
Abstract
A shift in practice by anaesthetists away from anaesthetic gases with high global warming potential towards lower emission techniques (e.g. total intravenous anaesthesia) could result in significant carbon savings for the health system. The purpose of this qualitative interview study was to understand anaesthetists’ perspectives on the carbon footprint of anaesthesia, and views on shifting practice towards more environmentally sustainable options. Anaesthetists were recruited from four hospitals in Western Sydney, Australia. Data were organised according to the capability–opportunity–motivation model of behaviour change. Twenty-eight anaesthetists were interviewed (July−September 2021). Participants’ age ranged from 29 to 62 years (mean 43 years), 39% were female, and half had completed their anaesthesia training between 2010 and 2019. Challenges to the wider use of greener anaesthetic agents were identified across all components of the capability–opportunity–motivation model: capability (gaps in clinician skills and experience, uncertainty regarding research evidence); opportunity (norms, time, and resource pressures); and motivation (beliefs, habits, responsibility and guilt). Suggestions for encouraging a shift to more environmentally friendly anaesthesia included access to education and training, implementing guidelines and audit/feedback models, environmental restructuring, improving resource availability, reducing low value care, and building the research evidence base on the safety of alternative agents and their impacts on patient outcomes. We identified opportunities and challenges to reducing the carbon footprint of anaesthesia in Australian hospitals by way of system-level and individual behavioural change. Our findings will be used to inform the development of communication and behavioural interventions aiming to mitigate carbon emissions of healthcare.
Introduction
Volatile and gaseous anaesthesia represent 5% of total national United Kingdom healthcare greenhouse gas (GHG) emissions,1,2 and within hospitals can account for one-third of the total carbon footprint of surgical operating rooms.3,4 An anaesthetist’s daily anaesthetic practice can, therefore, greatly impact the magnitude of their individual GHG emissions, with some anaesthetic agents (particularly desflurane and nitrous oxide (N2O)) contributing significantly more than others.5 –8
Some health systems internationally have pledged to, or have already achieved, reduced use of desflurane and/or N2O in clinical care.9,10 In Australia, these are still frequently used, 11 although a growing number of hospitals have made considerable financial and environmental savings by eliminating desflurane.12,13 A shift in practice by anaesthetists away from high global warming potential anaesthetic gas use could result in significant carbon and cost savings. Propofol-based total intravenous anaesthesia (TIVA) is a well-established anaesthetic technique internationally that has a substantially lower carbon impact than inhalational anaesthesia. 14 Yet it is used less frequently than volatile and gaseous anaesthesia 11 despite demonstrating clinical equivalence for many procedures. 15
Anaesthetists can play a critical role in reducing the environmental impact of their clinical practice and profession. Importantly, any changes in practice must not adversely affect patient outcomes, so changes must be based on evidence about safety and effectiveness in addition to environmental and cost impacts. Recent guidance has been published providing safe and effective measures that anaesthetists can individually take to reduce their carbon footprint.16,17 These include avoiding desflurane and N2O, practising ‘low-flow’ anaesthesia, and utilising non-inhalational methods, such as regional anaesthesia or TIVA. However, little is known about the psychological, social, behavioural and clinical factors that motivate or prevent choosing sustainable anaesthesia. 18 Identifying key determinants of behaviour may inform more effective design and implementation of interventions that encourage lower emissions clinical care. This study aimed first to understand anaesthetists’ perspectives on the carbon footprint of anaesthesia and views on shifting towards more environmentally sustainable options. We then aimed to use the capability–opportunity–motivation (COM-B) model of behaviour 19 to identify potential mechanisms for change.
Materials and methods
Ethics
Ethical approval was obtained from the Sydney Children’s Hospitals Network (SCHN) Human Research Ethics Committee (2021/ETH00551).
Study design
This qualitative study involved in-depth interviews with anaesthetists in Sydney, Australia.
Participants and setting
Anaesthetists were recruited from four public hospitals in Sydney, Australia. Participants were eligible to participate if they were currently employed anaesthetic doctors at any level (including registrars and fellows), working at a children’s hospital in Sydney or one of three hospitals in the Western Sydney Local Health District (WSLHD). WSLHD is one of 15 local health districts in New South Wales (NSW), Australia and provides health services to approximately 1.1 million residents. 20 It is important to mention that at three of the four hospitals, desflurane canisters had been removed from anaesthesia machines but could still be accessed on provider request.
Three anaesthetists on the investigator team circulated an email advertising the study to their anaesthesia departments. Recruitment occurred in two rounds. In the first round, any anaesthetist who expressed interest and met the eligibility criteria was included. Preliminary analysis of the first 15 interviews showed that several topics warranted further investigation for better understanding. We also recognised that several first-round participants were highly conscious of the environmental impacts of anaesthesia. To capture a more diverse sample, we altered the study advertisement to make the focus on environmental impacts less explicit (i.e. we removed mention of ‘environmentally friendly anaesthesia’ in the study description but stated ‘reducing carbon emissions’ as a focus of exploration). Following the second round of recruitment, yielding a further 13 participants, it was decided that no further recruitment was required, given that similar ideas and patterns were repeatedly discussed with no new themes identified (i.e. saturation was achieved).
Data collection
Basic demographic information was collected by a short online survey. Interviews were conducted virtually by phone or videoconference. The interview guide (see Supplementary online information) covered a range of topics about determinants of current practice, understanding of environmental impacts of anaesthesia, and views on choosing lower emission options.
Data analysis
Interviews were audio-recorded and transcribed verbatim. Data analysis was completed using NVivo software (QSR International Ltd., Burlington, MA, USA; 2020), following a framework approach, a matrix-based analysis method used to order and synthesise textual data. 21 The framework was informed by a combination of a priori topics relevant to addressing the aims (e.g. ‘clinician barriers to practice shift’; ‘reasons for choice of anaesthetics’) and themes that were derived from initial data analysis (e.g. TIVA as a more visible form of physical waste than gases). Several subcategories were included (e.g. ‘clinical care vs. environmental care’ under ‘perspectives of environmental impacts’).
We systematically applied the framework to each interview transcript by extracting text from the transcripts into the relevant category of the framework. Charting was facilitated by NVivo and involved organising the indexed data into a more manageable format. Mapping and interpretation involved pulling together key patterns and characteristics of the data, clarifying concepts, and interpreting and making sense of the entire dataset considering our aims.
Finally, we used the COM-B model 19 to map perceived challenges and facilitators to behaviour change identified in the interviews. It was important to understand these to identify potential mechanisms for change.
Results
Twenty-eight anaesthetists were interviewed between July and September 2021. The average interview length was 37 minutes (range 15 − 70 minutes). Characteristics of the participants are summarised in Table 1. The average age was 43 years, 11/28 (39%) were female and most participants (23/28, 82%) worked predominantly in a tertiary hospital (n = 3 worked predominantly in a metropolitan non-tertiary setting). Thirty-two percent (8/28) had completed their anaesthesia training before 2010. At the time of interviewing, two participants were registrars, and one was a research fellow.
Characteristics of participating anaesthetists employed at four hospital sites in Western Sydney, Australia (N = 28).
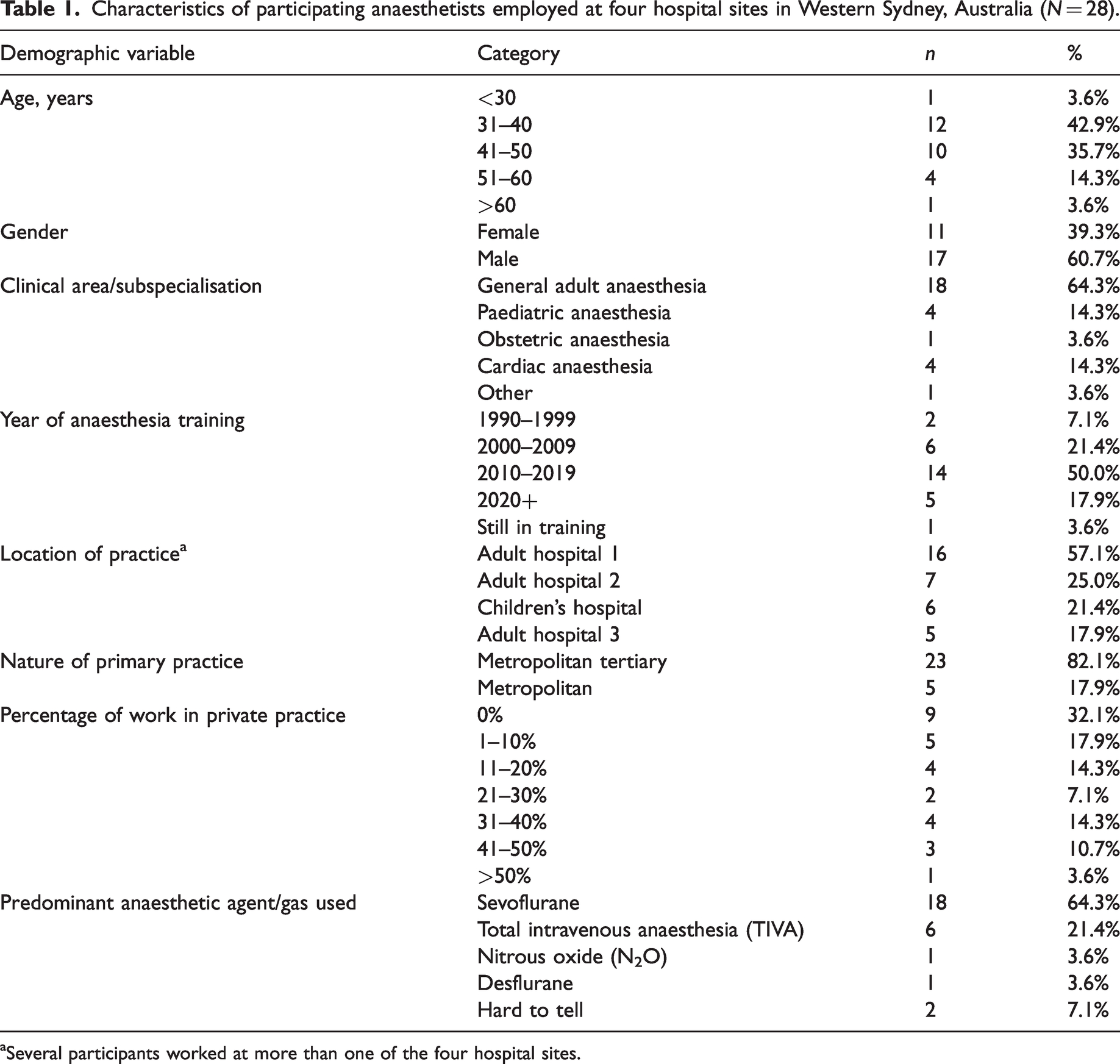
Several participants worked at more than one of the four hospital sites.
Sevoflurane was the most commonly reported anaesthetic agent used by the anaesthetists in this study (64%; n = 18), followed by propofol-based TIVA (21%; n = 6) (Table 1). The reported use of desflurane and N2O was rare among the sample, with only one participant reporting desflurane, and only one participant reporting N2O as their predominantly used anaesthetic agent.
Across the interviews, we identified capability−opportunity−motivational challenges to moving towards lower emissions anaesthesia options which we describe in Table 2 and the sections below, as well as suggestions that participants made for overcoming some challenges to change (Table 3). Text in italics below refers to direct quotations by participants, along with the respective participant ID number (‘[PX]’).
The challenges and barriers to shifting towards more environmentally sustainable anaesthesia: quotes by anaesthetists working across four metropolitan Sydney hospitals (N=28).
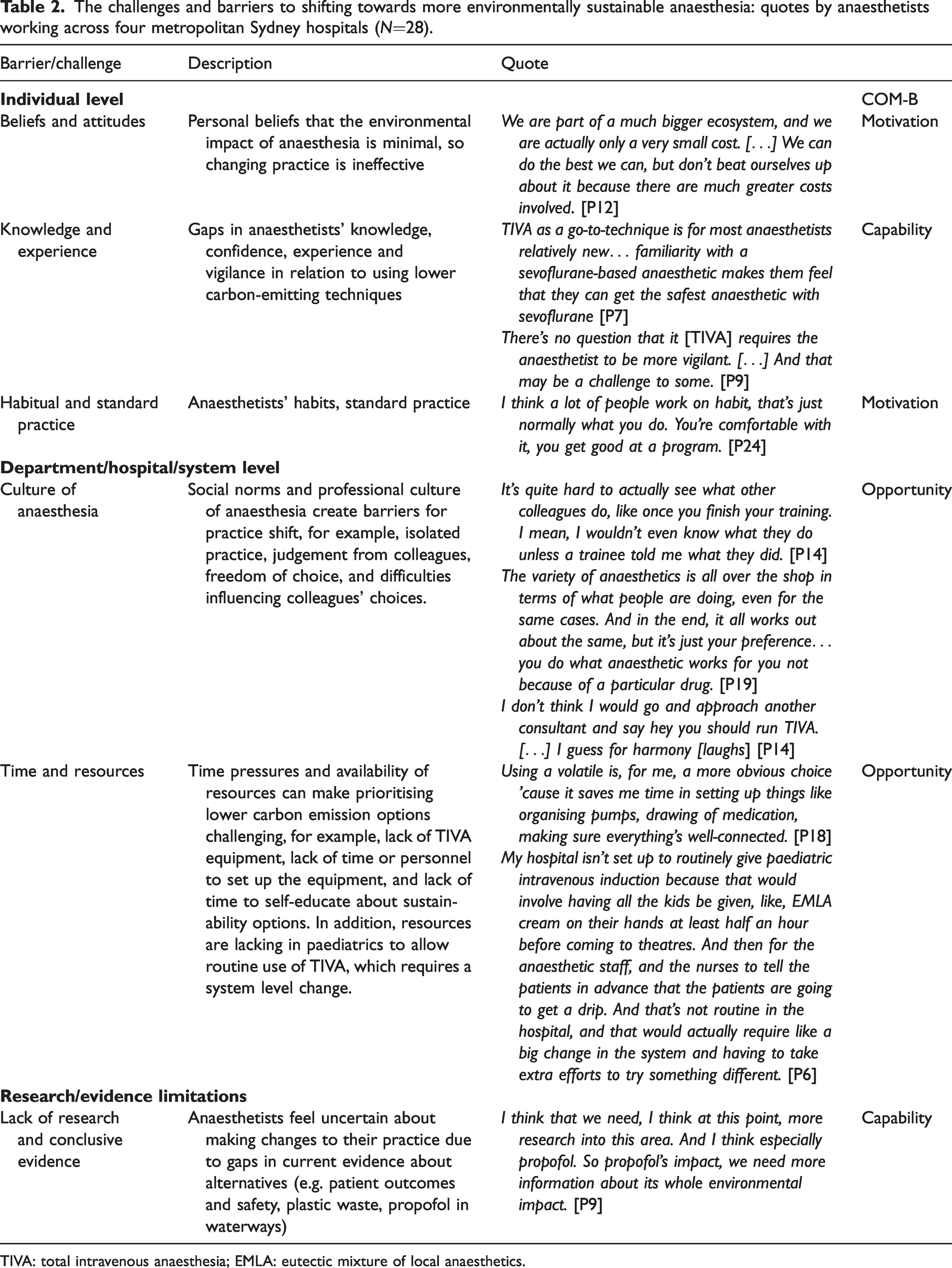
TIVA: total intravenous anaesthesia; EMLA: eutectic mixture of local anaesthetics.
Suggestions for overcoming some of the challenges and barriers to shifting towards more environmentally sustainable anaesthesia: quotes by anaesthetists working across four metropolitan Sydney hospitals (N = 28).
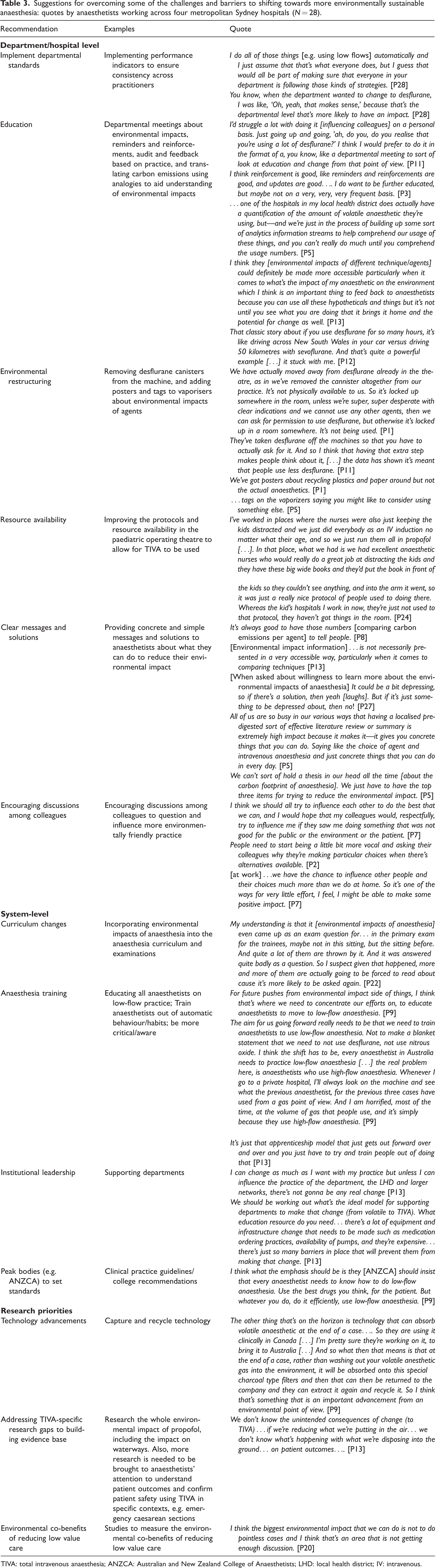
TIVA: total intravenous anaesthesia; ANZCA: Australian and New Zealand College of Anaesthetists; LHD: local health district; IV: intravenous.
Capability factors
Anaesthetists’ skills and experience with lower emissions anaesthetic options can influence confidence and ease in choosing greener anaesthesia techniques
Some participants perceived TIVA as ‘a little bit fiddlier’ [P20], risky (e.g. potential awareness), and requiring more vigilance from the anaesthetist: ‘TIVA requires a higher baseline level of attention and monitoring and care. There are more things that can go wrong at random times with TIVA than volatile [anaesthesia].’ [P20].
Some anaesthetists felt less skilled in using TIVA, for example, because ‘…for a lot of anaesthetists, TIVA is still a relatively new concept … and they are reluctant to use it’ [P10]. One participant explained that when they first completed training, the predominant way of anaesthetising was volatile-based, and ‘TIVA was seen as exceptional anaesthetic … non-mainstream and only reserved for special circumstances’ [P3], so their ‘comfort zone’ acquired from training was to give a volatile-based anaesthetic. On the other hand, anaesthetists who had trained more recently were less inclined to use more environmentally harmful agents, because they ‘didn’t really grow up using desflurane, so … got very comfortable with not using it’ [P11], ‘I just don’t even think of it as now something up my sleeve’ [P14].
A few participants held the opinion that registrars training with environmentally conscious consultants (who refused to use particular agents) could be disadvantaged. They explained that this could limit the opportunity to learn all anaesthetic techniques and diversify their skills through exposure and could even become an issue for patient safety, for example: There should be a bit less concern about the environmental impact on some of these techniques, which I think strongly discourages trainees from using certain techniques for a fear of—'Oh, you don’t care about the environment, hey—' questions from your consultants … it mentally impacts the ability of trainees to learn about using other techniques in a safe and skilled environment, whereas they might have to do it solo when their consultant isn’t around. [P20]
Anaesthetists can feel uncertain about making changes to their practice due to perceived gaps in current evidence
Several participants highlighted the complexity of choice between modes of anaesthesia when considering their environmental impact, stating that ‘it’s not just black and white that volatile [anaesthesia] is bad and TIVA is good’ [P21]. Many felt uncertain about changing practice due to a perceived lack of conclusive research evidence regarding a) the clinical and environmental impacts of alternative agents and techniques, and b) in support of removing or banning agents such as desflurane and N2O. There was also a strong sense of uncertainty regarding the broader ecological impacts of newer techniques such as TIVA, specifically the plastic waste involved and concern about the persistence, bioaccumulation and toxicity of propofol in waterways, which some felt were currently unresolved issues, for example: I think we need something to balance the scientific argument and really understand what propofol’s complete environmental impact will be. [P9] I haven’t necessarily got to the stage where I feel that I should be doing all my cases with TIVA, if in order to reduce the plastic footprint, I still haven’t quite reconciled the idea of the propofol waste and where that goes in terms of polluting our water supplies. [P26]
Opportunity factors
Social norms and the professional culture of anaesthesia can make it difficult to make greener choices or influence colleagues
Many participants described anaesthesia as an isolated practice, wherein anaesthetists tend to work alone, ‘not really exposed to other people’s practice’ [P21], particularly in private practice. As a result, some anaesthetists become isolated from newer techniques and workplace norms that encourage self-reflection, accountability and discussion around the environmental impacts of anaesthesia. Freedom of choice also meant that there was large variety in preferred techniques.
A small number of participants had experienced judgement and anger from colleagues who perceived making shifts for environmental reasons as ‘a tree-hugging thing’ [P13], for ‘a crazy greenie’ [P2]. Being judged as going against the norm was portrayed as a barrier to behaviour change because, ‘people like to follow the common practice in the department, no one wants to be someone on the extreme’ [P13].
Most participants said they would not feel comfortable attempting to influence their colleagues to use more environmentally friendly options due to ‘professional courtesy’ [P15], to maintain ‘harmony’ [P3] and avoid potential safety risks, for example: The last thing you want is to convert somebody into another type of anaesthetic or another version of the anaesthetic that they’re not used to and then have them provide unsafe anaesthesia. [P3]
Time pressures and the availability of resources can make prioritising lower carbon emission options challenging
Participants explained that delivering TIVA requires extra equipment and takes longer to set up than a volatile anaesthetic. When rapid patient turnover is a priority, volatiles are the ‘most obvious choice’ [P18] pragmatically, due to faster setup and perceived wake-up time, ‘the surgeon will get annoyed if you are slowing down the list’ [P13]. This was particularly an issue in private practice, in which patient lists are expected to move quickly. A few participants also mentioned that without having adequate personnel available (e.g. anaesthetic nurses), using TIVA is difficult and ‘too labour intensive’ [P10].
Most participants raised some concerns around the availability of equipment for TIVA (e.g. syringes, infusion pumps, ‘timely access to propofol bottles’) limiting their capacity to use it. Private hospitals were specifically noted as being ill-equipped for running TIVA: ‘the private hospitals didn’t buy the algorithms in their hardware’, and their impression was that private hospitals ‘didn’t see it as worthwhile because it’s an additional cost’ [P3].
A few participants discussed issues in hospitals where anaesthetists practise across multiple hospitals and therefore do not have the time to work out sustainability solutions, related to what one participant described as a ‘lack of institutionalised energy to decrease our environmental impact’ [P11].
Motivational factors
Personal belief that the environmental impact of anaesthetic gases is minimal, so reducing use may be ineffective
Some participants believed that the environmental impact of anaesthesia is minimal, comprising only a ‘small subsection’ of total hospital or healthcare emissions and compared with the environmental damage caused by other sectors, ‘our anaesthetic gases contribute to a very, very small proportion of GHG emissions’ [P9]. They reasoned that limiting the use of volatiles for environmental reasons may be an unnecessary or ineffective way to reduce GHG emissions, for example: Mining companies are doing a lot more environmental damage than I am by sometimes using sevo [sevoflurane]…. So, I’m not sure how important my choices are… [P28]
Interestingly, the proportion of GHGs attributed to anaesthesia was viewed differently between participants. For example, one participant interpreted the approximate percentage of emissions attributable to anaesthesia as small, ‘only about one percent of GHGs in the whole world’ [P25], while another participant perceived this same percentage as representing a significant impact: If you realise that you are one percent as healthcare workers, then you might actually go, ‘Oh, we’re not as insignificant as I first thought’. [P4]
Many participants explained that because volatile/gaseous anaesthesia is not visible, ‘sevoflurane is like an invisible waste’ [P12], it is easier to be unaware of the impact or to believe it is negligible. On the other hand, we were told that TIVA produces visible waste, ‘you can see a bag full of syringes and plastic rubbish’ [P12], so it can seem worse for the environment than the invisible impact of volatiles/gases. ‘Psychologically it just feels like you throw a lot more visible waste away’ [P12]. One participant voiced their perspective that anaesthetics can never be net zero, no matter what steps they take to minimise their personal contribution: ‘I can’t provide what I’m doing without using carbon. Anaesthetics will never be net zero without having an offset’ [P23].
Environmental care is perceived as secondary to patient care
While most anaesthetists indicated concern regarding the environmental impacts of anaesthesia, almost all reported that patient safety and comfort is their number one priority and the biggest factor affecting their choice of anaesthetic agent: ‘clinical care will always trump environmental impacts’ [P12]; ‘I don’t wanna give a worse anaesthetic just so that I can save a few tons of CO2’ [P13].
One participant explained that their overall impression was that anaesthetists would choose their anaesthetics based on ‘anaesthetic reasons first, and then cost reasons are secondary, and environmental reasons are on the radar of a very small subsection’ [P23]. However, there appeared to be a diversity of opinion on whether anaesthetists were motivated by environmental care. One argued that it does not have to be one or the other: ‘we can safely anaesthetise patients whilst being environmentally aware’ [P2]. Many described avoiding desflurane because of its ‘huge environmental cost’ [P3], despite perceiving it as having some advantages for particular patient groups.
Using particular anaesthetics habitually is comfortable and predictable
Many participants stated that they, or their colleagues, have developed a standard way of practising, in which they are ‘just going to work and doing what they were taught or what they’re comfortable with day-in-day-out’ [P28]. This way of practising brought comfort, certainty, predictability, and less effort, whereas seeking out or understanding alternative ways of practising was perceived as uncomfortable and unpredictable, for example: Most people wanna give the same anaesthetic everyday cause there’s a certainty a comfort in that, … whereas if you change over to something else, it’s highly unpredictable. You have to expend more effort. [P13] There are certain consultants you know will want TIVA and you know, before you start, it’s going to be a TIVA day…. And then there are other anaesthetists that, when you see their name, it’s going to be a sevoflurane day. [P10]
A sense of personal responsibility or guilt in relation to anaesthesia’s carbon footprint can motivate practice shift
It became evident from the interviews that, for some participants, awareness of the environmental impact of anaesthesia had translated emotionally and manifested in their practice. Some participants perceived themselves as personally having a key role to play in improving the sustainability of anaesthesia, while others mentioned that anaesthetists more broadly have a collective responsibility in reducing the environmental harms of their profession. Some reported a responsibility to protect future generations, which influenced their choices, for example: There was a year or so with lots of awareness and constantly feeling guilty … and so, I’m doing a little bit … because I have children and I’m really worried about the future, not just theirs but generally, that helps. [P16]
Several participants felt guilty about the harm they as anaesthetists are causing the environment, and tried to counter this by supporting sustainability initiatives at their hospital for example, or making environmentally friendly choices in their personal lives, such as recycling or installing solar panels. One participant described the contrast in their work versus home identity: At home, I’m very green, trying to recycle everything, limit the use of water and electricity…. Sometimes at work, I feel like I’m a different person cause there’s so much rubbish I produce. [P18] Sometimes I feel like, even more like guilt, as in like yesterday, I used a lot of volatiles. Maybe I should use some more TIVA today, to try to balance it out a little bit. [P1]
Opportunities and recommendations for practice shift
Various recommendations were made by participants to enable a shift towards more environmentally friendly anaesthesia (Table 3). These include education and training, implementing guidelines and audit/feedback models, environmental restructuring (i.e. modifying the physical environment to encourage more sustainable choices), improving availability of TIVA equipment, and building the research evidence base on TIVA safety and impact on patient outcomes.
Some participants mentioned department and hospital-level changes that have already been implemented in several hospitals, specifically targeting a reduction in desflurane use, including complete removal from anaesthesia machines. Other existing strategies included adding visual tactile reminders such as posters or labels on volatile bottles, prompting anaesthetists to consider the environment when making anaesthetic agent choices.
There was a consensus among participants that anaesthetists should not be forced to change their practice or told what to do. For this reason, many participants strongly felt that increasing awareness around the carbon impacts of anaesthesia was the best way forward. Several participants noted that education efforts should particularly target private practice for ‘big gains’ [P9].
One participant indicated reducing low value care in anaesthesia as an important strategy for reducing emissions: ‘I think the biggest environmental impact that we can do is not to do pointless cases and I think that’s an area that is not getting enough discussion.’ [P20].
Discussion
This study provides valuable insights into the perceived challenges of delivering more environmentally sustainable anaesthesia. We identified and mapped factors that motivate or prevent the transition to greener anaesthesia, in addition to suggested ways to overcome these from the perspective of clinicians on the frontline. Barriers to the wider use of greener anaesthetic agents were identified across all components of the COM-B model: capability (clinician skills and experience, uncertainty around state of the evidence); opportunity (social and professional norms, time and resource pressures); and motivational factors (personal beliefs, habitual clinical behaviour). A sense of responsibility and guilt was reported by several participants as a key motivation for selecting lower emission alternatives. Recommendations for shifting towards more environmentally friendly anaesthesia practice included access to education and training to address the knowledge and skill barriers, implementing guidelines and audit/feedback models, environmental restructuring, improving the availability of TIVA equipment to address resource barriers, reducing low value care, and building the research evidence base on TIVA safety and impact on patient outcomes.
Previous studies have identified similar challenges to providing greener clinical care to those identified in this study, including psychological and social barriers to action, conflict of priorities in care delivery, organisational constraints, and lack of leadership.22 –24 This study adds further understanding of individual and system-level factors preventing sustainable behaviour change, including the difficulties weighing up the consequences of visible (plastic) versus invisible (gaseous) wastes and clinician uncertainty regarding the available evidence on alternative options for anaesthesia, particularly concern about TIVA’s ecological contamination and unknown impacts on biodiversity. Previously underexplored social factors were also identified in this study, including how professional culture and lack of accountability may be hindering behaviour change. These social factors suggest that efforts to encourage a cultural shift in the profession may be warranted. Importantly, our results highlight the value of prioritising better system-level support for clinicians to practise greener healthcare through improved access to training and educational resources and encouraging institutional leadership and involvement.
Implications
Global calls for clinician action have already been made in this area, 25 and system-level initiatives such as the Greener NHS plan aim to reduce the use of desflurane and N2O. 26 Reducing the use of these agents should be prioritised to reduce global environmental impacts immediately without compromising patient care. 27 In Australia, our findings suggest that some anaesthetists feel a sense of collective responsibility to reduce the environmental impacts of their profession, with some reporting that their responsibility to protect future generations influences their choices. Shifts in personal choices are already proving impactful in lowering emissions by anaesthetists worldwide,28,29 including some hospitals and individual anaesthetists who have begun implementing change (e.g. removing desflurane canisters). Further action is needed to implement the clinician-focused strategies for practising more sustainably 13 (i.e. avoiding desflurane and N2O, practising low-flow anaesthesia, and using non-inhalational methods). Our study has identified several barriers that may be preventing the uptake of some of these strategies, as well as settings where volatile anaesthesia may be in higher use. We recommend that these be addressed as a priority as we cannot expect behavioural change without intervening on key barriers across all components of the COM-B model.
Mapping our results to the COM-B model highlights opportunities to move forward with intervening on clinical behaviours using evidence-based behaviour change techniques (BCTs) to promote sustainable practice. 19 For example, to overcome the identified capability challenges, effective interventions may include workshops or courses educating clinicians on the social and environmental consequences of high carbon-emitting agents and training clinicians in using lower carbon-emitting anaesthetic techniques. Carbon literacy should be addressed among anaesthetists to improve their ability to make decisions appropriately with an awareness of environmental consequences. Further research is needed to clarify and inform anaesthetists of the ecological impacts of TIVA (e.g. polluting waterways). Interventions targeting the opportunity factors could include restructuring the physical environment (e.g. increasing the availability of TIVA equipment) and supporting hospitals and anaesthetic departments to shift social norms by creating cultures that value environmental care.16,25 Furthermore, employing ‘clinical champions’ to encourage and advocate for sustainable practice and avoid low value care 30 could address the lack of institutionalised energy and capacity to prioritise sustainable behaviour change. 31 Finally, BCTs to target motivational barriers might include outcome-focused goal setting and, given that our data indicate responsibility as a motivation for change, emphasising the consequences of using high carbon-emitting agents. We recommend that future interventions should only implement and assess a few BCTs simultaneously, with a comparison group, to most accurately assess which are effective. 32
Strengths and limitations
The project was a collaborative partnership between researchers and clinicians to support change towards the delivery of more environmentally friendly anaesthesia. It demonstrates the challenges of practising more sustainably from the perspectives of a sample of Australian anaesthetists representing common practice settings. A noteworthy strength is mapping behavioural barriers and facilitators using the COM-B model to allow the relevant BCTs to be applied in future behaviour change interventions.
A limitation of this study is the recruitment of self-selecting participants from public metropolitan hospitals from one state in Australia, many of whom were already interested in and aware of the environmental impacts of anaesthesia. Desflurane canisters had been removed from anaesthetic machines in three of the four hospitals, and as such, we were unable to explore barriers to practice shift among anaesthetists primarily using higher carbon-emitting agents. We acknowledge that this study focused on general anaesthetic agents and note that many additional environmental impacts of anaesthesia contribute to its overall carbon footprint, including single-use equipment. This study also did not explore regional anaesthesia as a low carbon option as well as the relative benefits, harms and costs when comparing minimal flow volatile anaesthesia with TIVA. These topics warrant further research.
Conclusions
This qualitative study highlights opportunities and challenges to reducing the carbon footprint of anaesthesia in Australian hospitals by individual and system-level behavioural changes. As part of a larger programme of research aiming to mitigate carbon emissions and support long-term sustainability of healthcare, these findings are informing the development of communication and behavioural interventions to support change towards more environmentally friendly anaesthetic practice.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X231212211 - Supplemental material for Exploring anaesthetists’ views on the carbon footprint of anaesthesia and identifying opportunities and challenges for reducing its impact on the environment
Supplemental material, sj-pdf-1-aic-10.1177_0310057X231212211 for Exploring anaesthetists’ views on the carbon footprint of anaesthesia and identifying opportunities and challenges for reducing its impact on the environment by Matilde Breth-Petersen, Alexandra L Barratt, Forbes McGain, Justin J Skowno, George Zhong, Andrew D Weatherall, Katy JL Bell and Kristen M Pickles in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Acknowledgements
Katy Bell is supported by a National Health and Medical Research Council (NHMRC) investigator grant (no. 1174523). She is an Investigator for the Wiser Healthcare Collaboration, funded by a NHMRC Centre for Research Excellence grant (no. 2006545).
Forbes McGain has received grant funding from the NHMRC and Medical Research Future Fund, along with Australian and New Zealand College of Anaesthetists and College of Intensive Care Medicine of Australia and New Zealand grants. He receives royalties for a co-patented medical device (the McMonty hood).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.