
Abstract
Accidental extubation in the prone position is a medical emergency in which quick and low resource demanding airway management is required. Regaining oxygenation is the primary goal, but sometimes intubation may be required to regain oxygenation. Blind intubation through an i-gel® (Intersurgical Ltd, Wokingham, Berkshire, UK) may be a quick and low resource demanding method. However, the success rate of the use of an i-gel as an intubation conduit in the prone position is unknown. This was a prospective study in patients scheduled for lumbar surgery. General anaesthesia was induced in the prone position and an i-gel was inserted. After successful ventilation, up to three attempts at intubation using a VivaSight-SL single-lumen tube (Ambu A/S, Ballerup, Denmark) were performed. The first attempt was blinded for the operator and the patient’s head was in a neutral position. The second attempt was blinded for the operator with the patient’s head rotated laterally. The third attempt was on-screen and allowed various manoeuvres to facilitate intubation. A success rate of 70% was deemed clinically acceptable. The study was terminated early after 14 subjects because the success rate of 70% was not achievable. However, ventilation using the i-gel in the prone position was successful in 13 patients (93%). Intubation was successful in only one patient at the first attempt, one patient at the second attempt and three patients at the third attempt. Overall, the success rate was 36%. Blind intubation using an i-gel as an intubation conduit in the prone position is not recommended.
Netherlands Trial Register number NL6387 (NTR7659).
Background
Accidental extubation in the prone position is a medical emergency.1,2 Turning the patient to a supine position may not be readily possible, making airway management in the prone position mandatory. The primary objective of airway management is to achieve oxygenation, but tracheal intubation might be necessary (e.g. in patients requiring high positive airway pressures). Advanced airway instruments for intubation in the prone position are unlikely to be immediately available at the bedside (i.e. are stored in a more central location). This means that initial attempts at intubation may be required with equipment that is directly available, while the advanced instruments are obtained. Initial attempts should not delay or impede subsequent airway management and should be quick and low resource demanding.3 Insertion of a supraglottic airway device (SAD) should be considered, but this may not achieve sufficient oxygenation in patients requiring high airway pressures or in patients with nasogastric tubes due to the increased leakage.4
Blind intubation through an SAD may meet these requirements. Multiple types of SADs are available, including the i-gel® (Intersurgical Ltd, Wokingham, Berkshire, UK). The i-gel is an SAD that can be inserted within ten seconds in the prone position and facilitates airway establishment.5,6 In the prone position, mean airway seal pressures with the i-gel of 25 to 28 cmH2O are reported, which is comparable to other SADs.6,7 The i-gel is not specifically designed for blind intubation, unlike some other SADs, but its use as a blind intubation conduit has been reported in the supine position (but not the prone position), resulting in an intubation rate of 80%.8,9 The perceived advantage of using an i-gel over other SADs is the reduced time to insertion, given the absence of a need to inflate a cuff.
This study investigates whether the i-gel can be used as an intubation conduit in the prone position. We consider an intubation rate of 70% within one minute to be the minimum that would be clinically acceptable. In this study a VivaSight-SL single-lumen tube (Ambu A/S, Ballerup, Denmark) was used instead of a standard endotracheal tube for safety measures. In addition, only patients without signs of a difficult airway were eligible.
Methods
The study was designed as a prospective observational cohort study. Ethics approval was obtained by the Medical Ethical Committee of Southwest Holland (NL65936.098.18/18-063). Patients provided written informed consent prior to participation. The study was registered in the Netherlands Trial Register as NL6387 (NTR7659).
Participants
The study recruited subjects between February 2019 and July 2019. Patients scheduled for lumbar surgery lasting less than 60 minutes were considered eligible for participation. Exclusion criteria were body mass index (BMI) greater than 32 kg/m2, edentulous state, a mouth opening less than 3 cm, professional voice usage, or an increased aspiration risk (not fasted or hiatus hernia).
Study protocol
After the time out procedure, the patient positioned him or herself in the prone position. The head was rested on the surgical table, rotated to the preferred side of the patient. The arms were positioned in the ‘surrender position’. After confirmation of a comfortable position for the patient, pre-oxygenation was started. Anaesthesia was induced with propofol 2 mg/kg and remifentanil 50 µg and maintained with continuous infusions of propofol and remifentanil. When consciousness was lost, an i-gel SAD size 4 or 5 was inserted. Correct positioning of the i-gel was confirmed by obtaining end-tidal carbon dioxide (CO2) and a leakage volume less than 100 ml per breath. Ventilation was started with volume control, the settings were a tidal volume of 6 ml/kg and zero positive end-expiratory pressure (PEEP).
Mivacurium 0.2 mg/kg was administered for muscle relaxation and intubation was attempted with a pre-warmed and lubricated VivaSight-SL single-lumen tube, size 7.0, with the head in a neutral position and held slightly upward by the nurse anaesthetist. The nurse anaesthetist was able to view the monitor and was instructed to inform the anaesthesiologist to stop the attempt if harm was imminent (e.g. bleeding or arytenoidal dislocation). The anaesthesiologist who performed the intubation was not able to see the monitor on this attempt. After insertion of the tube, the cuff was inflated and a test breath was performed. If end-tidal CO2 was obtained or the video screen showed the tracheal lumen, tracheal placement was confirmed and the study ended. If tracheal intubation was unsuccessful, a second attempt was performed.
The second attempt was similar to the first, except for the head position, which was rotated to one side. If the second attempt was successful, the study was ended. If tracheal intubation was unsuccessful, a third attempt was performed.
The third attempt used on-screen visualisation. The anaesthesiologist was instructed to use the view obtained by the VivaSight-SL single-lumen tube and was allowed to use any manoeuvre or a gum elastic bougie to facilitate tracheal intubation. If this attempt was successful, the study ended and surgery began. If the attempt was unsuccessful, the study ended and the patient was either placed in the supine position for intubation or the procedure started without intubation using the i-gel for ventilation. Only when the correct position of the i-gel or VivaSight-SL single-lumen tube was confirmed, was the patient’s bed placed outside the theatre.
Data collection
The data were collected during the study by an independent observer. Baseline characteristics consisted of American Society of Anesthesiologists (ASA) Physical Status classification, height, weight, gender, age, mouth opening distance, thyromental distance and neck circumference. The duration of each manoeuvre, plateau pressures, leakage volume, glottic view, reasons for failure of intubation and the manoeuvres used during the third attempt were noted. When awake, the patient was asked about dysphonia, soreness of the throat or any other complaints.
Outcomes
The primary outcome was the successful intubation rate over the three attempts. The secondary outcomes were the success rate and time to insertion of the i-gel, the leakage volume and plateau pressure when ventilated using the i-gel, the number and duration of intubation attempts, the reasons for failure, and postoperative symptoms.
Sample size calculation and statistics
A success rate of 70% was considered clinically acceptable, as explained in the introduction. The sample size was determined at 50 subjects, as no previous data were available. A total of 50 subjects would yield a 95% confidence interval of ±12%, which we regarded acceptable for an explorative study. Data are presented as number (%) or median (interquartile range; IQR).
Results
Although it was planned to recruit and study 50 patients the study was terminated early after 14 patients, because the clinically acceptable intubation rate of 70% was no longer achievable. The secondary target of time to intubation of less than one minute was also unlikely to be achieved, because in most of the 14 patients a third intubation attempt was required. At this stage 73 patients had been screened, of whom 18 fulfilled the exclusion criteria, 31 declined participation and ten were excluded for logistic reasons.
Six of the 14 (43%) patients were men. The median age of the participants was 55 (IQR 48–62) years, with a median BMI of 26.3 (IQR 25.4–27.6) kg/m2. Eleven patients (79%) were classified as ASA class 2 and three (21%) as ASA class 3. No participants had signs of a difficult airway, as the median mouth opening distance was 5 (IQR 4.5–5) cm, the median thyromental distance was 9 (IQR 8–10) cm and the median neck circumference was 37 (IQR 36–41) cm.
Overall, five of the 14 participants could be intubated (36%). Table 1 displays the results of the secondary outcomes. Ventilation using an i-gel in the prone position was successful in 13 patients (93%). The first blind attempt of intubation was successful in one of these 13 patients and the second blind attempt was successful in one of the 12 remaining patients. In eight patients, no glottic view was visible by the VivaSight-SL tube. The glottic view was scored as a Cormack–Lehane score of 1 in four patients, and 4 in one patient. Reasons for unsuccessful blind attempts were oesophageal intubation (n = 3), blocking of the epiglottis (n = 2), and unable to pass the i-gel (n = 3). and The reasons were unclear in three patients. In order to intubate the patient successfully at the third attempt, a retraction of the i-gel of approximately 1–2 cm, rotation of the tube and cricoid pressure was needed in all three patients. However, these manoeuvres were also used in the unsuccessful eight patients.
Secondary outcomes.
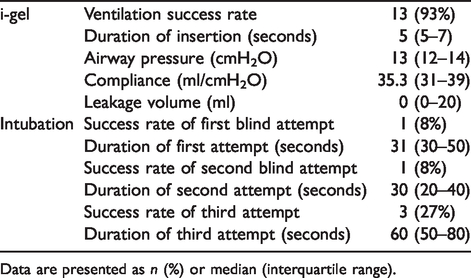
Data are presented as n (%) or median (interquartile range).
Discussion
This study ended prematurely because a clinically acceptable outcome of a successful intubation rate of 70% was no longer achievable. Most attempts for blind or on-screen intubation through the i-gel were unsuccessful and lasted over one minute. However, the insertion of an i-gel in the prone position was quick and successful in most patients. This study shows that the insertion of an i-gel in emergency situations in the prone position may be considered, but blind intubation is unlikely to be successful.
Patients with potentially difficult airways were excluded from this study, which leads to a selected cohort. One can expect that in regular clinical practice, successful intubation rates would be even lower. Therefore, we may also have overestimated the success rate of insertion of the i-gel in clinical practice. In addition, patients in the intensive care unit often have a gastric tube inserted, which could lead to a higher failure rate of ventilation through an i-gel. Therefore, the rate of successful ventilation using the i-gel should be interpreted with caution.
Studies and case reports demonstrated that an i-gel may be considered as an intubation conduit in the supine position.3,8–12 Manikin studies investigating the success rate of using an i-gel as an intubation conduit found conflicting results.13,14 Our study demonstrates that in the prone position one should not rely on an i-gel as an intubation conduit. Furthermore, this study demonstrates that results obtained in the supine position and in manikins cannot be extrapolated to the prone position.
We believe that the technique of using an SAD as an intubation conduit in the prone position should only be investigated as a rescue method in emergency settings, when no advanced materials are available. This is in line with the belief that blind intubation is rarely a solution.15 Furthermore, it may cause airway trauma, which hampers subsequent intubation. However, one cannot expect to have all the equipment readily available for rare situations. In such a case, the use of an SAD as a blind intubation conduit has the benefit of needing few advanced resources and little physician experience. Therefore, a proper evaluation in a controlled clinical situation was warranted, especially as manikin-based studies have shown a high success rate.13 Because of the design of an i-gel, these results cannot be extrapolated to other types of SADs. Therefore, further clinical studies should investigate the use of different SADs, if they fulfil the criteria of being readily available at the bedside.
It should be stressed that much effort should be made to prevent the loss of the airway in the prone position, given the difficulty of reintubation. If this occurs, despite all preventive measures, we recommend bag–mask ventilation as a first line technique. If bag mask ventilation is ineffective, we recommend that an SAD should be inserted. In the meantime, one must prepare for turning the patient to the supine position, if possible, or collect more advanced equipment for intubation in the prone position.
This study has several strengths and limitations. The main strength is that this study was performed in patients rather than manikins. Another strength is that no learning curve affected this study, as no anaesthesiologist participated in more than three patients. This reflects clinical practice, because accidental extubation in the prone position is rare. The first potential limitation is the choice of the VivaSight-SL as an endotracheal tube. We used a lubricated and pre-warmed tube with the smallest internal diameter available, but insertion in the i-gel was difficult. Still, the VivaSight-SL was chosen as a safety measure to prevent harm in the study population. A second limitation is the inability to draw conclusions on the reasons for failure or to provide recommendations for manoeuvres to achieve a higher success rate. A third limitation, as mentioned before, is that the airway conditions of these patients were better than patients in an emergency situation, when secretions and gastric tubes may be present and airway pressures may be higher. Fourth, one should consider that these results only apply to the i-gel and may not be generalisable to other SADs.
In conclusion, this study demonstrated that blind intubation through an i-gel in the prone position is unlikely to be successful. However, insertion of an i-gel may provide a temporary rescue airway in the setting of accidental extubation of a ventilated patient in the prone position, while a more advanced plan for re-intubation is made.
Footnotes
Acknowledgements
The author(s) would like to thank the departments of anaesthesiology and neurosurgery and the operating theatre personnel of the Haaglanden Medical Center, The Hague, The Netherlands for their assistance.
Author contribution(s)
MvD recruited the subjects, obtained the data and approved the final manuscript. BMH guided the study in clinical practice, interpreted the results and approved the final manuscript. MVK designed the study, analysed and interpreted the results and drafted the manuscript.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Wetenschapsfonds of the Haaglanden Medical Center, The Hague, The Netherlands.