
Abstract
There is a deficit of commercially available paediatric airway models for anaesthesia airway management training, particularly for infant front-of-neck access and customised airway planning. Acknowledging this, we created a three-dimensional printed prototype for an affordable, high-fidelity training device, incorporating realistic tactile feedback, reproducibility and potential for modification for specific patient pathologies. Our model, created on a Stratasys Polyjet J750™ (Rehovot, Israel) printer, is a novel and useful educational tool in paediatric airway management, and we are pleased to share access to this resource with readers. Our work adds credence to three-dimensional printing as an accessible, reproducible and pluripotent technology in clinical anaesthesia.
Background
The place of three-dimensional (3D) printing in anaesthesia is evolving. Recent publications reflect growing enthusiasm and scope for innovation, particularly in the realm of airway management in anaesthesia.1–8 Despite this, there is a paucity of work in 3D printed neonatal, infant and paediatric airways within anaesthesia. Paediatric airway crises are rare but high-stakes scenarios, highlighting the importance of simulation training. The continued challenge is for improved fidelity in teaching models, offering realistic haptics and anatomical accuracy, without the logistical and ethical complexities of live or cadaveric animal models. Modelling the paediatric airway presents an additional challenge as the stiffness of the airway and the elasticity of the tracheal cartilages change with age. Several small paediatric models have been developed within otolaryngology for bronchoscopy training,9–11 but these have not yet translated to the anaesthetic context, where application for front-of-neck access is relevant.
Our 3D printed multi-property simulative airway model: Conception and development
There are limited commercially available paediatric airway models for anaesthesia airway management training, 12 and no neonatal models to our knowledge. Furthermore, there is a gap in commercial models designed for infant front-of-neck access, in contrast to supraglottic airway placement. Acknowledging these deficits, our aim was to create a prototype for an affordable, high-fidelity training device, incorporating realistic tactile feedback, reproducibility and potential for modification for specific patient pathologies.
The initial prototype was developed in conjunction with the Victoria University School of Design, based on computed tomography (CT) imaging from a 4 kg five-month-old infant. The 3D Slicer software programme was used to create 3D meshes from the CT images, and Zbrush and Meshmixer to produce a 3D printable file. Netfabb software assisted with correcting mesh errors.
Producing a model with realistic tissue properties was a priority in the design process. Initial prints experimented with varying shore hardnesses (from rigid to soft and flexible) using Stratasys’s (Stratasys J750™, Rehovot, Israel) ‘Vero’ and ‘Tango’ materials. 13 The final 3D prints, reflecting greater tissue fidelity, were made using the newer photopolymer ‘Agilus30’ 14 with a Stratasys Polyjet J750 printer (see Figures 1 and 2). The J750 allows full colour, variable density and flexible properties to be produced in a single object in layers of 14 microns.
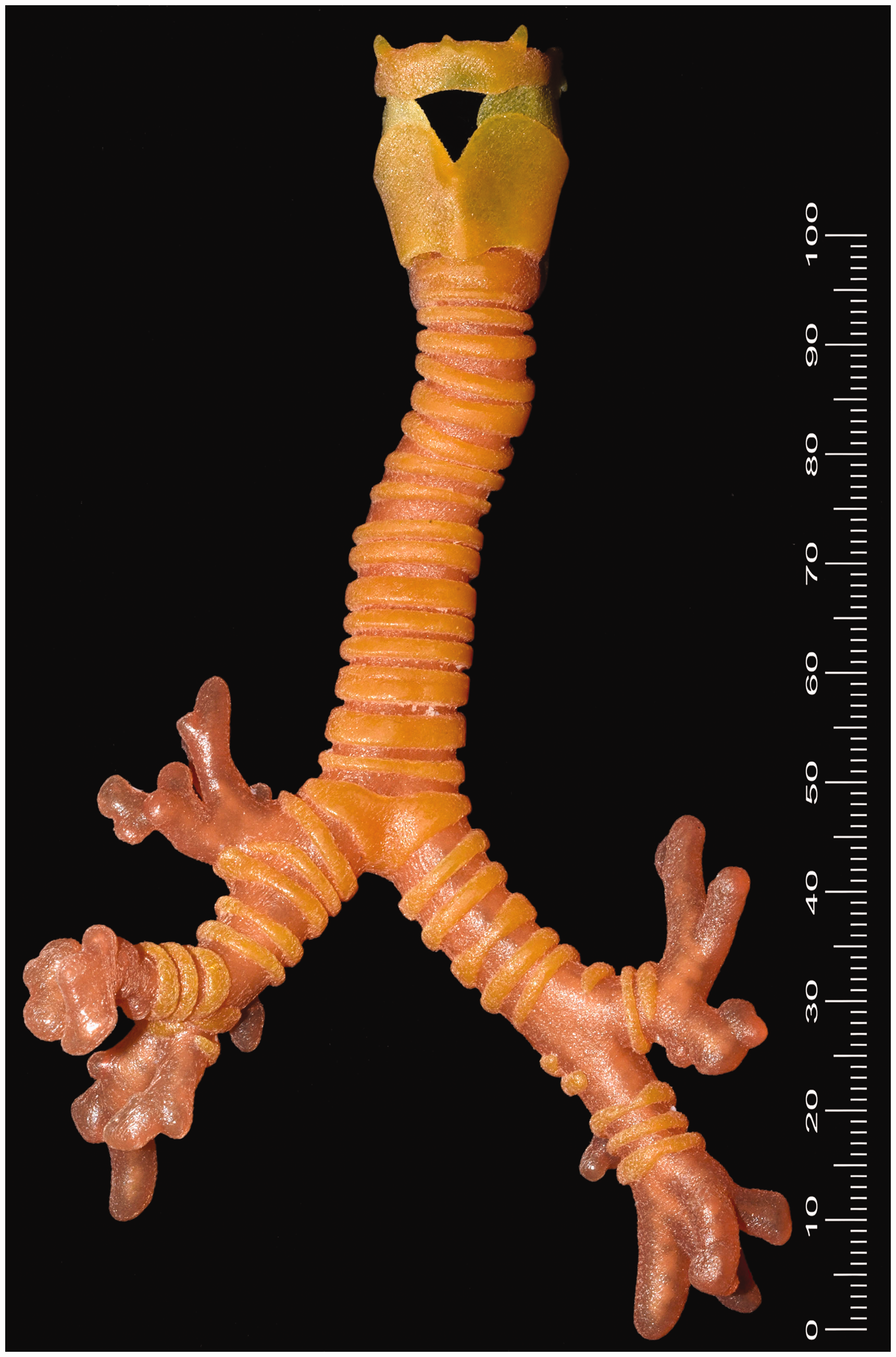
External view: three-dimensional printed multi-property paediatric trachea created in Wellington (scale reference in millimetres).

Cross-sectional view of upper airway (scale reference in millimetres).
The scope for anticipated application of our resultant model is broad. Addressing the gap in paediatric airway crisis education, we intend to use the model in departmental training for anaesthetic consultants and registrars in simulated ‘can’t intubate, can’t oxygenate’ (CICO) scenarios involving neonates, infants and small children. We plan to develop and refine our model further; for example, we intend to use a Newton metre to compare the distensibility of our model to that of animal cadaveric models. Interest has already been shown by the Department of Otolaryngology at Wellington Hospital in using the model for surgical bronchoscopic training. Rigid bronchoscopy images of our model obtained by a consultant otolaryngologist at Wellington Hospital (using a Storz Hopkins (Karl Storz Endoscopy Australia, Macquarie Park, NSW) telescope 0° 4 mm) are included herein (see Figures 3 and 4). In addition, there is potential for shared airway planning between anaesthesia and otolaryngology based on pathological airway modelling.
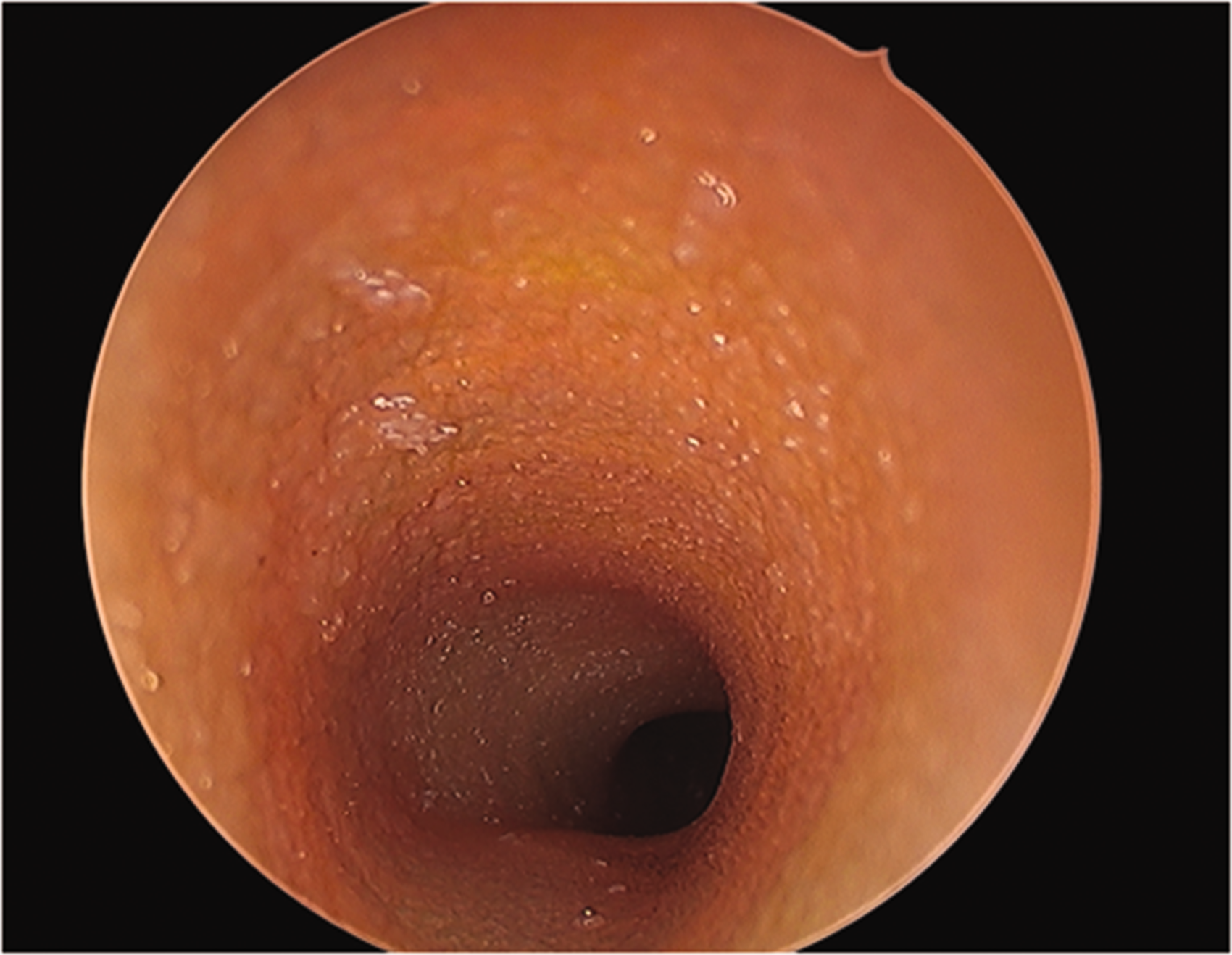
Tracheal view with Storz Hopkins (Karl Storz Endoscopy Australia, Macquarie Park, NSW) telescope 0° 4 mm.

Carinal view with Storz Hopkins (Karl Storz Endoscopy Australia, Macquarie Park, NSW) telescope 0° 4 mm.
While we acknowledge that the setup costs for the printer and materials for our model are significant, our work emphasises the potential for collaborative projects (in our case, with the Victoria University School of Design), and offers an economically viable alternative to commercial models. Furthermore, this project represents an example of what will be increasingly possible as 3D printing technologies become more readily available and financially accessible. In the interim, we hope to share this technology with our Australasian colleagues. We invite anaesthetists to send us electronic data files (for example, of airway pathologies for airway planning, or requests of age-specific models for CICO training) to be printed and posted, maximising accessibility to our printer and design.
The development of our 3D printed infant trachea prototype not only provides a novel and useful educational tool in paediatric airway management, but it also adds credence to 3D printing as an accessible, reproducible and pluripotent technology in clinical anesthesia.
Footnotes
Author contribution
Jane Christy Carter: conceptualisation, writing original draft, writing-review and editing. James Broadbent: conceptualisation, writing review and editing. Jeremy Young: supervisor, conceptualisation, writing review and editing. Ella Murphy: conceptualisation, writing review and editing. Bernard Guy: conceptualisation, supervision, writing review and editing. Katherine E Baguley: conceptualisation, writing review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.