
Abstract
Airway Management is the key for anaesthetists dealing with patients undergoing diagnostic procedures and surgical interventions. The present coronavirus pandemic underpins even more how important safe airway management is. It also highlights the need to apply stringent precautions to avoid infection and ongoing transmission to patients, anaesthetists and other healthcare workers (HCWs). In light of this extraordinary global situation the aim of this article is to update the reader on the varied aspects of the ever-changing tasks anaesthetists are involved in and highlight the equipment, devices and techniques that have evolved in response to changing technology and unique patient and surgical requirements.
Introduction
Airway management is the key for anaesthetists dealing with patients undergoing diagnostic procedures and surgical interventions. The present coronavirus pandemic underpins even more how important safe airway management is. 1 , 2 It also highlights the need to apply stringent precautions to avoid infection and ongoing transmission to patients, anaesthetists and other healthcare workers.
In light of this extraordinary global situation the aim of this article is to update the reader on the varied aspects of the ever-changing tasks anaesthetists are involved in and highlight the equipment, devices and techniques that have evolved in response to changing technology and unique patient and surgical requirements.
This is a collaborative effort by the executive members of the Australian and New Zealand Airway Management Special Interest Group (SIG). Each airway expert provided one or more updates in improving specific aspects of airway management based on their expertise or area of interest. All board members subsequently critically reviewed the article and adjusted the text where needed. All executive members of the Anaesthesia Continuing Education (ACE) Airway Management SIG subsequently endorsed the end result of the article. The authors hope this article provides the readers with an up-to-date synopsis of various airway topics in an attempt to improve patient care. It is the intention of the SIG to provide these reviews biennially.
Rapid growth of scientific publications on management of the difficult airway
The growth of scientific publications on the ‘difficult airway’ has dramatically increased in the past 20 years, dominating the anaesthetic literature and other research topics in anaesthesia. 3
The majority of anaesthesia innovation in the past 30 years impacts on different aspects of airway management, including:
monitoring: pulse oximetry, capnography, cuff pressure monitoring devices; drugs: inhalational agents, induction agents and other anaesthetic drugs; ventilators: ventilatory modes and non-invasive ventilation; airway devices: second generation supraglottic airway devices (SADs) and tracheal tubes.
Advanced airway adjuncts have proliferated, including fibreoptic scopes, the Aintree intubating catheter (AIC; Cook Medica, Bloomington, IN, USA) and ultrasound imaging. High-flow nasal oxygen (HFNO) allows us to prolong the safe apnoeic time while new videolaryngoscopes have improved the safety of intubation.
With such a large array of airway equipment at our disposal, it is essential that anaesthetists are informed about all aspects of modern airway management and understand the existing equipment, so that the most optimal technique can be applied to offer the best service to our patients.
Recent developments in Australia and New Zealand
Airway leads: Australia
The concept of airway leads was generated following recommendations and findings of the Fourth National Audit Project (NAP4) in the UK. 4 The aim of this initiative is to establish a network of practitioners to assist and to improve overall anaesthetic airway management. Airway leads were introduced in New Zealand in 2018 and subsequently in Australia in 2019. Local airway leads in Australia are supported by a state airway lead who is a nominated executive member of the Airway Management SIG. The role of the airway lead is not proscriptive and allows for variation and flexibility of practice according to local requirements.
Airway leads are involved and encouraged to facilitate a range of activities, including:
local airway management training; establishing local policies for airway management; ensuring appropriate difficult airway equipment is available and actively engaging with procurement; liaising with the intensive care unit and emergency departments; overseeing airway management audits and investigating adverse outcomes.
International airway management audits, including the American Society of Anesthesiologists closed claims projects in 1990, 2005 and 2012, 5 , 6 the NHS litigation authority closed claims study7, NAP4, 4 and the Australian audit of airway incidents project8 have repeatedly highlighted inadequate clinical judgement as a cause of airway incidents. The Australian airway lead initiative will provide invaluable advice and support through safety and quality activities as well as individual counselling and consultation.
Currently, the Australian and New Zealand College of Anaesthetists (ANZCA) professional document PS61 ‘Guidelines on equipment to manage a difficult airway during anaesthesia’ is under review and there are expectations that airway leads will play a vital role in the administration of the new guidelines. While the range of airway management devices and techniques rapidly expands, so does the airway leads network, which will provide an important resource for procurement, training and ongoing research.
Airway database
As previously described by Feinleib et al., 9 airway databases can be considered to fulfil one of two primary purposes. The first is patient protection, with the aim of informing and facilitating safer future care, or airway data collection, to allow the study of difficult airway incidents, aetiology and complications. Australia does not presently have a national patient protective airway database. Although simple in concept many practical hurdles need to be addressed for a robust registry to be created. Issues include patient privacy and identification, standardisation of the airway information collected and the ability to include enough clinically relevant detail which can be updated with future episodes of care. Information needs to be available across health jurisdictions and at the point of care and have an adequate source of funding for setup and maintenance of the database. Striving towards this goal is nonetheless an important step in patient safety.9–11
Internationally, national level airway databases have been successfully introduced. The Difficult Airway Society (DAS), UK, has funded a patient protection and data collection registry. This has navigated the complexity around patient information storage to create an online portal. Hospital trusts must sign up to be able to access the system, and any practitioner with significant airway experience can make an entry. There is presently no universal agreement as to which cases should generate an airway alert. 12 Another dual-purpose airway database operating in New Zealand and the United States links into the MedicAlert difficult airway/intubation registry. There is, however, an annual cost associated with this registry which must be borne by either the patient or the healthcare provider.11–13
Even in the presence of a high-quality database, a patient who presents to a different health organisation or hospital remains the vital link to alerting the clinician to the availability of difficult airway information. The patient needs either recollection that a previous problem occurred, a wallet card style notification, or MedicAlert bracelet. Informing the patient at the time of previous difficulty with airway management is a critical step but one which can be unreliable. 9 , 11
The Queensland Statewide Anaesthesia and Perioperative Care Clinical Network (SWAPNET) group have been working toward a patient protective airway database in Queensland with long-term goals of a national database.14,15 With the help of wide consultation with clinical anaesthetists throughout the state of Queensland, the following inroads have been made:
development of a standardised airway alert collection form in paper and electronic format;
16
agreement on definitions for difficult airway, difficulty with bag–mask ventilation, supraglottic airway ventilation, and tracheal intubation (both direct and via videolaryngoscopy);
17
guidelines for when a difficult airway alert needs to be generated;
17
guidelines as to how to disseminate difficult airway information;
17
added terminology into systematised nomenclature of medicine—clinical terms (SNOMED CT); that is, the language used for the electronic reporting of clinical information, to include difficult airway alert;
14
approval for uploading of the difficult airway alert form into the state-wide electronic health platform ‘The Viewer’ (accessible in public and private hospitals). This sits on the front page as an alert in a similar manner to an allergy.
14
A long-term goal is to utilise the national ‘My Health Record’ as a portal for the difficult airway alert information. Consultation with the Australian Digital Health Agency towards this intention is in progress; however, it will be several years before a national patient protective airway database is a reality in Australia.
Advanced airway assessment techniques
Nasendoscopy
Nasendoscopy has a variety of indications in airway management, including assessment of the upper airway and trachea, with a pivotal role in planning tracheal intubation and extubation.18,19 It also allows examination of in situ airway devices such as SADs, tracheal tubes and tracheostomy tubes. It is used for assessment of the middle column that may be either narrowed or distorted by infections, laryngeal tumours or upper airway oedema.
Nasendoscopy is commonly performed on awake patients in the sitting or semi-reclined position. Mastery of the technique also improves the ability to pass a bronchoscope through the nose from a position in front of the patient, facilitating awake fibreoptic intubation (AFOI) (Figure 1). After explaining the procedure to the patient, the nose is prepared using lidocaine spray with phenylephrine. The vasoconstrictor shrinks the mucosa of the inferior turbinate, increasing the size of the nasal passage. The nasendoscope is passed under vision between the septum and the turbinates, usually inferior to the inferior turbinate, parallel with the hard palate. At the back of the nasopharynx, the patient is asked to phonate or poke out their tongue, and the scope is flexed downwards to allow vision of the glottis.
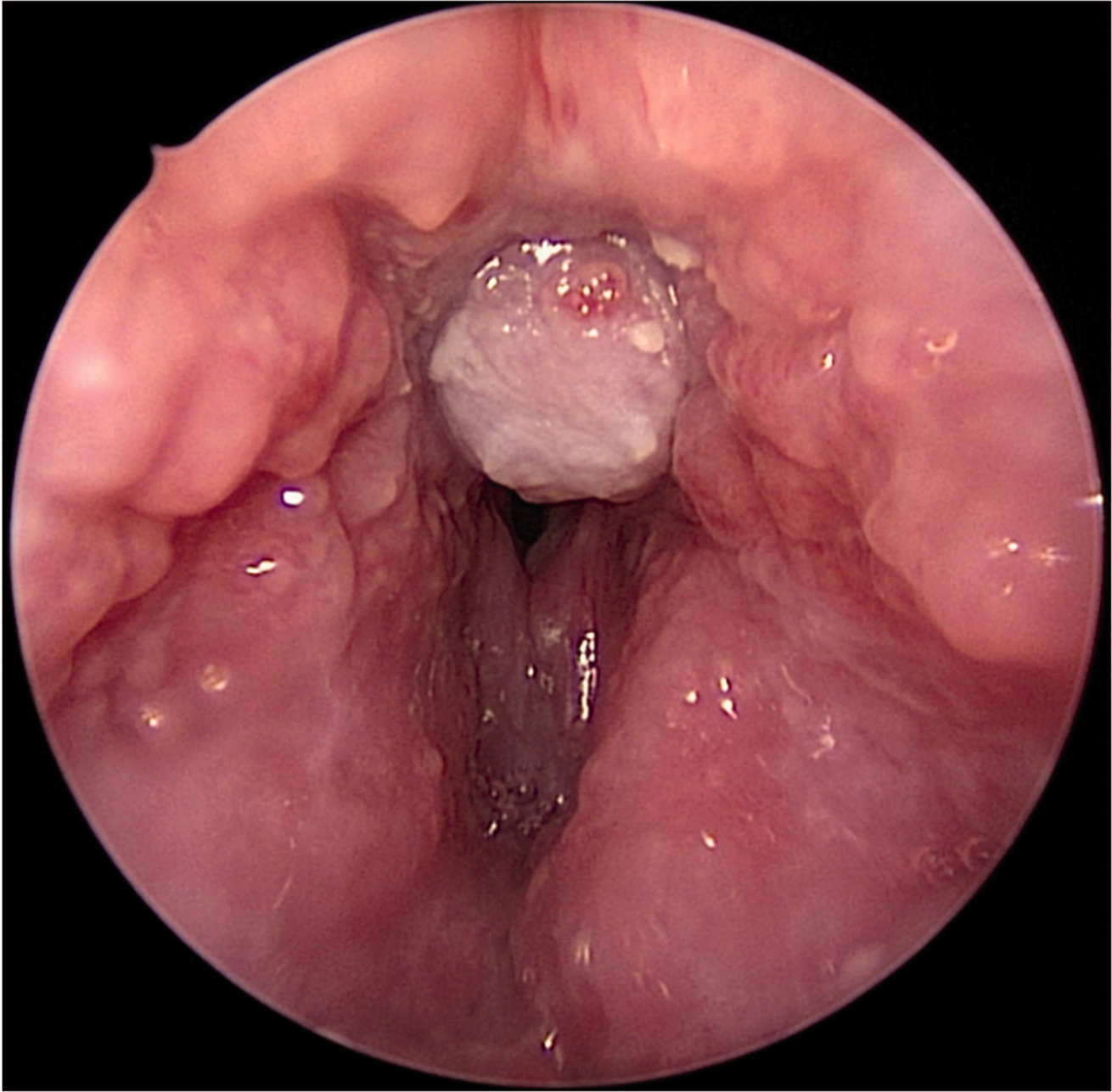
View of tumour just above the vocal cords.
The results of nasendoscopy may not directly correlate with airway changes that occur in the supine position following the induction of anaesthesia. However, the results of the examination are invaluable when used in the context of a full assessment in a variety of difficult airway scenarios. It is easily learned and is a useful adjunct to an anaesthetist’s airway toolkit.
Ultrasound for airway management
Ultrasound of the airway has been in clinical use since the early 1990s. Since then, there has been significant improvement in both the quality of equipment and images produced. Point-of-care ultrasound (POCUS) can be used in all stages of airway management. A high frequency, 38 mm linear transducer is sufficient in analysing the majority of anterior upper airway structures.
Tongue thickness can be measured by placing the probe positioned submentally in the medial sagittal plane. A tongue thickness greater than 6.1 cm is an independent predictor of difficult tracheal intubation. 20
Placing the ultrasound probe transversely, above the thyroid cartilage, allows for dynamic assessment of the vocal cords. This may be useful in the assessment of stridor and respiratory distress perioperatively, along with allowing for the accurate identification of vocal cord palsy postoperatively. 21 The use of ultrasound to assess subglottic diameter is superior to an age- and height-based formula in estimating tracheal tube size in the paediatric population. 22 The most commonly recommended technique of airway ultrasound is in the preoperative marking of the cricothyroid membrane, as it has shown significantly higher success rates than traditional palpation techniques. 23
Gastric POCUS has been described as a reliable technique to estimate the volume of gastric content in fasted and non-fasted patients in a range of different populations. 24 Ultrasound has a high diagnostic capability in confirming tube position in airway management in real time, before the first ventilation attempt. 25
Ultrasound is a useful tool in assessing the position and the diameter of the trachea before tracheostomy insertion. Overlying vessels and structures at the proposed insertion site can be identified before incision. Ultrasound assessment will also aid in the selection of the best tracheal ring interspace for tube insertion and provide information for choosing the appropriate size and length of tracheostomy tube. Ultrasound for airway management is still in its development phase. Scans are easily and quickly performed, but the results may still be operator dependent. Therefore, further training and research is required prior to mainstream use.
Advanced airway management techniques
High-flow nasal oxygenation
HFNO provides oxygen flow rates that will match or exceed a patient’s inspiratory flow rate and allows a predictable titration of the inspired oxygen concentration up to 95%–100%. 26 The technique can provide a useful and well-tolerated adjunct to difficult airway management. The physiological benefits of HFNO include improved respiratory mechanics, increased functional residual capacity, as well as a degree of carbon dioxide washout, which limits the increase of arterial carbon dioxide tension during apnoea. HFNO also provides flow rate–related positive end-expiratory pressure, especially with closed mouth breathing. 26
Of relevance to the anaesthesia and critical care environments, the use of HFNO has been described as an alternative to conventional facemask pre-oxygenation and as a means of providing an increased apnoeic oxygenation time following the induction of anaesthesia. This can allow an extended period of time in which to secure the airway. 27 HFNO has also been used to provide oxygenation during awake tracheal intubation (ATI) 28 during ‘shared airway’ procedures for patients with airway obstruction. This has been demonstrated for both spontaneously breathing and apnoeic patients. 29
In order to allow the HFNO technique to be used effectively and safely, the patient must have a patent upper airway, and care should be taken not to combine the HFNO technique with a tight-fitting facemask attached to a closed or semi-closed breathing circuit. Also use caution and remove the prongs during complete airway obstruction as this risks high airway pressures, barotrauma and gastric insufflation.
In addition, the combination of HFNO, alcohol skin preparation and an ignition source such as laser or diathermy has been linked to cases of airway fires. 30 Several institutions report the equipment including an air blender that can reduce the fractional inspired oxygen to 0.3 or less during appropriate phases of ‘shared airway’ surgery. Of note, the manufacturer of one of the more commonly used products providing HFNO does not recommend its use in this type of surgery. Other contraindications to the use of HFNO include complete nasal obstruction, the presence of a base of skull fracture/cerebrospinal fluid leak and an untreated pneumothorax.
Fibreoptic intubation
In Australia, services that qualify for Medicare rebates show that there were 2858 (0.09% of all anaesthetic services) bronchoscopic interventions for a difficult airway in a total of 3,061,532 service episodes, which include monitored care and regional-based techniques in the last financial year. These figures exclude patients who are treated free of charge in public hospitals or are covered by the Department of Veterans' Affairs and workers' compensation. It is very likely that the figures underestimate the number of bronchoscopic interventions.
The incidence of difficult intubations is estimated to be between 2.2% and 5.8%. 4 From Canadian and UK-based studies, ATI is required in up to 1.7% of endotracheal intubations, 31 with the vast majority being performed by flexible bronchoscopy even in centres that used videolaryngoscopy most of the time. 32 The reported failure rate for AFOI was between 1% and 2%. 31
NAP4 identified numerous cases in which AFOI should have been used 4 but was not, possibly due to poor judgement, lack of skill or confidence, and inappropriate equipment selection. Given the low incidence of cases requiring ATI it is possible for an anaesthetist or trainee to fail to perform an AFOI for long periods, which has implications for knowledge, confidence, skill acquisition and retention.
This has led to the publication of ANZCA’s booklet ‘Topicalisation and sedation for awake fibreoptic intubation’ (https://www.anzca.edu.au/resources/sig-resources/2019-airway-management-sig-afoi-topicalisation-sed) and DAS guidelines for ATI in adults 33 to assist with the principle of awake intubation. Benchtop training, 34 bronchoscopic simulators 35 and airway workshops 36 can help skills acquisition to gain expertise rather than having to rely on performing a number of procedures to gain experience.
A recent meta-analysis of eight studies concluded that videolaryngoscopy for elective ATI was associated with a shorter intubation time while retaining a similar success rate and safety profile. 37 However the studies excluded patients with limited mouth opening.
El-Ganzouri et al. devised a simplified scoring system involving mouth opening, thyromental distance, Mallampati, neck movement, jaw pronation, body weight and a history of difficult intubation, which is applicable to device selection in terms of conventional laryngoscopy, videolaryngoscopy and ATI. 38 In simple terms, for a score greater than 7, an ATI technique should be used.
Bronchoscopes have not historically been considered to be rescue devices except in skilled hands. However, the combined video-assisted fibreoptic intubation is proving to be versatile for both elective and rescue situations. 39
Single-use bronchoscopes are increasingly being utilised with new variants coming from Karl Storz (Tuttlingen, Germany) and Verathon (Bothell, WA, USA), which will challenge the established Ambu Scopes (Ambu aScope; Ambu A/S, Ballerup, Denmark) and create an interesting discussion regarding the environmental and relative cost of using disposable scopes.
Vision-guided insertion of SADs
The UK DAS 2015 guidelines 40 for the management of unanticipated difficult intubation stressed the importance of preoperative airway assessment and the problems associated with the lack of reliability of predictors of difficult airways. The guidelines examine the need for adequate planning and preoxygenation, including optimising patient positioning to increase the chance of first-time success. They also stress the first-line use of devices such as videolaryngoscopes, fibreoptic scopes and bougies. Limiting the maximum number of intubation attempts, having a management plan and prompt declaration of failure reduces the chance of harm to the patient. Management plans included declaring ‘failed intubation’, waking up the patient, placement of a SAD, or proceeding to an emergency front-of-neck access (eFONA) (scalpel or needle technique). The guidelines repeatedly stress that ‘blind insertion techniques’ should not be used, as these insertions are associated with trauma and serious adverse outcomes.
Intubation is the primary method of airway management for fewer than 40% of general anaesthetics in the UK, with the use of SADs dominating. 4 It is therefore not surprising that SADs have such a prominent role in airway management since their development by Brain in 1981, which revolutionised airway management. Twenty years later the first prototype of a second generation SAD, the LMA ProSeal (LMA ProSeal Airway; Teleflex, Co. Westmeath, Ireland) followed. Although second generation SADs have many desirable features, they are nevertheless inserted in the same ‘blind’ way as first generation devices, whereby clinicians still rely on a set of subjective indirect tests to confirm their correct placement. However, studies have revealed that 50% to 80% of all SADs, irrespective of brand and size, do not fit snugly in the designated hypopharynx and that safety may be compromised with gas leaks and obstruction of the airway. 41 , 42
Research has demonstrated the problems of incorrectly positioned, blindly inserted SADs and proposed a flow chart promoting an ‘insert-detect-correct-as-you-go’ vision-guided insertion technique, using corrective manoeuvres as you need them. 43 , 44 As such, real-time, vision-guided insertion of a SAD avoids malpositioning, confirms adequacy of chosen size, first and second seal, and results in superior gas exchange and high oropharyngeal leak pressure, which helps in preventing gastric aspiration, not requiring any further action during the maintenance phase of anaesthesia. 45
Using a visualised insertion technique for all instrumentation of the oropharynx-larynx is an achievable goal, avoiding malpositioning and trauma to the airway while also guaranteeing a better positioned airway device. Therefore, anaesthetists are encouraged to rethink old strategies and develop ways to ‘see’ directly or indirectly how airway devices, for example, SADs, are inserted in a better anatomical fit with optimal functional results during airway management.
Avoid blind intubation through SADs
Following the widespread uptake of Dr Archie Brain’s LMA-Classic in the late 1980s, clinicians very quickly saw the benefits of using SADs as a conduit and performing blind intubation of the trachea through them. 47 This led to the publication of a number of case reports highlighting the harm related to blind intubation through these devices. A comparative study of blind intubation through the I-gel or the Intubating LMA (ILMA, Fastrach™, Teleflex, Co. Westmeath, Ireland) showed first time insertion success rates as low as 69%. 48
Therefore, the authors recommended the avoidance of blind intubation through SADs. New second generation SADs are emerging that either specifically allow or facilitate tracheal intubation. A study by Yoo et al. looked at blind intubation through the AuraGain (Ambu A/S, Ballerup, Denmark). The results demonstrated a very low success rate of 71% and concluded that this device was not suitable for blind intubation. 49 Direct view using a fibreoptic scope with the endotracheal tube loaded increases the success rate but is technically more challenging. Atherton et al. described the ventilation-exchange bougie, known as the AIC (Cook Medical, Bloomington, IN, USA) in 1996 which fits snugly over a reusable intubating fibreoptic scope, thus allowing guided intubation through an LMA Classic. 50 AIC-facilitated intubation has also been described with other SADs including the LMA Proseal 51 and the I-gel. 52 Not all second generation SADs are reliable conduits and difficulty with AIC-guided intubation through an LMA Supreme has been reported. 53 The study of Van Zundert et al. 53 highlighted the difficulty of using an Aintree with a size 3 LMA Supreme. All new SADs will need to be assessed to ensure they are reliable conduits for fibreoptic-assisted intubation.
In conclusion, most airway management guidelines stress the importance of limiting futile attempts at laryngoscopy and progressing in a timely fashion to rescue techniques using second generation SADs. If a decision is made to attempt intubation through the SAD, blind techniques should NOT be attempted. The choice of SAD for rescue should be based on the proved success of that device as a conduit for visualisation of the larynx and intubation. It behoves us all as an anaesthetic community to ensure this important technique is taught and practised ensuring a successful outcome for our patients.
Updates on ‘can’t intubate can’t oxygenate’
The ‘can’t intubate, can’t oxygenate’ (CICO) scenario occurs when oxygenation cannot be achieved using the anatomical conduits of the upper airway. The term directs the clinician to the immediate priority of oxygenation. While the debate continues as to the most appropriate technique to facilitate oxygenation during a CICO crisis, there have been recent advancements in this space. 54 Thorough preoperative airway assessment and planning have been encouraged although this does not guard against CICO. 40 Planning for failure ensures the clinician has communicated the airway plan and sequence of actions to be followed should this be required.
The contribution of human factors to adverse outcomes during emergency management is widely accepted. 4 The ACE Airway Management SIG working party has produced a document on human factors and transition specific to CICO. Cognitive aids may improve non-technical skills during airway emergencies. Effective communication is a core non-technical skill and critical language has been encouraged to improve clarity and understanding especially relevant during a crisis. 55 Like the equipment, language needs to be simple, intuitive, precise and familiar. eFONA and CICO rescue have been recommended as universal terms for use in a crisis.
eFONA procedures in anaesthesia refer to all airway management techniques performed below the larynx by way of the anterior surface of the neck with the purpose of providing rescue oxygenation, by scalpel or cannula techniques. ANZCA acknowledges that there is a difference of opinion relating to the preferred management of performing eFONA and does not mandate a particular approach to eFONA.
ANZCA has incorporated CICO training as one of the mandatory modules of which two are required for completion each continuing professional development triennium. The algorithm of Heard et al. 56 is supported by the ANZCA Airway Management Group document ‘Transition from supraglottic to infraglottic rescue in the “can’t intubate can’t oxygenate” (CICO) scenario’ 57 and has been incorporated into the effective management of anaesthetic crises participant manual. 5
Palpation, ultrasound or pre-incision may be used to identify the cricothyroid membrane or trachea. Ultrasound may be useful in the elective setting; however, its use in an emergency CICO scenario is not universally recommended. 23
The ACE Airway Management SIG has recently reviewed the difficult airway trolley. It has recommended that eFONA equipment is part of the essential airway equipment on all difficult airway trolleys in critical care areas and that it should be available at the point of care.
Equipment should be available for both adult and paediatric patients where appropriate. Thankfully, the incidence of CICO in otherwise healthy children is exceedingly rare. 58 If equipment and the expertise of an ear, nose and throat surgeon are available, then surgical tracheostomy may be the best option in most instances. Clinicians and institutions are encouraged to ensure that suitable equipment is immediately available and that airway practitioners are familiar with the techniques and equipment available.
Non-technical skills
The bow-tie diagram, a mapping tool to assess airway incidents
Unexpected difficulties in airway management are challenging to study due to their rarity, 4 differing severity and causation models. The most reputable level of evidence is case series, case reports and case-based audits, leading to an abundance of varying data and recommendations.
The bow-tie diagram (Figure 2) is a risk evaluation tool, which is used to analyse causal relationships. It has been extensively used in high-risk industries and has been proposed as a mapping tool for anaesthetic incident analysis.59,60 It represents the fusion of a ‘fault’ tree and an ‘event’ tree, linking the cause and effect of decision-making processes. The diagram allows for a visual correlation between hazards, preventive measures, management and outcomes of incidents, which are all important considerations in airway management and planning.
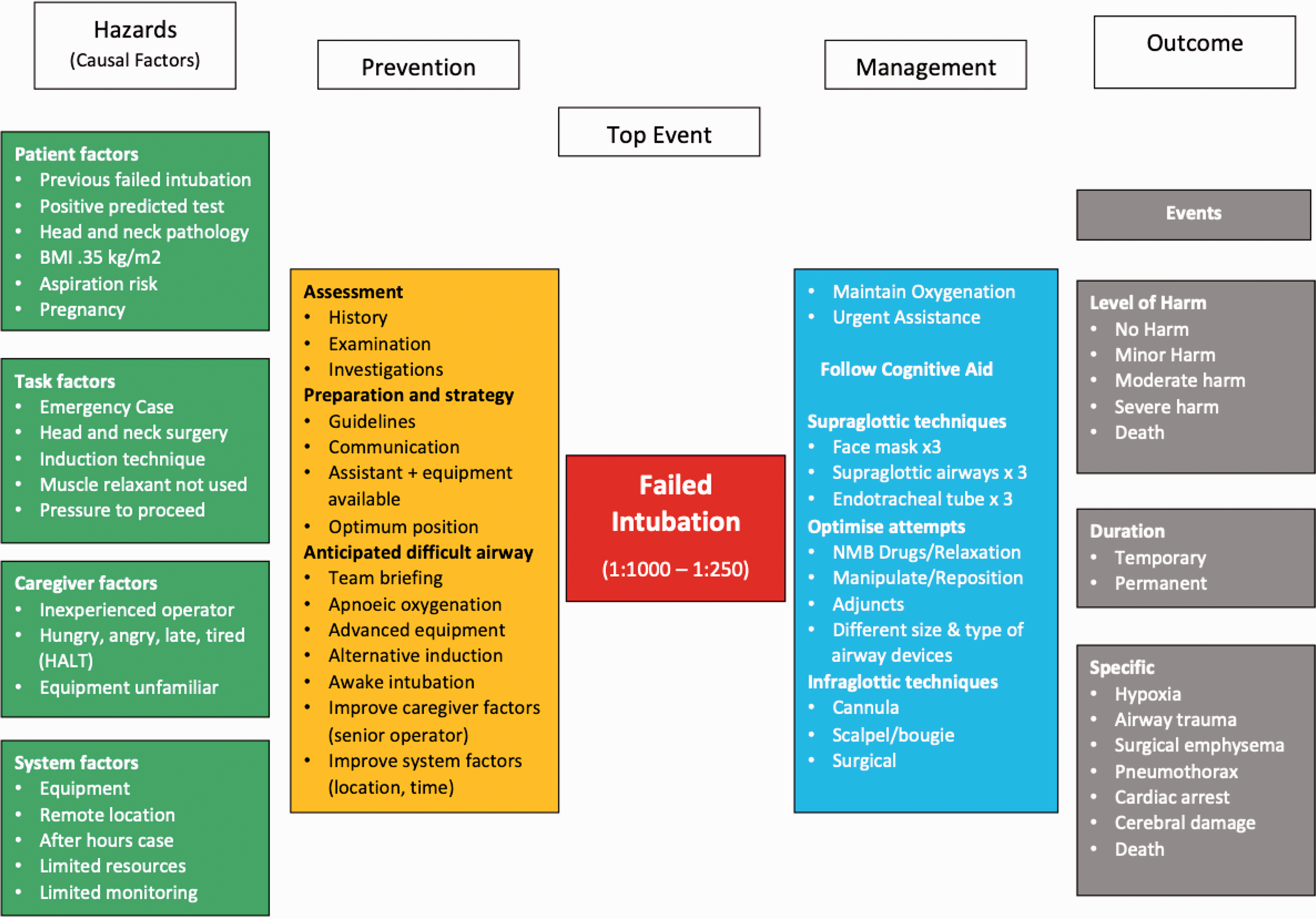
‘Bow-tie’ diagram failed intubation outlining risk factors, prevention strategies, management and outcomes of failed intubation. Reprinted with permission of Endlich and Culwick. 63
The incidence of failed intubation has been described as one in 1000–2000 cases in the elective general population and one in 250 in the emergency setting. 4 Outcomes range from minor harm to catastrophic events. 4 Analyses of databases 4 , 61 have collated data regarding the risk factors which may lead to a failed intubation.
Major airway societies have developed guidelines for the management of unexpected difficult airways, emphasising prevention and preparation for the unexpected difficult airway before induction. 40 , 50 The management of failed intubation requires quick decision-making. Detailed algorithms may not be cognitively accessible in this situation and require the use of visual aids to facilitate their implementation in real time. 55 , 57
Outcomes of failed intubation are categorised into generalised outcomes, as per the Agency for Healthcare Research and Quality 62 scale, describing the severity and duration of the incident and into specific outcomes, providing detailed information. In order to memorise easily the information that is required to assess, prevent and manage airway events, it is advantageous to use the bow-tie diagram to group the information into risk factors, principles for prevention, management (should prevention fail), and then the possible resulting outcomes. 63
Cognitive aids
Since the American Society of Anesthesiologists released their first algorithm for difficult airway management in 1993, 64 followed by the first DAS flowcharts in 2004, 65 a vast array of algorithms and cognitive aids have appeared in the anaesthetic literature. 55 , 57 Some, like the aforementioned DAS flowcharts are comprehensive, detailed and designed more as a learning or preparation tool. Others, like the locally designed Vortex cognitive tool 55 and the ANZCA transition to CICO cognitive aid 57 are less complex and designed more for use during an airway emergency. A number of context-specific tools have also recently appeared, including flow charts to guide difficult airway management in the obstetric 66 and the critically unwell patient. 67 The need for decision-support tools in airway management was emphasised by the authors of NAP4 in the UK, 4 in which errors in decision-making were felt to have contributed to many of the reported serious airway complications.
A soon to be published survey looking at institutional preparedness to manage critical anaesthetic airway events in Australian and New Zealand teaching hospitals provides some interesting insights into what algorithms and cognitive aids are currently utilised at the point of care and in teaching. 68 The survey achieved a 91% response rate, with 129 teaching hospitals providing data.
A large proportion (70%) of responding hospitals indicated that there was at least one cognitive aid routinely available in their operating theatres for the management of difficult airways or CICO events. Those most commonly reported as being available were the DAS flow chart (25% of Australian and 39% of NZ responders) and the Vortex cognitive tool (24% of Australian and 22% of NZ responders), the Royal Perth Hospital CICO algorithm (15% of Australian and no NZ responders) and the ANZCA transition to CICO cognitive aid (14% of Australian, 11% of NZ responders).
An even higher proportion (91%) of the responding hospitals indicated that they provide training in the management of the unanticipated difficult airway and CICO events. The responding hospitals indicated that their training was most commonly based on, or included, the following algorithms or cognitive aids: the Royal Perth hospital CICO algorithm (59% of Australian, and 36% of New Zealand responders), the Vortex cognitive tool (60% of Australian and 36% of New Zealand responders) and the DAS flowchart (35% of Australian and 50% of New Zealand responders). It would be interesting to know whether a similar proportion of the private hospitals and smaller public hospitals, which were not included in the survey, are providing decision support tools at the point of care and training based around specific algorithms or cognitive aids.
Conclusions
Advanced techniques in airway assessment and management, the use of non-clinical skills, and techniques to prevent incidents caused by failed airway management are continuously evolving. The ACE Airway Management SIG is a group of enthusiastic airway experts involved in all of these aspects. The teaching and training of the mentioned techniques are regularly facilitated in workshops and at scientific meetings. The airway lead network is evolving all over Australia and New Zealand and guidelines and recommendations are regularly reviewed and assessed.
Footnotes
Acknowledgements
The author(s) acknowledge the contribution and support of current and past Anaesthesia Continuing Education Airway Management Special Interest Group members.
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.