
Abstract
Healthcare contributes to environmental harm. Trainee-led Research and Audit in Anaesthesia for Sustainable Healthcare (TRA2SH) is an Australasian network focused on sustainable anaesthesia practice. TRA2SH hypothesised that trainee-led audits alongside education presented on a scheduled national day, called Operation Clean Up, can improve engagement with sustainability initiatives. This paper aims to describe the first two years of Operation Clean Up in terms of goals, achievements and data collected so far. Environmental themes for Operation Clean Up were chosen based on available evidence (life cycle analyses and observational studies). The first Operation Clean Up (OCU 2020) focused on reducing the unnecessary use of single-use disposable absorbent pads (known as ‘blueys’ in Australia, ‘greenies’ in New Zealand). OCU 2021 included: refuse desflurane, reduce bluey use, reuse drug trays, and recycle paper and cardboard. TRA2SH provided an information pack to trainees who presented educational material to their department and fed back procurement figures to quantify each item. Descriptive statistics were used to analyse de-identified pooled data submitted to a centralised database.
Eight departments submitted data for OCU 2020 and six provided follow-up data. Bluey use was reduced from a median of 37 to 34 blueys per ten surgical encounters. Fifteen departments submitted pre-campaign data for OCU 2021 with follow-up data to be collected during OCU 2022. Baseline data showed a median bluey use of 31 per ten surgical encounters. Volatile-related emissions were calculated; desflurane’s proportion was 70% of these emissions yet was 11% of volatile procurement. Two participating departments removed desflurane from their formulary following OCU 2021. Operation Clean Up is a practical model for implementing sustainability initiatives using trainees as eco-leaders.
Keywords
Introduction
The impact of climate change on health and the impact of the healthcare system on the environment are increasingly recognised as critical issues for the future of humanity and our planet.1–3 The World Federation of Societies of Anaesthesiologists has published seven fundamental principles for delivering environmentally sustainable anaesthesia worldwide. 3 These include choice of medications and equipment; minimising waste and overuse of resources; and improving anaesthetists’ education, research, quality improvement and local healthcare leadership activities. 3
TRA2SH
Trainee-led Research and Audit in Anaesthesia for Sustainable Healthcare (TRA2SH) is a collaborative network created by trainees for trainees, aiming to stimulate positive culture change in sustainable practices in anaesthesia. TRA2SH recognises that anaesthetic trainees can raise awareness, educate, advocate and play a key role in eco-leadership in their departments. Implementing the existing environmental evidence base to current practice requires an implementation strategy to drive realistic, feasible, acceptable change that can be sustained over time. TRA2SH has been publicised by Australian and New Zealand College of Anaesthetists (ANZCA) publications, social media and regional trainee committees with 315 members at the time of submission. Initially trainees could join by emailing interest, and later via the TRA2SH website www.tra2sh.org. Members receive a quarterly newsletter and an invitation to join a closed communication platform (Discord) used as a support network to share information, brainstorm project ideas and troubleshoot issues. TRA2SH does not support or distribute political viewpoints and remains focused on delivering high-value patient care that is environmentally and economically sustainable.
Operation Clean Up
The goal of TRA2SH is to integrate evidence-based sustainable practices into mainstream anaesthesia. TRA2SH hypothesises that trainee-led audits of product usage, accompanied by feedback and education to departments, may improve compliance with sustainability initiatives. Operation Clean Up (OCU) is planned to be an annual event to promote awareness of achievable sustainability issues in the operating theatre. OCU utilises an implementation triad of trainee champions, inter-professional education, and audit feedback—factors that have been shown to influence practice and clinician compliance with evidence-based guidelines. 4
The first OCU, held in March 2020, focused on reducing bluey use. ‘Bluey’ is an Australian colloquial term for a single-use disposable absorbent pad (also known in other regions as pinkie, greenie, incopad, or chux pad). The primary purpose of blueys is to reduce dermatitis and pressure sores from prolonged fluid exposure. 5 They are made of a cotton absorbent layer, sandwiched between two plastic layers, 6 take in excess of 100 years to break down 7 and cannot be recycled. The trainees who volunteered for OCU were encouraged to identify areas where blueys are used for reasons other than their primary purpose and where they do not contribute to patient care (e.g. bluey tablecloths). TRA2SH encouraged locally acceptable solutions as departments’ practices vary considerably.
The second OCU, held on Earth Day 2021, expanded to include ‘refuse desflurane’, ‘reduce bluey use’, ‘reuse drug trays’, and ‘recycle paper and cardboard’. We used the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) framework, 8 to make OCU recommendations based on our confidence (very low, low, moderate, high) of how close the true effect is to the estimated effect based on the quality of evidence. To determine the environmental impact of a process or product, observational process-based life cycle analysis is the gold standard. 9 There is high confidence in the evidence regarding the environmental impact of desflurane and reusable drug trays, and moderate confidence in the evidence for recycling. To our knowledge, there are no studies outlining the environmental harm of disposable absorbent pads (blueys). There is high confidence, based on high quality life cycle analysis, that bluey components10–12 and disposable (versus reusable) incontinence pads 13 cause considerable environmental harm. We have thus moderate confidence that the unnecessary medical use of blueys is harmful to the environment. Reducing desflurane was chosen because it has a 100-year global warming potential (GWP100) 2540 times greater than carbon dioxide. 14 One 240 ml canister of desflurane will directly release 893 kg of carbon dioxide equivalents (CO2e) into the atmosphere, 15 whereas one 250 ml canister of sevoflurane releases 50 kg CO2e. 15 Reusable drug trays have half the environmental footprint of single-use plastic drug trays, even when energy was derived from coal. 16 General education regarding recycling was included as 60% of anaesthetic waste has the potential to be recycled 17 and trainees are well suited as educators and leaders in expanding recycling activities in theatres.
Methods
The TRA2SH steering committee selected items for OCU based on the hierarchy of environmental intervention (refuse, reduce, reuse, recycle), the life cycle evidence base that is available, and the item fulfilling ‘SMART’ (specific, measurable, achievable, realistic, time-bound) goals. The TRA2SH steering committee was responsible for creating an OCU resource pack. Trainee volunteers were recruited via the ANZCA e-newsletter, an email invitation to TRA2SH members, social media, word-of-mouth, and a sign-up page via www.tra2sh.org. Once a trainee volunteered to run OCU in their department, a link to the OCU-resource folder was emailed, containing educational material such as journal articles, posters that can be tailored to participants’ local departments and evidence-based presentations. The email included a welcome letter, which contained background information and instructions on how to host OCU. The steps included where to find a departmental mentor, to seek local approval to conduct a local audit and share data, to present information to the department, and to join or create a sustainability team. Contact details were saved on REDCap—a secure password-protected centralised electronic data capture tool hosted at the University of Melbourne. 18 Trainees were only contacted in relation to OCU and could opt out at any time. The trainee who ‘signed up’ remained the contact for their site but they could recruit other local staff to assist in their campaign. No human research was conducted so this project did not meet requirements for ethics committee review. 19 Individual hospital requirements for data governance were varied, so local data sharing approval was sought individually by each OCU participant.
Once a trainee gained permission to share data outside their institution, they submitted their local data via REDCap. 18 We collected procurement data on volatiles, blueys and drug trays as well as the number of surgical encounters in a year. Departments could participate in the entire bundle or focus on a particular item and complete the specific data form for the chosen item. Additional information on where vaporisers were kept and what drug trays were made of was also collected. Stand-alone endoscopy suites were excluded. Annual data were defined as 1 January to 31 December, and surgical encounter as a single patient encounter even if multiple procedures were performed. For each participating theatre suite, the number of blueys procured was paired with the number of surgical encounters. We reported median bluey use per ten surgical encounters from pooled paired data. The life cycle of volatiles 20 and local volatile use and cost for 2019 and 2020 were fed back to departments as part of the OCU ‘refuse desflurane’ campaign. Individual hospital data were pooled and analysed using descriptive statistics. Carbon dioxide equivalent emissions (CO2e in kg) were calculated from the formula (GWP100 × density ×volume)/1000. 15 Expressing CO2e (kg) as kilometres driven by a typical Australian car was calculated using the median grams of carbon emission equivalents per kilometre (CO2e g/km) for Australia’s 2020 top 20 selling cars 21 (158 g/km CO2e). Cost figures in New Zealand dollars were converted to Australian dollars. 22 No quantitative data were collected on recycling because recycling metrics are not available for all hospitals, and a recycling survey has been published elsewhere. 23
Results
OCU 2020
Nineteen trainees expressed interest in delivering TRA2SH’s first OCU in 2020. Eight Australian theatre suites (from five states/territories) provided pre-campaign bluey procurement data for 2019 and six provided follow-up data for 2020.
OCU 2021
Seventy-seven trainees from 35 departments across Australia, New Zealand and the UK expressed interest in volunteering for OCU 2021. Fifteen departments participated by submitting data. Twelve departments were from Australia, across five states and territories, and three from New Zealand. Twelve sets of data were collected for each individual item (blueys, desflurane or drug trays) but these were not from the same 12 hospitals. Of the 15 departments that submitted data in 2021, two had participated in OCU in 2020.
Blueys
The first eight participating departments cumulatively procured 437,050 blueys in 2019. Two departments were lost to follow-up. The six departments that provided post-campaign data showed a 10% decrease in theatre activity. In these six hospitals, the median number of blueys used per theatre was reduced from 5135 (interquartile range (IQR) 4590–6066) to 4077 (IQR 3821–4634) over the year. Median bluey purchasing was reduced from 37 (IQR 36–45) to 34 (IQR 30–37) blueys per ten surgical encounters (Table 1). Absolute bluey procurement was reduced in all but one hospital, which reported the same number of blueys ordered for both years. For the ‘reduce bluey use’ campaign in OCU 2021, 12 trainees submitted their theatre suite’s procurement and surgical encounter data. Follow-up data for 2021 is expected in 2022.
Disposable absorbent underpad (‘bluey’) procurement paired with number of theatres in operating suite and surgical encounters.
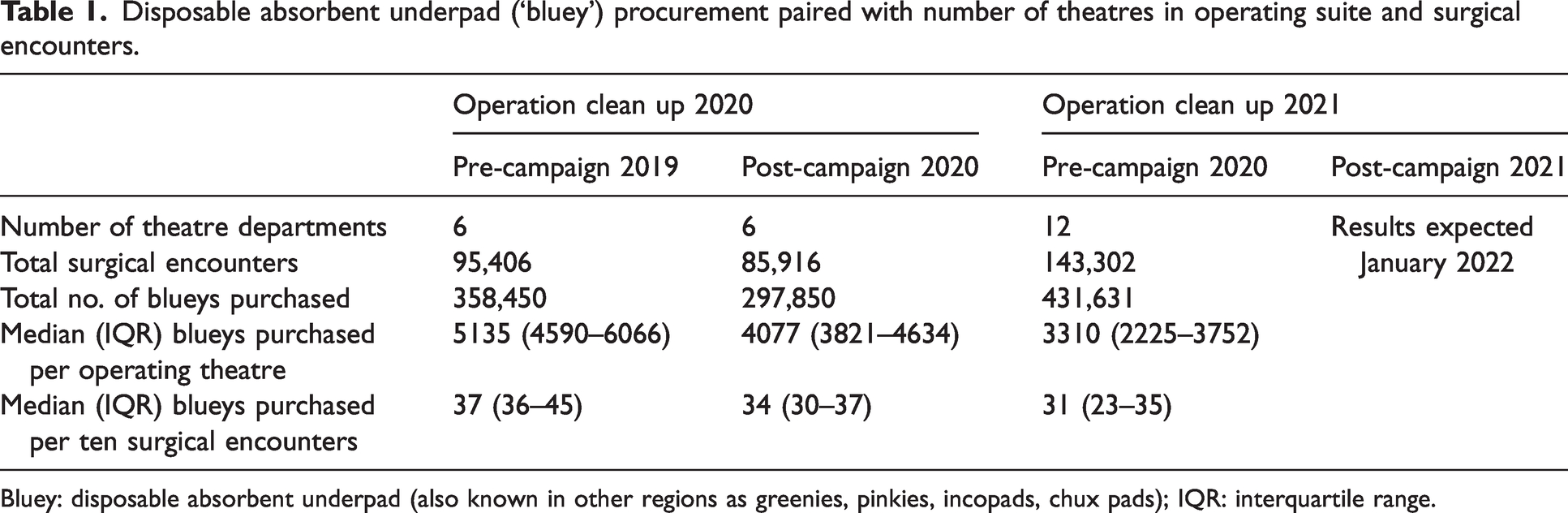
Bluey: disposable absorbent underpad (also known in other regions as greenies, pinkies, incopads, chux pads); IQR: interquartile range.
Desflurane
Pre-intervention volatile procurement data (sevoflurane, desflurane and isoflurane) were provided by 11 hospitals for 2019 and 12 hospitals for 2020. Isoflurane procurement was negligible and was thus excluded. In this sample, the reported annual surgical encounters in 2020 reduced by 5.4%, while desflurane procurement fell by 50% between 2019 and 2020 (see Table 2). Over this two-year period, desflurane represented only 11% of volatiles purchased by volume, yet produced 70% of calculated emissions directly released into the atmosphere at the point of care. The calculated emissions of desflurane were equivalent to 1.77 million kgCO2e or 11.2 million kilometres driven by a standard Australian car (calculated as 158 g/km CO2e). 21
Volume of desflurane and sevoflurane procured with associated calculated emissions.
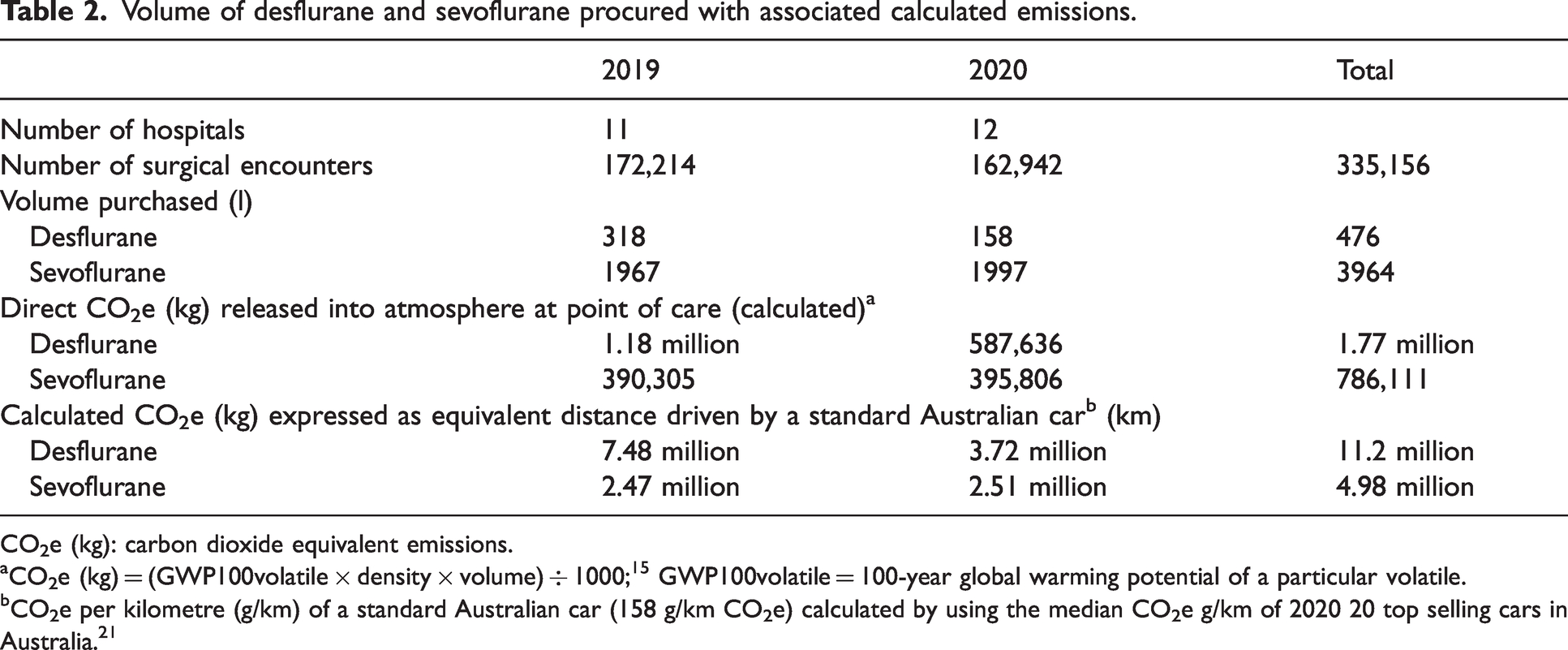
CO2e (kg): carbon dioxide equivalent emissions.
aCO2e (kg) = (GWP100volatile × density × volume) ÷ 1000; 15 GWP100volatile = 100-year global warming potential of a particular volatile.
bCO2e per kilometre (g/km) of a standard Australian car (158 g/km CO2e) calculated by using the median CO2e g/km of 2020 20 top selling cars in Australia. 21
From the participating hospitals, ten submitted cost data for 2019 and 11 for 2020. The median cost of one 240 ml canister of desflurane was nearly double the median cost of one 250 ml canister of sevoflurane in 2019 and up to four times more in 2020. Table 3 shows the cost comparison of sevoflurane and desflurane per minimum alveolar concentration (MAC) hour at different hypothetical flow rates for this sample. Delivering sevoflurane at high fresh gas flow (FGF) 6 l/min was financially comparable to delivering desflurane at low FGF (1 l/min). Three hospitals reported that desflurane vaporisers were kept on the machine, four reported that desflurane was kept in the operating theatre or anaesthetic room but not on the machine. The remaining five did not keep desflurane in their operating theatre or anaesthetic room but it was available in the department.
The median cost of volatiles in our sample reported as the median cost per hour of volatile administration using hypothetical fresh gas flows.
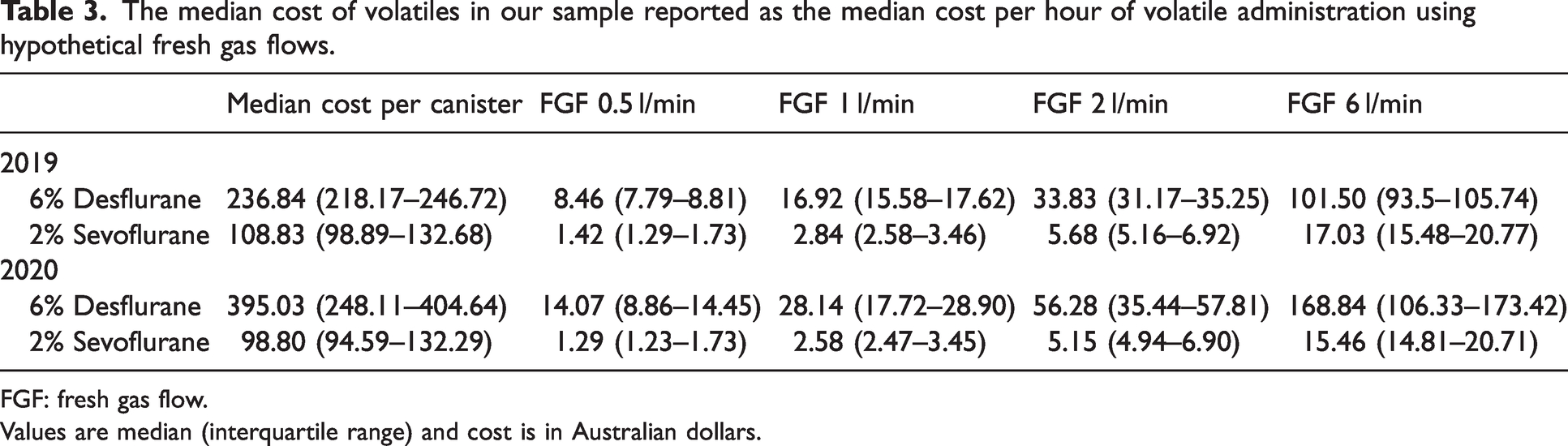
FGF: fresh gas flow.
Values are median (interquartile range) and cost is in Australian dollars.
Drug trays
Twelve hospitals submitted data on the types of commonly used drug trays. Four used a reusable plastic drug tray that was washed and/or sterilised, and the remaining eight used single-use trays that were either oil-based plastics, cardboard, bamboo, or sugar cane. One of these hospitals also has single-use aluminium drug trays available. Two of the single-use plastic trays were sterile, contained gauze and absorbent paper, and were packaged. None contained intravenous cannulation equipment.
Discussion
OCU is a novel model for implementing sustainability, which has demonstrated that trainees can be engaged in Australasian public hospitals and act as ‘champions’ to provide evidence-based education and feedback through audit. McKimm and McLean, in their description of eco-leadership, noted that ‘changing behaviour, organisations and cultures is challenging and needs a long-range perspective, requiring individuals to become active and proactive agents for environmental change and sustainability’. 24 Whether OCU was successful in quantitative terms requires a long-range view, ongoing engagement and continued measurement, given our small sample size. Success was seen in achieving the goals of TRA2SH of greater engagement; 77 trainees expressed interest in OCU 2021 compared to 19 in OCU 2020. Junior doctors from 21 public Australasian operating suites delivered a locally tailored educational campaign accompanied by audit and feedback, and TRA2SH hosted a successful online one-day conference in November 2021 providing trainees with the opportunity to present their local OCU projects. TRA2SH has continued to grow through publicity related to OCU, with 315 members on the mailing list of TRA2SH and 668 Twitter followers at the time of submission. Encouraging and supporting ‘eco-leaders’ throughout anaesthetic departments is a realistic and practical approach to promote the uptake of evidence-based sustainable practice, and may recruit other individuals to be active locally too. Eco-leaders can lead by example and engage others through conversation. The eco-leaders of TRA2SH may be junior, but their campaign may lead to greater engagement from influential decision-makers. A visible day of activity such as OCU may enhance the rate and scope of junior eco-leaders’ influence, but this project did not measure to what extent.
Trainees rotating to different departments and hospitals have both advantages and disadvantages. Trainees can continue their environmental leadership in each department and share information between hospitals. Disadvantages include difficulty obtaining follow-up data once they have moved on, and that changes may not be maintained over time. This highlights the importance of trainees finding senior mentors and forming multidisciplinary sustainability theatre groups with permanent staff.
The ‘reduce bluey’ campaign focused on the unnecessary uses of blueys (e.g. as tablecloths). Even when surgical encounters were taken into account, there was a wide range of bluey use between individual theatre suites. Pooled data showed a small reduction in bluey use. This may be due to chance, or may be due to a real reduction as a result of local education campaigns. Bluey use is likely to be cultural and may take time to change. The aim of TRA2SH is to stimulate a positive culture change in sustainability, which includes for clinicians to consider the environmental impact of items and to reduce the use of low value care. Instigating ways to reduce the enormous amount of operating theatre waste 25 can be overwhelming. Focusing on one visible item to act as a ‘sustainability totem’ may make environmental engagement more accessible and cultural change more probable. Blueys are specific, measurable and reducing their use without harming patients is achievable and realistic. OCU 2021 pre-campaign median bluey use per ten surgical encounters was less than post-campaign data for OCU 2020 (Table 1). We speculate that the ‘reduce bluey use’ campaign extended beyond the participating departments of OCU 2020, based on anecdotal reports and feedback. One hospital fed back that nursing staff on the wards, inspired by OCU 2020, started their own ‘reduce bluey use’ campaign. Beyond the OCU campaigns, TRA2SH continued to provide information about the sustainable use of blueys and their alternatives in the ANZCA bulletin, at an ANZCA sustainability workshop, at the ANZCA Annual Scientific Meeting, on the TRA2SH website, and on social media. We hypothesise that an annual event combined with sharing information, rotating trainees and word-of-mouth could propagate practice changes in non-participating institutions. While reducing the use of blueys will reduce their contribution to hospital waste, TRA2SH recognises that replacing blueys with reusable alternatives may alter the environmental footprint for the worse. Further research comparing the efficacy and environmental impact of reusable and disposable towels in preventing contact dermatitis and pressure sores is needed.
The desflurane data may reflect a ‘green bias’. Nine participating departments did not keep desflurane on the anaesthetic machine, which may account for some of the 50% fall in purchasing; however, it is likely that desflurane use was already declining. We believe that feedback on the cost and environmental impact of baseline desflurane use is compelling—two participating departments have removed desflurane from the pharmacy formulary following OCU 2021. We propose that continuing to use desflurane, even at minimal flows, is no longer justified as desflurane produces a disproportionate volume of direct emissions. Our data also show that the cost of desflurane is increasing. We will collect follow-up data in OCU 2022 and hope that this article’s pooled pre-campaign data will inspire public and private anaesthetic departments to remove desflurane vaporisers from the anaesthetic machine as a first step to reduce desflurane use (see https://www.tra2sh.org/refuse-desflurane). As an alternative, low flow sevoflurane is safe,26,27 and is associated with reduced emissions and cost. 28
Although one of the OCU campaign goals was to ‘reuse drug trays’, we recognise the significant challenges of implementing a new product in a clinical area and that this is generally beyond the expectations for trainees. However, OCU can create opportunities to discuss the merits of reusable equipment through a triple bottom line (patient, planet and purse) lens. Single-use plastic trays are double the financial and environmental cost (when they include sheet and gauze) compared to a reusable plastic tray. 16 We were also interested to learn more about the non-plastic single-use drug tray products being used in hospitals. Bamboo and sugar cane bagasse are products marketed to reduce plastic waste, but there is no direct evidence to quantify the carbon footprint of these trays. These items may be marketed as ‘biodegradable’ or ‘compostable’, but unless they are placed into composting waste streams, both products (along with cardboard) can produce methane from anaerobic decomposition in landfill. 29 ‘Bio-plastics’ may pose problems for plastic recycling if placed into recycling streams. 29 No life cycle analysis of aluminium drug trays is available. Single-use aluminium takeaway containers have a high carbon footprint, but are highly recyclable. 30 Any OCU success regarding drug trays may become evident beyond the timescale of an annual OCU cycle. Departments wishing to replace a plastic tray may choose a reusable option rather than a biodegradable product, as a result of trainee-led education. With hospitals moving towards a renewable energy mix,31,32 the environmental and financial benefit of reusable equipment becomes greater. 33
Comprehensive life cycle analysis is the gold standard for generating evidence for the environmental impact of a product or process, which may be a new concept for anaesthetists. 9 Life cycle analyses exist for anaesthetic agents and plastic drug trays, but not for non-plastic drug trays, disposable absorbent pads (blueys) and indeed most other items in medicine. We encourage an expansion of life cycle research of medical products and national best practice guidelines in procurement practices that provide a ‘triple bottom line’ approach to transition to more sustainable healthcare.
The next OCU will be on Friday 22 April 2022.
Footnotes
Author Contribution(s)
Acknowledgements
The author(s) acknowledge the 2021 TRA2SH steering committee for their contributions to the delivery of OCU. They would also like to thank Sebastian Ang, Stewart Brown, Tejas Chikkerur, Ryan Devlin, Jack Dixon, Steven Gaff, Alice Hickey, Kate Howell, Courtney Jones, Alison Kearney, Terence Kwok, Forbes McGain, Rajesh Pachchigar, Alistair Park, Jinesh Patel, Sally Perks, Liz Robinson, Catherine Stirzaker, David Story, Genna Verbeek, Tharindu Vithanage, Sarah Wong, Kewei Xu and all the other participating allied healthcare staff for their enthusiasm and contributions to OCU.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.