
Abstract
Clinicians assessing cardiac risk as part of a comprehensive consultation before surgery can use an expanding set of tools, including predictive risk calculators, cardiac stress tests and measuring serum natriuretic peptides. The optimal assessment strategy is unclear, with conflicting international guidelines. We investigated the prognostic accuracy of the Revised Cardiac Risk Index for risk stratification and cardiac outcomes in patients undergoing elective non-cardiac surgery in a contemporary Australian cohort.
We audited the records for 1465 consecutive patients 45 years and older presenting to the perioperative clinic for elective non-cardiac surgery in our tertiary hospital. We calculated individual Revised Cardiac Risk Index scores and documented any use of preoperative cardiac tests. The primary outcome was any major adverse cardiac events within 30 days of surgery, including myocardial infarction, pulmonary oedema, complete heart block or cardiac death.
Myocardial perfusion imaging was the most common preoperative stress test (4.2%, 61/1465). There was no routine investigation of natriuretic peptide levels for cardiac risk assessment before surgery. Major adverse cardiac events occurred in 1.3% (18/1366) of patients who had surgery. The Revised Cardiac Risk Index score had modest prognostic accuracy for major cardiac complications, area under receiver operator curve 0.73, 95% confidence interval 0.60 to 0.86. Stratifying major adverse cardiac events by the Revised Cardiac Risk Index scores 0, 1, 2 and 3 or greater corresponded to event rates of 0.6% (4/683), 0.8% (4/488), 4.1% (6/145) and 8.0% (4/50), respectively.
The Revised Cardiac Risk Index had only modest predictive value in our single-centre experience. Patients with a revised cardiac risk index score of 2 or more had an elevated risk of early cardiac complications after elective non-cardiac surgery.
Introduction
Over two million Australians each year undergo elective non-cardiac surgery. 1 There is a considerable risk of cardiac complications after surgery which remains a significant cause of postoperative mortality. 2 , 3 Accurate cardiac risk assessment is a part of the comprehensive consultation when individuals consider elective surgery. Clinicians commit substantial effort to improve risk assessment, while no population-based prophylactic interventions have been shown to reduce perioperative cardiac morbidity and mortality.4–7
Clinicians have an expanding set of tools to assess cardiac risk before surgery, including risk calculators, 8 , 9 non-invasive imaging, cardiac stress testing (CST) and, more recently, blood testing for natriuretic peptides (NPs).10–12 The optimal risk assessment practice is unclear, but the clinician must consider prognostic accuracy, patient acceptability, the timing of investigations, and healthcare costs. The 2016 Canadian Cardiovascular Society guidelines 13 recommend cardiac risk stratification with the Revised Cardiac Risk Index (RCRI), a risk calculator in patients 45 years and older planning elective non-cardiac surgery. The Canadian guidelines diverge from their counterpart European 14 and United States 15 guidelines. Notable disagreements include the use of CST and measuring NP levels before surgery (Table 1). In the absence of Australian guidelines, we sought to audit our perioperative practice and determine if the RCRI is a useful risk calculator for our contemporary clinical practice. The utility of the RCRI is well known internationally. 16 , 17 However, our patterns of surgical intervention, patient comorbidity and healthcare system may impact its performance. We investigated the prognostic accuracy of the RCRI for cardiac risk stratification and outcomes in patients undergoing elective non-cardiac surgery in an Australian tertiary hospital.
Canadian, European and United States guidelines for preoperative cardiac risk assessment.
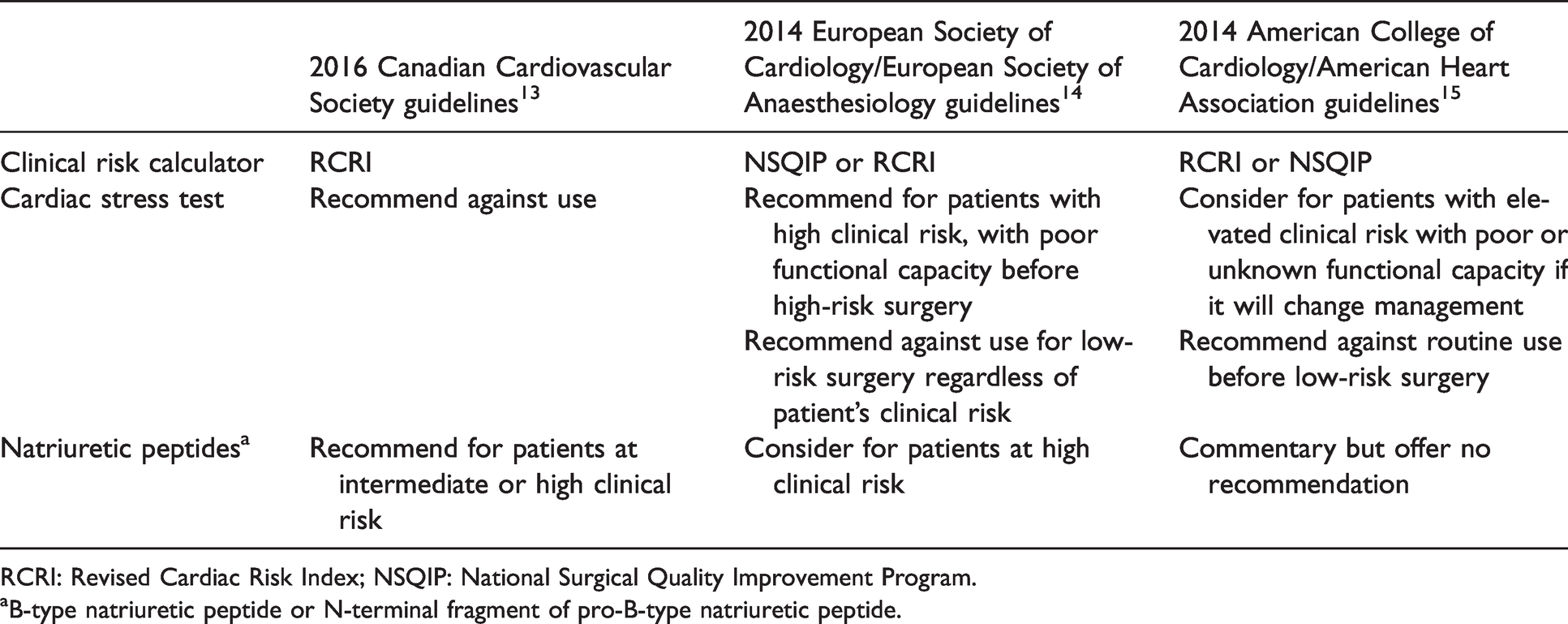
RCRI: Revised Cardiac Risk Index; NSQIP: National Surgical Quality Improvement Program.
aB-type natriuretic peptide or N-terminal fragment of pro-B-type natriuretic peptide.
Methods
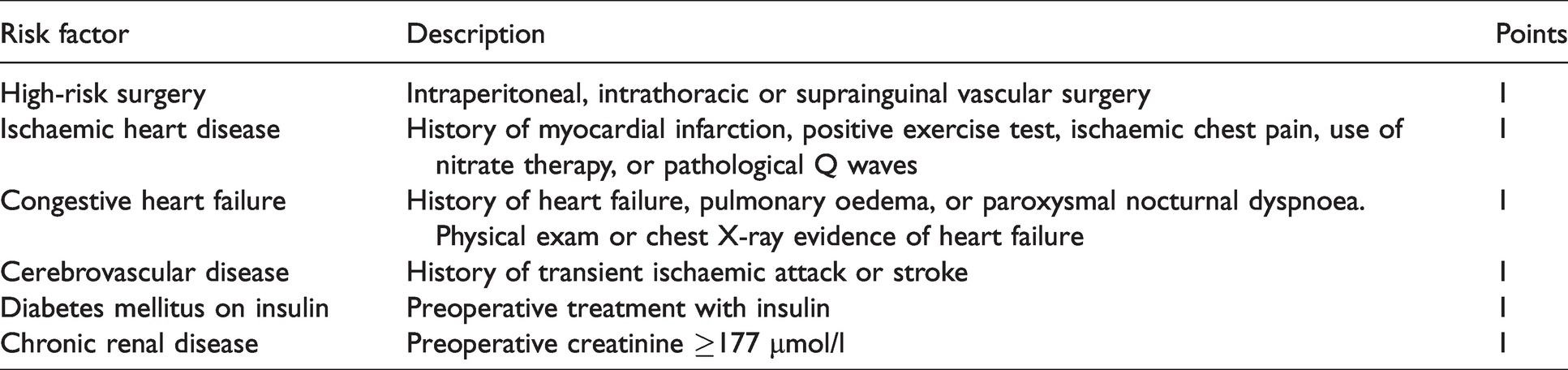
We conducted a retrospective audit of patients who attended the perioperative assessment clinic for elective non-cardiac surgery at John Hunter Hospital (JHH), Newcastle, Australia. The audit was authorised by research ethics and governance, Hunter New England local health district, authorisation number: AU201903-16. Inclusion criteria included patients 45 years of age or older planning to have elective non-cardiac surgery, and we identified consecutive patients from 1 June 2017 to 31 August 2017. Investigators reviewed Hunter New England Health (HNE) electronic records for demographics data, background medical history, type of planned surgery, American Society of Anesthesiologists (ASA) physical status classification score, perioperative medications and cardiac investigations. We reviewed individual preoperative risk factors and calculated each patient’s RCRI score, a scale between 0 and 6 (Table 2). 8
Revised Cardiac Risk Index.8
We collected the frequency of preoperative cardiac tests available to the perioperative clinic, including exercise treadmill test, stress echocardiogram, myocardial perfusion imaging, and NPs, B-type natriuretic peptide (BNP) and N-terminal fragment of proBNP (NT-proBNP).
The primary outcome was any major adverse cardiac events (MACE) within 30 days of surgery, including myocardial infarction, pulmonary oedema, complete heart block or cardiac death. We defined myocardial infarction according to the fourth universal definition (troponin rise and/or fall with at least one value above the 99th percentile upper reference limit and at least one other ischaemic feature); 18 pulmonary oedema required imaging reviewed or formally reported interstitial oedema; and complete heart block required evidence on an electrocardiogram. Cardiac death must be a direct consequence of myocardial infarction, ventricular arrhythmia, cardiac arrest, or heart failure. Secondary outcomes were the following individual outcomes: myocardial infarction, exacerbation of heart failure, and all-cause mortality up to 365 days after surgery. Exacerbation of heart failure was any hospital presentation with evidence of fluid overload requiring escalation of diuretics.
The institution’s cardiac and stroke outcomes unit identified outcomes through linkage data of HNE health electronic record coding of medical diagnosis for admission and discharge. The HNE health network includes all public hospitals and facilities in a large region of 131,785 km2 across 25 local government areas. 19 One reviewer verified outcomes identified using linkage data. A full review of each patient’s electronic records, including medical notes, troponin, 12-lead electrocardiogram and radiographs, endeavoured to capture any missed postoperative events. We followed up all abnormal troponin results to determine if they met the criteria for myocardial infarction. 18 Deaths were obtained through the Registry of Births, Deaths and Marriages records of deaths in New South Wales using a name, date of birth and postcode. In-hospital deaths were manually determined using medical notes.
Statistical analysis
Event rates with Clopper–Pearson’s 95% confidence intervals (CIs) are presented for major cardiac complications stratified by RCRI scores 0, 1, 2 or 3 or greater. We tested the association between RCRI score and major cardiac complications using the area under the receiver operator curve (AUROC) with DeLong’s 95% CI. Reference event rates with DeLong’s 95% CI were calculated from the original RCRI cohort. 8 All statistics were produced using R. 20
Results
The perioperative service reviewed a total of 1725 patients in the audit time frame. Eighty-six did not meet the eligibility criteria. We removed 174 duplicate patient records, as some patients had multiple clinic appointments in the audit period. We audited a total of 1465 unique patient medical records, with a total of 1366 patients undergoing surgery (Figure 1). Baseline demographics for patients who had surgery at JHH included a mean age of 66 years, 51.5% men, median ASA score was III, and half of our cohort had at least one RCRI risk factor (Table 3). The median time from clinic review to surgery was ten days (interquartile range 18 days, full range 0–604 days).
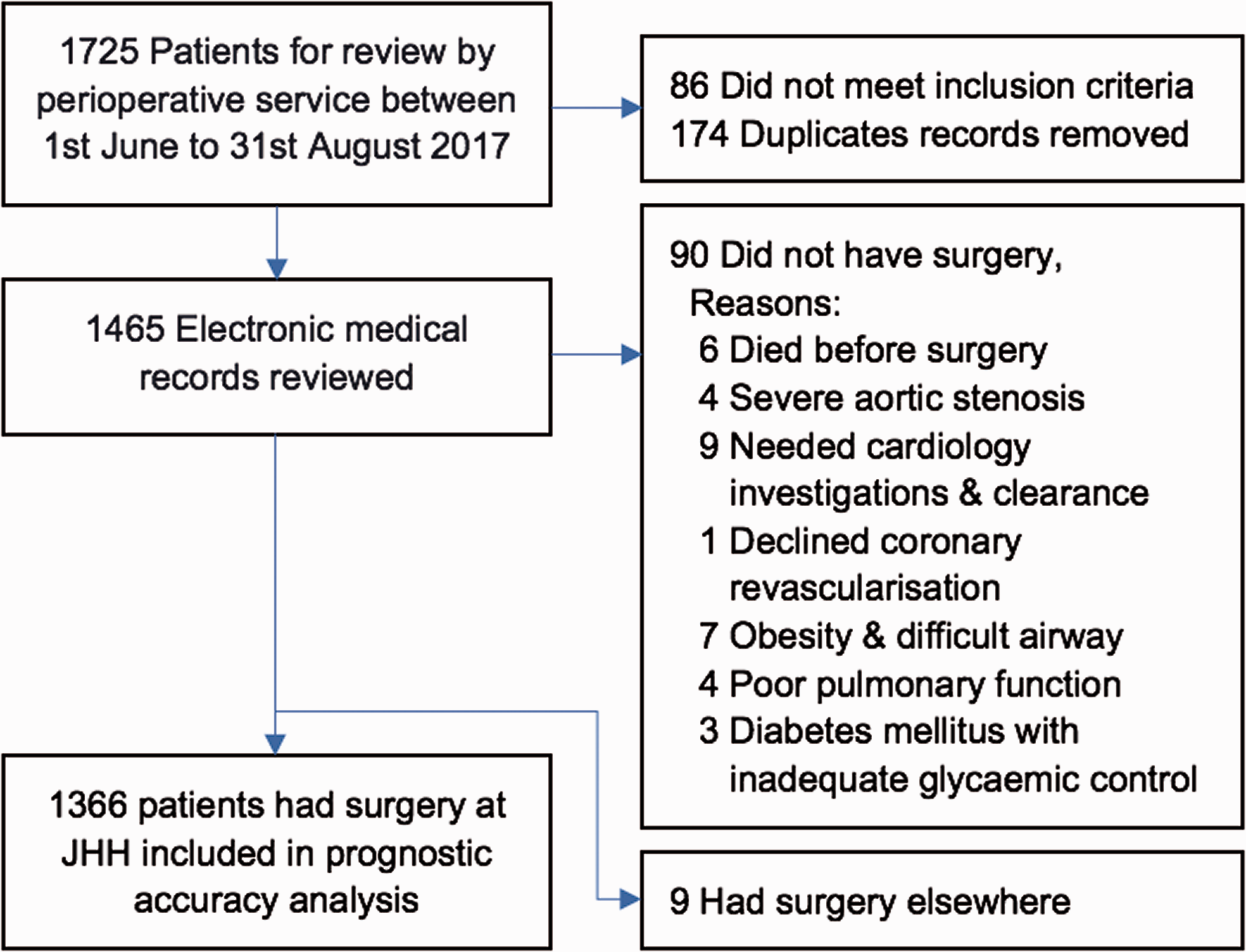
Patients considered for elective non-cardiac surgery at John Hunter Hospital.
Baseline demographics of 1366 patients reviewed in the perioperative clinic between 1 June and 31 August 2017 who subsequently underwent non-cardiac surgery at John Hunter Hospital.
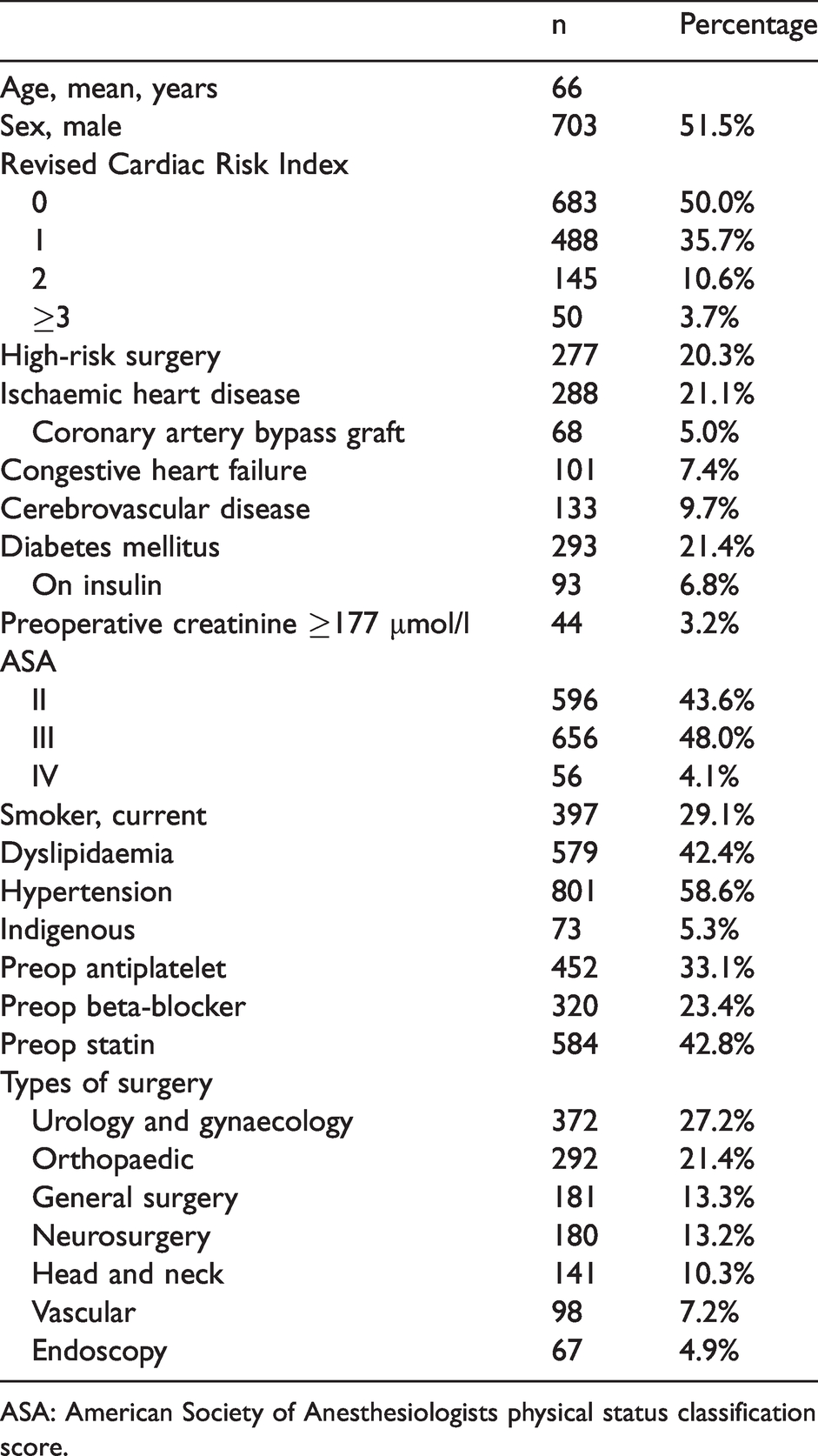
ASA: American Society of Anesthesiologists physical status classification score.
Ninety-nine (6.8%) of 1465 patients booked for review in the perioperative clinic did not undergo surgery at JHH. Six patients died before surgery, 84 patients did not have planned surgery, while nine patients had surgery at another public or private hospital. High perceived cardiac risk accounted for 14 cancellations, including four patients with severe aortic stenosis. Non-cardiac medical comorbidity contributed to 18 cancellations, seven due to morbid obesity and concerns regarding difficult airway management, four due to poor pulmonary function and three due to poorly controlled diabetes mellitus. Some patients were lost to follow-up. The most common known reason patients did not have planned surgery was unacceptable risk–benefit after consultation between the patient, anaesthetist and surgeon. Orthopaedic joint replacement and spinal surgery accounted for the highest number of cancellations.
CST results available for the 1465 patients reviewed in the clinic included: 27 (1.9%) exercise treadmill test; 22 (1.5%) stress echocardiogram; and 61 (4.2%) myocardial perfusion imaging. There was no routine investigation of serum BNP or NT-proBNP levels for cardiac risk assessment before surgery.
Postoperative outcome
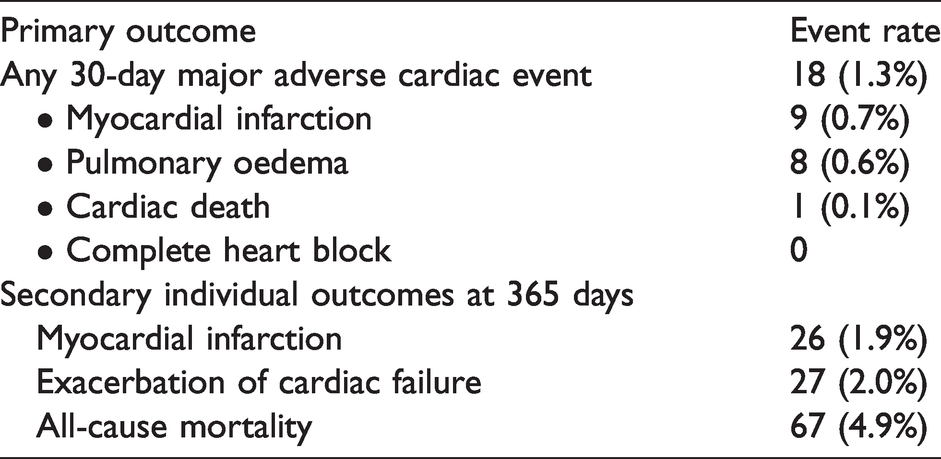
The primary outcome, MACE, occurred in 18 (1.3%) of 1366 patients within 30 days of surgery (Table 4). Secondary outcomes are individually reported outcomes within 365 days of surgery. In this period, 26 (1.9%) patients had a myocardial infarction, of which five were ST-elevation myocardial infarction, with two patients dying before reperfusion therapy. Twenty-seven (2.0%) patients had a hospital presentation with exacerbation of cardiac failure requiring escalation of diuretics. Sixty-seven (4.9%) patients had died within 365 days of surgery; over half had active cancer or were receiving palliative care.
Postoperative outcomes of 1366 patients who underwent elective non-cardiac surgery at John Hunter Hospital.
Prognostic accuracy of Revised Cardiac Risk Index
The RCRI score had a modest ability to predict for the primary outcome, any major cardiac complication within 30 days of surgery (AUROC 0.73, 95% CI 0.60 to 0.86). Event rates stratified by RCRI scores 0, 1, 2 and 3 or greater were 4/683 (0.6%, CI 0.2% to 1.5%), 4/488 (0.8%, CI 0.2% to 2.1%), 6/145 (4.1%, CI 1.5% to 8.8%) and 4/50 (8.0%, 2.2% to 19.2%), respectively (Table 5).
Major adverse cardiac events by Revised Cardiac Risk Index score.
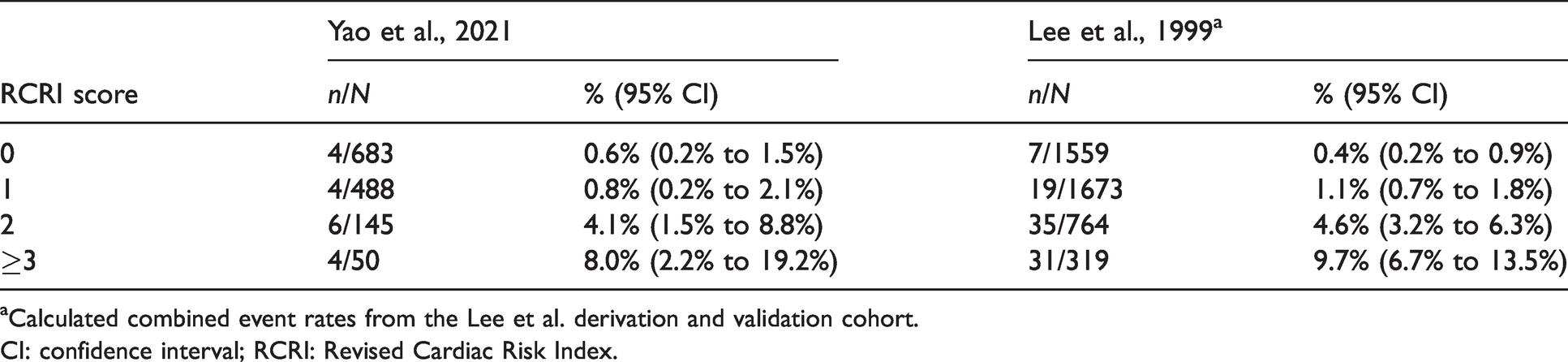
aCalculated combined event rates from the Lee et al. derivation and validation cohort.
CI: confidence interval; RCRI: Revised Cardiac Risk Index.
Discussion
In our contemporary cohort of patients undergoing elective non-cardiac surgery, we found the RCRI had only modest prognostic accuracy for MACE. Patients in our cohort with an RCRI score of 2 or greater had a significantly increased risk of perioperative MACE. Event rates within each RCRI score category were similar in our cohort compared to the original cohort described by Lee et al. 8 Several differences in our cohort may result in a lower overall cardiac risk compared to other published cohorts. 8 , 16 , 17 We included low-risk day-only surgeries while other cohorts excluded patients with an expected length of stay in hospital of less than two days. 8 However, referral to the preoperative clinic for assessment is at the discretion of the referring surgeon, such that patients perceived to be at very low risk may not have attended our clinic for assessment. Patients referred to our clinic represent a small proportion of the total institutional surgical volume. In this context, the prognostic value of the RCRI may not apply to other higher risk populations. No preoperative cardiac risk calculator is highly accurate in predicting postoperative cardiac events. 9 We chose the RCRI over other risk calculators 9 because of its ease of use, general applicability and validation in published research. 16
CST such as stress echocardiography or nuclear scintigraphy imaging can be used to document perioperative risk. 21 , 22 However, the net benefit of CST above RCRI is unknown. 13 A small subgroup of our cohort had CST, and we could not make a meaningful comparison with the RCRI.
The METS trial 23 compared four risk assessment methods before non-cardiac surgery: subjective reported functional capacity; cardiopulmonary exercise test (CPET); Duke activity status index (DASI); and NT-proBNP. A baseline predictive model including age, sex and RCRI were compared against these four methods. Only DASI, a self-reported 12-item questionnaire of daily function, improved the predictive model for 30-day myocardial infarction or death, but it failed to improve risk classification. Both DASI and NT-proBNP improved the predictive model for the broader outcome of 30-day myocardial injury or death. Low peak oxygen consumption on CPET, a heart-lung capacity test, did not improve cardiac risk prediction but was associated with overall moderate to severe in-hospital complications. This trial had reduced statistical power due to lower than anticipated event rates.
BNP and NT-proBNP can improve cardiac risk assessment. 10 Elevated preoperative NPs are independent predictors for adverse cardiovascular events after surgery.10–12, 24 , 25 An individual patient meta-analysis found NPs had value beyond RCRI for predicting non-fatal myocardial infarction and cardiovascular death after vascular surgery. 11 NT-proBNP offers a unique approach to assess cardiac risk through different biological mechanisms compared to functional capacity (CPET or DASI). 23 While RCRI risk factors are static, NPs are dynamic markers of cardiac stress with a biological gradient. Increasing concentrations of NPs are associated with a proportionally greater risk of cardiac complications after surgery. 11 , 12 The 2016 Canadian Cardiovascular Society guidelines strongly recommend measuring NPs before surgery in patients aged 65 years or older, 45–64 years with known cardiac disease, or patients with an RCRI score of 1 or greater. 13 There was low utilisation of NPs in our single-centre experience, reflecting that NPs are not reimbursed in Australia for cardiac risk assessment before surgery. Patients wanting this blood test could pay an out-of-pocket fee to have it done privately. Measuring BNP or NT-proBNP levels as a part of comprehensive cardiac risk assessment in patients at elevated clinical risk may improve access for regional and rural Australians considering surgery, especially as point-of-care tests are now widely available.
The limitations of this audit include retrospective data collection and validation. Our recruitment period was short, three months, and may not have accounted for seasonal variation in elective surgery presentations. Cardiac investigations performed for perioperative risk assessment may have been to investigate new symptoms. Outcomes recorded were limited to patients presenting to a public health facility within the HNE network. We did not capture complications managed in general practice or private institutions. There was no systematic monitoring of postoperative cardiac complications.
Future research should directly compare the RCRI and CST in an elevated risk cohort to clarify any additional predictive value of CST above and beyond a clinical risk calculator. A prospective study incorporating the RCRI and NPs for cardiac risk assessment before surgery will determine if such a strategy is safe and cost-effective.
Conclusion
The RCRI had only modest predictive value for early cardiac complications after elective, non-cardiac surgery in our single-centre experience. Our patients with a RCRI score of 2 or more had an elevated risk of early cardiac complications after surgery.
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.