
Abstract
Prophylactic administration of uterotonics ensures adequate uterine contraction at elective caesarean section to prevent substantial haemorrhage. Royal College of Obstetricians and Gynaecologists guidelines advise the administration of oxytocin at 5 IU as a ‘slow bolus’ but there are variations in clinical practice. This study aimed to determine the beliefs and uterotonic usage practices at elective caesarean section by surveying anaesthetist members of the Obstetric Anaesthesia Special Interest Group in Australia and New Zealand. Questionnaires were emailed to Obstetric Anaesthesia Special Interest Group members and the response rate was 33%, with analysis of 279 completed reports. Oxytocin was the most commonly used first-line uterotonic, but extensive variation in oxytocin bolus use was identified. Thirty-eight per cent of anaesthetists routinely administered Royal College of Obstetricians and Gynaecologists guideline-recommended 5 IU, whereas 38% favoured low dose (<5 IU), 10% high dose (≥10 IU) oxytocin and 13% carbetocin (100 µg). More than 50% felt the evidence was weak for guideline-recommended 5 IU. Wide variation in the duration of oxytocin administration was also identified. Fifty-eight per cent of anaesthetists routinely gave follow-up oxytocin infusions, most commonly at 40 IU over 4 hours, but there was significant variation in the dosage (10–40 IU) and administration duration (1 hour to ≥6 hours). In conclusion, there is significant variation in oxytocin usage practices at elective caesarean section among Australian and New Zealand anaesthetists. This variation may be due to a lack of strong evidence to guide practice. This emphasises the need for high quality trials in this clinically important area.
Introduction
Postpartum haemorrhage (PPH) rates, a major source of maternal mortality, are on the increase worldwide.1,2 Uterine atony is consistently recognised as the most common cause of PPH.3,4 Failure of the uterine smooth muscle to contract around the spiral blood vessels which feed into the site where the placenta was attached promotes bleeding and can lead to rapid blood loss. 5 Royal College of Obstetricians and Gynaecologists (RCOG) guidelines therefore recommend the prophylactic ‘slow’ administration of 5 IU oxytocin to ensure adequate uterine contraction at elective caesarean section to prevent substantial haemorrhage.6,7
Conversely, there are wide variations in recommendations among international guidelines for first-line uterotonic usage at elective caesarean section. 6 For example, the Society of Obstetricians and Gynaecologists of Canada (SOGC) recommends that carbetocin, a long acting oxytocin analogue, should be used as the uterotonic agent of choice to prevent PPH at elective caesarean delivery. 8 On the other hand, a recent consensus guideline on the use of uterotonic agents during caesarean section recommends the administration of either oxytocin or carbetocin immediately following the delivery of the fetus at caesarean section. 9 This guideline also recommends the administration of oxytocin at a significantly lower dose (i.e. 1 IU) at elective caesarean section in comparison to other guidelines that have traditionally recommended a 5 IU bolus dose.6,9 This variation in guideline recommendations may be explained by a lack of adequately powered trials to assess the impact of first-line uterotonic agents at elective caesarean section on important maternal outcome measures such as serious maternal morbidity including hysterectomy.10,11
Taken altogether, when decisions aimed at the administration of first-line uterotonics at elective caesarean section are based on weak evidence and a diverse range of guidelines rather than using a unified, evidence-based approach, there may be a risk of considerable variation in clinical practice among obstetric anaesthetists.11,12 This variation in clinical practice may impact maternal outcomes. There has never been a survey to determine the uterotonic usage practices and beliefs of anaesthetists in the setting of elective caesarean section in Australia and New Zealand. To address this knowledge deficit we conducted a survey of anaesthetists in the region of Australia and New Zealand.
Materials and methods
Our survey was developed by modifying a previously published questionnaire of oxytocin usage at elective caesarean section among obstetric specialists (see Supplementary Appendix). 13 We did not include intrapartum caesarean sections due to their more complex nature, rendering it more difficult to interpret the consistency of practice. The survey explored uterotonic usage practices at elective caesarean section among anaesthetists that were members of the Obstetric Anaesthesia Special Interest Group (SIG) in Australia and New Zealand. This group was chosen because the anaesthetists who belong to this group have a strong interest in obstetric anaesthesia. Anaesthetists who join the special interest group can study, report and develop educational events such as continuing medical education meetings on obstetric anaesthesia. Furthermore, the SIG is jointly managed by the following professional anaesthesia bodies: the Australian and New Zealand College of Anaesthetists (ANZCA), the Australian Society of Anaesthetists and the New Zealand Society of Anaesthetists. This survey was approved by the executive committee of the Obstetric Anaesthesia SIG and the Tasmanian Health and Medical Research Ethics Committee (H0014821).
The survey was developed in electronic format through the University of Tasmania and administered via the Limesurvey software platform. The ANZCA Clinical Trials Network provided administrative support. Obstetric Anaesthesia SIG members were randomly selected from the database using a computer-generated sequence and an email was sent containing a link to the electronic survey on 25 May 2015. An email reminder to complete the survey was sent on 9 June 2015. The survey was initially piloted among anaesthetists with an interest in obstetric anaesthesia at the Royal Hobart Hospital, Tasmania, Australia. Questions surveyed the administration of uterotonics for the third stage at elective caesarean section. The questions specifically addressed: the use of oxytocin bolus, perceived strength of evidence for boluses, perceived frequency of side effects of boluses, and the use of an additional infusion of oxytocin (syntocinon). An opportunity for free-text responses was provided.
Anaesthetists were asked about the dosages of oxytocin boluses and infusions and also the rates of administration. The RCOG guideline was the only international guideline to specify an oxytocin dose at caesarean section when the survey was designed in 2015. 6 For oxytocin bolus, 5 IU was therefore regarded as the reference standard according to RCOG guidelines. 7 An oxytocin bolus dose less than 5 IU was regarded as a low dose and a dose greater or equal to 10 IU was regarded a high oxytocin dose.
Statistical analysis
Data were analysed using descriptive methods. All data were analysed using R Core Team (2013) (R: A language and environment for statistical computing, R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org/).
Results
A total of 900 surveys were sent to a random selection of members of the Obstetric Anaesthesia SIG, of which 301 responded for a response rate of 33% (Figure 1). Of these, 18 were excluded (six because they contained no data and 12 because they were completed by anaesthetists who did not practice obstetric anaesthesia). A further four surveys were excluded because only demographic data were provided, thus leaving 279 surveys for analysis.
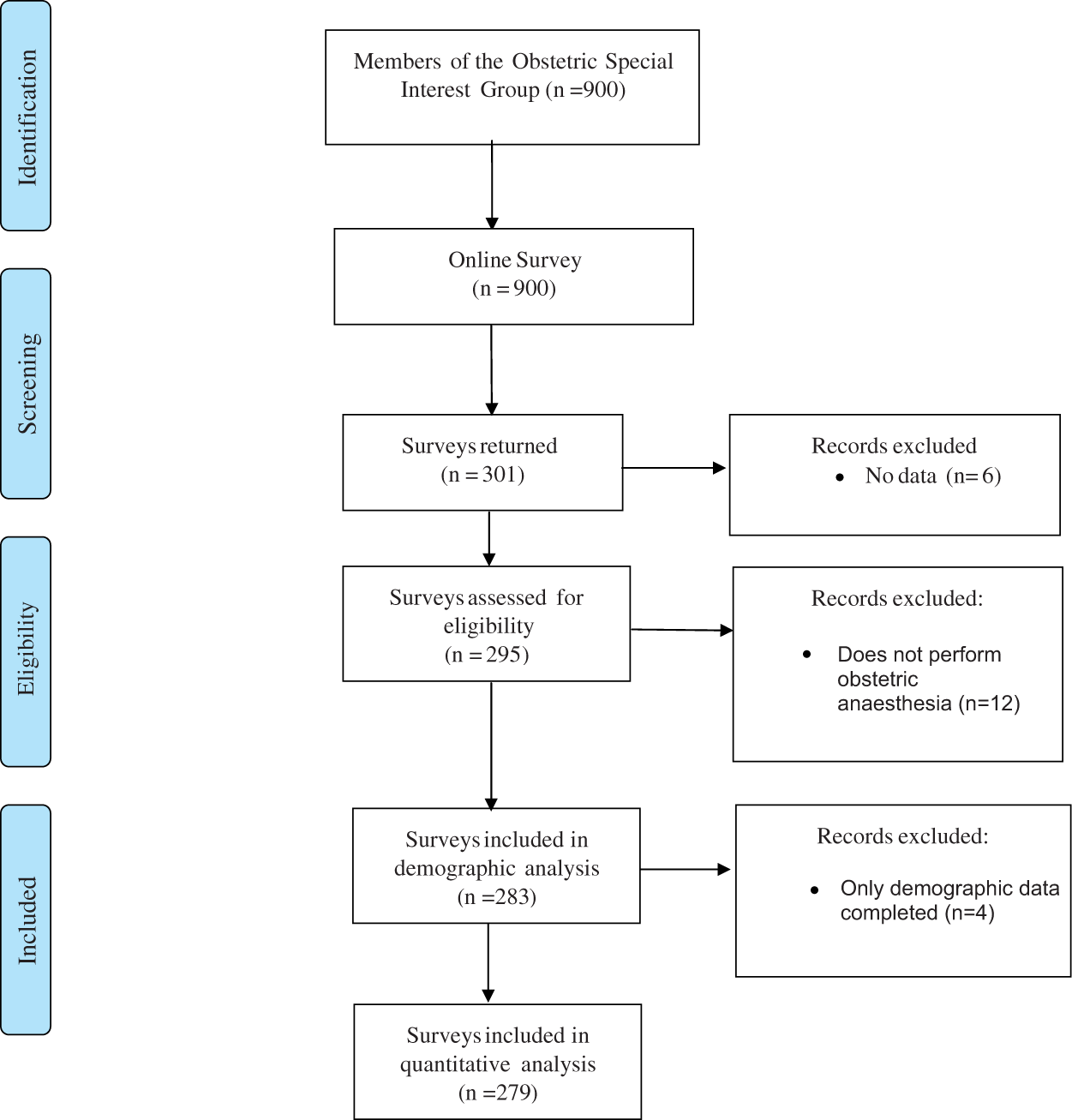
Study flow chart.
The respondent characteristics are detailed in Table 1. Of the 283 surveys with demographic data, the majority of members were more than 40 years of age, practised in a metropolitan city, had more than 10 years’ anaesthesia experience and regularly practised obstetric anaesthesia.
Baseline demographic and characteristics of survey anaesthetists.
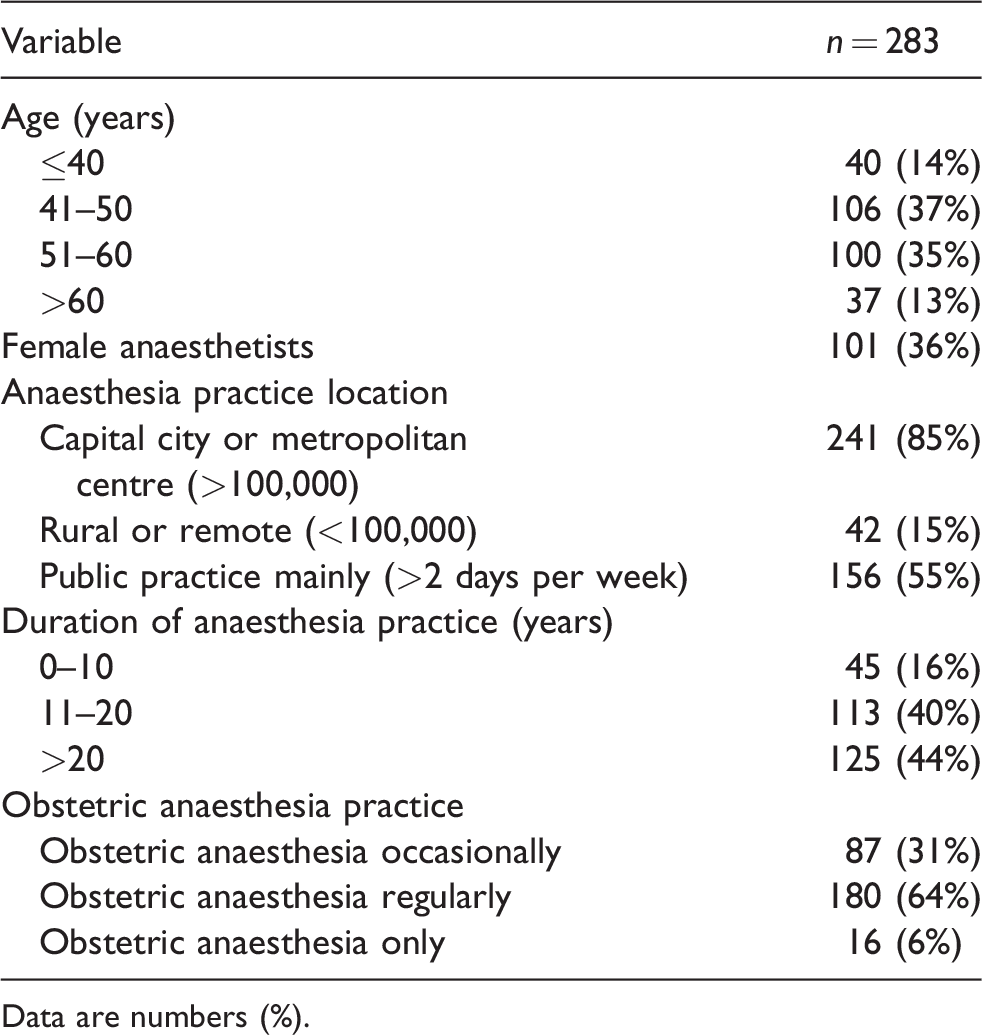
Data are numbers (%).
Use of oxytocin as a bolus dose at elective caesarean section
Thirty-eight per cent of anaesthetists routinely administered RCOG guideline-recommended 5 IU, 38% favoured low dose (<5 IU), 10% high dose (≥10 IU) oxytocin, and 13% preferred carbetocin (100 µg) (Table 2). Wide variation in the speed of oxytocin administration was observed, with the majority of anaesthetists reporting they administered oxytocin quickly, in less than 10 seconds (63%). Of the 278 anaesthetists administering oxytocin or its synthetic derivative carbetocin, only 17% would administer it over a period of at least 60 seconds.
Use of oxytocin as a bolus dose at elective caesarean section.
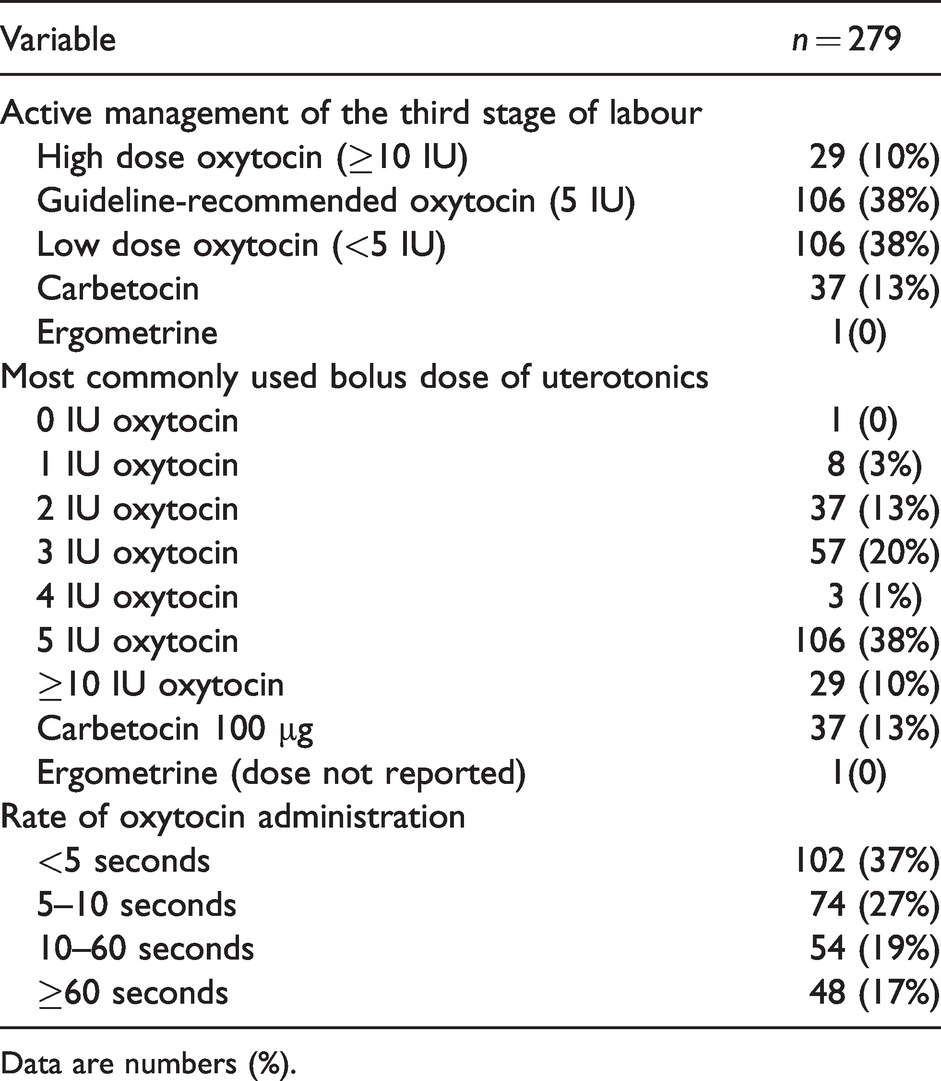
Data are numbers (%).
Anaesthetists’ perception of oxytocin bolus usage at elective caesarean section
There was wide variation in the lowest oxytocin dose that anaesthetists would consider administering at elective caesarean section (Table 3). Doses of 5 IU (24%), 3 IU (29%) and 2 IU (23%) were most frequently reported. Only 9% reported that the strength of the evidence for 5 IU oxytocin usage was strong or very strong, with the majority (54%) reporting that the evidence was weak or very weak. Two broad themes emerged from the free-text discussion on the strength of the evidence base for the bolus dose of oxytocin at elective caesarean section. First, a high number of anaesthetists (39%) expressed significant uncertainty regarding the evidence base for the oxytocin bolus dose at elective caesarean section. Conversely, a number of participants felt that there was at least some evidence to support the efficacy of lower than guideline recommended 5 IU oxytocin and that this practice would reduce the frequency of adverse events. Regarding the evidence for lower oxytocin doses, a small group of participants felt that there was sufficient evidence to support the usage of 2–3 IU to induce adequate uterine contraction. Among another small group of participants, the general consensus was that dose-finding studies showed that the effective dose for oxytocin was less than 1 IU and could be as low as 0.35 IU.
Anaesthetists’ perception of oxytocin bolus usage at elective caesarean section.
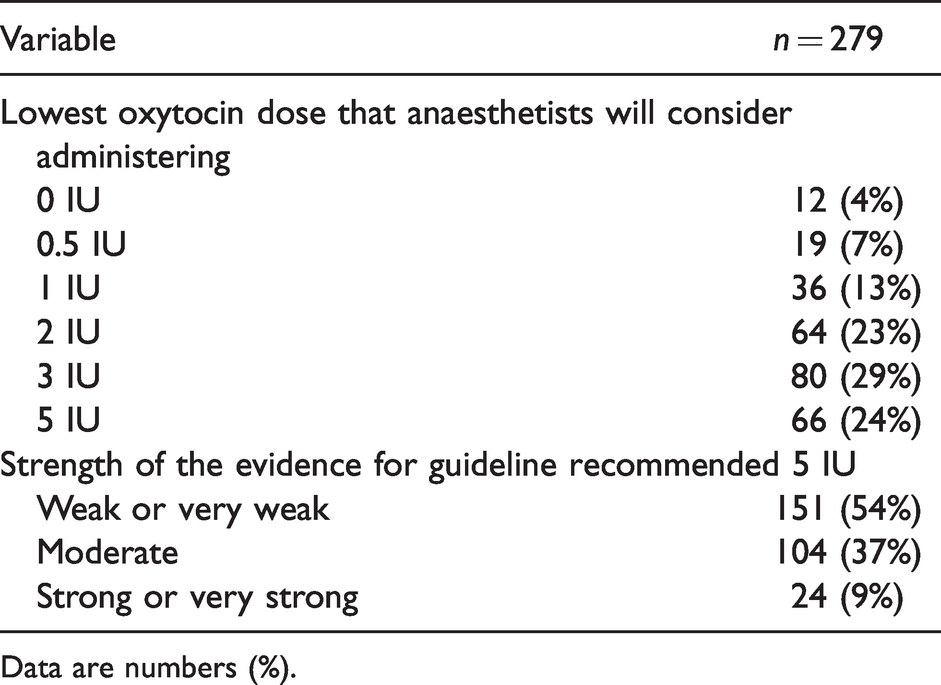
Data are numbers (%).
Use of oxytocin as an additional infusion after initial bolus administration at elective caesarean section
With regard to the use of oxytocin as an additional infusion, 58% of anaesthetists reported that they administered it routinely and 38% selectively (Table 4). It was most commonly administered over a 4-hour duration (78%).
Use of oxytocin infusion after initial bolus administration at elective caesarean section.
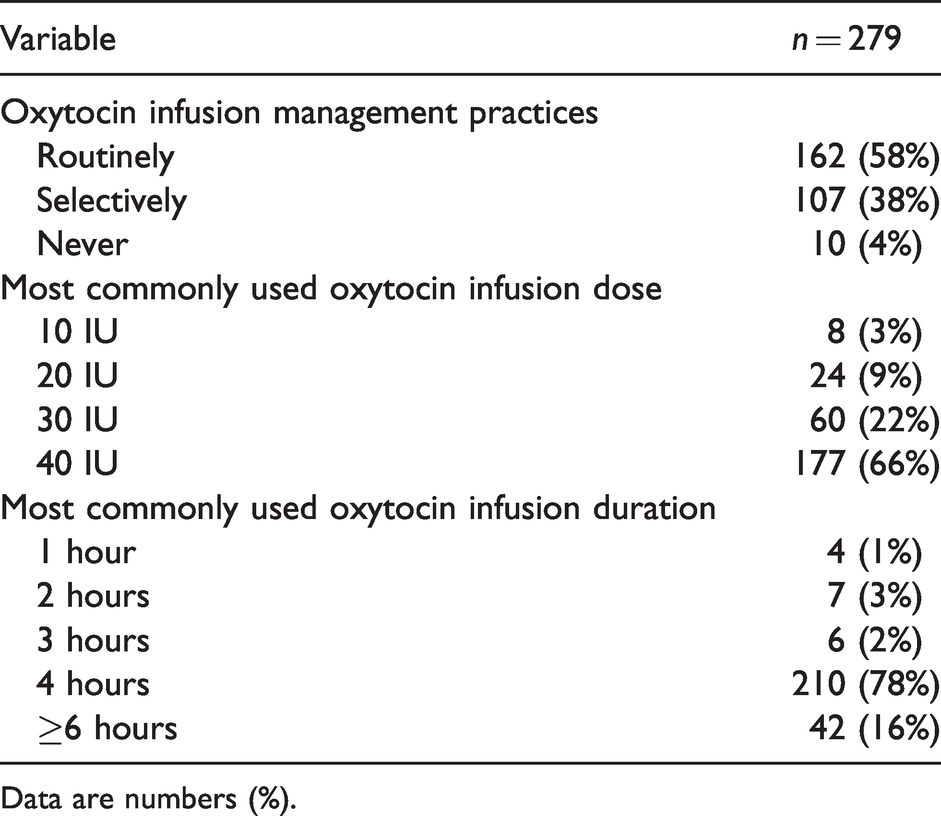
Data are numbers (%).
Perceptions on the frequency of side effects after the administration of an oxytocin bolus
There was wide variation in the perceived frequency of side effects reported by anaesthetists following bolus administration of oxytocin. (Table 5) Of all the individual side effects surveyed, only flushing (15%) and tachycardia (29%) reportedly occurred frequently, in more than 10% of women when they received an oxytocin bolus.
Anaesthetists’ perceptions of the frequency of side effects after the administration of an oxytocin bolus.
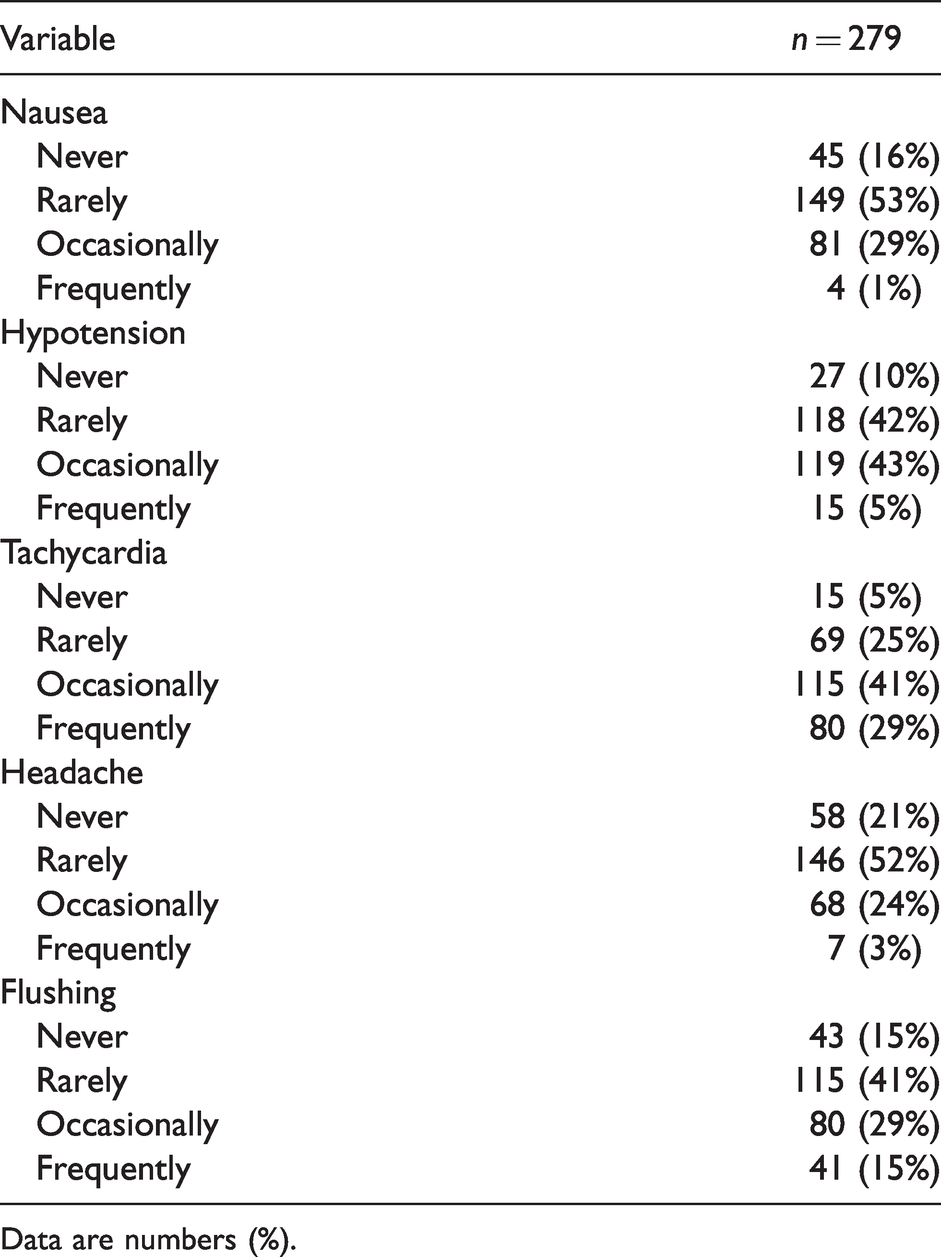
Data are numbers (%).
Discussion
This is the first survey to determine uterotonic usage practices at elective caesarean section among anaesthetists from Australia and New Zealand. This study found significant variation in uterotonic usage among anaesthetists from this region. Overall, these findings are concordant with results of international surveys that revealed extensive variation in uterotonic usage practices at caesarean section.12–15 The majority of anaesthetists indicated that they believed that the evidence was limited for RCOG guideline-recommended 5 IU oxytocin at elective caesarean section. This would suggest that there is a lack of strong evidence to guide practice, and this may be a contributory factor towards the observed variation in practice. 11
Oxytocin bolus
Founded on the principles of the active management of the third stage of labour, RCOG guidelines recommend a slow intravenous bolus dose of 5 IU of oxytocin after delivery of the infant at caesarean section. 6 The vast majority of survey participants administer oxytocin as their preferred first-line uterotonic at elective caesarean section.16,17 However, extensive variation in oxytocin bolus use was identified among survey participants in comparison to RCOG guideline recommendations. Approximately 40% administer guideline-recommended 5 IU, whereas 40% routinely administered low dose (<5 IU) and 10% a high dose (≥10 IU) oxytocin. It should be noted that the dosing requirements for oxytocin in labouring women, particularly in augmented labour, are likely to be higher. 9 Furthermore, the majority of anaesthetists reported that they administer oxytocin relatively quickly in less than 10 seconds despite RCOG guidelines recommending the administration of a ‘slow bolus’. 6 The significance of this finding for clinical practice is uncertain as it was not possible to determine the relationship between oxytocin dose and the rate of administration. This is important because the interaction between the absolute oxytocin dose and the rate of bolus administration determines the magnitude of cardiovascular changes associated with oxytocin administration. The rapid administration of a 1–2 IU oxytocin bolus may therefore be less important than the rapid administration of higher doses such as RCOG guideline-recommended 5 IU. Despite this wide variation in clinical dose and administration rate, most participants reported a low frequency of side effects. The survey also showed wide variation in the lowest oxytocin dose that an anaesthetist would consider administering at elective caesarean section, ranging between 5 IU and incrementally lower doses, including no oxytocin by one respondent. The responses in this survey may reflect that there is no real consensus on what the best approach should be and this is underpinned by a lack of effectiveness data especially for lower oxytocin doses. 11
Infusion
The majority of survey participants (58%) routinely administered an oxytocin infusion after the initial bolus dose. However, there was wide variation in the dosage (10–40 IU) and administration duration (1 hour to ≥6 hours). It is noteworthy that the consensus guideline for elective caesarean section recommends the routine administration of a low dose (2.5–7.5 IU/h) oxytocin infusion following the initial bolus. 9 This recommendation is supported by a recently reported randomised controlled trial (n=51) which showed similar efficacy in terms of uterine tone, PPH rates and the occurrence of adverse events between high rate oxytocin infusion (15 IU/h) versus low rate (2.5 IU/h) at elective caesarean delivery.
In comparison, RCOG guidelines do not advise the routine administration of an oxytocin infusion at caesarean section. 6 The guideline recommendation is supported by evidence from a large trial in 2069 women booked for elective caesarean section. 18 This multicentre, randomised, double blind, placebo controlled trial confirms that the addition of a high rate oxytocin infusion (10 IU/h) versus no oxytocin infusion, following an initial 5 IU oxytocin bolus dose, does not reduce the occurrence of major obstetric haemorrhage, defined as blood loss of 1000 ml or more. However, the addition of an oxytocin infusion resulted in a reduction in the need for additional uterotonics. 18
Overall, this dichotomy of practice (the administration of an additional oxytocin infusion or not) revealed by this survey is therefore consistent with the lack of confidence in the current evidence base. This uncertainty may be further confounded by a lack of consistency among international guidelines that may result in wide variations in clinical practice. 6
Carbetocin
A trend towards the administration of a longer acting synthetic oxytocin analogue among some anaesthetists has emerged. Carbetocin was the first-line uterotonic of choice among one in eight survey participants at a dose of 100 µg. Two guidelines support the use of carbetocin as a first-line uterotonic in elective caesarean section.6,9 Both guidelines recommend the administration of 100 µg carbetocin as a slow bolus. However, the consensus guideline by Heesen et al. goes a step further and proposes that smaller doses (as low as 20 µg) may be adequate. 9 This recommendation is concordant with several dose finding studies that have suggested that a carbetocin dose of as low as 14.8 µg is effective in producing adequate uterine contraction in 90% (ED90) of low risk non-labouring women undergoing elective caesarean section.19–21 The augmented length of action of carbetocin compared with oxytocin reduces the necessity for an oxytocin infusion after the primary dose. 9
It should be noted that the PPH outcome data supporting the effectiveness of carbetocin at caesarean section is not concordant. A Cochrane review by Su et al. updated in 2012 reported reductions in PPH rates and the requirement for further uterotonics with carbetocin administered as a 100 µg intravenous dosage across all the trials. Four of the six included trials were conducted in women undergoing caesarean section. 22 In contrast, a recent Cochrane network meta-analysis which comprised 140 randomised trials with information from 88,947 women, and reflected all combinations of prophylactic uterotonic drugs, after both vaginal and caesarean births, found no evidence to support a reduction in major PPH, defined as blood loss of 1000 ml or more, between any combination of uterotonic, including carbetocin and oxytocin alone. 17 Conversely, the absence of directly similar studies makes it challenging to make definitive inferences. The limitations of meta-analysis are increasingly acknowledged suggesting that large definitive trials of first-line uterotonics are now warranted. 23
Given the variation in uterotonic usage at elective caesarean section revealed by this survey, it is important to explore further and understand the impact of clinical variation on outcomes in healthcare. This approach is an important first step in improving patient health outcomes through applying appropriate evidence-based care. 24
Limitations
The sample was intentionally targeted towards anaesthetists of the Obstetric Anaesthesia SIG. This was undertaken because these members were more likely to administer obstetric anaesthesia regularly and thus represent an expert group of relevant practising clinicians. On the other hand, this sampling strategy could have led to an overestimation of the effect size on the basis of responders providing answers they felt were acceptable rather than those being carried out in practice (responder bias). Furthermore, the response rate was low, but not markedly different to other ANZCA-endorsed surveys of bi-national practice.25,26 The inferences made, together with potential responder bias, may therefore not generalise to all obstetric practices in Australia and New Zealand. The survey was conducted in 2015 and therefore it is possible that practices may have changed subsequently. It is possible that the responses provided in 2015 could reflect current guideline practice, but we cannot know this with certainty. Furthermore, it is possible that anaesthetists with strong opinions on the safety or efficacy of uterotonics may have been more likely to respond, and may therefore differ from anaesthetists who did not respond. Within the survey, we intentionally chose to include a gap in oxytocin dosing from 5 IU to 10 IU, because this reflects the most commonly used doses in the literature; however, this means that we may have missed anaesthetists who administered oxytocin doses between 5 IU and 10 IU. When comparing the demographics of respondents to this survey with the wider anaesthetist population there is a similar ratio of male to female anaesthetists, but our survey population had more years’ experience at giving anaesthesia and were more inclined to work in public practice. 25 Also, despite randomly selecting participants, we cannot rule out the possibility of data skewing from overrepresentation of respondents in specific health networks or jurisdictions.
Conclusions
This study found substantial variation in uterotonic usage practices at elective caesarean section among surveyed anaesthetists from Australia and New Zealand. More than three-quarters of these anaesthetists use oxytocin as their first-line uterotonic; however, there was substantial variation in the dose and rate of administration of both boluses and infusions. This variation in practice is likely to be a result of a lack of evidence and absence of standardisation among international guidelines. Large pragmatic multicentre clinical trials are now required to address the effectiveness and safety of first-line uterotonics at elective caesarean section.
Footnotes
Acknowledgements
The author(s) are grateful for the assistance from the ANZCA Clinical Trials Network, in particular Karen Goulding.
Author contribution(s)
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JES was supported by a National Health and Medical Research Council of Australia Career Development Award (reference 1045373). The remaining author(s) have no conflicts of interest to declare.
Finance
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.