significant changes in treatment. In the past decade, the introduction of new direct acting antiviral medications has seen high cure rates with a sustained viral response across all virus genotypes. These medications are well tolerated with minimal side-effects. Should a patient on these medications require anaesthesia, there are few clinically significant interactions with commonly used anaesthesia medications, and minimal perioperative investigations are required, although delaying elective surgery until after the completion of treatment regimens should be considered to maximise treatment success. As anaesthetists may practise exposure-prone procedures, regular screening for hepatitis C virus infection remains recommended to enable both patient protection and treatment of the anaesthetist prior to the development of any long-term complications of hepatitis C virus infection. Similarly, early diagnosis and treatment of occupationally acquired hepatitis C virus infection after body fluid exposure is associated with high cure rates with minimal risk of long-term liver damage. Although hepatitis C virus infection remains a significant public health issue in Australia and New Zealand, improvements in outcomes as a result of new treatment regimens have allowed the World Health Organization to target the elimination of hepatitis C virus infection as a public health threat by 2030, and public health strategies are being implemented to achieve this goal.
Keywords
Introduction
Hepatitis C is a major global public health concern caused by infection with the hepatitis C virus (HCV). Up to 80% of individuals develop chronic infection, in which persistent viraemia is associated with chronic liver disease and liver malignancies. 1 Management of HCV infection in the past decade has evolved from interferon-based therapies with low uptake of treatments, low cure rates and significant side-effects to modern direct-acting antiviral medications (DAAs) which achieve cure rates of 94%–99% with minimal side-effects regardless of virus genotype. 2 Although the implementation of these therapies is relatively recent, there is already evidence of increased survival in patients who have undergone successful DAA treatment. 3
Despite significant changes in treatments and outcomes, in conducting searches of medical and scientific literature databases we have been unable to find any general reviews of HCV and anaesthesia published since 2000, noting that the last review regarding occupational hazards of HCV for anaesthetists occurred in 2004. Although there has been little change in the diagnosis and understanding of the pathogenesis of HCV infection, this review is warranted due to the development of well tolerated and highly effective treatment regimens. These new therapies may influence the choice of anaesthesia and timing of surgery, as well as treatment of occupationally acquired infection. In this review we therefore aim to review the natural history of treated and untreated HCV infection, guidelines with respect to best practices relating to anaesthesia for patients undergoing HCV treatment, the management of the HCV-positive anaesthetist, and the management of needlestick or body fluid exposure from an HCV-positive patient.
Although this paper primarily discusses the management of HCV in the Australian and New Zealand healthcare settings, similar treatment regimens are recommended worldwide. 4
Methods
Using the search terms ‘hepatitis C’, ‘anaesthesia’ and ‘review’, the search engines PubMed and Google Scholar were explored to find articles published since 2010, at which time DAAs were being licensed for introduction into clinical practice. These searches failed to produce any results. Again using PubMed and Google Scholar, searches were then conducted for review articles regarding HCV treatment, and internet searches for treatment and infection control guidelines related to HCV infection, using the search terms ‘hepatitis C treatment’, ‘infection control’ and ‘anaesthesia’. With respect to hepatitis C treatment, using the World Health Organization (WHO) guidelines as a basis for comparison, national guidelines for Australia, New Zealand, the United States, Canada and South East Asia were assessed to ensure that these guidelines were consistent with WHO guidelines, and that practice was uniform. With respect to the management of potential occupational HCV exposure and occupational ramifications, national and international guidelines were found through the Google internet search engine. In addition, an internet search using the Google internet search engine was conducted with the search term ‘hepatitis C treatment drug interactions’ to locate online resources for hepatitis C treatment drug interactions. One of the identified resources required input of selected medications to determine interactions. Using this website, drug interactions were determined by selecting all currently used hepatitis C treatment medications, and by selecting co-medications by class. The classes selected were anaesthetic and muscle relaxants, analgesics, antihistamines and gastrointestinal. Within each class, the list of medications was reviewed to identify medications currently used in anaesthesia practice. Using the interactions classification of this website, medications used in anaesthesia practice were classified as safe with no clinically significant drug interaction expected for all treatments, or safe with the exception of interactions with specific medications which were listed. These drug interactions were crosschecked with the general medical online point-of-care medical resource UptoDate. 5
HCV infection
This form of hepatitis was first recognised in 1975 with the discovery of transfusion-related hepatitis not associated with hepatitis A or hepatitis B (non-A, non-B hepatitis) and became defined in 1989 with the discovery of HCV and the development of diagnostic tests. 6 There are seven major genotypes of HCV (although one genotype is present in only a small number of individuals) and 67 subtypes which occur in distinct geographical regions. The genotype most prevalent in both Australia and New Zealand is genotype 1, which may be associated with a higher risk of developing severe liver disease and hepatocellular carcinoma. 7 Unlike the response to previous antiviral therapies in which different genotypes had different cure rates, DAAs achieve high cure rates for all genotypes.
HCV has an incubation period of 14–182 days with an average range of 14–84 days. Transmission is predominantly via exposure to the blood of infected persons. This occurs primarily through the sharing of contaminated needles; however, transmission within healthcare settings can be from blood product transfusions or where insufficient sterilisation of equipment has occurred. 1 , 8 Importantly, there has been no reported HCV infection attributable to blood transfusion in Australia in the years 2009–2018. 9 Sexual transmission is an emerging risk factor, while vertical transmission can occur in 6% of infected mothers. 1 After an acute infection, up to 45% of young healthy people have been found to be able to mount a sufficient immune response to clear the virus spontaneously. 10
Diagnosis is made by the detection of HCV antibodies. Seroconversion occurs 28–70 days after infection. 11 If infection is suspected before seroconversion, HCV infection can be diagnosed by the detection of HCV ribonucleic acid (RNA), which may be detected as early as 14–21 days after infection. 11 Once positive serology is detected, RNA testing is performed to confirm current infection, determine genotype and establish viral load.
Chronic HCV was traditionally defined as having detectable HCV RNA six months after diagnosis; however, this definition is becoming increasingly irrelevant as new treatments have seen the initiation of treatment prior to this six-month period. HCV antibodies persist for life, even after clearance of RNA (either spontaneously or through treatment).
Medicare-eligible Australians started receiving subsidised DAAs from March 2016, with over 85,000 people having accessed DAA therapy by the end of 2019. 12 Australia’s National Hepatitis C Strategy 2018–2022 is in line with global targets set by the WHO to eliminate HCV as a public health threat by 2030. 13 Decreasing incidence rates of HCV infections from the Australian Collaboration for Coordinated Enhanced Sentinel Surveillance of sexually transmitted infections and blood-borne viruses (BBVs) indicate progress towards achieving the goal of Australian HCV elimination. 14 The New Zealand National Hepatitis C Action Plan remains under development. 15
As HCV may be asymptomatic, it is difficult to estimate the exact prevalence of HCV in the population. At the end of 2017, there were over 180,000 people in Australia living with chronic HCV infection and approximately 50,000 people in New Zealand. 14 , 16 In Australia it is estimated that 80% of cases of HCV infection are diagnosed, with an estimate of approximately 40,000 undiagnosed cases, and the New Zealand Ministry of Health estimates that in excess of 20,000 people may be undiagnosed. 14 , 15 This cohort of undiagnosed patients is across all known recognised high-risk groups for infection, and strategies to increase diagnosis and treatment are required to make elimination possible.
Iatrogenic HCV infections are rare but there have been cases of medical personnel infecting patients, including anaesthesia providers transmitting HCV to patients. 17
Current treatments for HCV
Antiviral agents used for HCV treatment in Australia and New Zealand are listed in Table 1. The initial therapy regimen for HCV in Australia and New Zealand is an eight–12-week course of a combination of DAAs. Several different combined treatments exist, with the treatment being individualised according to the genotype, the presence of cirrhosis and/or liver decompensation, previous treatment history, potential for drug–drug interactions and comorbidities. 18 The most common genotypes in Australia and New Zealand are genotype 1 (approximately 50%) and genotype 3 (approximately 40%). 19 In Australia the first-line pan-genotypic DAA combinations for treatment-naive patients who have compensated liver disease are sofosbuvir with velpatasvir for 12 weeks or glecaprevir with pibrentasvir for eight–12 weeks. 18 Those who do not respond to these regimens require the combination of sofosbuvir with velpatasvir and voxilaprevir. 18 In New Zealand glecaprevir with pibrentasvir is prescribed, with the combination of ledipasvir with sofosbuvir reserved for patients with severe liver disease. 20 Ribavirin, which prior to the development of DAAs was used in the treatment of HCV, is still prescribed as an additional treatment in a subset of patients with decompensated cirrhosis.
In patients without significant comorbidities, HCV treatment may be initiated and managed in the primary care setting. Patients may therefore not have a specialist hepatologist overseeing their management, which may have implications for management of the patient on DAAs presenting for surgery, which is discussed further below. Contraindications to managing HCV treatment in the primary care setting include genotypes 4, 5 and 6, the presence of cirrhosis, co-existent hepatitis B virus or HIV infections, renal impairment, complex comorbidities and medication requirements, and previous failure of DAA treatment. 21
Patients who fail to clear the virus or have decompensated liver disease may require treatment regimens of up to 24 weeks’ duration. 18 These patients would normally be managed in specialist centres.
The DAAs target multiple steps in the HCV replication life cycle. The four classes of DAAs are non-structural (NS) 3/4A protease inhibitors, NS5B nucleoside polymerase inhibitors, NS5B non-nucleoside polymerase inhibitors and NS5A inhibitors. 22 Their targets are the HCV-encoded proteins, essential to viral replication, processing and assembly.
The protease inhibitors work by preventing the viral proteases from cleaving the translated polyproteins. Polymerase inhibitors prevent further replication of the viral genome either by causing conformational change of the polymerase enzyme (non-nucleotide inhibitors) or by prematurely terminating the formation of new viral RNA (nucleotide inhibitors). 23 Finally, the NS5A inhibitors inhibit the NS5A protein, which is a non-structural protein thought to be crucial in regulating viral replication.
Current antiviral regimens are exceptionally well tolerated, with the most common side-effects being headache, fatigue, nausea and diarrhoea. 18 Baseline laboratory monitoring including a full blood picture, liver and renal function tests, electrolytes and HCV polymerase chain reaction testing should be established on initiation of treatment. 18 In contrast to interferon-based regimens, the DAAs require less on-treatment surveillance. The follow-up and monitoring during treatment should be on an individualised basis with specific populations requiring more intensive monitoring. 18
DAAs are now associated with average cure rates in excess of 90%. 24 Treatment is determined to be successful when there is undetectable plasma HCV RNA at least 12 weeks after the end of a treatment course, defined as a sustained virological response (SVR). 18 Successful viral eradication is considered a cure, and those who do not have cirrhosis and normal liver function tests after SVR can be managed as if they never had HCV. 18 After successful treatment of HCV, reinfection from a new source is possible with both the initially treated virus genotype and other genotypes.
Anaesthesia implications of HCV treatment
Absolute compliance with treatment regimens increases success rates. Suboptimal adherence to treatment regimens, such as mistimed and missed dosages, was associated with the development of drug resistance and failure of therapy in now superseded therapies. Although not proven with DAAs, this remains a potential adverse outcome of interrupting treatment. Given that the majority of treatment regimens are for eight–12 weeks, in most clinical situations it would be feasible to delay elective surgery until after treatment is completed to enable optimal success from treatment. If emergency surgery is required, whenever possible DAAs should be continued throughout the perioperative period. DAA regimens are not associated with renal complications, but HCV patients are at higher risk of having renal disease. Renal function should therefore be assessed preoperatively. Preoperative liver function should also be assessed.
There was one frequently referenced online hepatitis C drug interaction website. A review of this website demonstrated few clinically significant interactions with commonly administered anaesthesia drugs. 25 This website resource also includes DAAs that are not prescribed for treatment of HCV in Australia and New Zealand. The resource is not exhaustive and does not list all anaesthetic medications that are commonly used in Australia and New Zealand. Cross-referencing of these interactions was undertaken using UpToDate. 25 On the basis of reviewing these resources, Table 2 provides a list of perioperative medications for which no clinically significant drug interactions have been reported in use with ribavirin and all the DAAs that are currently being prescribed for HCV treatment in Australia and New Zealand. It also lists those perioperative medications in which there is a potential for drug interactions. Although not all commonly used anaesthesia medications have been studied and listed, Table 2 provides a significant number of medications and alternatives.
Antiviral agents used for Hepatitis C virus treatment in Australia and New Zealand.
Interactions between direct-acting antivirals used in Australia and New Zealand and commonly used perioperative medications.
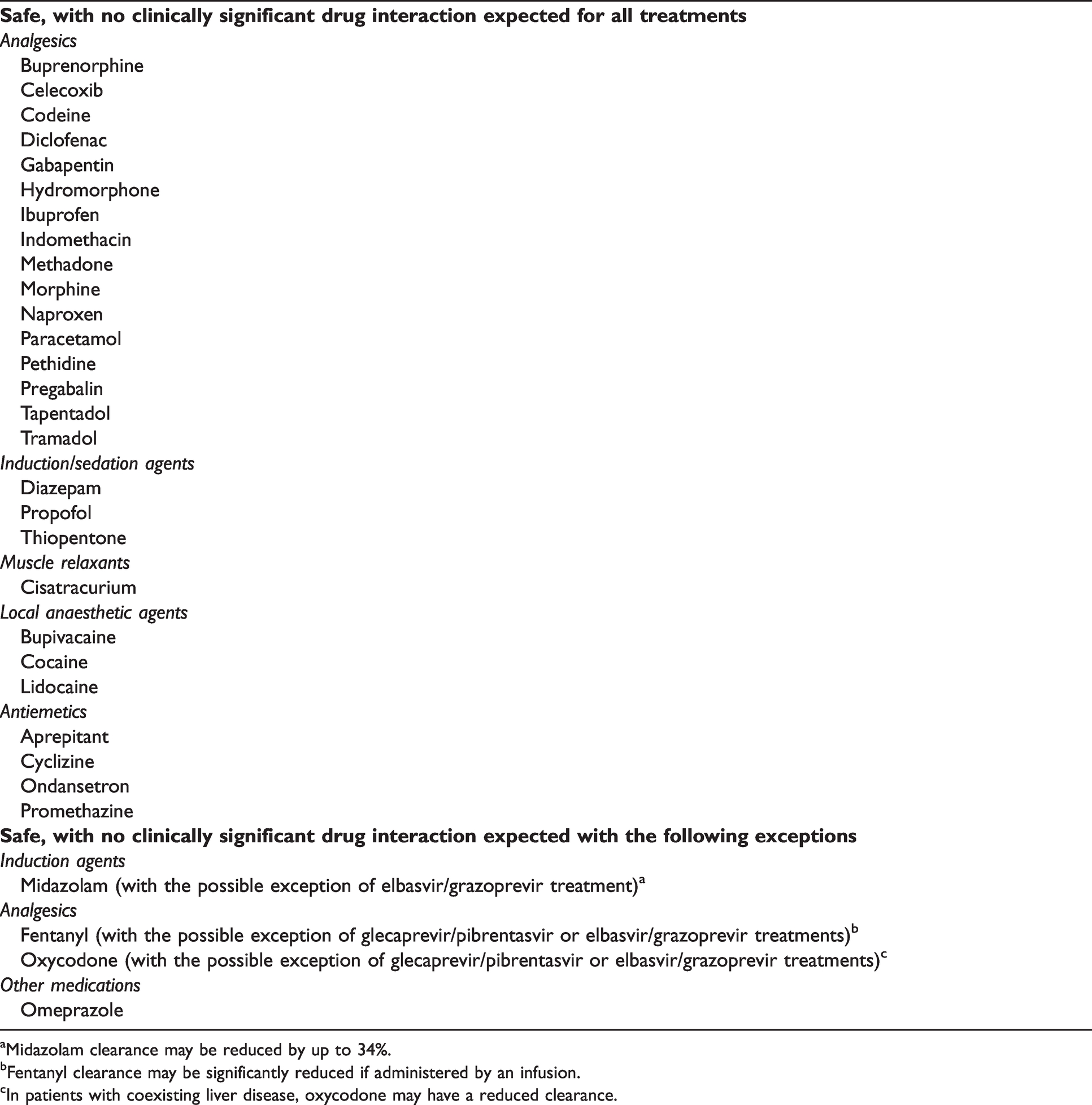
aMidazolam clearance may be reduced by up to 34%.
bFentanyl clearance may be significantly reduced if administered by an infusion.
cIn patients with coexisting liver disease, oxycodone may have a reduced clearance.
There are no published reports of interactions between DAAs and sevoflurane or desflurane. Given the low incidence of post-anaesthetic liver dysfunction with these agents and the minimal metabolism that occurs, it is unlikely that these agents would have any significant interactions with DAAs.
Occupational exposure to HCV
Occupational exposure to BBVs remains a feared consequence of working in healthcare. Exposure to HCV may be by sharps injury or needlestick (‘sharps injuries’), or by mucous membrane or cutaneous (non-intact skin) exposure.
After analysis in the 1990s, the average incidence of seroconversion after sharps injuries from an HCV-positive source was quoted as 1.8% (range 0%–7%). 26 However, the incidence may be much lower as a recent data analysis suggests a seroconversion rate of 0.2% for percutaneous injuries and 0% for mucocutaneous exposure. 27
Institutional protocols should be followed with assessment of the HCV status of both the source (if possible) and the recipient of the exposure. The source status may be determined by HCV antibody and/or RNA, depending on institutional protocol. However, some recent guidelines recommend HCV RNA testing for all initial source testing as the preferred option. 28 If the source is HCV RNA negative, usually no further follow-up is required. If the source is HCV RNA positive or unknown, the exposed healthcare worker (HCW) may be considered for HCV RNA testing three to six weeks after the exposure, and then if HCV RNA is positive referred for follow-up and early treatment. If the HCW is HCV antibody positive at initial testing, HCV RNA testing should be performed to determine if the HCW has previously cleared HCV, or if they are currently infected. The Royal College of Pathologists of Australasia includes consideration of HCW HCV RNA testing in its guidelines for appropriate tests after needlestick injury if the source of the exposure is HCV RNA positive. 29 Completion of HCW follow-up involves further HCV antibody testing at four to six months in all situations in which the source was positive to confirm absence of infection. Common practice also involves further HCV antibody testing up to six months after exposure from source negative patients to detect infection in the rare situation in which the donor may have been HCV antibody and RNA negative during the initial phase of infection.
HCV post-exposure prophylaxis (PEP) is not recommended after HCV exposure. DAAs have been considered for PEP. 27 , 30 However, their use is not recommended on the basis that first, the risk of transmission is very low; second, spontaneous clearance may occur; third, should seroconversion occur the rate of cure is extremely high; fourth, there is unlikely to be a mechanism for PEP; and finally, there have been no studies demonstrating a benefit from PEP. 31 , 32
The anaesthetist with HCV infection
Between 1998 and 2012 there were 376 documented cases worldwide of HCV transmission from HCV-infected anaesthetic providers to patients. 33 Transmission occurred in both those complying with standard BBV infection control precautions, and in those HCWs known to be using illicit drugs and patients’ medications for their own use. 33
In both Australia and New Zealand, practice guidelines apply to all HCWs who have evidence of HCV or other BBV disease. 33 , 34 The main determinant factor as to whether a medical practitioner with active HCV infection may continue their practice is whether the practitioner undertakes non–exposure-prone procedures (non-EPPs) or exposure-prone procedures (EPPs).
The Communicable Diseases Network Australia provides definitions for non-EPPs and EPPs. 35 Non-EPP defined procedures are those in which the hands and fingers of the HCW are visible and outside of the body at all times, and procedures or internal examinations that do not involve possible injury to the HCW’s hands by sharp instruments and/or tissues provided routine infection prevention and control procedures are adhered to at all times. EPPs are those in which there is a risk of injury to the HCW resulting in exposure of the patient’s open tissues to the blood of the HCW. These procedures include those in which the HCW’s hands (whether gloved or not) may be in contact with sharp instruments, needle tips or sharp tissues (spicules of bone or teeth) inside a patient’s open body cavity, wound or confined anatomical space where the hands or fingertips may not be completely visible at all times.
Relevant to anaesthesia procedures, within these guidelines endotracheal intubation, bag-mask ventilation, insertion and maintenance of arterial or intravenous cannulae whether inserted centrally or peripherally, simple suturing, and insertion of intercostal catheters in non-trauma situations are listed as non-EPPs. Laryngeal mask airway (LMA) insertion and the insertion and maintenance of epidural and spinal anaesthesia lines are not considered within this classification; however the Society for Healthcare Epidemiology of America consider these to be procedures in which BBV transmission is theoretically possible but unlikely. 36
There is continued discussion as to whether the provision of anaesthesia is a non-EPP specialty. The Australian and New Zealand College of Anaesthetists does not define whether anaesthesia is an EPP or a non-EPP specialty. 37 There are situations in anaesthesia practice when insertion of gloved fingers into the mouth may occur and the fingertips are not always visible. Examples may include facilitating LMA or nasogastric tube placement. However, there are alternatives available to allow insertion without placing fingers in the mouth, and as such it is possible to practise anaesthesia as a non-EPP specialty. Within the practice of pain medicine, there are procedures such as implantation of stimulators and other devices in subcutaneous tissue planes where fingertips may not always be visible. It is therefore up to each individual practitioner to determine whether their own scope of practice contains EPPs.
The Medical Board of Australia in partnership with the Australian Health Practitioners Regulation Agency has recently revised its guidelines with respect to practitioners and students in relation to BBVs. 38 HCWs who perform EPPs must take reasonable steps to know their BBV status and should be tested for BBVs at least once every three years. The Medical Council of New Zealand guidelines suggest testing at an interval of between one and five years depending on the type of practice of the HCW. 34 Both these Australian and New Zealand guidelines state that HCWs must not perform EPPs while they are HCV RNA positive, but may be permitted to return to EPPs after successful treatment or following spontaneous clearance of HCV RNA.
Conclusion
Once diagnosed, HCV infection is now a readily curable disease, with a considerably reduced risk of developing the long-term complications associated with chronic infection. The current DAAs pose few clinically significant difficulties for anaesthesia practice. Increasing tolerance by patients and compliance with current HCV treatments suggests it is likely that the prevalence will decrease within the community. Should an anaesthetist sustain occupational exposure to HCV, the risk of long-term infection and its sequelae is minimal given the effectiveness of treatment. It is highly probable that an anaesthetist who becomes infected with HCV will be successfully treated and be able to return to full EPP practice.
While the anaesthesia-related challenges of the disease diminish, the challenges that HCV infection and its disease burden impose on the community remain. Despite the WHO target for elimination of the infection as a public health threat by the end of this decade, there remain significant obstacles to this being achieved. Even if there is a substantial reduction in the prevalence of the disease there may remain a substantial cohort of high-risk undiagnosed patients with a propensity to continue community transmission. With the increasing uptake and success of the novel treatments, hopefully more people with HCV will be diagnosed and access therapy. As such, an awareness of anaesthesia implications of HCV treatment remains important.
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.