
Abstract
In patients admitted to hospital, preoperative mild cognitive impairment predicts postoperative complications. The effect of mild cognitive impairment on discharge readiness among the day stay surgery population is unknown. Our aims were to determine the incidence of impaired cognitive performance at discharge after day stay endoscopy and whether pre-existing mild cognitive impairment was associated with its development. A single-centre cohort study of elective day stay endoscopy patients was undertaken. Over a three-month period, data were collected from 69 patients aged 65 years and over. Patients were cognitively assessed on admission and discharge using the Montreal cognitive assessment tool and the three-minute diagnostic confusion assessment method. At baseline, patients who scored 1.5 or more standard deviations below age-adjusted levels on the Montreal cognitive assessment tool in conjunction with a subjective memory complaint were classified as having mild cognitive impairment. At discharge, patients were classified as having impaired cognitive performance if there was a reduction in the Montreal cognitive assessment tool score by at least two points. We also assessed delirium and subsyndromal delirium at discharge using the three-minute diagnostic confusion assessment method. We identified mild cognitive impairment in 23 patients (33.3%) on admission, and impaired performance on the Montreal cognitive assessment tool test at discharge in 35 (50.7%) patients. There was no association between mild cognitive impairment on admission and impaired cognitive performance at discharge (50.0% versus 51.1%, P = 0.94). This study demonstrates that evidence of impaired cognitive performance on the Montreal cognitive assessment tool testing is present after day stay endoscopy in over 50% of elderly patients, but this is not associated with preoperative cognitive status.
Keywords
Introduction
Previous studies have identified an incidence of postoperative cognitive decline of up to 18% of patients following endoscopy in the day surgery suite.1,2 Although this incidence may be related to persistent effects of sedative and anaesthetic agents, 3 it is possible that postoperative cognitive decline in this group of patients may be associated with pre-existing cognitive impairment. This would be consistent with previous studies which have shown that individuals with pre-existing cognitive impairment requiring hospital admission are more likely to experience cognitive complications including the development of postoperative delirium during their admission. 4
In contrast to individuals requiring hospital admission, there is little information on the association between pre-existing cognitive impairment and further cognitive impairment following day procedures. Given the growing number of procedures that are now performed as day cases, particularly endoscopies,5,6 it is important to understand the cognitive effects that may be present at the time of discharge, possibly as a result of undiagnosed preoperative cognitive impairment. This is underscored by the high prevalence of mild cognitive impairment (MCI) in the general population over 65 years, the age group which most commonly presents for day surgery in the endoscopy suite. 7 Identifying if prior cognitive impairment is a risk factor for further postoperative cognitive impairment and delirium in this group of patients would enable clinicians and patients to be better informed about the likely cognitive effects after day procedures especially in the context of same-day discharge.
MCI is defined as an impairment in cognition that is not severe enough to be classified as dementia and which does not impact daily function. It requires patients to have a subjective cognitive complaint, perform at least 1.5 standard deviations (SD) below population norms on cognitive testing and have no impairment in instrumental activities of daily living.8–10 It has been estimated to affect close to 20% of those aged 65 years and over and has been reported to be higher in those presenting to hospital.11,12 Recent retrospective work by Gaulton et al. 7 demonstrated more than 16% of individuals presenting for day surgery showed evidence of current cognitive impairment, and this rises to 51.7% in elective coronary angiography patients. 12
Subsyndromal delirium (SSD) recognises that confusional cognitive impairment is a continuum and refers to a state between delirium and normal cognition. SSD attribution requires patients to develop at least one feature of delirium, without meeting the entire criteria. 13 For patients admitted to hospital, the development of SSD has been associated with an increased length of stay, functional decline up to one year post-surgery14,15, as well as increased mortality once discharged. 16
We hypothesised that MCI on admission for day endoscopy (gastroscopy and/or colonoscopy) would be associated with a further impairment of cognition at discharge. The primary aim was to determine the incidence of impaired cognitive performance on the Montreal cognitive assessment (MoCA) tool testing following elective endoscopy and any association with preoperative cognitive impairment. Secondary aims were to identify the prevalence of MCI on admission, and the incidence of postoperative delirium, including SSD at discharge.
Methods
Patients and setting
We performed a prospective, clinical observational study between 4 March and 29 May 2019. The study was approved by the institutional ethics review board (St Vincent’s Hospital Melbourne, Human Research Ethics Committee, Australia, LRR 287/18) and written, informed consent was obtained from all participants.
Eligible patients were aged 65 years or more presenting for elective day endoscopy procedures at St Vincent’s Hospital Melbourne, Australia. A convenience sample of patients was recruited on the day of their procedure. We did not recruit patients with a prior known diagnosis of cognitive impairment, neurological disease (e.g. Parkinson’s disease), previous neurovascular disease (e.g. stroke or transient ischaemic attack) or anticipated difficulty completing neuropsychological assessment (such as English not being the primary language, blindness or deafness). On recruitment, patient demographic information, including relevant medical history, was collected on a case report form (CRF). The following were recorded: age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) physical status, a history of diabetes mellitus, hypertension, hypercholesterolaemia, peripheral vascular disease, previous myocardial infarction, smoking status, previous general anaesthesia, educational level as both number of years completed and completion of post-school training. No variables were collected for consideration of the effects of prolonged fasting, dehydration or bowel preparation on the results.
Neuropsychological testing
All study participants completed two neuropsychological screening tests (for cognition and delirium) administered by a trained interviewer both before and after their endoscopic procedures. Testing after the endoscopic procedure occurred once a patient had been deemed fit for discharge using existing hospital discharge criteria by post-anaesthesia care unit (PACU) nurses who were unaware of which patients were included in the trial.
We utilised the MoCA 17 for cognitive screening and the three-minute diagnostic confusion assessment method (3D-CAM) 18 for delirium screening. These tests were selected because of their high inter-rater reliability as well as high sensitivity for identifying MCI and delirium, respectively. Two different versions of the MoCA (v7.1 and v7.2) were used at the different timepoints to minimise any learning effect. In order to ascertain subjective impairment prior to endoscopy (to identify MCI), patients or an informant (partner, accompanying person), were asked to report any subjective memory complaint through a series of four questions. These were: (a) Do you have any difficulty with your memory? (yes/no); (b) Do you feel that your memory is worse than it should be for your age? (yes/no); (c) Do you feel that your memory has changed recently? (yes/no); (d) Has anyone mentioned to you that your memory has changed? (yes/no).
Visual analogue scales were also utilised to determine whether anxiety or depression were present at the time of testing and whether these were associated with poorer test performance. Patients were asked to mark an ungraded line (10 cm in length) anchored by 0 and 100 at either end. This is a simple, reliable and validated technique used for measuring the current state of anxiety and depression. 19
Patients were classified as having MCI if they maintained independence in daily function, they or their informant reported a subjective memory complaint and performed at least 1.5 SD below published population norms on the baseline MoCA.8–10 Patients were classified as having impaired cognitive performance on MoCA testing if their MoCA score declined by at least two points at discharge compared to admission, even if this score remained within the normal range. Impaired cognitive performance is defined in this study as a decline by at least two points on the MoCA at discharge. This threshold was chosen in line with the study by Krishnan et al., 20 which demonstrated the significance of a decline of two or more points in patients developing MCI as well as allowing for normal variation in performance from one test to another. Impaired cognitive performance is not a diagnostic entity, and it is possible for individuals to be classified as having experienced a reduction in their MoCA score by at least two points at discharge and not meet the criteria for MCI. The outcomes of impaired cognitive performance on MoCA testing and MCI were dichotomised for analysis in accordance with consensus guidelines in order to identify individuals at risk of cognitive side-effects at discharge, rather than average change within a group. 21
Patients were also screened for delirium using the 3D-CAM tool. In order to be classified as having delirium, patients were required to have features of an acute onset or fluctuating course with inattention as well as at least one of disorganised thinking or altered consciousness state. 22 Patients were classified as having developed SSD if they developed one or more features of delirium at discharge when compared to their baseline assessment but did not meet the criteria for delirium. 13
Clinical management
All clinical care followed routine clinical practice. No restrictions were placed on the endoscopist or the anaesthetist who were both unaware of patients’ recruitment and test outcomes. Procedural sedation involved a combination of propofol, midazolam and fentanyl at the anaesthetist’s discretion. Intra-operative hypotension was treated with vasopressor agents as clinically appropriate. All patients received supplemental oxygen via a Hudson mask or via high-flow nasal oxygen. Key clinical variables were documented in the CRF. Post-procedural care and evaluation for discharge readiness by standard criteria were completed by trained PACU nurses who were also blinded to baseline test results.
Outcomes
The primary outcome was impaired cognitive performance after the procedure, defined as a decrease of at least two points in the MoCA score at the time of discharge compared to their baseline score. Patients with incomplete cognitive testing at discharge were excluded from analysis. An association of impaired cognitive performance with preoperative cognitive impairment (defined by preoperative MCI) was also a primary outcome.
After the procedure, delirium and SSD were also identified using the 3D-CAM.
Statistical analyses
It was planned to recruit a sample of over 75 patients which would be likely to provide over 20 patients with MCI for subsequent comparisons. 12 Group comparisons were made using independent t-tests for continuous variables and chi-square or Fisher’s exact test for dichotomous data. Spearman’s correlation to determine relationships with two continuous variables was also used. Paired t-tests were used to compare baseline and discharge neuropsychological data. All hypothesis testing was two-tailed. A P value of less than 0.05 was considered significant. Associations were determined using univariable logistic regression analysis; 95% confidence intervals (CIs) were also determined. Tests were performed using STATA (version 12.0; Stata Corporation, College Station, TX, USA).
Results
Over the study period of three months, 814 patients were screened. We identified 167 eligible patients and approached a convenience sample of 95 patients. Of these, 73 agreed to participate, four of whom were lost to follow-up (Figure 1). A total of 69 patients were assessed on discharge.
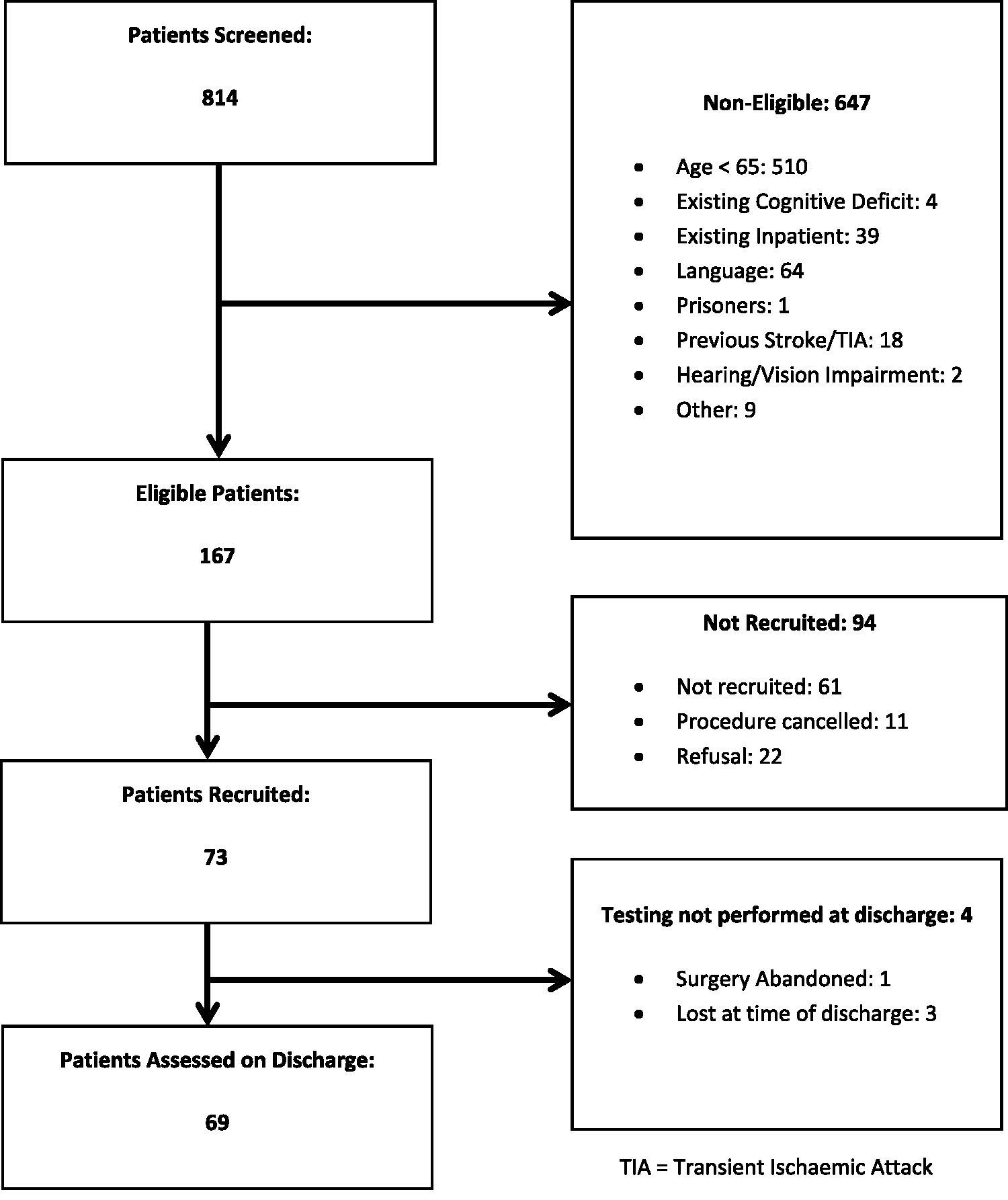
Study flow chart.
On admission, MCI was identified in 31.5% (23/73) of patients. The patients’ baseline characteristics and relevant medical history are shown in Table 1 for descriptive purposes.
Descriptive characteristics and demographic data for patients presenting for elective endoscopy with and without mild cognitive imparment.
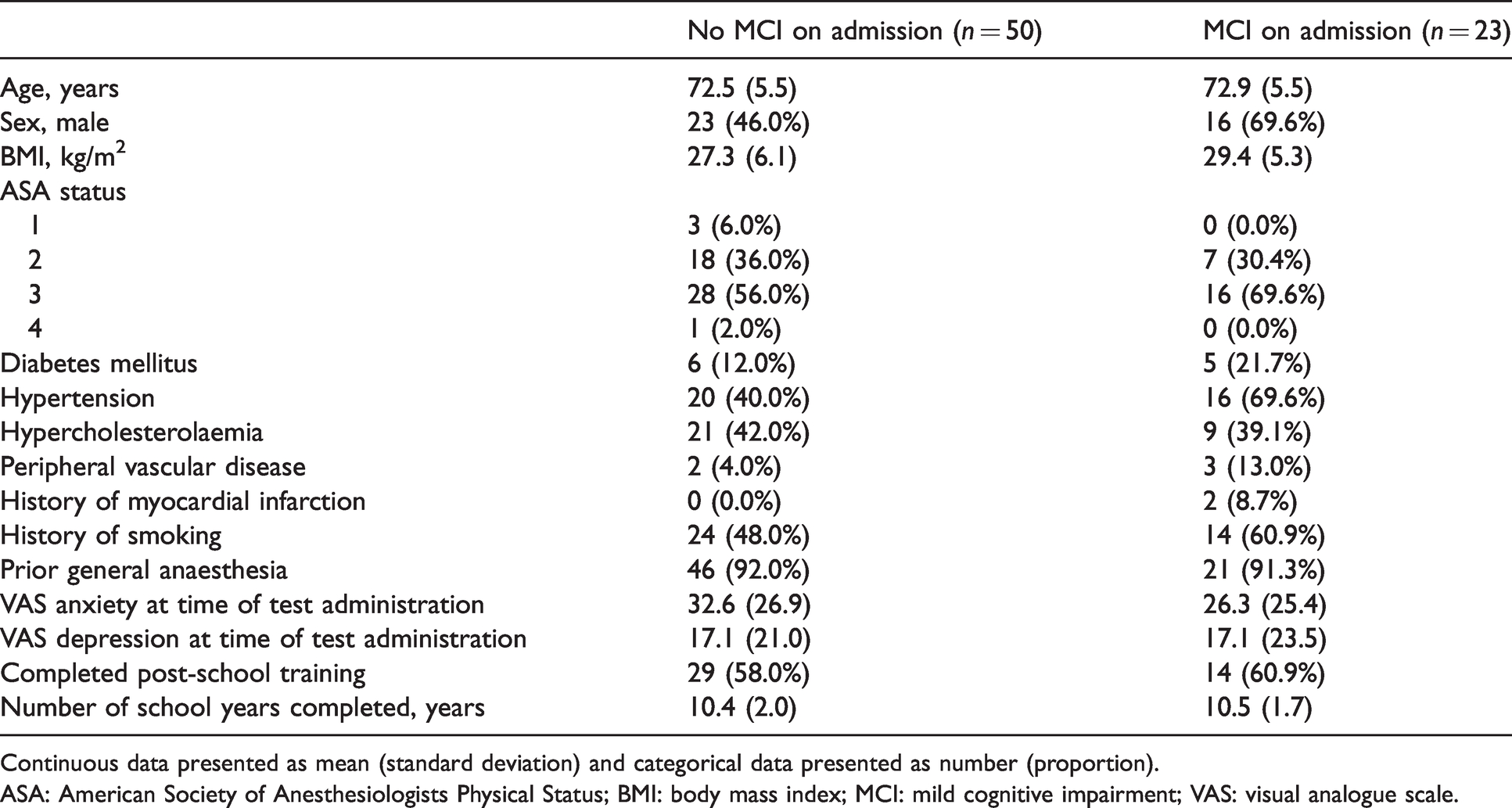
Continuous data presented as mean (standard deviation) and categorical data presented as number (proportion).
ASA: American Society of Anesthesiologists Physical Status; BMI: body mass index; MCI: mild cognitive impairment; VAS: visual analogue scale.
Those with MCI on admission had a mean (range) MoCA score of 21.2 (16–24), while those without MCI had a mean (range) score of 24.7 (15–30). Of those 50 patients who did not have MCI on admission, 24 still reported a subjective memory complaint without the objective criteria required for classification as MCI.
Propofol was used in all 69 patients with 17 (24.6%) also receiving intravenous (IV) fentanyl, four (5.8%) receiving IV midazolam and 20 (30.0%) receiving both IV midazolam and fentanyl. The mean (standard deviation; SD) duration of anaesthesia was 28.2 (18.5) minutes, and the mean (SD) elapsed time between end of procedure and testing at discharge was 76.2 (36) minutes.
Sixty-nine patients were tested at discharge. One patient had their procedure abandoned due to a seizure, while another three were unable to be tested at the time of discharge for logistical reasons. Of these four patients, only one had MCI on admission.
Cognitive status on admission and discharge is shown in Table 2. There was a small but significant decline in MoCA score at discharge from a mean (SD) of 23.8 (3.6) to 22.2 (4.0), P < 0.01. The mean reduction was by 1.6 points, within the standard deviation of MoCA scores on admission (95% CI –1.02 to –2.55). Of 69 patients, 35 (50.7%) were assessed at discharge with impaired cognitive performance on MoCA testing, defined by a decrease in MoCA score of 2 or greater. Table 3 demonstrates that 11 of these patients had MCI on admission, a prevalence of 50.0%; 24 did not have MCI on admission, an incidence of 51.1% (P = 0.93). Three patients (4.3%, 95% CI 0.1% to 12.2%) were discharged with hypoactive delirium, and 12 patients (17.4%, 95% CI 9.3% to 28.4%) were discharged with SSD. Overall, 42 patients (60.9%, 95% CI 48.4% to 72.4%) experienced a decrease of at least two points in their MoCA score at the time of discharge and or the development of new delirium, or SSD at the time of discharge. The overlap of these constructs is shown in Figure 2.
Cognitive status on admission and discharge for elective endoscopy.
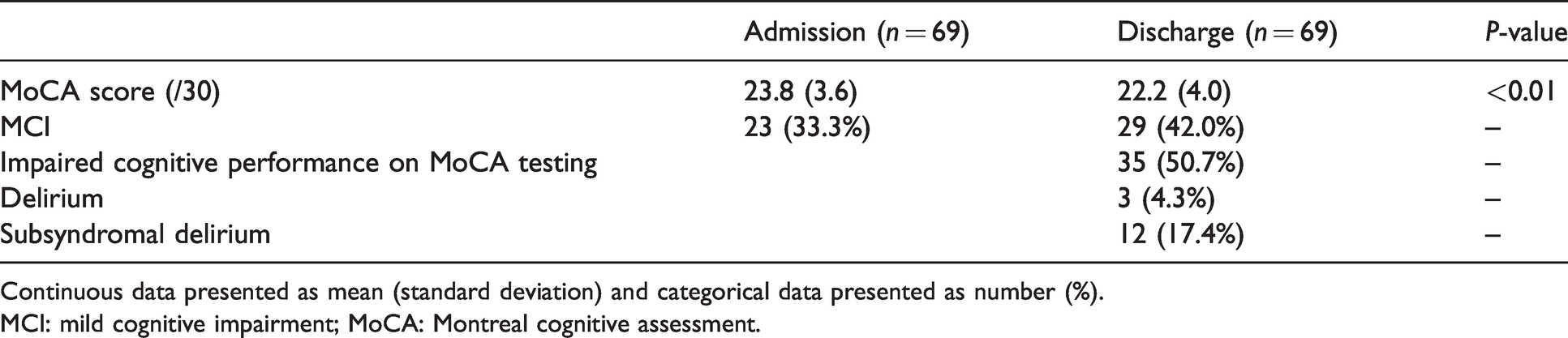
Continuous data presented as mean (standard deviation) and categorical data presented as number (%).
MCI: mild cognitive impairment; MoCA: Montreal cognitive assessment.
Cognitive effects at discharge by presence of mild cognitive impairment at admission.
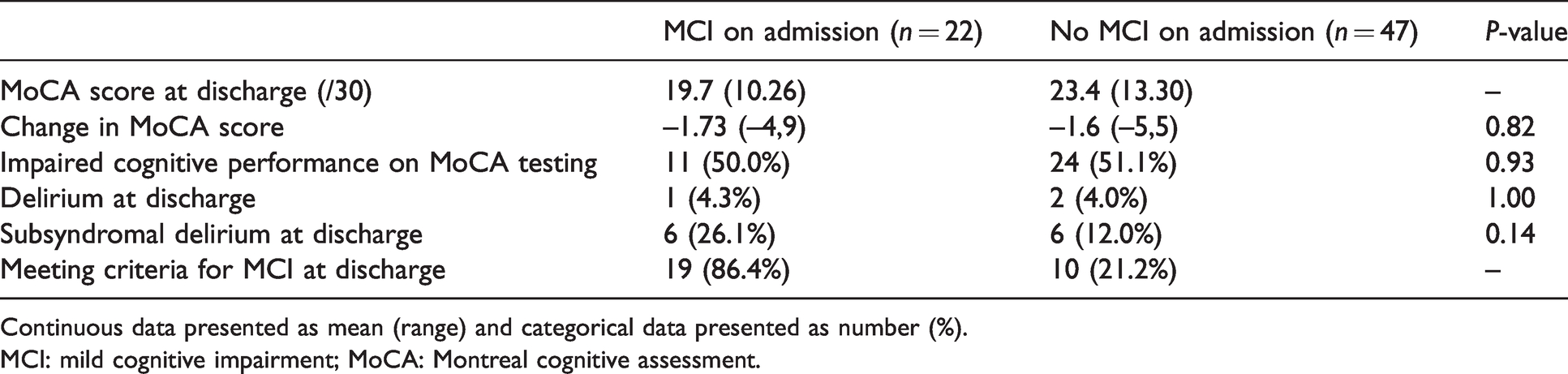
Continuous data presented as mean (range) and categorical data presented as number (%).
MCI: mild cognitive impairment; MoCA: Montreal cognitive assessment.
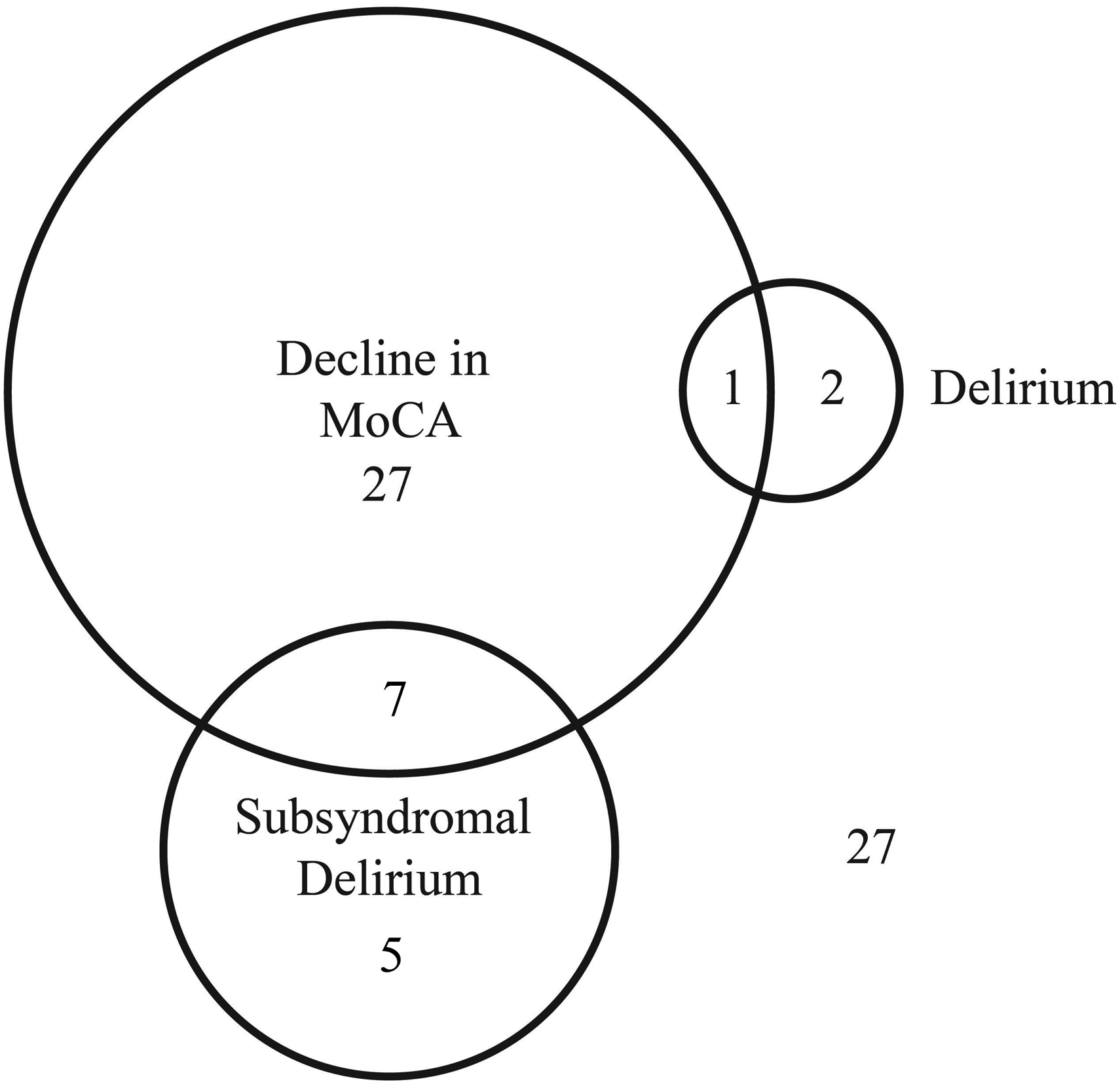
Cognition at discharge. Impaired cognitive performance on Montreal cognitive assessment (MoCA) testing was defined as a decrease in MoCA score of two or more points. Of the 69 patients assessed at discharge, 35 recorded a decrease of two or more points, three were assessed with delirium and 12 with subsyndromal delirium. The overlap between these perioperative neurocognitive disorders is shown in the Venn diagram.
There was no association between MCI on admission and impaired cognitive performance on MoCA testing at discharge. Table 3 compares the cognitive effects at discharge between those with MCI on admission and those without. Those with MCI on admission experienced a decline in MoCA score by a mean (SD) of 1.73 (3.3) points, while those without MCI on admission declined by 1.60 (2.2) points. After adjusting for multiple comparisons using the Holm–Bonferroni method there were no univariable associations observed between baseline demographic variables and any of the cognitive outcomes. The duration of the procedure as well as time spent in recovery were also not associated with cognitive outcomes. There was no significant difference in the incidence of delirium or SSD between patients with or without MCI on admission (50.0% versus 51.1%, P = 0.93).
Ten patients (21.2%) who did not have MCI on admission fulfilled the diagnostic criteria for MCI at the time of discharge when their cognitive assessment on discharge was combined with their preoperative evaluation of independence of daily functioning and subjective memory complaint. Three out of the 22 patients with MCI on admission no longer met the criteria for MCI at the time of discharge, having improved their MoCA score at discharge. In total 29 patients (42%) were discharged meeting the criteria for MCI. The overlap between these patients and those with SSD or delirium at discharge is shown in Figure 3.
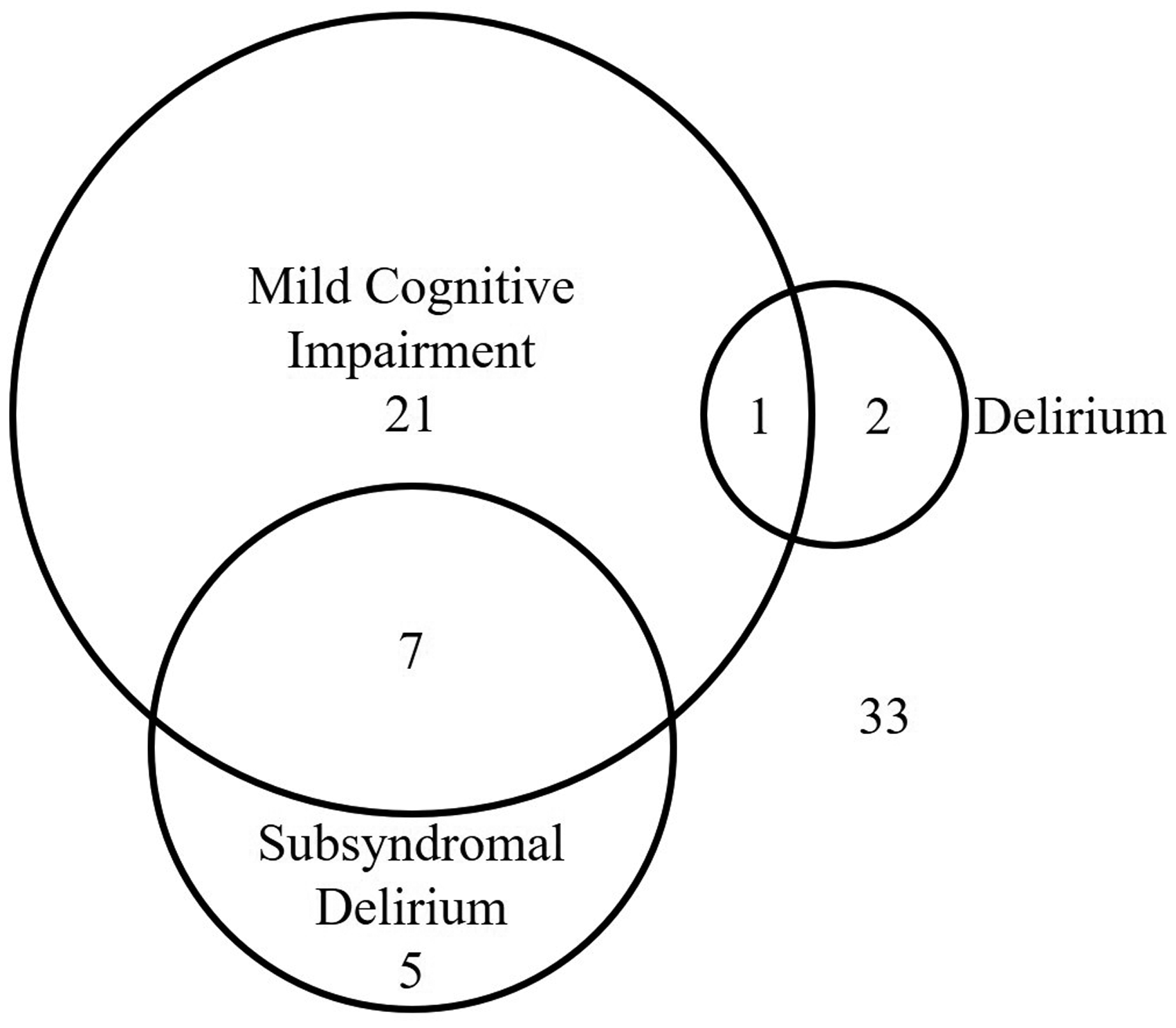
Mild cognitive impairment (MCI) at discharge. Of the 69 patients assessed at discharge, 29 fulfilled the criteria for MCI at discharge, three were assessed with delirium and 12 with subsyndromal delirium. The overlap between these perioperative neurocognitive disorders is shown in the Venn diagram.
Discussion
In patients presenting for elective endoscopy aged 65 years or older, we identified impaired cognitive performance on MoCA testing in 50.7% of our study population, as defined by a reduction in MoCA score by at least two points. Twenty-one percent of patients who did not have MCI on admission fulfilled the criteria for a diagnosis of MCI at discharge due to a decline in MoCA score together with a pre-existing memory complaint. A total of 42% of all patients met the criteria for MCI at discharge compared to 31.5% on admission.
There was no significant association between impaired cognitive performance at discharge and preoperative cognitive impairment. In addition to those with a decline in MoCA score at discharge by at least two points, we also identified delirium or SSD in a further six patients.
The fact that patients’ cognitive function is altered immediately following procedures involving anaesthesia or sedation has been anecdotally acknowledged for many years. For this reason, postoperative patients are required to be accompanied home, refrain from driving and be observed by someone for 24 hours. A previous study demonstrated early cognitive impairment following endoscopic procedures at a lower incidence of 18%, 2 compared with the 50% in this study. This difference may be explained by previous studies using different cognitive screening tools and definitions to identify an impairment in cognition 23 or it may be a type II error given the small sample size.
The significance of a MoCA score reduction by two points compared to baseline was used as this cut-off has been associated with an increased risk of future cognitive impairment in patients with stroke 24 as well as its association with the development of mild cognitive impairment. 20 In addition, other studies found that those who developed early cognitive impairment were at increased risk of developing longer-term postoperative cognitive dysfunction. 25 However, our study involved cognitive testing performed within a few hours of receiving an anaesthetic. There may be residual pharmacological effects which contribute to the decline in MoCA scores observed in this study and therefore no prognostic implications should be assumed without subsequent testing.
Nonetheless, whether temporary or permanent, the magnitude of a reduction in MoCA score by at least two points may be clinically important. There is no clear information available about how long these cognitive changes last or what implications, functional or cognitive, these changes imply. It is also unclear whether those who are discharged home with delirium improve more rapidly (perhaps due to familiarity with their surroundings) than those who remain in hospital, particularly if they are accompanied by a family member or carer. Concerningly for clinicians, it is also unknown whether the observed cognitive decline at discharge influences comprehension of discharge instructions and procedural findings conveyed to the patient. Ultimately, this study raises questions about the readiness for discharge, or the need for support, in elderly patients following endoscopy procedures.
Twenty percent of patients who did not have MCI preoperatively met the criteria for MCI at discharge, which is a potentially concerning finding. The clinical course of patients who formally develop MCI is varied, with some patients progressing to dementia, some remaining with MCI and up to 25% reverting to normal cognition at future testing.26,27 In our study, there were three patients who reverted to meet the criteria for normal cognition at the time of discharge, reflecting natural variability in test measures. It is known, however, that a diagnosis at any point in time increases the risk of progression to dementia.28,29 It may be that MCI is a clinically significant diagnosis regardless of when the diagnosis occurs; however, in the context of potential residual pharmacological effects from anaesthetic drugs, formal attribution of MCI would need to be based on testing at a later time. This finding may, however, indicate a vulnerability or decreased cognitive reserve in these patients even if not subsequently meeting the criteria for MCI.
The inclusion of delirium or SSD as secondary outcomes in day procedure cases recognises that these entities, although they have received little attention in this setting, may have important implications for longer-term cognitive outcomes, as has been shown for hospital admissions. The development of postoperative delirium in hospital is important to identify as it increases 6–12 month mortality, 25 and is associated with longer-term cognitive impairment with further functional decline requiring institutionalisation.30–32 SSD is also associated with an increased length of hospitalisation, lower functional status up to one year postoperatively,14,15 and increased mortality following discharge. 16
Given that delirium and SSD are poorly recognised in hospitals around the world 33 and are not routinely screened for on discharge, this study raises important questions about the safety of discharging elderly day stay patients and their readiness to be sent home. This study saw three patients (4.3%) discharged with delirium and 12 additional patients (17.4%) discharged with SSD who were not otherwise clinically identified outside of the study. The treating teams of the three patients with hypoactive delirium were informed of this finding prior to the patient being discharged.
The study did not identify an association between cognitive status on admission and impaired cognitive performance on MoCA testing at discharge. This ran contrary to our hypothesis that MCI at baseline would be associated with a greater incidence of impaired cognitive performance at the time of discharge. This may be due to the small numbers of participants (type 2 error), sampling error (via convenience sampling) or that the memory impairment observed at discharge reflects the persistent effects of sedative agents (propofol, midazolam or fentanyl) seen in all patients regardless of preoperative cognitive status. This effect has previously been identified. 34
It should be noted that this study was a pragmatic design focused on real life administration of day case anaesthesia and was not designed to discriminate between individual clinical practices. However, a previous randomised controlled trial by Padmanabhan et al. 2 found that the development of impaired cognition at discharge was not significantly different between those who received propofol sedation alone compared to those who received either fentanyl or midazolam as adjuvants.
Conclusions
Impaired cognitive performance on MoCA testing is highly prevalent in patients over 65 years of age following day case endoscopy. We observed a reduction in the MoCA score of at least two points in 50.7% of patients at discharge and an additional 8.7% were discharged with delirium or SSD. MCI on admission, although common, was not associated with an increased incidence of impaired cognitive performance as defined by a reduction in MoCA score of at least two points. Twenty percent of patients who did not have MCI on admission were discharged meeting the criteria for MCI. Due to a small sample size, these results should be viewed as exploratory and hypothesis generating. This result raises questions about the importance of routinely evaluating the cognitive readiness for discharge by screening for subtle cognitive effects that are otherwise difficult to identify during routine interactions and may impact longer-term outcomes. Further research is required into determining the longer-term significance of these results as well as the safety implications for patients in the short term who are discharged with impaired cognition following day case surgery.
Footnotes
Acknowledgements
The authors would like to thank research assistants Emily Fitzgerald and Erika Fortunato (Department of Anaesthesia and Acute Pain Medicine, St Vincent’s Hospital Melbourne, Australia), for their assistance in completing this study.
The study was completed under the University of Melbourne, Doctor of Medicine Research Project Program.
Declaration of conflicting interests
The author(s) have no conflicts of interest to declare.
Funding
The research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.