
Abstract
This audit of airway incidents was conducted over six months in 12 tertiary level hospitals across Australia and New Zealand. During that time, 131,233 patients had airway management and 111 reports were submitted (incidence 0.08%). The airway incidents included a combination of difficult airway management (83), oxygen desaturation (58), aspiration (19), regurgitation (14), laryngospasm (16), airway bleeding (10), bronchospasm (5) and dental injury (4), which gave a total of 209 events in 111 reports. Most incidents occurred during general anaesthesia (GA; 83.8%) and normal working hours (81.1%). Forty-three percent were associated with head and neck surgery and 12.6% with upper abdominal procedures. Of these patients, 52% required further medical treatment or additional procedures and 16.2% required unplanned admission to an intensive care unit or a high dependency unit. A total of 31.5% of patients suffered from temporary harm and 1.8% from permanent harm. There was one death. The factors associated with a high relative risk (RR) of an airway incident included American Society of Anesthesiologists Physical Status (ASA PS) (ASA PS 2 versus 1, RR 1.75; ASA PS 3 versus 1, RR 3.56; ASA PS 4 versus 1, RR 6.1), and emergency surgery (RR 2.16 compared with elective). Sedation and monitored anaesthesia care were associated with lower RRs (RR 0.49 and RR 0.73 versus GA, respectively). Inadequate airway assessment, poor judgement and poor planning appeared to be contributors to these events. Future teaching and research should focus on these areas to further improve airway management and patient safety.
Introduction
In 1993, the Australian Incident Monitoring Study (AIMS) provided ground-breaking information concerning critical incidents during anaesthesia.1–4 Since that time, the Fourth National Audit Project (NAP4) of the Royal College of Anaesthetists has provided a better understanding of airway management complications in hospitals. 5 NAP4 data are now, however, over a decade old and reflect practice within the United Kingdom (UK) at that time. Many changes in both Australian and UK practice have been adopted in the wake of NAP4 findings and it was therefore considered timely to conduct a prospective audit of airway incidents in a selection of Australian and New Zealand tertiary level hospitals. The aim was to record the current incidence of airway incidents in these hospitals, and to identify areas on which to focus further efforts to improve airway safety. For the purposes of the audit, airway incident was defined as any unexpected airway event resulting in a near miss of harm, temporary harm, or permanent harm.
Methods
Airway Special Interest Group members working in major tertiary hospitals across Australia and New Zealand were contacted and invited to participate in this audit. Of these sites, 12 provided a positive response and the hospitals audited were the Royal Brisbane and Women’s Hospitals, Royal Adelaide Hospital, St Vincent’s Hospital (Sydney), Royal North Shore Hospital (Sydney), Royal Melbourne Hospital, The Alfred (Melbourne), Wellington Hospital, North Shore Hospital (Auckland), Royal Darwin Hospital, Royal Perth Hospital, Cairns Hospital and Princess Alexandra Hospital (Brisbane). Each hospital had at least one site coordinator, to provide local support for the Anaesthesia Airway Audit project (AAAp). The audit was conducted over six months from 3 April to 5 October 2018, inclusive. Numerator and denominator data were collected contemporaneously.
The reporting of difficult airway events during AAAp was overseen by members of the Airway Management Special Interest Group in conjunction with the webAIRS anaesthetic incident reporting programme. WebAIRS is supported by the Australian and New Zealand Tripartite Anaesthetic Data Committee (ANZTADC). 6 This committee is run jointly by the Australian Society of Anaesthetists, New Zealand Society of Anaesthetists and Australian and New Zealand College of Anaesthetists. A dedicated website was set up within the webAIRS portal to accommodate the recording of the difficult airway event data (https://www.anztadc.net/aaap.aspx). Data were entered via mandatory tick-boxes. Free text options were included to allow reporters to add narrative about the event and reflections about contributing and alleviating factors.
The reporting of all airway events over the six-month audit collection period was under the supervision of site-specific coordinators. All participating sites agreed to report all airway events during the study period, and each site coordinator monitored and ensured that all airway events were reported to the audit. The denominator data for the complete study period were collected utilising the local medical record keeping systems and then extracted at the conclusion of the study.
The data were collected in compliance with the National Health and Medical Research Council recommendations for Quality Assurance data. Additionally, multicentre ethics approval is maintained at the Royal Brisbane and Women’s Hospital Human Research Ethics Committee (HREC/11/QRBW/311) and the Nepean Blue Mountains Local Health District (HREC/12/NEPEAN/18). In New Zealand, ethics approval has been obtained from the Health and Disability Ethics Committee (MEC/09/17/EXP). All 12 sites taking part in the audit were registered with webAIRS prior to commencing the audit.
Airway incidents to be reported included any event where the treating anaesthetist considered the situation was not controlled, unexpected oxygen desaturation occurred, or there was a necessary deviation from the proposed initial airway management strategy. Typical cases included aspiration, dental injury, oral trauma, oxygen desaturation and unexpected intensive care unit (ICU) or high dependency unit (HDU) admission due to airway management complications. In addition, any situations where a patient had to be woken up as part of their airway management were included. All cases of emergency front-of-neck access (eFONA) were to be reported, as were all deaths related to airway management complications.
The narrative and the codified data of all airway incident reports were initially assessed independently and evaluated by all authors. Findings were compared and discussed with consensus decisions made where necessary. Reports that contained test data, duplicated data, did not contain a description of the event or did not include an airway event, were excluded.
Results
There were 111 difficult airway events during the audit period in the 12 tertiary level hospitals. The total number of cases managed during this time was 131,233, giving an airway event incidence of 0.08%. Denominator data for American Society of Anesthesiologists Physical Status (ASA PS), urgency of case, and type of anaesthesia were provided by all 12 hospitals. Denominator data for age and gender were provided by 11 hospitals. Unfortunately, denominator data for body mass index kg/m2 (BMI), time of day, and type of surgery were provided by only four or fewer hospitals (Table 1). The airway incidents included difficult airway management (83), oxygen desaturation (58), aspiration (19), regurgitation (14), laryngospasm (16), airway bleeding (10), bronchospasm (5) and dental injury (4), which gave a total of 209 events in 111 reports.
Denominator data for the participating sites.
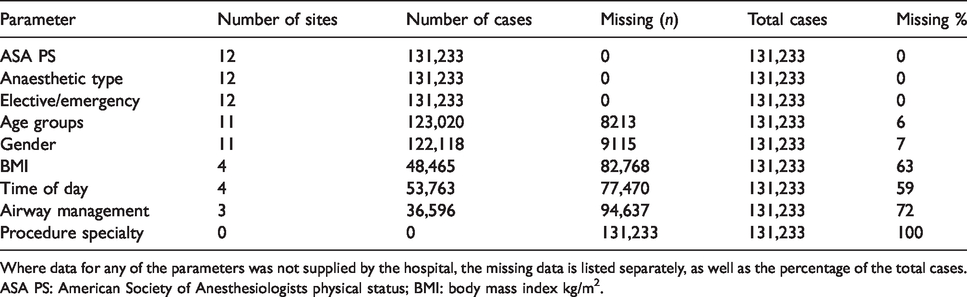
Where data for any of the parameters was not supplied by the hospital, the missing data is listed separately, as well as the percentage of the total cases.
ASA PS: American Society of Anesthesiologists physical status; BMI: body mass index kg/m2.
The distribution of patients by gender, ASA PS and age groups are shown in Table 2. There were 48 males and 59 females (four cases were not specified). Most of the airway incidents were in the 50- to 59-year age group (20.7%) and in patients with ASA PS classification 3 (45.1%). The relative risk (RR) of airway incidents in patients ASA PS 2, 3 and 4 versus ASA PS 1 was 1.75, 3.56 and 6.1, respectively. The RRs of airway incidents in patient age groups 30–39 years, 40–49 years, 50–59 years, 60–69 years, 70–79 years and 80–89 years versus <30 years were 0.73, 0.83, 1.17, 0.77, 0.65 and 0.49, respectively. The RR of an airway incident in males versus females was 1.18.
Demographical data of study patients.
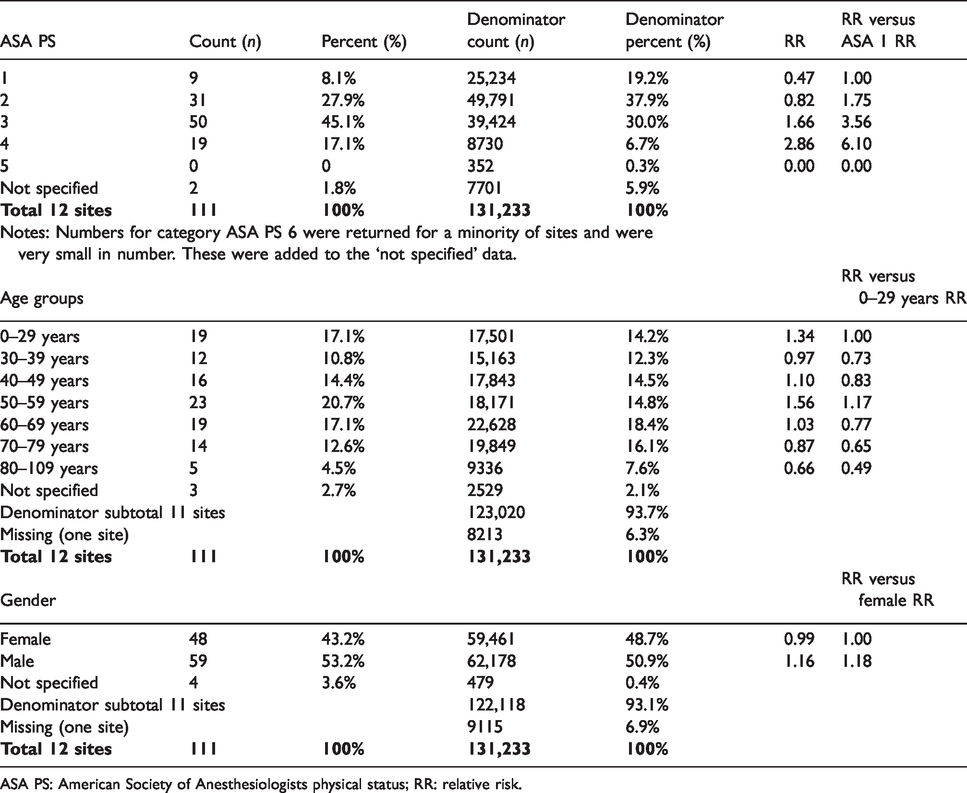
ASA PS: American Society of Anesthesiologists physical status; RR: relative risk.
As expected, most of the incidents occurred during general anaesthesia (GA; 83.8%) and during working hours (81.1%) (Table 3). However, nearly 10% of all incidents occurred during sedation (Table 3). The RR of an airway incident during sedation or monitored anaesthesia care (i.e. with no drugs) versus GA was 0.49 and 0.73, respectively. The RR of an airway incident during emergency cases was 2.16 versus elective cases.
Type of anaesthesia and airway events.
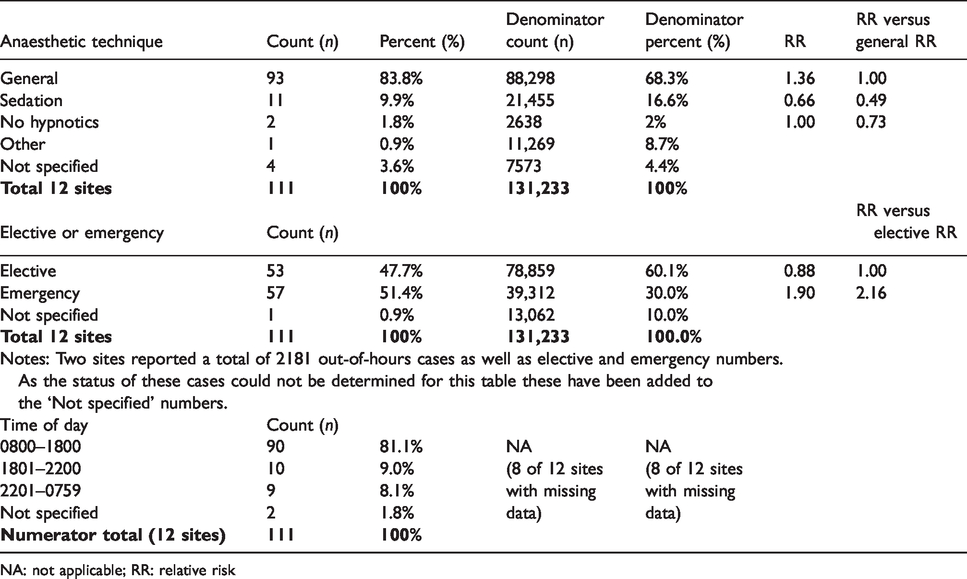
NA: not applicable; RR: relative risk
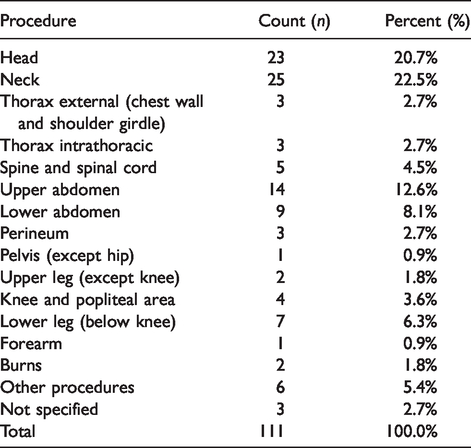
Most of the incidents occurred during induction or the first 10 min post induction (50.5%) and 18% occurred during emergence or postoperatively (Table 4). Most occurred during head and neck (43.2%), upper abdominal (12.6%) or lower abdominal surgery (8.1%) (Table 5). Insufficient denominator data were collected for the calculation of RRs for different types of surgery.
Timing of airway events during anaesthesia.
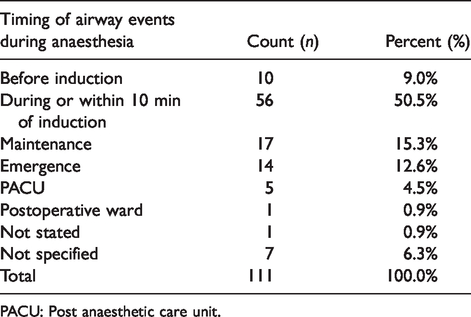
PACU: Post anaesthetic care unit.
Type of surgery.
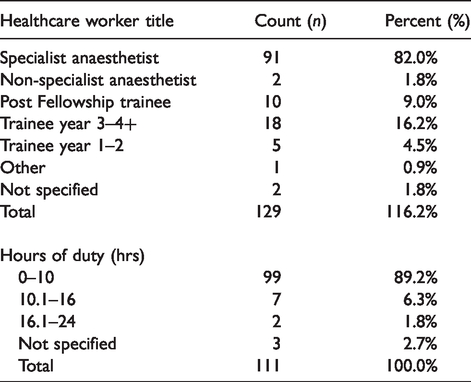
Either senior anaesthetists (82%), senior trainees (3 or more years’ experience – 16.2%) or anaesthetic post Fellowship trainees (9%) were managing the patient during the airway incidents (Table 6). As expected, these personnel were commonly working within the first 10 h of starting duty at the time of the incident (89.2%) (Table 6). However, 8.1% of airway incidents were being managed by personnel who had been working 10–24 h after the start of their duty. Insufficient denominator data for seniority of anaesthetists and hours worked were available for calculation of RRs.
Healthcare worker title of personnel in charge of case and airway incidence (NB: more than one rank of anaesthetic cover could be present) and the number of hours the healthcare worker was on duty.
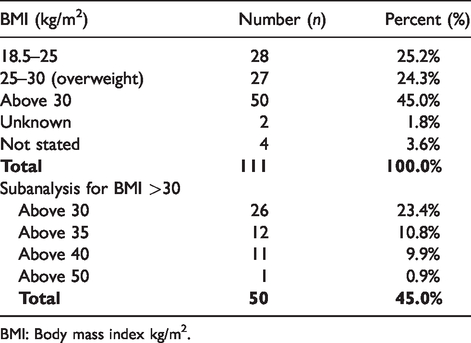
Most of the reported incidents occurred in patients with a BMI > 30 (45%) (Table 7), with 21.6% occurring in patients with a BMI >35 (Table 7). Insufficient denominator data for BMI were collected for calculation of RRs of increased BMI levels.
BMI and number of reports.
BMI: Body mass index kg/m2.
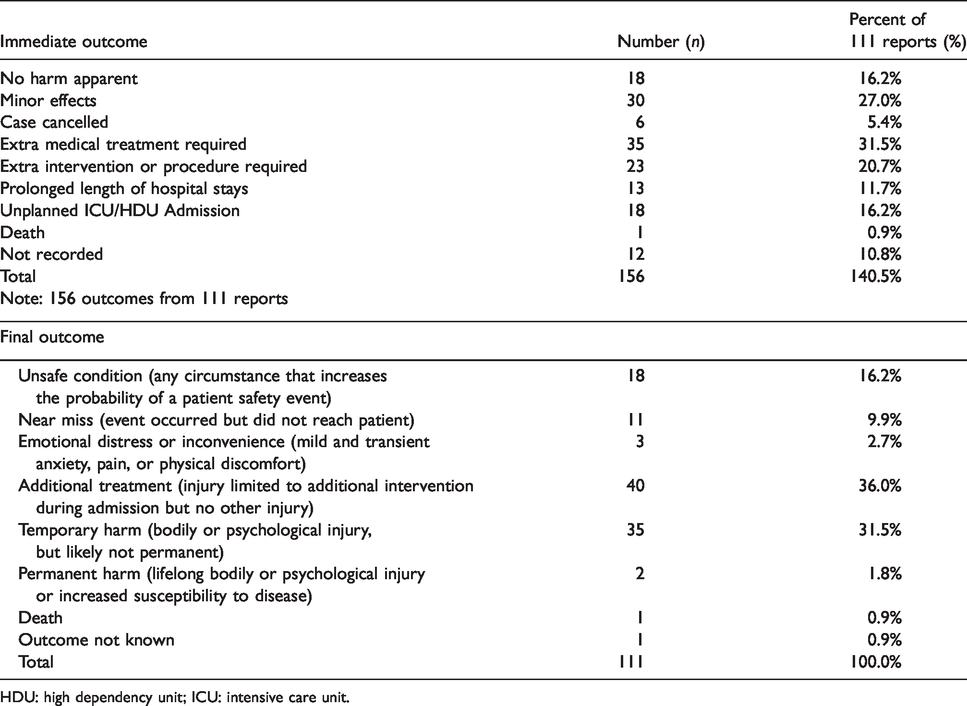
The immediate patient outcome was most commonly either no adverse effect or minor harm (43.2%; Table 8) as judged by the personnel reporting the incident. However, 52.2% required further medical treatment or additional procedures and 16.2% required admission to either an ICU or HDU. One patient died during the audit period from airway-related complications. There were eight cases where front-of-neck airway (FONA) access was required. Three (2.7%) were true emergency FONAs (eFONA), defined as events where facemask ventilation, supraglottic airway insertion and laryngoscopy and attempted tracheal intubation had failed. The others were awake tracheostomies in patients with recognised upper airway obstructions. All FONAs were performed by surgeons, and all were associated with good patient outcomes.
Immediate and final patient outcomes.
HDU: high dependency unit; ICU: intensive care unit.
About 65% of long-term (final) outcomes were classified as no temporary or permanent harm. There was temporary harm in 31.5% of incidents and permanent patient harm in two patients (1.8%). There was one death, which initially involved difficult ventilation accompanied by desaturation whilst using a supraglottic airway. This was followed by a difficult intubation, but high airway pressures persisted, and a cardiac arrest occurred, which may have been partly related to difficult airway management. Although no injury occurred in the majority of cases, 36% patients required ongoing management and use of hospital resources.
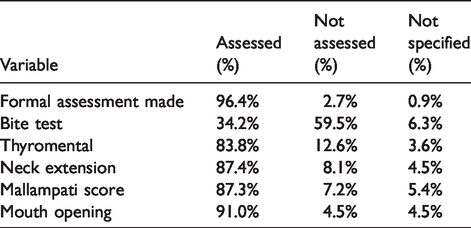
The results for airway assessment are shown in Table 9. Just over 96% reported a formal airway assessment. In three patients (2.7%) the airway was not formally assessed: it is not known whether these reports were from patients receiving monitored care only. In one patient (0.9%) the question was not answered.
Formal airway assessment.
Discussion
The overwhelming finding of this prospective audit in 12 tertiary referral hospitals across Australia and New Zealand was a low incidence of airway incidents. There were only 111 airway incidents during the anaesthetic management of 131,233 patients, an incidence of 0.085%, or about one incident for every 1180 episodes of anaesthesia care. Moreover, most patients were mostly managed successfully, with temporary harm occurring in only 31.5% of incidents, and permanent harm in only 1.8%. There was also one death, which occurred in a patient who had a complex medical history. Her unfortunate outcome can partly be related to her failed airway management.
This audit is one of several audits that have been performed in Australia, New Zealand, the UK, and United States (US) over the past three decades. The first major audit was AIMS in 1993.1–4 The commonest complications in that investigation were oesophageal intubation, arterial desaturation and regurgitation of gastric contents. Obesity, limited neck mobility and mouth opening, and inadequate assistance were major contributing factors to these complications. 4 AIMS was followed by the American Society of Anesthesiologists (ASA) Closed Claims Project in 1990, which showed the most common adverse events were injury following inadequate ventilation, oesophageal intubation, and difficult tracheal intubation. 7 These findings led to the development of the ASA difficult airway management practice guidelines in 1993. 8 Later, Cook and colleagues found similar results with their analysis of the National Health Service Litigation Authority Closed Claims data in the UK from 1957 to 2007 and NAP4 and the Difficult Airway Society (DAS). 5 , 8 More recently, examination of the Anesthesia Closed Claims Project database from the years 2000 to 2012 showed that outcomes have remained poor and comparable with ASA’s previous report. 10
These studies repeatedly demonstrate that inadequate airway planning and judgement errors remain major contributors to patient harm. However, the main drawback of this type of analysis is the lack of a denominator for calculating the risk of injury. Also, the data are retrospective.
The AAAp was a prospective audit, with broad inclusion criteria ranging from minor to severe complications. In this audit, it was left to the reporting personnel to report ‘near miss’ cases and events that reached the patient where they felt that suboptimal airway management had taken place. NAP4 focused on more severe outcomes involving FONA access, brain injury, unplanned ICU admission or death, and reported an incidence of 1:22,000 general anaesthetics (0.005%). It is therefore not appropriate to make direct comparison of the current audit with the NAP4 audit. 11
Another advantage of this audit was the contemporaneous collection of denominator data for risk factors, such as ASA PS, type of anaesthetic and urgency of surgery, from which RRs could be calculated. One of the hospitals was unable to provide denominator data for age and gender, so the RRs for age and gender were based on data from the remaining 11 hospitals. However, these 11 hospitals contributed 93% of the patients. Unfortunately, insufficient denominator data were available for calculation of RRs related to the type of surgery, seniority of anaesthetists or BMI.
The factors associated with a high RR of an airway incident included ASA PS 2 versus 1 (RR 1.75), ASA PS 3 versus 1 (RR 3.56), ASA PS 4 versus 1 (RR 6.1) and emergency surgery (RR 2.16 versus elective) (Table 2). Sedation and monitored anaesthesia care were associated with lower RRs (0.49 and 0.73 versus GA respectively) (Table 3). Age and gender had little influence on RR (Table 2), except for patients >80 years, who appeared to have a lower RR (Table 2), but only a small number of patients were in this age group.
Most incidents occurred during or before anaesthesia induction (60%), but 12.6% occurred on emergence and a further 5.4% after leaving the operating theatre or suite (Table 4), indicating that incidents can occur at any time during the intra- and postoperative period.
The most common surgical procedures during which incidents occurred were head and neck (43.2%) (Table 5). Although sufficient denominator for type of surgery was not available for calculation of the RRs of head and neck surgery versus other types of surgery, it is unlikely that 43.2% of all procedures were head and neck, suggesting that head and neck procedures represent a higher RR of airway incidents. The remaining incidents occurred across a wide range of surgery types (Table 5).
Most incidents occurred between 0800 and 1800 h (81% of incidents) and were supervised by a specialist anaesthetist (82% of incidents) and within 10 h of the anaesthetist commencing duty (89% of incidents) (Table 6). Unfortunately, the denominators for after-hours cases, seniority of anaesthetist and extended hours of duty (>10 h) were not available for the calculation of RRs for these factors. Nevertheless, 8.1% of incidents occurred when the anaesthetist had been on duty >10 h, and 18% of incidents occurred with no specialist anaesthetist present.
A total of 45% of the incidents occurred in patients with a BMI >30 (Table 7). According to data published by the Australian Institute of Health and Welfare (AIHW) in 2017, 12 the number of men and women in Australia who were obese (BMI>30) was about 28%. If this was the prevalence in the audit population, then obesity would also be an important risk factor for airway incidents (RR>1.6). Obesity and increased difficulty with airway management was also reported in NAP4. 5 Unfortunately, the BMI denominator data were not available from the majority of participating hospitals. In the authors’ opinion, the lack of routine collection of these data has important issues for understanding its impact on airway management. We recommend that BMI should be recorded for all patients on admission to healthcare facilities in Australia and New Zealand, and that this information should be readily available for administrators and researchers.
Some degree of airway assessment was recorded in 96.4% of all incidents (Table 8). However, not all airway assessments were comprehensive (Table 8). For example, a bite test was not recorded in about 59% of incident reports, and thyromental distance was not recorded in 12.6%, neck extension in 8.1%, Mallampati score in 7.2% and mouth opening in 4.5%. It is not clear whether the absence of these tests contributed to the development of the airway incidents overall. During the qualitative assessment of the text boxes and narratives, four authors independently concluded that inadequate airway assessment and strategy had been a contributor to the development of the majority of difficult airway events. While the overall performance of airway assessment is high, the lack of comprehensive testing suggests the need for improved airway assessment education in many instances. 13
The importance of utilising nasopharyngoscopy as part of airway assessment and planned airway management strategy is exemplified by a report involving a patient with a vallecular carcinoma. 14 Preoperative nasopharyngoscopy demonstrated the lesion was partially obstructing the glottic view. An awake fibreoptic intubation was considered but the reporting personnel decided against this strategy. The anaesthetist elected to perform a spontaneous breathing induction followed by direct and indirect laryngoscopy, both of which failed. Facemask ventilation was reported as ‘manageable’. A muscle relaxant was administered and a combined approach with a second laryngoscopy by one anaesthetist and asleep fibreoptic intubation by a second anaesthetist was successful. This type of case highlights the importance of assimilating airway assessment by highly experienced anaesthetists into a comprehensive airway management strategy.
Extubation remains a common time for airway events to occur. Negative pressure pulmonary oedema (NPPO) occurred in two cases. Both cases involved young men following routine and uneventful surgery. Laryngospasm was recognised in each case on arrival at the post anaesthesia care unit (PACU). NPPO was diagnosed early and managed in the ICU with either high flow nasal oxygen (HFNO) or continuous positive airway pressure (CPAP). Both patients were discharged without any sequelae.
Several difficult airway events occurred in areas outside the operating theatre, including radiological and gastroenterology suites. The former sites commonly involved patients requiring out-of-hours emergency endovascular clot retrieval coiling. These patients frequently had either a high BMI and/or indicator of a difficult upper airway, yet were managed in a remote area by junior staff with limited difficult airway equipment and limited supervision. Similarly, airway events in gastroenterology suites were reported due to gastric aspiration (n = 6) in patients with high BMI and/or a difficult upper airway as well as several comorbidities. These results reflect the findings of Kluger and colleagues’ study and we support their recommendations for appropriate planning for emergency out-of-hours cases in off-site areas. 15 A low threshold for requesting the assistance of a second anaesthetist is recommended in such cases. We propose future studies to examine airway incidents in both radiology and gastroenterology units for strategic planning to improve patient safety.
Eight FONAs were performed during the audit period. While unplanned FONA is relatively uncommon, it is often performed during clinical scenarios that are associated with poor patient outcomes. All the FONAs during this study were performed successfully by surgeons and good patient outcomes were achieved. Two cases involved patients who had undergone uneventful drainage of submandibular abscesses. In both cases, the difficult airway events occurred at the completion of surgery when the tracheal tubes were being exchanged. This led to failed intubation attempts and eFONA by surgeons was required and successfully performed. These two cases emphasise the need for interdisciplinary airway management planning. Both patients would be expected to require intensive care ventilation for only a short period of time postoperatively. Benefits versus risks about the need of an endotracheal tube exchange need to be taken into consideration, and, if required, performed with the safest technique possible. 16 Another eFONA was performed in a patient who presented with a postoperative tonsillectomy haemorrhage. Videolaryngoscopy was unsuccessful and asleep surgical emergency tracheostomy was required. The remaining five FONAs were performed on patients with an acute upper respiratory obstruction due to pre-existing airway problems or injuries. All of these patients were successfully managed with an awake tracheostomy by an ear, nose and throat (ENT) surgeon while senior anaesthetists provided monitored anaesthetic care. It is of note that the decision to perform an awake tracheostomy in three of these five patients was guided by nasopharyngoscopy assessment of the lesions before upper airway attempts were performed.
These cases highlight the rapidity of upper airway compromise and the importance of multidisciplinary assessment and management. Previous work has focused on ongoing airway assessment and tailored airway strategies. 16 , 17 Further studies are required to refine management of this time-critical multidisciplinary task, particularly in human factor analysis.18–21 The entire operative and anaesthetic team should participate in shared ‘deliberate practice’, which is a specific type of training where the goal is to continually improve performance and patient outcomes. 22
One patient in the audit had to be taken from the ICU to the operating theatre for exploration of a bleeding tracheostomy site. The airway management was complicated by low SaO2 readings, difficult ventilation and severe hypotensive episodes (possibly due to the high ventilatory pressures required) due to a large blood clot in the lower trachea and left main bronchus. This clot was eventually removed by rigid bronchoscopy and with a good patient outcome. This case exemplifies the need for urgent surgical exploration of tracheostomy bleeding. 23
There was one death during the audit period. This involved an ASA PS 3, mildly obese patient between 60 and 70 years of age. This patient had a complex medical history and had received many previous general anaesthetics using a supraglottic airway without airway problems. This anaesthetic technique was repeated, but soon after induction there was a precipitous drop in SaO2 and high airway pressure. Multiple supraglottic attempts failed, until finally, a smaller tracheal tube was successfully inserted. However, the patient was still difficult to ventilate, suffered a cardiac arrest and could not be resuscitated. The cause of the refractory high airway pressure was not stated and the contribution of the difficult intubation to the cardiac arrest could not be determined from the narrative description. The authors thought that the airway event may have partially contributed to the death, but the primary cause was difficult ventilation. The reporting team stated that the lessons learnt included ‘not to be falsely reassured by previous anaesthetic survival’ and ‘high-risk patients remain high-risk for relatively low risk surgery’.
Although HFNO has made important inroads into normal and difficult airway management, a patent upper airway is an essential prerequisite. Oxygen desaturation may still occur in patients with complete upper airway collapse or reduced functional residual capacity (e.g. associated with a high BMI, pregnancy or sepsis).24–27 Several cases demonstrated these shortcomings of HFNO and emphasise the need of efficient airway management manoeuvres during difficult airway management and the avoidance of complacency.
While the long-term outcome of most incidents was no harm or temporary harm (65%), the immediate and final outcomes of all incidents often involved extra medical treatment or intervention, cancellation of the case, emotional distress, higher acuity postoperative care (i.e. ICU or HDU) and prolonged hospital stays (Table 9). The outcomes represent a high human and financial cost, independent of harm occurring. The incidents with permanent harm or death would have a higher human cost, mostly for the patients, but also for all personnel involved. The financial costs to hospitals and the community would also be very high. For this reason, all airway incidents should be avoided where possible, and even the low incidence recorded in this audit should still be cause for concern.
There are several recognised limitations in this audit. This study focused largely on tertiary level city hospitals and so the data may not reflect statistics in smaller metropolitan hospitals, rural and remote areas, or private institutions. However, it does provide information for hospitals that are likely to manage difficult airway issues on a frequent basis. Other limitations are inherent to any incident reporting system. These include fear of punitive action, poor understanding about what should be reported and lack of awareness of how incidents will be analysed and handled to improve patient safety. 28 We used an anonymous on-line reporting system to minimise these issues. In addition, the site coordinators at each hospital were a readily available resource to facilitate reporting. Nevertheless, it still might be possible that not all events were reported or that events with lower severity of harm were not included. The limitation in relation to the absence of denominator data from several hospitals has already been mentioned. As with any audit, the evaluated data only apply mostly to 12 hospitals participating. The extent to which the findings are ‘generalisable’ to other hospitals would depend on their similarity in relation to case mix and anaesthesia care delivery to these 12 hospitals.
Conclusion
This audit has provided a description of airway incidents in 12 tertiary level hospitals across Australia and New Zealand. The findings represent an up-to-date snapshot of airway incidents in typical Australian and New Zealand hospitals with a view to identifying areas that require improved strategic planning for patient care. Despite advances in airway equipment technology and education, airway incidents continue to occur, with their attendant human costs and resource implications. Based on the authors’ assessment of the reports of these events, the areas requiring particular attention include the importance of integrating airway assessment with its decision-making and improving airway management strategies for head and neck surgery, gastric regurgitation, obesity, inadequate assistance and unexpected difficult airway management in off-site areas.
Footnotes
Acknowledgments
The authors acknowledge the contribution and support of current and past Airway Special Interest Group members. Leading site coordinators for this audit include (alphabetical order): Anton Booth, Pierre Bradley, Gordon Chapman, Sheila Hart, Drew Heffernan, Greg Houghton, Gerri Khong, Michal Kluger, Gene Lee, Kian Lim, Adam Rehak, James Sartain, Reny Segal, Brian Spain, Kris Usher and Eldon Ward. Their invaluable efforts were key to the quality of this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed no financial support for the research, authorship, and/or publication of this article.