
Abstract
The COVID-19 pandemic has strained surgical systems worldwide and placed healthcare providers at risk in their workplace. To protect surgical care providers caring for patients with COVID-19, in May 2020 we developed a COVID-19 Surgical Patient Checklist (C19 SPC), including online training materials, to accompany the World Health Organization Surgical Safety Checklist. In October 2020, an online survey was conducted via partner and social media networks to understand perioperative clinicians’ intraoperative practice and perceptions of safety while caring for COVID-19 positive patients and gain feedback on the utility of C19 SPC. Descriptive statistics were used to characterise responses by World Bank income classification. Qualitative analysis was performed to describe respondents' perceptions of C19 SPC and recommended modifications. Respondents included 539 perioperative clinicians from 63 countries. One-third of respondents reported feeling unsafe in their workplace due to COVID-19 with significantly higher proportions in low (39.8%) and lower-middle (33.9%) than higher income countries (15.6%). The most cited concern was the risk of COVID-19 transmission to self, colleagues and family. A large proportion of respondents (65.3%) reported that they had not used C19 SPC, yet 83.8% of these respondents felt it would be useful. Of those who reported that they had used C19 SPC, 62.0% stated feeling safer in the workplace because of its use. Based on survey results, modifications were incorporated into a subsequent version. Our survey findings suggest that perioperative clinicians report feeling unsafe at work during the COVID-19 pandemic. In addition, adjunct tools such as the C19 SPC can help to improve perceived safety.
Introduction
The strain placed on surgical systems by the COVID-19 pandemic has been profound. It has resulted in cancellations of elective operations and delays in emergency and essential surgical care in an already fragile ecosystem. 1 Surgical systems have rapidly adapted to provide ongoing access to emergency and essential surgical care, while ensuring patient and provider safety. However, the risk to frontline healthcare workers during this pandemic is substantial, and systemic, infrastructure and resource constraints pose huge challenges.2–5
To address some of the safety concerns imposed by the pandemic, perioperative care providers mobilised to provide guidance on operating room conduct.6–13 Practically, introducing new guidelines during a viral pandemic is difficult. While intended to be helpful, they may add a cognitive load to already stressed clinicians. This can result in implementation of COVID-19 infection prevention practices with variable fidelity.
In the early weeks of the pandemic, Lifebox (https://lifebox.org), in collaboration with the World Federation of Societies of Anaesthesiologists (WFSA)(https://wfsahq.org) and Smile Train (https://www.smiletrain.org), developed a COVID-19 Surgical Patient Checklist (C19 SPC) (Figure 1).
14
This perioperative safety tool was designed to aid surgical teams in coordinating new behaviours when caring for COVID-19 surgical patients and meant to be used in conjunction with the World Health Organization Surgical Safety Checklist (WHO SSCL). It was developed through a consultative process that included review of available best practice evidence, recommendations by reputable international organisations and perioperative clinician consensus with feedback from partners across several high- (HIC), middle- and low-income (LIC) countries. The goal was to promote recommended practice for operating room behaviours that reduce the risk of SARS-CoV-2 transmission to perioperative care providers. The checklist also incorporated a resource page for rapid access to information on aerosol
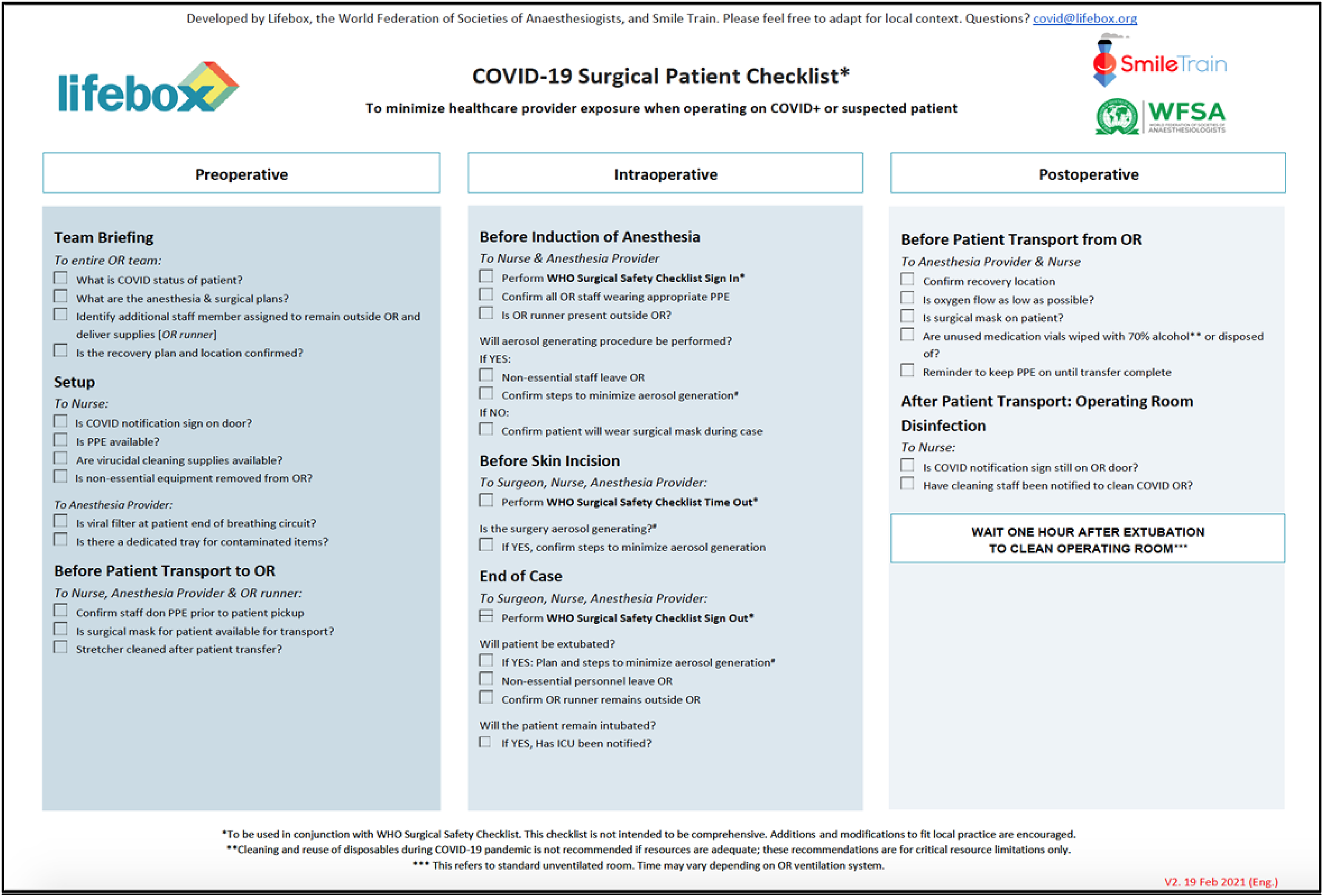
COVID-19 Surgical Patient Checklist, updated February 2021.
The C19 SPC was disseminated through partner and social media networks beginning in May 2020. To accompany this distribution, a package of training materials was created by Lifebox and Jhpiego (Johns Hopkins Program for International Education in Gynecology and Obstetrics) (https://www.jhpiego.org) and is hosted online (https://www.lifeboxlearningnetwork.com/course?courseid=covidspc). In addition to the online training resources, from May 2020 to March 2021 Lifebox, Smile Train and Jhpiego delivered eight Training of Trainer sessions to partner institutions via Zoom. Trained trainers reported delivering an additional seven training sessions locally in person.
While consensus recommendations for theoretical adaptation of the WHO SSCL during the COVID-19 pandemic have been previously published, 21 actual implementations of these recommendations have not been studied. The aim of this evaluation was to use a structured approach to better understand perioperative clinicians’ intraoperative practice and perceptions of safety while managing COVID-19 positive or suspected patients undergoing surgery. We also wanted to gain feedback on the utility of the C19 SPC to help inform future modifications.
Methods
Survey design
Institutional Review Board exemption was obtained from Boston Children’s Hospital (20 July 2020). An online cross-sectional survey was created to evaluate the use of the C19 SPC by perioperative providers when caring for COVID-19 positive or suspected patients undergoing surgery. To ensure cross-disciplinary and broad geographic input and content validity, a questionnaire was developed by representatives from anaesthesia, surgery and nursing disciplines from Ethiopia, India, Cambodia, Nigeria, Rwanda, the United States and the United Kingdom. In addition to basic demographics, the questionnaire included questions on the use of the C19 SPC, associated training, most and least useful aspects of the C19 SPC, recommended modifications, and perceptions of safety during the COVID-19 pandemic. Free text responses were incorporated to obtain qualitative data regarding key concerns of survey respondents when managing COVID-19 positive patients, the impact of the C19 SPC utilisation on operating room practice, any challenges in its use and their reasoning for any changes in perception of safety when using the C19 SPC. Suggested modifications by respondents to the C19 SPC were also requested. The full survey tool is available in online supplementary materials.
Survey administration
To receive broad geographic input, the questionnaire was translated into nine languages and an invitation to participate was distributed online via open dissemination through the Lifebox, Smile Train, Jhpiego and WFSA partner networks and social media over a one-month period in October 2020. These groups and local partners work collaboratively on initiatives to improve the safety of global surgery and anaesthesia. Their networks were used to distribute the questionnaire widely with the intention of findings being actionable in real time if training or other resource needs were identified. An individual’s participation was voluntary and anonymous. The Survey Monkey website (Survey Monkey, Palo Alto, CA, USA) was used for data collection. Survey responses were collected anonymously.
Data analysis
Collected responses were exported to Microsoft Excel v.16.47 (Microsoft Corporation, Redmond, WA, USA). Quantitative data were analysed in Stata (15.1, Statacorp LLC, College Station, TX, USA) using descriptive statistics and chi-square, Kruskal–Wallis, analysis of variance and t-test where appropriate to compare groups, with alpha set at 0.05. Free-text response questions were not mandatory; however, all responses to free-text questions were included in the analysis. To identify emerging themes related to safety concerns, reasoning for altered safety perception, suggested modifications, challenges, and impact of C19 SPC utilisation, qualitative data derived from free-text responses were coded thematically by three members of the research team and a codebook inductively and iteratively derived. The excerpts were separated, organised and coded manually using Microsoft Excel v.16.47. Discussion among three of the authors was used to assign the initial codes and develop the coding framework. A second group of three authors applied codes from the codebook in a blinded fashion to excerpts to determine inter-rater reliability. The six authors reviewed together to reach consensus on discordantly coded excerpts until the codebook and themes were finalised.
Results
While 547 perioperative clinicians from 63 countries completed the questionnaire (Table 1) only 539 were analysed. Eight completed questionnaires were excluded from the analysis as no country was listed therefore an income group could not be assigned. The highest proportion (32.8%) were from Sub
Participant demographics and hospital characteristics.
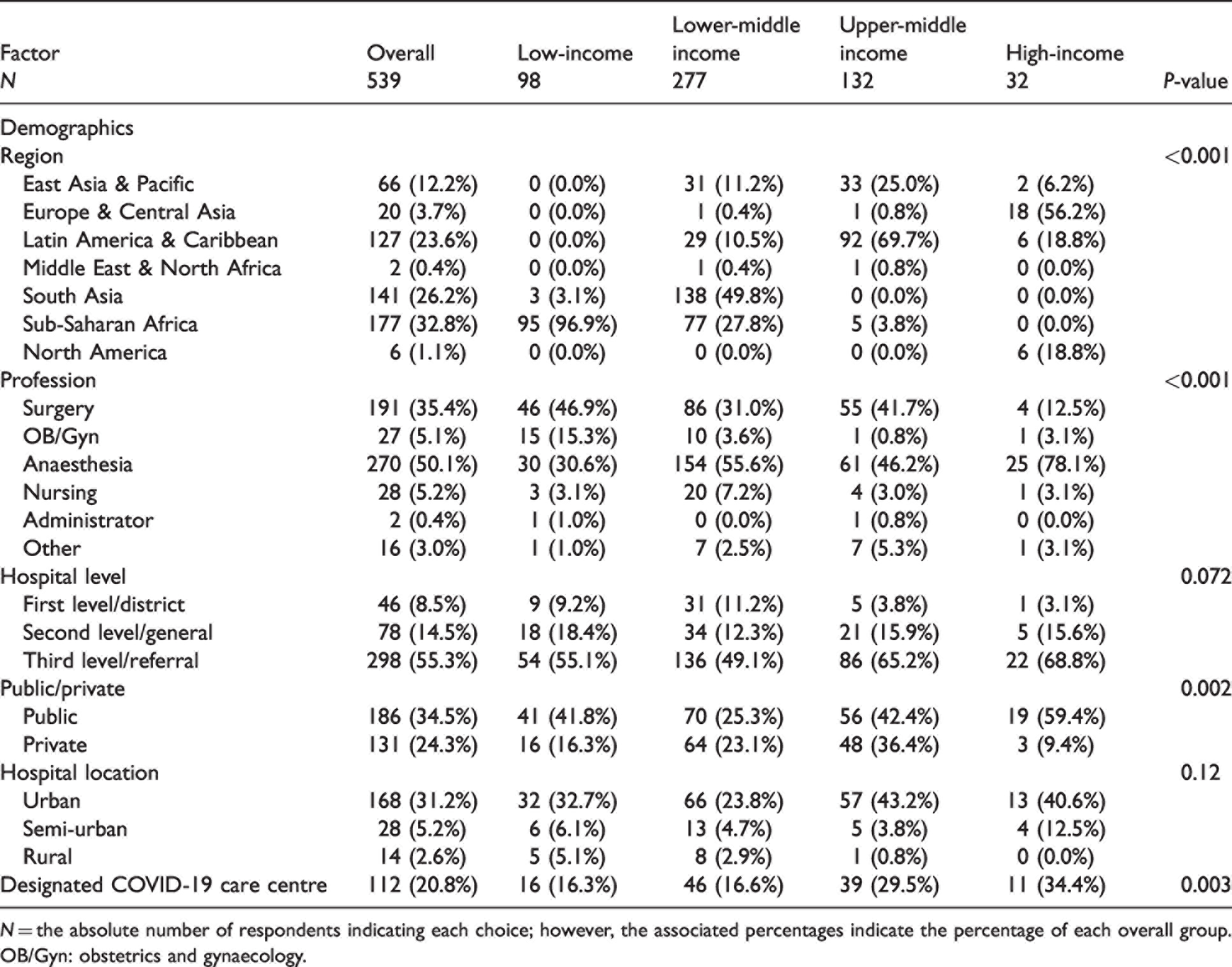
N = the absolute number of respondents indicating each choice; however, the associated percentages indicate the percentage of each overall group.
OB/Gyn: obstetrics and gynaecology.
Overall, about half of respondents had cared for COVID-19 positive patients (49.9%) and were aware of the C19 SPC (56.6%) (Table 2). Nearly half (45.3%) had received training on the C19 SPC and 34.7% had personally used it. Of those, a quarter (26.2%) had adapted the checklist to their local context and just over half (51.3%) reported a change in practice following its implementation. Few (12.8%) had encountered difficulties with implementation. Those who were unaware of the C19 SPC were asked to review it and provide feedback. Almost all respondents (83.8%) of the 234 who had not seen the C19 SPC agreed the checklist appeared useful. Half (52.1%) of respondents reported feeling safe caring for COVID-19 positive or suspected patients and 62.0% reported feeling safer using the C19 SPC.
COVID-19 Surgical Patient Checklist use and impact on perceived safety.
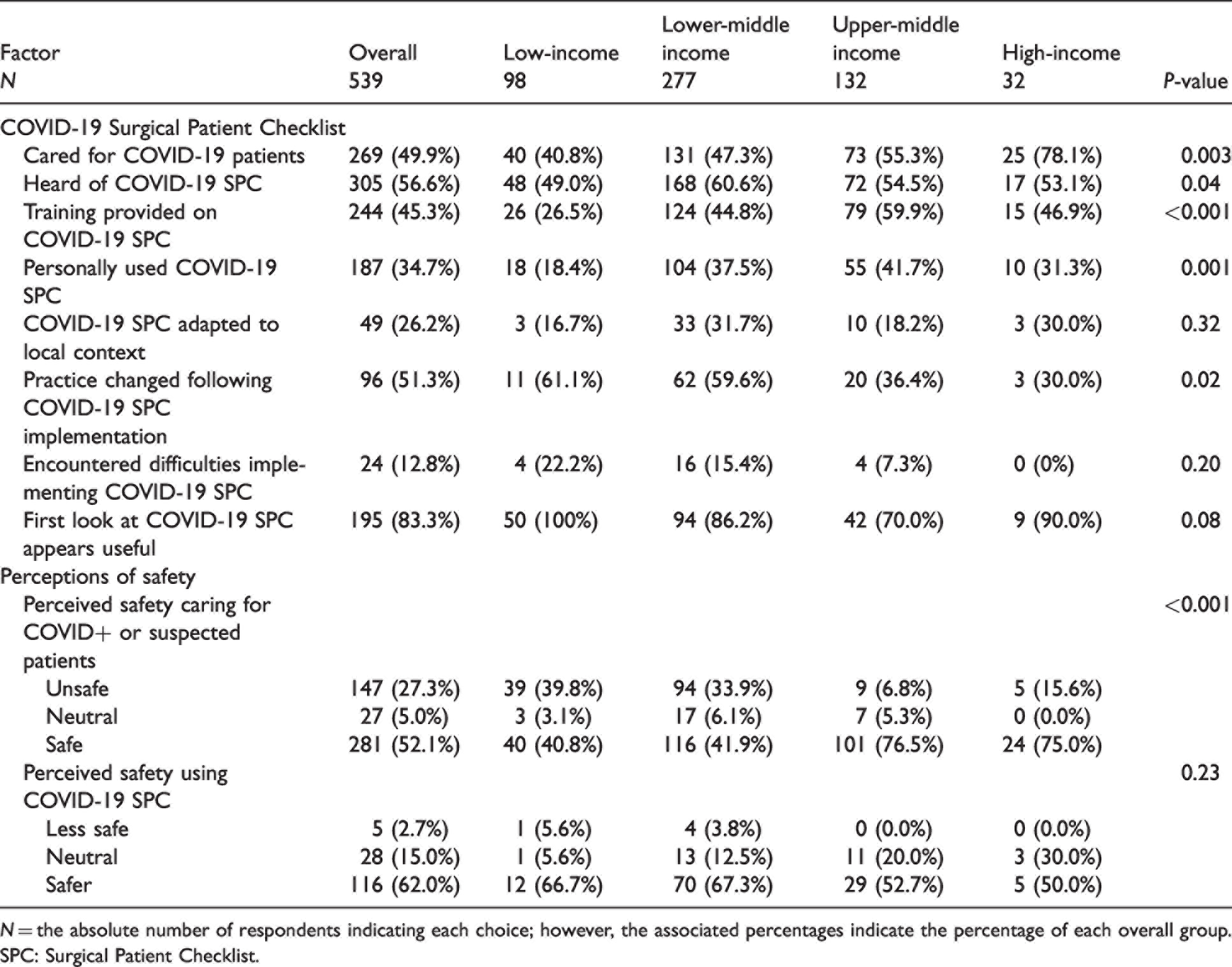
N = the absolute number of respondents indicating each choice; however, the associated percentages indicate the percentage of each overall group.
SPC: Surgical Patient Checklist.
When stratified by World Bank income classification, fewer clinicians from LICs had cared for COVID-19 positive patients (P = 0.003), and fewer had received training on the C19 SPC (P < 0.001). However, more clinicians from LICs saw practice change following implementation (P = 0.02). Respondents from all income groups viewing the C19 SPC for the first time agreed it appeared useful. Respondents from LICs were more than twice as likely to report feeling unsafe at work as those in HICs (39.8
Respondents were asked to report their greatest concern when managing COVID-19 positive patients. Most clinicians cited fear of personal infection with COVID-19 or transmission to family members, colleagues or other patients (Table 3). Other commonly reported fears centred on aerosol production and contamination of the operating room, the surgical patient’s risk of developing complications related to COVID-19, and workplace functionality, such as unclear infection prevention and patient care protocols, and inconsistencies in patient testing. Shortages of resources such as PPE were a major concern amongst respondents, when caring for COVID-19 positive patients.
Qualitative codebook.
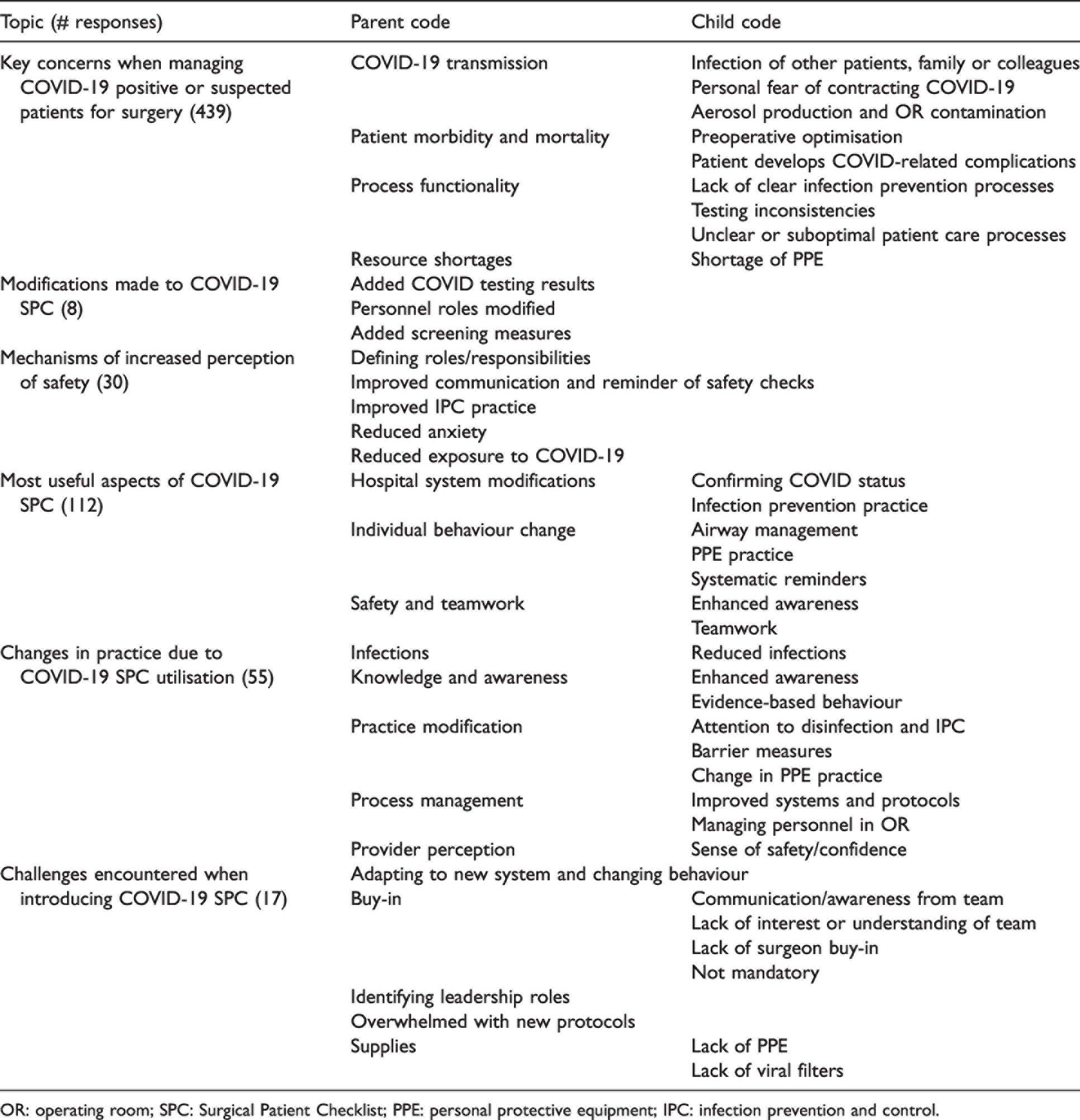
OR: operating room; SPC: Surgical Patient Checklist; PPE: personal protective equipment; IPC: infection prevention and control.
A few respondents reported making context-relevant modifications to the C19 SPC (Table 3), such as adding a prompt to review COVID-19 test results, rearranging personnel roles to align with their hospital workforce and adding symptom screening questions. Those who felt safer at work when using the checklist for surgical patients cited clearer roles and responsibilities, improved communication and safety practice and reduced anxiety as some reasons for their increased sense of safety.
The most useful reported aspects of the C19 SPC fit broadly into three themes: hospital system modifications, such as COVID-19 test confirmation and infection prevention and control (IPC) practice; individual behaviour changes, such as PPE donning and doffing and airway management; and safety and teamwork. Respondents that reported changes in practice as a result of using the C19 SPC cited improved attention to evidence-based and IPC practice and improvement in the personal protective measures taken by the team. They also reported improvements in the system and operating room protocols used as a result of using the C19 SPC, and improved personnel management, as well as a greater sense of safety and confidence at work.
Although few had encountered difficulties with implementation, some challenges were reported when introducing the C19 SPC. Themes that emerged included challenges with behaviour change, lack of buy-in from surgeons or other surgical team members, and difficulty identifying leadership roles to drive the checklist. Some respondents reported that they were overwhelmed with the number of new COVID-19 related protocols and practice. For others, the biggest challenges were simply a lack of material resources like PPE and viral filters to fulfil the C19 SPC recommendations.
Discussion
This survey of global perioperative clinicians found that many respondents feel unsafe in the workplace and that their biggest concerns are related to COVID-19 transmission to themselves, their colleagues or their family members. Findings suggest that use of the C19 SPC for perioperative care of surgical patients helped clinicians to feel safer and reportedly led to practice change in a majority of respondents who had used it. As noted by this work and others,21–24 checklists can improve teamwork and communication, and clarify team member roles and responsibilities in the operating room–an important element of safe, multidisciplinary patient care. While rapid endorsement of checklists by numerous organisations such as societies and specialty colleges can increase awareness, distribution and uptake, the importance of adaptation to local context cannot be overemphasised.25–28 Similarly, our survey found that over a quarter (26.2%) of respondents who had used the C19 SPC reported that they had adapted it.
The survey participants provided vital feedback on the C19 SPC components based on their practice and real world experience. However, less than half of the respondents reported that they had used the C19 SPC, highlighting a need for further dissemination and strategies to increase its use. Of the two-thirds of respondents who had not used it, a high proportion (83.8%) reported that they felt it appeared useful.
After analysis of survey results and feedback, the C19 SPC was modified to reflect recommended changes suggested by the end users (Figure 1). These changes included rewording and reorganisation for clarification, flow and role allocation, verification of COVID-19 status of patient, clarification around PPE use and updates to guidance for aerosol-generating procedures. This updated C19 SPC was made available online and modifications for the local context were encouraged as required. Notification of the updated checklist was disseminated through partner and social media networks. In addition, some of the qualitative findings of this study, particularly around implementation challenges such as institutional buy-in, assigning roles and staff being overwhelmed with COVID-19 protocols, informed updates in the C19 SPC training materials.
The recent work by Panda et al. 21 outlines consensus recommendations assembled by an international panel for theoretical adaptation of the WHO SSCL as part of a surgical team response to the COVID-19 pandemic. Elements that they recommended in their adapted checklist include review of patient COVID-19 status, discussion of surgical and anaesthesia plans, use of safety checks around PPE use, establishment of equipment availability and specimen handling and confirmation of patient recovery location. Their recommendations also proposed a framework for hospital teams to rapidly implement this modified checklist that included the importance of support by relevant leadership, content modification to the local context, simulation-based training and frequent revision as scientific knowledge of best practice related to COVID-19 advanced.
Our work developing and implementing a C19 SPC through our partner network further supports these theoretical recommendations and underscores the importance of including provider safety measures into routine surgical care during the pandemic. Through a separate consultative process, items for inclusion in the C19 SPC included many of those recommended by Panda et al., reinforcing the key concerns of perioperative providers when managing COVID-19 positive patients. While Panda and colleagues’ theoretical recommendations were to modify the WHO SSCL, the C19 SPC was developed using an alternative approach. It is meant to be used as an adjunct with the WHO SSCL and includes prompts to perform the WHO SSCL at relevant timepoints. Both approaches encourage checklist revision based on context-specific modifications. Some hospitals in our study merged the two Checklists, so that only one tool was needed in the operating room. This approach can avoid the use of additional tools that can lead to user fatigue and lack of buy-in. However, some facilities may prefer to keep them separate, as the C19 SPC is focused on protecting providers in the context of COVID-19 in the workplace whereas the WHO SSCL is aimed at patient safety.
Limitations
This study has several limitations. The survey tool was distributed to providers partnering or in communication with the groups that designed and implemented the C19 SPC. Their responses may not be representative of other perioperative clinicians working in contexts not affiliated with Lifebox, Smile Train, Jhpiego or WFSA. The inclusion of social media as a method of survey distribution, while aiming for a broad reach and mirroring the distribution of the checklist, did not enable a response rate to be measured. Furthermore, each country is experiencing waves of COVID-19 infection at different timepoints. Responses were based on the prevalence and practice environment at the time of the survey and may not reflect current perceptions of safety or infection prevention practice. As some higher-income countries are reaching vaccination of a high proportion of their populations, other lower-income, countries are experiencing the worst surges yet, highlighting the importance of continued attention to provider safety. It is worth noting that a large proportion of LIC respondents were from Sub-Saharan Africa. In addition, the survey tool did not ascertain details of checklist use such as proportional case utilisation, appropriate use or completion of individual items.
Conclusion
Adjunct surgical checklists may improve context-specific patient and healthcare worker safety. Lessons from the COVID-19 pandemic may have a broad impact on improving infection prevention and control in low- and middle-income countries. 29 In health systems facing systemic challenges compounded by shortages of material resources, 30 the C19 SPC for operating rooms is an affordable solution that may aid in both the perception and the reality of healthcare worker safety as the pandemic continues to place them at risk. Furthermore, this tool and lessons from its development and implementation may inform the response to future events in the healthcare landscape.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X221092455 - Supplemental material for Perioperative provider safety in the pandemic: Development, implementation and evaluation of an adjunct COVID-19 Surgical Patient Checklist
Supplemental material, sj-pdf-1-aic-10.1177_0310057X221092455 for Perioperative provider safety in the pandemic: Development, implementation and evaluation of an adjunct COVID-19 Surgical Patient Checklist by Nichole E Starr Conceptualization Formal analysis Investigation Methodology Project administration Validation Writing – original draft Writing – review & editing Jolene N Moore Conceptualization Formal analysis Investigation Methodology Writing – review & editing Constance S Harrell Shreckengost Investigation Validation Writing – review & editing Katie Fernandez Formal analysis Investigation Project administration Writing – review & editing Reshma P Ambulkar Investigation Writing – review & editing Nina Capo-Chichi Conceptualization Investigation Methodology Validation Writing – review & editing John E Varallo Formal analysis Writing – review & editing Adesoji O Ademuyiwa Conceptualization Methodology Writing – review & editing Sophallyda Krouch Conceptualization Investigation Validation Writing – review & editing Pankaj Singh Rana Writing – review & editing JC Allen Ingabire Investigation Writing – review & editing Thomas G Weiser Conceptualization Formal analysis Investigation Methodology Writing – review & editing Tihitena Negussie Mammo Investigation Methodology Writing – review & editing Faye M Evans Conceptualization Formal analysis Investigation Methodology Writing – review & editing in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Acknowledgements
We would like to acknowledge Eliana Lillevik, Luciano Barbosa, Daniela Farchi, Dr Laila Woc-Colburn, Dr Gustavo Moraes, Suko Dwi Nugroho, Nguyen Tri Dung, Dr Rong Hu, Priya Desai and Senait Bitew for their contributions to language translations, survey distribution and data collection.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: NS received salary support during the conduct of this study from NIH Fogarty International Center (Global Health Equity Scholars NIH FIC D43TW010540).
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.