
Abstract
Massive transfusions guided by massive transfusion protocols are commonly used to manage critical bleeding, when the patient is at significant risk of morbidity and mortality, and multiple timely decisions must be made by clinicians. Clinical decision support systems are increasingly used to provide patient-specific recommendations by comparing patient information to a knowledge base, and have been shown to improve patient outcomes. To investigate current massive transfusion practice and the experiences and attitudes of anaesthetists towards massive transfusion and clinical decision support systems, we anonymously surveyed 1000 anaesthetists and anaesthesia trainees across Australia and New Zealand. A total of 228 surveys (23.6%) were successfully completed and 227 were analysed for a 23.3% response rate. Most respondents were involved in massive transfusions infrequently (88.1% managed five or fewer massive transfusion protocols per year) and worked at hospitals which have massive transfusion protocols (89.4%). Massive transfusion management was predominantly limited by timely access to point-of-care coagulation assessment and by competition with other tasks, with trainees reporting more significant limitations compared to specialists. The majority of respondents reported that they were likely, or very likely, both to use (73.1%) and to trust (85%) a clinical decision support system for massive transfusions, with no significant difference between anaesthesia trainees and specialists (P = 0.375 and P = 0.73, respectively). While the response rate to our survey was poor, there was still a wide range of massive transfusion experience among respondents, with multiple subjective factors identified limiting massive transfusion practice. We identified several potential design features and barriers to implementation to assist with the future development of a clinical decision support system for massive transfusion, and overall wide support for a clinical decision support system for massive transfusion among respondents.
Introduction
Major bleeding can occur in any surgical, trauma, obstetric, or medical patient and often requires large volumes of blood products, termed massive transfusion (MT). 1 The definition of MT varies but can be defined as the administration of five or more units of red blood cells in less than four hours. 2
Resuscitation using an MT remains difficult to manage, requiring vast amounts of hospital resources, often urgently and unexpectedly, and similar to other resuscitation scenarios places significant stress on hospital staff and impedes decision-making. 3 , 4 To facilitate this, institutions commonly adopt massive transfusion protocols (MTPs), which may assign roles, prescribe communication pathways, specify the type and quantity of blood products to be transfused, and provide guidance on further assessment of bleeding, markers of successful resuscitation and ongoing management specific to the cause of the bleeding. 5 MT often occurs in the context of surgery, 6 therefore anaesthetists are pivotal to this process, as they manage multiple concurrent processes and make time-critical decisions.
Current haemorrhage guidelines recommend laboratory assessment at regular intervals to guide transfusion decision-making and to detect coagulopathy.7–9 The slow turnaround time and incomplete assessment of coagulation by conventional assays (for example, activated partial thromboplastin time and fibrinogen) limits their utility in rapidly changing resuscitation scenarios. 10 To reduce the delay inherent in laboratory-based coagulation assessments, point-of-care (POC) viscoelastic haemostatic assays (VHAs) such as thrombelastography (Haemonetics, Braintree, MA, USA) and rotational thromboelastometry (ROTEM; TEM International GmbH, Munich, Germany) are now available to guide the assessment of coagulopathy and management of MT. 11 However, compared to standard coagulation tests, these tests increase the number of parameters available and/or results used by clinicians to guide decision-making. 12
Although many institutions have implemented algorithms to guide the use of VHAs for transfusion decision-making in dynamic haemorrhage scenarios, there is a lack of good quality evidence to support them. 13 A computerised clinical decision support (CDS) system is software designed to assist decision-making by comparing patient information against a knowledge base to generate patient-specific assessments or recommendations. 14 Studies examining these systems have demonstrated improved clinical outcomes in a number of emergency scenarios, such as trauma resuscitation and blood transfusion, to help clinicians make treatment decisions based on the best available evidence. 15 , 16
The multicentre Implementing Treatment Algorithms for the Correction of Trauma Induced Coagulopathy (iTACTIC) trial is due to report its findings soon. 17 It will compare the effect of VHA-guided trauma resuscitation with conventional trauma resuscitation on patient outcomes, and potentially provide evidence for rule-based or algorithmic decisions in MT. Given that CDS systems have not yet been examined in the context of MT, successful design and implementation will be influenced by a number of factors. These are likely to include prior MT experience, institutional MTP structure, the availability of laboratory testing and whether clinicians will use such a system if available. While this information may help establish the context of possible MT CDS system implementation, the influence of these factors will require careful consideration during both the design and implementation of a future MT CDS system.
The aim of this study was to investigate the MT practice of Australian and New Zealand anaesthetists, perceived obstacles to optimal care and attitudes towards CDS systems. The results of this survey will also be used to guide the design of a CDS system for MT by identifying potential features such as automated laboratory result interpretation in the context of MT aetiology. This study will also identify potential barriers to implementation by identifying subjective limitations and exploring participant experiences.
Methods
To explore the experiences and attitudes of anaesthetists towards MT and CDS systems, an online survey was conducted. The study was approved by Western Sydney Local Health District Human Research Ethics Committee (2019/ETH12247). Participation was voluntary, and consent was implied by completion of the survey. We have provided a checklist for reporting results of internet E-surveys (CHERRIES) checklist, as recommended by the Enhancing the Quality and Transparency of Health Research (EQUATOR) network. 18
The survey was designed in consultation with clinicians from a broad range of relevant disciplines, and was piloted with ten anaesthetists and anaesthetic trainees in our department to ensure intelligibility, minimise bias, and limit the burden to less than 20 questions in ten minutes.
The survey was approved by the Australian and New Zealand College of Anaesthetists (ANZCA) and was distributed to a random sample of 1000 out of their 5658 registered anaesthesia specialists and 1597 trainees across Australia and New Zealand, in public and/or private practice. The ANZCA Clinical Trials Network (CTN) facilitates surveys distributing invites to a stratified random sample of up to 1000 participants to minimise survey fatigue. In October 2019, the ANZCA CTN correspondingly distributed invitations to participate by email. The CTN sent two reminder emails over the following two months. SurveyMonkey (Portland, OR, USA) was used to construct the survey and collect results.
The survey consisted of 17 questions (see Supplementary Appendix 1, available online), eight of which allowed open-ended, free-text responses, and covered the following four areas:
demographics and MT experience (sex, years of clinical experience, region of practice, MTP experience, transfusion-related education) to create a snapshot of currently practising anaesthesia providers; availability of hospital services relevant to MT (hospital size and specialties, MTP and laboratory and POC test availability); factors preventing optimal care; and attitudes towards CDS systems (preferred communication and information display mediums, desired information during MTP, likeliness to use and trust a MT CDS system).
Other major surgery was defined as non-cardiac/non-transplant major surgery.
Data analysis
Survey results were summarised and analysed using the chi-square (χ2) or Fisher’s exact test when appropriate for exploratory analysis, with statistical significance considered to be P < 0.05. Statistical analyses were performed using SPSS (version 25; IBM Corp., Armonk, NY, USA). Open-ended responses were analysed thematically by one author (BJS). Responses were categorised until saturated.
Results
Of the 1000 surveys, 968 were successfully distributed by email (32 potential respondents were removed following randomisation but prior to distribution, including 29 who unsubscribed from survey participation and three whose emails bounced). Of these 968 surveys, 228 were successfully completed (23.6% completed response rate). One respondent was retired at the time of survey completion and was removed from analysis, therefore 227 survey responses were analysed. Respondents were similar with respect to sex and practice location when compared to active ANZCA trainees and specialists across Australia and New Zealand (see Supplementary Appendix 2).
Demographics and massive transfusion experience
Most respondents (83.3%) were anaesthesia specialists, of whom 91.5% had over ten years of clinical experience and 55% had over 20 years of clinical experience (Table 1). There was no significant difference in MTP involvement between trainees and specialists (P = 0.31). A minority of overall respondents (20.7%) had not been involved in an MT in the past 12 months, while only 11.9% had been involved in more than five MTs in the same period. Most respondents (70.1%) had completed a transfusion-related educational or training course in the past two years. Only 12.8% were unsure or stated that they had not previously completed any course, the majority of whom were trainees (44.8%) compared to a small number of specialists (6.3%).
Respondent demographics (n = 227).
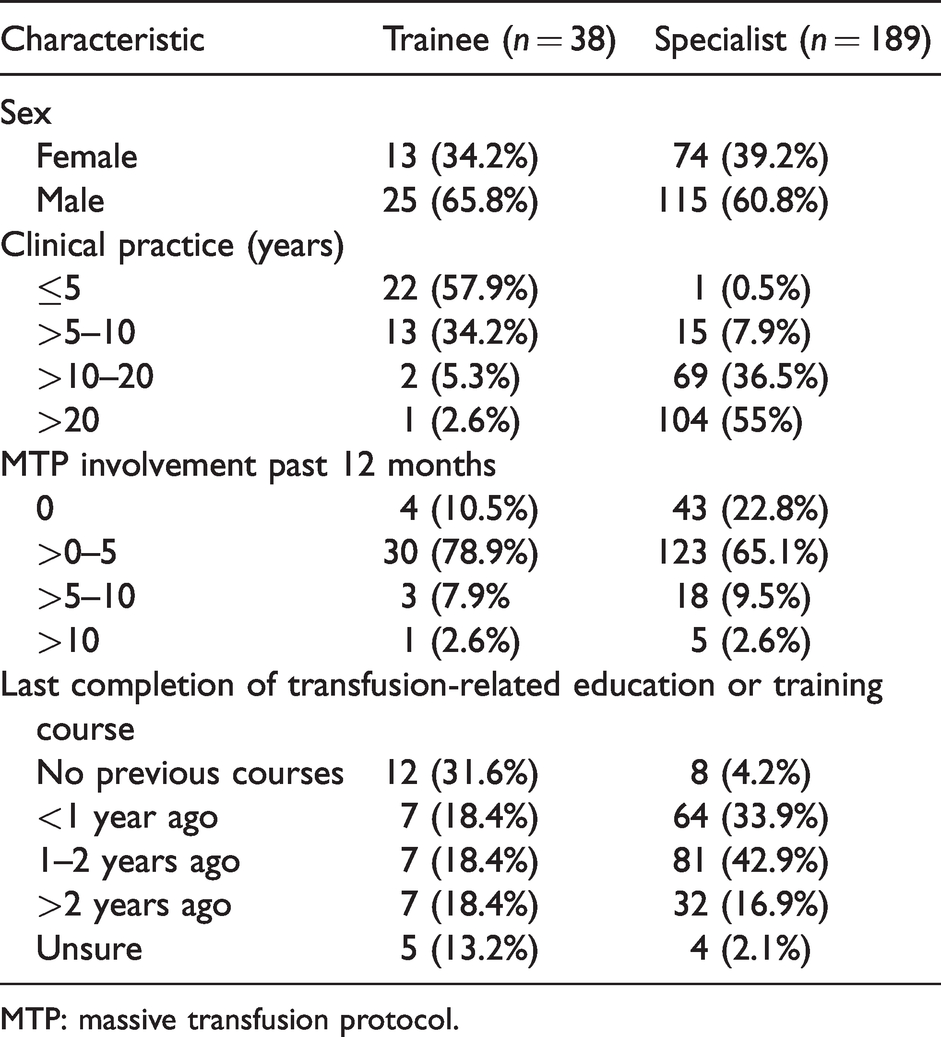
MTP: massive transfusion protocol.
Availability of hospital services relevant to massive transfusion
The majority of respondents (71.3%) reported working in a hospital with 250 or more inpatient beds; only two respondents reported working in a hospital with less than 50 beds (Table 2). The three most common specialties available at each respondent’s hospital were gastrointestinal surgery (93.8%), other major surgery (82.4%) and obstetrics (81.5%). Most respondents (90.9%) reported having an MTP at their hospital, with 24.1% having multiple MTPs and 32.6% having MTPs which were guided by VHAs. Arterial blood gas analysis was the most commonly available POC test (of relevance to MT), both inside (69.6%) and outside (63.4%) the theatre complex. Both thrombelastography and ROTEM were more commonly available inside the theatre complex than outside it (38.3% versus 7.5%, respectively, for thrombelastography and 26.9% versus 19.4%, respectively, for ROTEM).
Respondent hospital characteristics (n = 227).
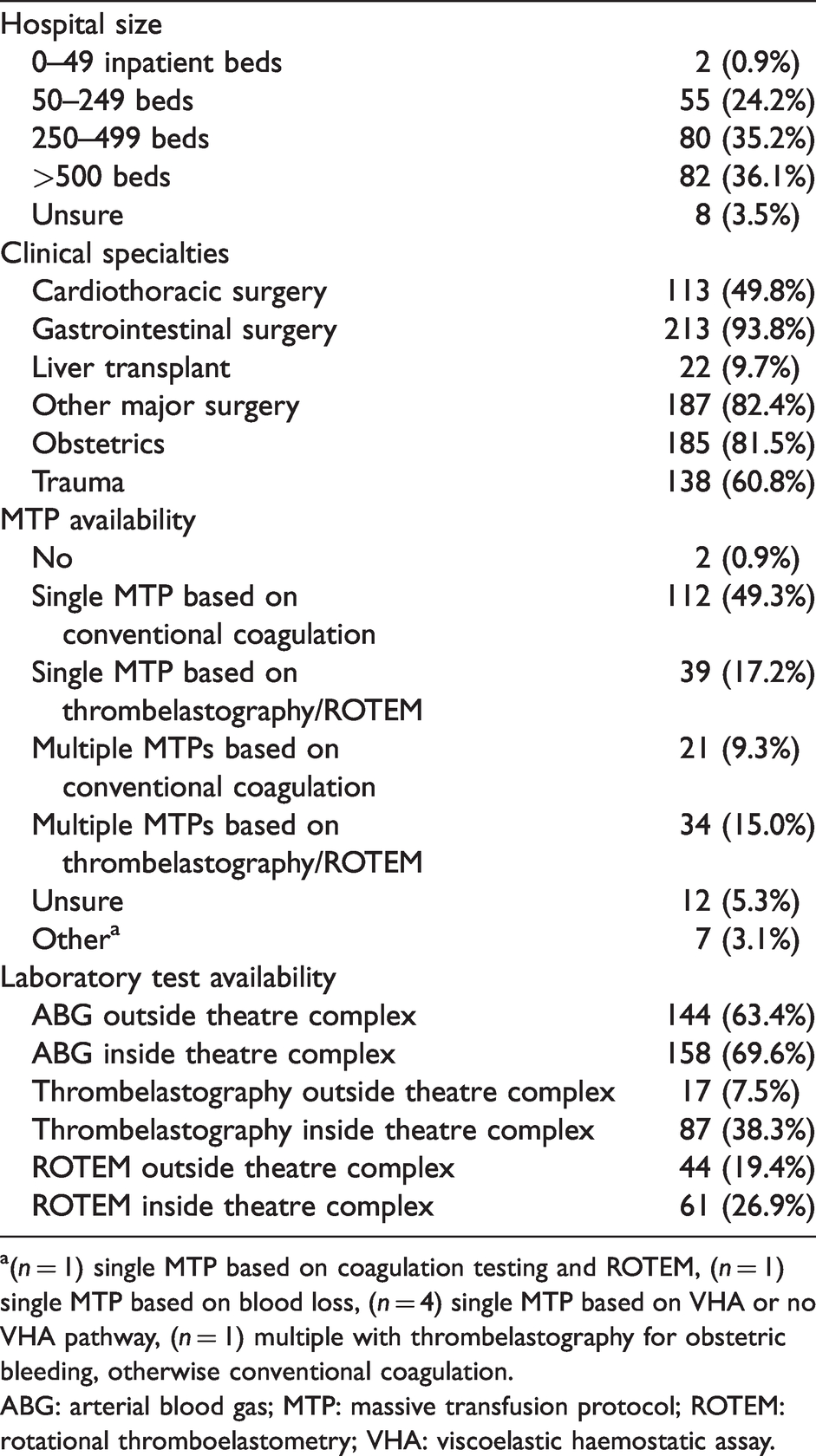
a(n = 1) single MTP based on coagulation testing and ROTEM, (n = 1) single MTP based on blood loss, (n = 4) single MTP based on VHA or no VHA pathway, (n = 1) multiple with thrombelastography for obstetric bleeding, otherwise conventional coagulation.
ABG: arterial blood gas; MTP: massive transfusion protocol; ROTEM: rotational thromboelastometry; VHA: viscoelastic haemostatic assay.
Factors preventing optimal care
Reported limitations to the effective and efficient conduct of MT are shown in Figure 1. The three most frequent factors overall that were felt strongly by respondents to constrain MT management were access to POC coagulation assessment (18.9%), multiple competing tasks (16.7%) and timely access to clinical information (13.2%). Compared to specialists, trainees perceived a higher severity for each factor to limit their conduct of MT, with all except timely access to clinical information and logistical issues reaching statistical significance (see Figure 1). Most respondents overall (67%) did not perceive their transfusion knowledge and decision-making to limit their conduct of MT. Another limitation identified by some respondents on open response was the limited availability of blood products, particularly platelets, in smaller institutions.
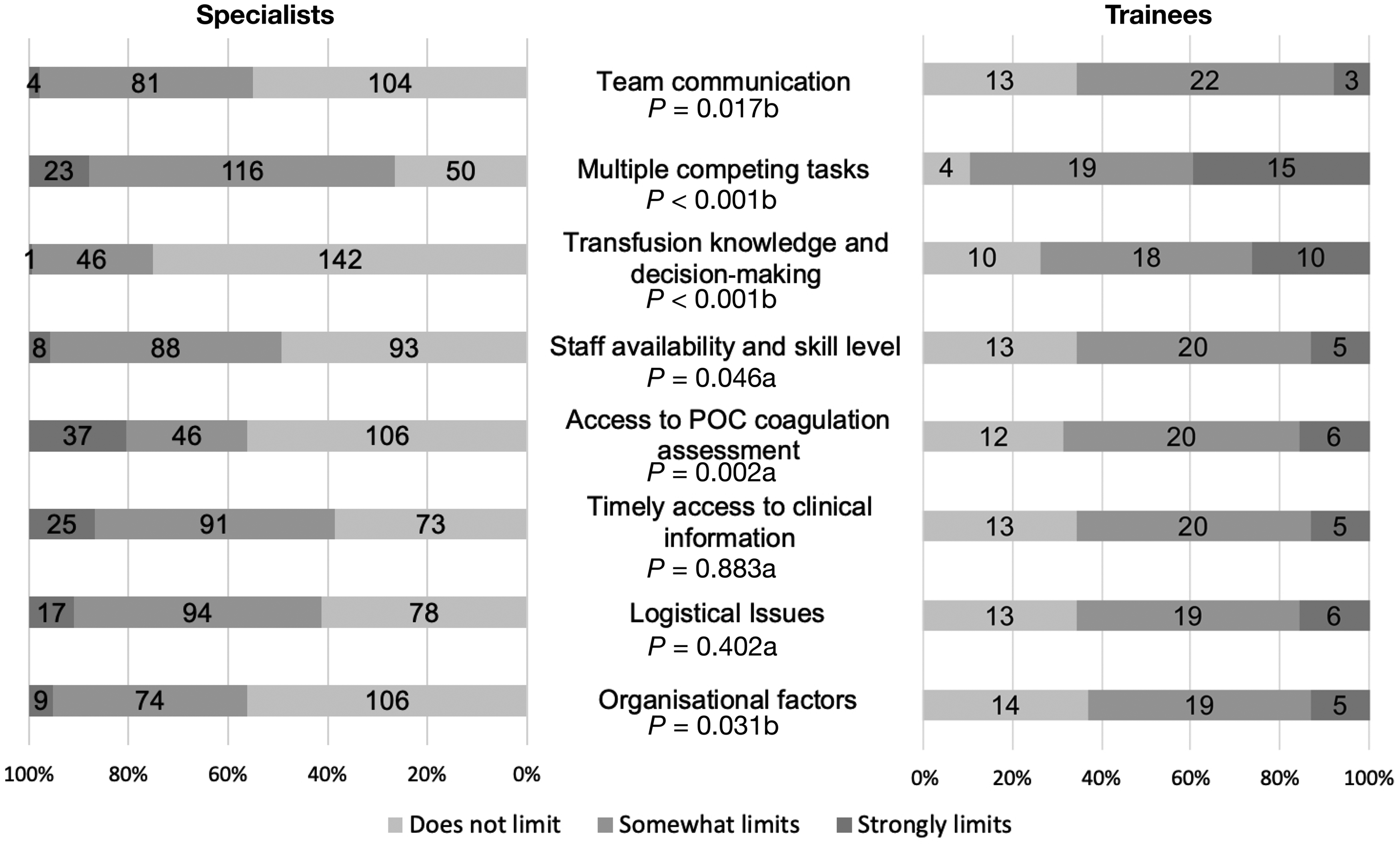
Perceived limitations to effectively and efficiently conducting massive transfusion. POC: point-of-care; n: number of respondents; a: chi-square; b: Fisher’s exact test; P-values represent a comparison between specialists and trainees for each limiting factor.
Attitudes towards decision support systems
The majority of overall respondents preferred to communicate with the hospital blood bank or haematologist by voice using either a mobile phone (50.2%) or telephone (39.2%), with no significant difference between specialists and trainees (P = 0.315) (Table 3). The majority of respondents also desired to have live results of thrombelastography/ROTEM with transfusion recommendations (81.5%), tally of blood products transfused (79.3%), antiplatelet or anticoagulant reversal guidance (70.9%), and laboratory results in the context of guideline targets (70%) immediately available. Compared to specialists, more trainees (71.1% versus 53.4%, χ2 3.991, P = 0.046) preferred a current transfusion ratio to be available, and 63.2% of trainees versus 40.7% of specialists (χ2 6.438, P = 0.011) preferred a computerised MTP flowchart showing the current situation to be immediately available. The majority of respondents preferred this information to be communicated visually using graphical/trends (70%) and text/numbers (59.5%), with a similar preference between trainees and specialists. The majority of respondents reported that they were likely, or very likely, both to use (73.1%) and to trust (85%) a theoretical CDS system for MT, with no statistically significant difference between trainees and specialists (χ2 0.787, P = 0.375 and χ2 0.119, P = 0.73, respectively).
Respondent attitudes and preferences for decision support (n = 227).
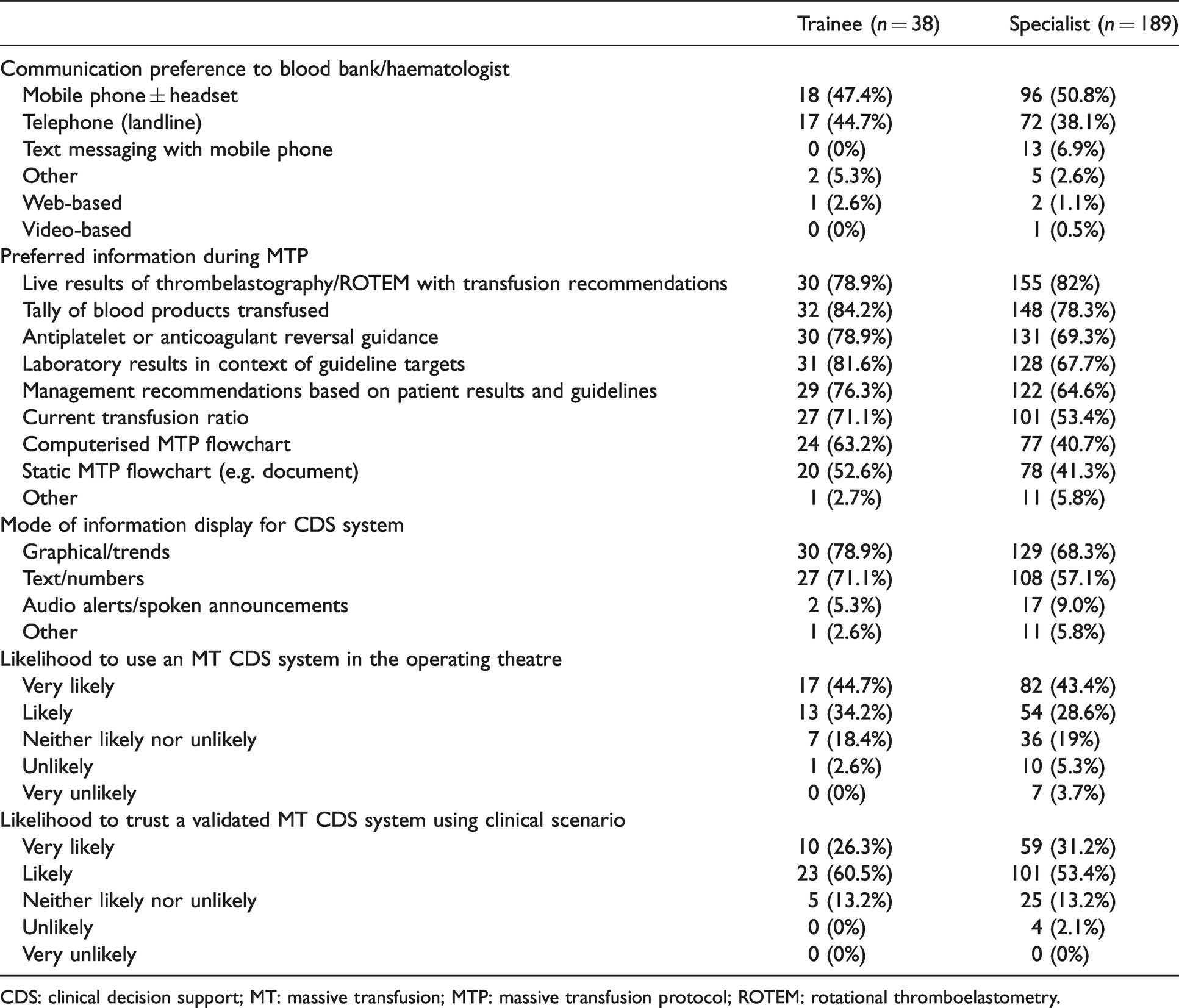
CDS: clinical decision support; MT: massive transfusion; MTP: massive transfusion protocol; ROTEM: rotational thromboelastometry.
Thematic analysis
Free-text comments about decision support for MT were made by 54 (23.8%) respondents, including seven trainees. Thematic analysis divided the comments into suggestions, concerns and general comments, as shown in Table 4. Respondents were generally supportive of CDS systems for MT but some were concerned about its role in these inherently complex scenarios:
Thematic analysis of survey comments.
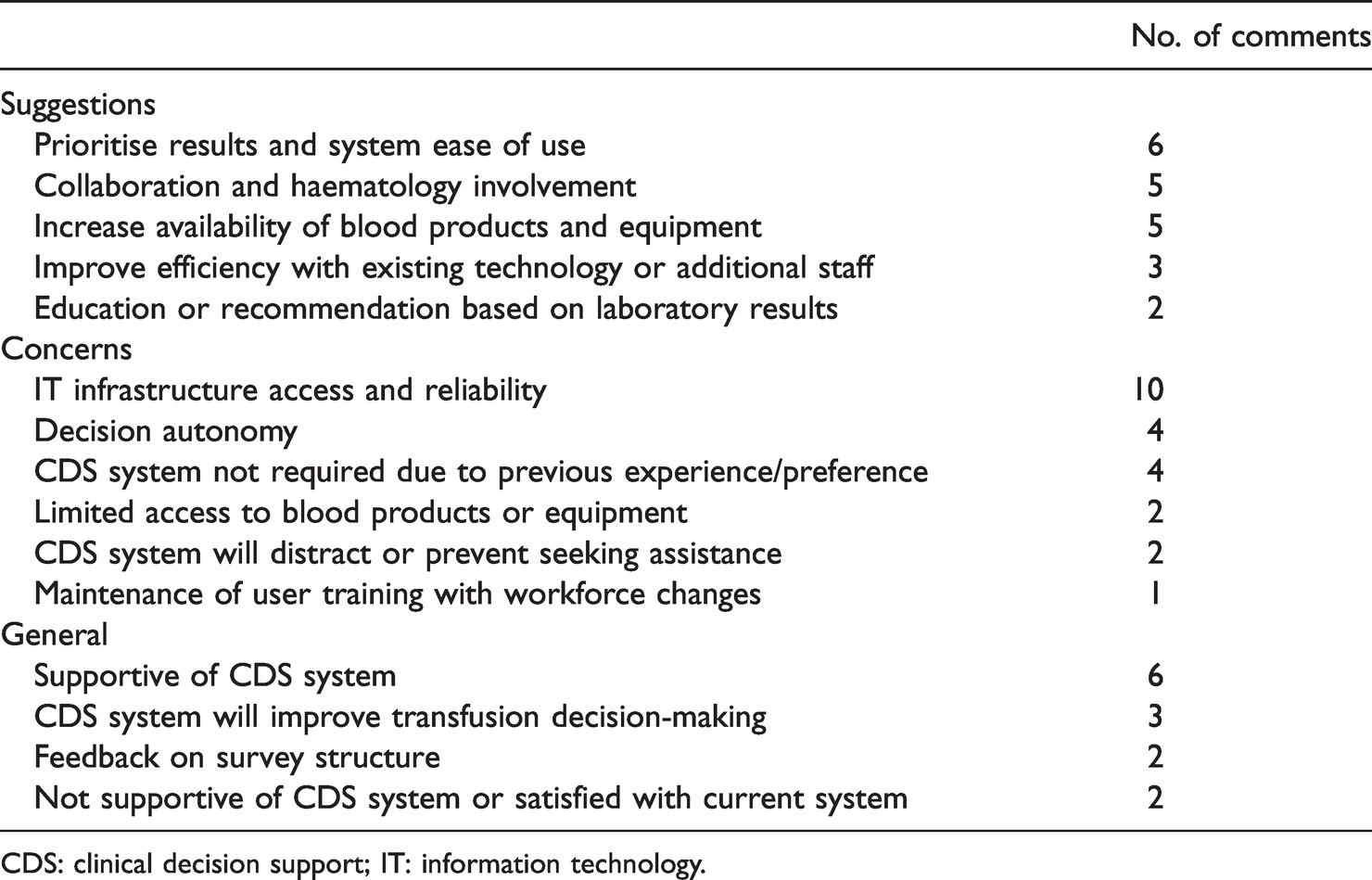
CDS: clinical decision support; IT: information technology.
They would have to be recommendations only as it is difficult to put all of the clinical situation information in as it evolves so rapidly in these scenarios.
There were also concerns about access to and reliability of computer infrastructure: Reliability of computer systems and access is a huge barrier including wifi and cellular accessibility.
This represents a separate but important issue for successfully implementing any CDS system where software is only as useful as the infrastructure that supports it.
Discussion
While the response rate to our survey was poor, there was still a wide range of MT experience among respondents, with multiple subjective factors identified limiting MT practice. We also identified several potential design features and barriers to implementation to assist with the future development of a CDS system for MT, and overall wide support for a CDS system for MT among respondents.
The respondents were predominantly anaesthesia specialists with more than five years of clinical experience. Interestingly, despite almost three-quarters of respondents working in a hospital with more than 250 beds, experience with massive bleeding events was low, with 88.1% of respondents having conducted five or fewer MTPs in the past 12 months and over 20% of respondents recalling having conducted no MTPs in the past 12 months. This indicates that, on average, MT is a relatively rare event for an individual anaesthetist, particularly specialist anaesthetists, in Australia or New Zealand. However, 70% of respondents had completed a transfusion-related course in the past two years and so most were reasonably up to date with current practice and guidelines in this field.
MTPs are implemented almost universally at respondent hospitals, with only two respondents not having an MTP available and 12 respondents being unsure. The availability of POC (of relevance to MT) inside the theatre complex was low, with only 69.6% of respondents having access to blood gas analysis and a minority of respondents having access to thrombelastography or ROTEM (38.3% and 26.9%, respectively). The limited availability of thrombelastography and ROTEM may reflect that VHAs are not yet part of most Australian or New Zealand MTPs; nevertheless their use is recommended by international transfusion guidelines.7–9, 19 This may also support facilitated access to laboratory results to reduce time delays when POC laboratory testing is not available. Communication preferences of trainees and specialists were firmly in favour of voice-based technologies, with almost 90% of all respondents preferring either telephone or mobile phone–based communication. The strong preference for voice-based communication would potentially limit the role of electronic messaging as part of a CDS system for MT.
Cognitive load and decision support
Clinical teams encounter many problems during MT. The nature and severity of these problems may vary depending on the institution, the clinical scenario, the individual staff involved, and even the time of day. Clinicians managing MT have to deal with multiple competing tasks and limited access to vital information. Effective MT management depends on clear communication and the completion of several tasks in a coordinated manner. It may be supported in a number of ways, and this has traditionally been addressed through increased education and training, simulation and the revision of clinical workflows. The practical application of guidelines, protocols, cognitive aids or algorithms through the use of a CDS system may help in these scenarios. However, high task complexity has been shown to reduce the utility of CDS systems and therefore must be implemented with care. 20 This point was reflected by one respondent who ‘would use the system to support but not direct [their] decision-making’. Cognitive aids in particular require education and familiarity to maximise efficacy. 21 They are also often static and difficult to apply in scenarios with multiple variables, and have been shown to reduce team communication. 21 Efforts to apply an algorithmic approach to transfusion decision-making have focused mainly on computerised physician order entry systems. These systems apply rule-based prompts to support the appropriate transfusion of blood products with haemoglobin cut-offs for red blood cell transfusions. 22 They have been shown in the non-MT context to reduce blood product wastage and in some scenarios to improve patient outcomes. 23 Extending this approach to MT in the form of a dynamic CDS system may multiply this benefit, as several time-critical transfusion decisions need to be made simultaneously or in quick succession. 24
Decision support for massive transfusion
Our survey demonstrates a desire for expedited delivery of laboratory results in MT, and for a dynamic, evidence-based MT CDS system, especially among trainee respondents. Previous work on decision support for complex tasks identified that, with increasing complexity, experienced clinicians desire information rather than decision support. 25 Visual attention is limited and noise pollution is high during emergency situations, so it is essential to convey this information in the optimal manner. 26 Visual display was overwhelmingly preferred by respondents, and the value of auditory signals was questioned. Successful implementation of such an approach relies on clinician engagement. The majority of respondents to our survey were likely both to use and to trust a hypothetical CDS system for MT. The increasing use of information technology–based solutions to clinical problems makes reliability a critical issue. This concern was raised by a number of our survey respondents and is a common experience of many clinicians. 27
Strengths and limitations
This survey invited the participation of a large random selection of ANZCA-registered anaesthesia specialists and trainees across two countries. The response rate of 23.6% raises the possibility of participation bias. Despite this, assessment of available respondent demographics showed a close match to anaesthesia providers more generally in Australia and New Zealand (Supplementary Table 1). The majority (70%) of participants having recently completed transfusion-related education may represent a response bias. Invited participants with an interest in CDS systems may have also been more likely to participate, further compounding the responder bias. All inferential statistics were exploratory in nature and would require confirmation in subsequent studies. To our knowledge, the survey is also the first of its kind to examine anaesthetist attitudes towards CDS systems in the context of MT.
This binational survey of anaesthesia providers has shown that individual respondent experience of MT is often limited, and that there are common subjective factors preventing efficient management. Use of a theoretical CDS system for MT was supported by the majority of respondents, who also provided information to guide design and overcome implementation barriers for a CDS system for MT. Given the complexity and variability of clinical scenarios involving MT, the development of a CDS system for MT will require a careful and considered approach that engages clinicians across a broad range of MT experience.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X20974035 - Supplemental material for Massive transfusion experience, current practice and decision support: A survey of Australian and New Zealand anaesthetists
Supplemental material, sj-pdf-1-aic-10.1177_0310057X20974035 for Massive transfusion experience, current practice and decision support: A survey of Australian and New Zealand anaesthetists by Brenton J Sanderson Jeremy D Field Lise J Estcourt Erica M Wood Enrico W Coiera in Anaesthesia and Intensive Care
Supplemental Material
sj-pdf-2-aic-10.1177_0310057X20974035 - Supplemental material for Massive transfusion experience, current practice and decision support: A survey of Australian and New Zealand anaesthetists
Supplemental material, sj-pdf-2-aic-10.1177_0310057X20974035 for Massive transfusion experience, current practice and decision support: A survey of Australian and New Zealand anaesthetists by Brenton J Sanderson Jeremy D Field Lise J Estcourt Erica M Wood Enrico W Coiera in Anaesthesia and Intensive Care
Footnotes
Acknowledgements
The author(s) would like to thank the Australian and New Zealand College of Anaesthetists for distributing the survey.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: EMW is supported by a National Health and Medical Research Council investigator grant (1177784). BJS received funding for this research through the project grant and scholarship (20/014) from the Australian and New Zealand College of Anaesthetists and a scholarship offered by Australia’s National Blood Authority (ID410).
Supplemental material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.