
Abstract
Burn-injured patients provide unique challenges to those providing anaesthesia and pain management. This review aims to update both the regular burn anaesthetist and the anaesthetist only occasionally involved with burn patients in emergency settings. It addresses some aspects of care that are perhaps contentious in terms of airway management, fluid resuscitation, transfusion practices and pharmacology. Recognition of pain management failures and the lack of mechanism-specific analgesics are discussed along with the opioid crisis as it relates to burns and nonpharmacological methods in the management of distressed patients.
Keywords
Introduction
Burn injury is regarded as the most severe trauma that a patient can sustain and hope to survive. Apart from their roles providing anaesthesia during early definitive debridement of burn eschar with temporary wound closure using dermal substitutes or allograft, damage control surgery, airway management, resuscitation and intensive care, anaesthetists involved in burn care develop expertise and understanding of pain and anxiety management, dressing changes, nutrition, modulation of hypermetabolism and inflammation, and infection control in this group of patients who can sometimes be very challenging yet uniquely rewarding. Anaesthetists outside of burn centres may only ever care for burn patients acutely on rare occasions, or for survivors having unrelated surgery after recovery from their burns. This review is intended to give an overview of the challenges burn injury may pose.
Burn care has advanced greatly in the last 50 years, with improved mortality outcomes, but life never returns to normal for many patients. The challenge for the near future has been set in simple terms: to strive for no deaths, no scars and no pain. 1 We understand that surviving a major burn leaves the patient with biological systems that are permanently changed. Burn survivors have increased mortality from all causes, 2 including accidental and violent deaths, cancers of the mouth, larynx, liver, lungs and oesophagus, infectious diseases including influenza and viral pneumonia, and myocardial fibrosis, and also have a higher rate of ischaemic heart disease. 3 Diabetes risk increases for the first five years following the burn, with persistent insulin resistance demonstrated in some patients. 4
Systemic inflammation
Burn injuries can be categorised by their aetiology, whether flame or scald, chemical or electrical. Deeper to the skin which acts as a barrier, underlying tissue can be damaged further due to local tissue responses. These zones of burn were originally classified by Jackson: a coagulated zone of necrosis; a zone of stasis which has vascular leakage and local vasoconstriction due to inflammation—regarded as a watershed area that is potentially salvageable; and a third zone of hyperaemia secondary to vasodilation. 5 In burns larger than 30% total body surface area (TBSA) this last zone extends to most of the body, where the circulatory changes can cause burn shock. Oedema formation occurs in two phases: an abrupt increase in water content of damaged tissue initially; and in the second phase increased fluid flux into both burned and intact skin and soft tissues from around 12--24 h post-burn. Doubling of the fluid content in damaged cells occurs within an hour, whereas the second phase only occurs after fluid resuscitation has started. Cell membrane potential is decreased in cardiac, hepatic and endothelial cells as well as other tissues distant to the site of injury, and although the precise mechanism remains unclear it is likely related to failure of adenosine triphosphate (ATP) and ATPase activity. A hypermetabolic response is triggered by a significant rise in catecholamines, cortisol, glucagon and dopamine, which persists for up to three years post-burn. 6 A genomic alteration in white blood cells persists for up to a year following large burns. 7 Extensive burn injuries trigger the release of pro-inflammatory mediators leading to complement activation, 8 cytokine production including tumour necrosis factor alpha (TNF-α), interleukins (IL) 1β and 6, and increased nitric oxide levels leading to dilated and congested blood vessels, including cerebral vessels. 9 In animal models of smoke inhalation, microhaemorrhage and albumin leakage into brain tissue can be demonstrated with loss of basement membrane integrity. 10 Initial and early cognitive changes are commonly seen in large burns, including drowsiness, confusion, disorientation, delirium and even psychotic reactions. This early cerebral aspect of burns has often been overlooked but it should alert the clinician to the resultant longer-term challenges that this injury poses.
Anaesthesia and intensive care for burn-injured patients
Airway management
The larynx closes involuntarily in response to heat, thus protecting the lower airways to some extent. Thermal injury to the larynx results in early hyperaemia with erythema and swelling, extending to the mucosa of the aryepiglottic folds, false cords and lingual surface of the tongue, with relative sparing of the arytenoids and subglottic area. In keeping with its physiological function of temperature control, the mucosa of the upper airway absorbs heat before it reaches the trachea. Temperatures above 160°–200°C cause rapid vascular congestion, with vocal fold tissue separating due to oedema and eventual complete distortion of laryngeal landmarks. Delayed inflammation and softening of tracheal cartilage can occur but will usually declare itself by 24 h. 11
The Emergency Management of Severe Burns (EMSB) course teaches the concept that if there is doubt about the airway remaining patent until the patient arrives at the receiving burn centre then the patient should be intubated. 12 Specific indications for intubation include those where a clear need for airway protection exists, such as markedly reduced level of consciousness, impending or actual airway obstruction, excessive airway secretions, facial trauma, and need for ventilation due to other causes of oxygenation failure.
Various centres have reported their experience suggesting the threshold for intubation may be too low and pointing out that intubation is not without inherent risk. 13 There is potential for harm in the event of failed intubation leading to a surgical airway where the intubation perhaps wasn’t entirely necessary. Failed intubation occurs more frequently outside the operating room (OR) and rescue of the burned airway should be considered for inclusion in simulation training to improve success rates. 14 Pre-hospital intubations may contribute to higher pneumonia rates 15 and have been associated with longer time to extubation after arrival in the burn centre and increased length of hospital stay compared with intubation in the emergency department, 16 supporting the view that the patient should only be intubated pre-hospital if any immediate risk to airway patency exists. Specific criteria for intubation have been suggested by the American Burn Association in 2011, including full thickness facial burns, stridor, respiratory distress, supraglottic swelling on either direct laryngoscopy or nasendoscopy, upper airway trauma, altered mentation, hypoxia/hypercarbia or haemodynamic instability. 17 The conditions under which intubation is less likely to be indicated include a burn mechanism other than flame, burns that did not occur in an enclosed space, less than 20% TBSA thus not needing fluid resuscitation, partial thickness facial burns or flash burns, or when the transfer time to the receiving burn centre is less than three hours. 18
Patients for whom there is not a clear clinical indication for intubation during the primary survey may benefit from nasendoscopy to differentiate between the presence of erythema versus more worrisome features of oedema or carbonaceous debris, although current evidence suggests that endoscopy of the larynx does not offer better information than history and clinical examination. 19 Nasendoscopy might have a role in flash burns to the face without definitive symptoms of distress, but should ideally be repeated within a few hours if there is any concern about worsening symptoms that may indicate progression.
Intubation for airway protection also comes at a price, with mechanical ventilation contributing to decreased filling pressure, further impairing already decreased cardiac output and urine production, and leading to increased fluid requirement. A strategy of delayed intubation for patients without definitive indications, who are able to maintain their own airway and oxygenation, may therefore be of benefit. 20
The apparent change in decision threshold towards earlier intubation and mechanical ventilation has been attributed to principles taught on formal trauma courses such as Advanced Trauma Life Support, Early Management of Severe Trauma and EMSB. 21
Twill tape is often used to secure the endotracheal tube in facial burns, and silicone strips underneath can help to reduce the risk of pressure ulcers. 22 Wiring the tube to the teeth or maxillary screw fixation may be necessary.
Paediatric high volume–low pressure cuffed endotracheal tubes in children aged 0--10 years with burn injury have been reported to be associated with lower rates of air leakage and need for tube changes. 23
Burn contractures of the mouth or neck may necessitate fibreoptic intubation 24 or, in some cases, a combination technique with videolaryngoscopy with the tube loaded over a fibreoptic bronchoscope. 25
Laryngeal healing following inhalational injury is prolonged, with re-epithelialisation taking up to 10 weeks in the vocal folds, and the subglottic area requires a similar time as the cutaneous wound to heal. Preservation of the basal cell layers helps earlier healing, but granulation or prolonged intubation may lead to stenosis. Early infiltration by inflammatory cells and fibroblasts contributes to epithelial migration and coverage of damaged areas with collagen deposits seen within a week after the injury, and this is followed by dense scarring and lamination over the injured area which only resolves later when scar maturation occurs. Azithromycin has been used to modulate IL-17, postulated to be driving the local inflammatory response involved in subglottic stenosis. 26 Voice change is common, and complications from scarred glottic structures need to be identified early. Outcome benefit from tracheostomy earlier than 14 days has not been conclusively shown in either burns or critically ill patients, 27 but difficult repeated or prolonged intubation in burn patients may contribute to pressure necrosis, oesophageal perforation or granulation and ulceration of the posterior glottic webs leading to fibrosis 28 or dysphagia. 29
Temperature management
Burn ORs can be uncomfortable for staff. Raising the ambient temperature aims to compensate for the loss of temperature regulation by the skin and the hypermetabolic response with severe burns that results in a core temperature elevation to approximately 38°--38.5°C, thought to be due to a hypothalamic set point mechanism. 30 This response is related to the burn size and hyperdynamic phase of burn injury, driven by catecholamines and increased resting energy expenditure. Heat redistribution from the core to the periphery through vasodilation after induction of anaesthesia is compounded by increased evaporation and heat loss from the large areas being exposed during surgery. Ambient temperatures close to thermoneutral for the patient cause physical and cognitive fatigue in team members, and gowned surgical staff potentially shed sweat or skin leading to increased risk of contamination of open wounds. Forced air warmers are not always efficient due to the large surgical exposure limiting their contact with the patient. 31 Water mattresses or conductive heat transfer pads have also been used, but have their own risks for contact burn and infection. A novel technique involving an intravascular temperature regulation device placed into the inferior vena cava via the femoral vein has shown promise in a small non-blinded trial. 32
Not enough recent burn-specific evidence is available to recommend the best intraoperative approach to temperature management. Currently available studies have high heterogeneity preventing a systematic review. Warming strategies for other surgical procedures have been reviewed but are not entirely applicable in the burn patient. Hypothermia on arrival to the emergency department or burn centre has been associated with higher mortality posing an ongoing challenge to balance the first aid measures of cooling the burn whilst keeping the patient warm. 33 Cooling the burn has the benefit of direct thermal energy removal and reduction of swelling, but also reduction in tissue expression of genes that drive apoptosis and cell proliferation in tissue adjacent to the burn. There is, therefore, a theoretical benefit of mild hypothermia through reduction of the cytokine storm. 34
Fluid resuscitation and management during burn excision
The main goal of fluid resuscitation is prevention of burn shock, cell shock and subsequent multiple organ failure that may occur following severe burns over 20% TBSA in adults, and 10% TBSA in children. The aims of fluid resuscitation have remained largely unchanged over the last 50 years since the seminal work of Baxter and Shires who aimed to calculate the amount of fluid that would restore the cardiac output at 24 h post-burn. 35 Fluid is lost from the circulation from the time of the burn injury, with early failure of the endothelial glycocalyx integrity proportional to the extent of the burn 36 leading to increased permeability with oedema of both burned and non-burned tissue. This is driven by intense catecholamine release with persistent beta-adrenergic receptor stimulation, also implicated in subsequent myocardial depression that is commonly seen. Intense initial systemic and pulmonary vasoconstriction occurs in the face of low cardiac output with decreased oxygen delivery and consumption which slowly recovers over 24--48 h. The recovery time to baseline is decreased by using well-known formulae based on the total burn size and body weight to predict the fluid resuscitation required over the first eight and subsequent 16 h, trying to mimic the timing of the fluid loss over the first 24 h.
Modifications of the original Parkland or Brooke formulae are the most commonly used, with a military version known as the ‘Rule of 10’ also developed to simplify resuscitation in combat situations (see Table 1). In major burns the fluid resuscitation volume at 24 h commonly reaches 6 ml/kg/%TBSA.
Fluid management formulas used for prediction of fluid required in first 24 h post-burn.
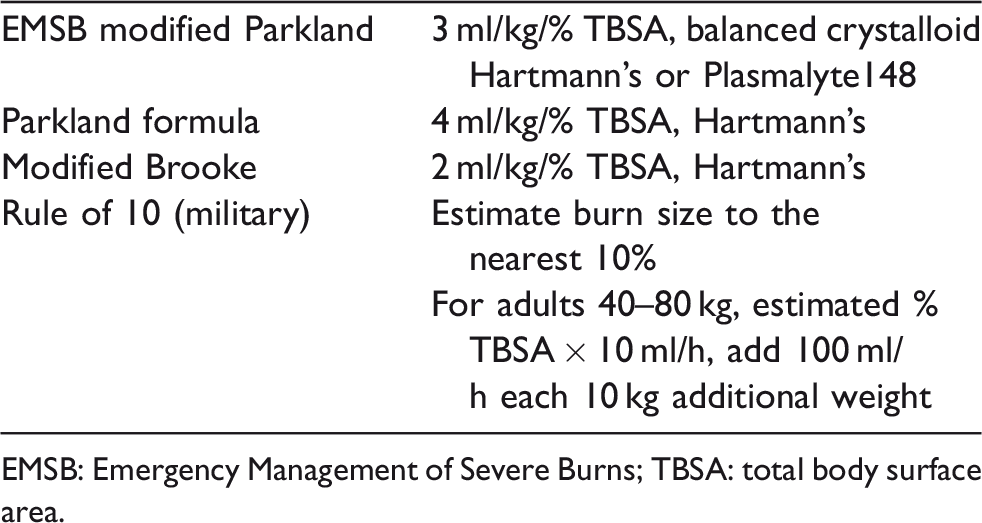
EMSB: Emergency Management of Severe Burns; TBSA: total body surface area.
It is commonly stated that the ideal hourly urine output is 0.5 ml/kg in adults and 1 ml/kg in children but this has never been formally defined in human clinical trials. Hourly monitoring of urine output nevertheless remains the most useful measure to guide the hourly fluid administration rate, along with metabolic trends of lactate and base deficit.
Goal-directed resuscitation has been reviewed recently. 37 Studies are plagued by small numbers and lack of blinding without convincing survival benefit, 38 with goal-directed therapy implicated in higher than predicted fluid administration. Recent surveys, mostly in European countries, found the most common monitoring, when used, to be pulse contour analysis or transpulmonary thermodilution, with some centres using oesophageal Doppler or pulmonary artery catheters. 39 A recent systematic review of studies comparing invasive monitoring with traditional endpoints showed no survival benefit, with no difference in lactate levels but improved cardiac index and urine output at 24 h with the use of transpulmonary thermodilution. The authors point out that multicentre studies would be required to provide adequate power, with randomisation and clinician/observer blinding, as well as possible exclusion of patients not likely to survive. 40
Over-resuscitation, termed ‘fluid creep’ or ‘resuscitation mortality’, can occur when fluid volumes exceed 6 ml/kg/%TBSA. Complications including abdominal and limb compartment syndromes, respiratory distress syndromes and impaired wound healing may result. 41 Patients with larger burns (>40% TBSA), electrical burns or skeletal immaturity (age less than around 6 years) seem to be at higher risk of abdominal compartment syndrome and the need for decompression laparotomy contributes to increased mortality. 42
The choice of fluid remains controversial, aside from an assumption that a balanced salt solution is the best option in large burns to avoid the hyperchloraemic metabolic acidosis associated with large volume normal saline administration. 43 Ringer’s lactate was the original crystalloid and remains the most common choice, with very few studies comparing other crystalloids. 44 Albumin used for burn resuscitation reduces required fluid volumes and the incidence of compartment syndrome without showing survival benefit or reducing respiratory or renal complications. 45 ,46 Interest has re-emerged in albumin as a rescue therapy, however, when hourly fluid requirements reach twice that predicted by the Parkland formula, or when the predicted volume at 12 hours post-burn exceeds 6 ml/kg/%TBSA, as suggested by a survey of burn clinicians at the 2016 American Burn State of the Science meeting. 41 This involves earlier commencement of colloids than that recommended by the original Parkland and Brooke formula which suggested colloids only in the second 24 hours post-burn.
Animal studies suggest that plasma restores syndecan levels and attenuates both systemic and pulmonary glycocalyx degradation seen during burn shock. 47 Some older human trials reported reduced volume requirements and virtually no abdominal hypertension following resuscitation with plasma but did not report long-term relevant outcomes such as survival or length of stay. 41
Another potential agent for minimisation of endothelial disruption is vitamin C which acts as an electron donor, reducing free radical oxygen species in the endothelium where induced nitric oxide levels exceed the physiological scavenging capacity after burns. Small randomised controlled trials in subjects with large TBSA burns have shown benefit in terms of reduction in fluid requirements, weight gain and ventilator days. Vitamin C results, however, in an osmotic diuresis which has been implicated in higher rates of acute kidney injury and oxalate nephropathy, leaving uncertainty about which patient groups may benefit. 48 Its use has not been widely implemented but vitamin C is best avoided in patients with early renal dysfunction. 49
Acute kidney injury may occur in up to 25% of burn-injured patients with risk factors such as larger burn size or extent of full thickness burn and higher injury scores on admission. 50 It occurs in up to 15% of patients even those with smaller burns between 10%--20% TBSA51 and also predicts future longer-term renal impairment. 52
Bleeding and transfusion
Burn patients differ from other trauma patients in their haemostatic response, which is characterised by acute traumatic coagulopathy and a haemorrhagic phenotype that leads to disseminated intravascular coagulation. The excessive inflammatory response in patients with high burn severity usually results in hypercoagulability but under certain conditions can trigger a lethal triad of hypothermia, acidosis and lactataemia which can contribute to massive blood loss. 53 Laboratory tests of coagulation have proved to be poor predictors of coagulation in burn patients, whereas viscoelastic tests give better real-time indication of coagulopathy as discussed in a recent review. 54 Clot strength and microstructure decreases with progressive haemodilution, which is another risk of over-resuscitation. 55
Blood loss during excision of large burn eschar has the potential to exceed a blood volume, despite the current practice of using tumescent infiltration techniques. 56 The role of tranexamic acid in other areas of trauma surgery has been defined by trauma studies, 57 none of which share the hypercoagulation seen in burn injury, but it is likely best reserved for situations where secondary fibrinolysis can be demonstrated. 58
Transfusion triggers in burns have traditionally been set at a haemoglobin concentration of 100 g/l in order to ensure adequate oxygen delivery to the wound. The Transfusion Requirements in Critical Care (TRICC) trial published in 1999 changed our thinking about the level of the trigger and lower haemoglobin levels which gradually became accepted. 59 Whether or not the findings from that study could be replicated in the burn setting was addressed by a multicentre trial, involving 345 patients from 21 centres in USA, Canada and New Zealand, which compared a restrictive trigger of 70 g/l with 100 g/l haemoglobin. This Transfusion Requirement in Burn Care Evaluation (TRIBE) trial transfused 7000 units of blood in total and found no difference in the primary outcome of bloodstream infection or non--bloodstream infection, and no difference in secondary outcome measures of mortality, pneumonia, wound infection, hospital length of stay, intensive care unit (ICU) length of stay, organ dysfunction or wound healing. 60 Further planned subgroup analysis of patients with burns larger than 60% TBSA was conducted using the results from 25 subjects in the liberal group versus 21 in the restrictive group demonstrating no differences in the primary bloodstream infection or other infection or mortality outcomes, although patients in the restrictive group had fewer ventilator days. 61 The age of transfused units has been noted to increase with the modern practice of fewer transfusions, raising concerns about the potential effect of aged blood on outcome. The TRIBE trial showed that neither the age of blood nor the proportion of very old blood transfused affected multiple organ dysfunction scores, time to wound healing or in-hospital mortality. 62 The trial demonstrated that it is safe to use a trigger of 70 g/l haemoglobin for transfusion. It also demonstrated that blood is currently transfused outside the OR more often than during surgery.
As with trauma practice, transfusion using ratios of blood products during burn excision remains controversial and continues to evolve. Aggressive 1:1 transfusion of packed red blood cells and fresh frozen plasma led to decreased markers of coagulopathy and acidosis in a single-centre paediatric trial, 63 while an earlier observational trial reported that a 1:1:1 ratio of red cells, fresh frozen plasma and platelets as well as some cryoprecipitate did not result in better haemostasis or prevention of platelet dysfunction. 64
Total intravenous or volatile anaesthesia
During periods of respiratory failure, total intravenous anaesthesia (TIVA) is required for cases where an anaesthesia ventilator is inadequate during surgery and the ICU ventilator is taken to the OR. In burn patients with respiratory failure there is some evidence to suggest non-survivors have higher levels of IL-8, shown to be down-regulated by sevoflurane. No randomised trials have been done, however, to investigate any effect of the anaesthetic agent on outcome following burn surgery.
Cancio et al. at the US Army Institute of Surgical Research continued ICU sedation with ketamine at 8 mg/kg/h combined with methadone in doses of 0.26–0.54 mg/kg and/or fentanyl at 8.6–10.3 µg/kg/h. They suggested that TIVA did not result in higher pressor requirement even though the patients given TIVA were sicker with larger burn size and had a higher rate of inhalation injury. 65
Propofol in burn patients has enhanced clearance and increased volumes of distribution. Adult patients weighing 73 kg (versus 67 kg controls), with mean (standard deviation (SD)) 41% (19%) TBSA burns after 16 (14) days post-burn, given a 2 mg/kg bolus, showed V1 of 48.4 l versus 27.6 l and central clearance of 4.2 l/min versus 1.7 l/min when analysed with non-linear mixed effect modelling best fit to a three-compartment model. After an initial drop in arterial blood flow during the first 12 h following the burn, liver blood flow increases during the hyperdynamic phase by 150% up to 35 ml/kg/min with hepatic clearance rates of propofol approaching 60 ml/kg/min. 66 These pharmacokinetic changes predict inaccuracy with propofol infusion models as demonstrated by a study in 18 adult burn patients with mean 30.6% (SD 5%) TBSA using the Marsh propofol TIVA model during gradual induction of anaesthesia allowing for calibration. There was a nonlinear biphasic bispectral index (BIS) response (A-2000™ monitor, Aspect Medical Systems Inc, Norwood, MA, USA) with a lower mean BIS of 50 at a predicted effect site concentration of 3.5 µg/ml which did not decrease at higher propofol infusion rates. 67 The cause of this non-linear relationship and inability to decrease the BIS beyond 50 with increasing doses of propofol is uncertain, but could be due to early recovery from vecuronium leading to electromyogram interference, or the older three-electrode BIS sensor used during the study possibly leading to interpretation of the frontal electromyogram as an electroencephalogram.
Propofol sedation in ICU has been estimated to provide up to 17% of daily energy requirements. Excess fat more than 30% of total requirements leads to hepatic lipogenesis, 68 worsening the tendency to fatty liver in burn patients and may lead to longer ventilation times through an unknown mechanism. Anaesthetists using TIVA with propofol should therefore record the dose given and take into account the total fat load, with a reduction made to the daily caloric intake from other sources.
Considering that neither current pharmacokinetic target-controlled infusion models for propofol anaesthesia nor the accuracy of depth of anaesthesia monitors have been adequately validated specifically for use in burn patients, 69 and bearing in mind the additional fat load, TIVA should be used with some caution. 70
Sevoflurane pharmacokinetics have been described in a small study of 12 adult burn patients with mean 36% (SD 11%) TBSA for procedural sedation and surgery, showing higher measured plasma concentrations, higher volume of distribution and prolonged elimination half-life without a higher fluoride concentration compared to controls. Renal function did not change as assessed using neutrophil gelatinase-associated lipocalin levels. 71
Other pharmacological considerations
The effect of suxamethonium on potassium release is well recognised as a contraindication for administration later than 48 h after the burn injury. Burn-related inflammation and local muscle denervation leads to up-regulation of acetylcholine receptors, as well as extrajunctionally expressed receptors of both immature and α-7 nicotinic acetylcholine receptors. 72 This leads to altered receptor kinetics with a greater and continued release of potassium, associated with serum potassium levels up to 9 mmol/l in the original case series from Gronert et al.73–75 and further discussed by Martyn et al. 76 Wound healing and mobilisation are the minimum requirements for reconsideration of suxamethonium after the burn injury, with caution recommended due to the lack of data on when receptor expression returns to normal.
Burn patients may have a relative resistance to non-depolarising muscle relaxants due to a variability in volume of distribution and enhanced intercompartmental clearance at the terminal phase, 77 as well as variable tissue distribution, or even loss through wounds. 78 Changes in plasma proteins with lowered albumin and raised α-1 acid glycoprotein may explain some of the raised volume of distribution.
Methadone acts through µ-opioid receptor agonism, as well as antagonism at the N-methyl D-aspartate (NMDA) receptor with added reuptake inhibition of serotonin and noradrenaline. These added mechanisms are thought to lead to increased effectiveness in neuropathic pain as well as a proposed prevention of transition of acute to persisting pain. Side-effects to consider in the burn patient include QT prolongation, especially when the patient is also treated with cytochrome P450 (CYP) inhibitors such as macrolide antibiotics, diltiazem or verapamil, or azole antifungals which can inhibit CYP2C19 and CYP3A4. 79 In critically ill burn patients methadone has been associated with a reduction of delirium rates 80 as well as reduced ventilator time. 81
Morphine pharmacokinetics in burns remain relatively unchanged with first-order kinetics observed even during long-term infusion over three weeks in burn patients, with dose variation between 4 and 39 mg/h, with clearance rates of 14.8–40.3 ml/min/kg. 82 Morphine has some anti-inflammatory action through binding of µ-3 receptors whilst fentanyl does not bind this receptor, and this has been proposed as an explanation for some burn patients having higher temperatures when treated with fentanyl compared to morphine. 83
Fentanyl volume of distribution has been shown to be increased in a three compartment model after a single dose of 200 µg in patients between seven and 35 days post-burn. The results of this study confirmed lower than expected plasma concentrations but less of an increase in clearance as an effect of increased cardiac output, 84 confirming previous findings that clearance and cardiac output are of lesser importance. 85 Slow-metabolising cytochrome genotypes have been identified, including CYP2D6*9, CYP2D6*29 and CYP3A4*1B, that affect fentanyl pharmacokinetics due to decreased clearance potentially leading to increased plasma concentrations. 86
Pharmacokinetic changes during continued infusions of a number of drugs in critically ill patients have been the subject of a systematic review that showed reduction in clearance in general with increased volumes of distribution, 87 and another using available studies of antibiotics confirmed increased volumes of distribution and clearance rates with potential for underdosing. 88
Nutrition
Prolonged hypermetabolism following burns leads to muscle protein and weight loss, immune suppression, decreased wound healing, increased infection risk, physiological exhaustion and eventually increased risk of mortality. 89 Early enteral feeding has become the accepted standard of care, with preserved gut mucosal integrity and motility reducing the risk of ileus or intestinal ischaemia. 90 A recent meta-analysis of randomised controlled trials showed decreased mortality as well as reduced rates of gastrointestinal (GI) bleeds and sepsis favouring feeding before 24 h compared to later than 48 h following burn injury. 91 Early feeding has been defined as commencing within four to six hours after burn injury. 92 Feeding should ideally be via a post-pyloric enteral feeding tube to minimise perioperative cessation (which may lead to a caloric deficit of 50% for the day of surgery). Feeding without cessation avoids the need for catchup feeding. 93
Challenges of managing burn pain
The burn pain experience occurs over a prolonged period. During the initial phase the pain is usually described as background pain, with breakthrough pain such as the procedural pain associated with dressing changes and surgery, and then persistent pain that lasts for years following the initial recovery. Pain distress is common during the acute phase despite the use of opioids and/or ketamine. Patients may experience any combination of factual or delusional memories of the events surrounding the trauma or the subsequent OR visits for surgery, wound care or intensive care experiences. 94 Despite best efforts at pain management, for some patients the pain experience following burn injury and the subsequent memory of pain will remain the worst that the patient has ever suffered. For others the pain memory that remains can be a positive one in which, for example, everyone did their best to help alleviate the pain experienced during dressing changes and after procedures. The statement describing the gate theory by Melzack and Wall in 1965, namely that ‘it is possible for central nervous system activities subserving attention, emotion, and memories of previous experience to exert control over the sensory input', remains relevant. 95
The biological domains of burn pain include nociceptive changes following tissue damage and cytokine release, ongoing inflammation, genomic and neuroendocrine responses, as well as spinal cord changes. Biological mediators produced in the burn wound and subsequent scar have been implicated as important contributors to maintenance of the nociceptive signal, including oxytocin in burn scar tissue and its link with psychological distress, 96 the role of the vanilloid receptor in thermal hyperalgesia and the potential for centralisation of pain, 97 damage-associated molecular pattern proteins (DAMPs) and stress hormones including cortisol. Cortisol and norepinephrine (noradrenaline) / epinephrine (adrenaline) remain elevated for several years following burn injury in children, only approaching a return to baseline some three years following the injury, 98 mirroring the pain trajectory in some patients. Nerve growth factor (NGF) released from regenerating skin causes hyperexcitability of primary sensory neurons and drives release of more neurotransmitters to the branches of fibres closely adjacent to cutaneous nociceptors, and activates release of substance P, calcitonin-related gene peptide (CGRP) and platelet-activating factor, leading to increased vascularity and redness associated with increased pain. 99 The NGF antagonist tanezumab has been considered to reduce pain and sensitisation in the scar, but early trials in osteoarthritis have showed increased rates of osteonecrosis, 100 and no other biologically targeted agents are available.
A review of randomised controlled double-blind clinical trials for the treatment of burn pain only found 14 studies that met the inclusion criteria, with most trials focused on the treatment of procedural pain, two on background pain and one on neuropathic pain. 101 This demonstrates the need for further multicentre trials with careful trial design to focus on patient-centred and longer-term outcomes, with adequate blinding. Many trials are underpowered and report surrogate outcomes that may not be important to the patient or their family. Trial design of both pharmaceutical and nonpharmaceutical interventions is challenging in the burn population, with difficulty in both recruitment and retention. Lower socioeconomic status and lower education levels are commonly encountered, further complicated by issues with transportation to the research location for patients who often live outside the immediate area of the burn centre. Psychosocial factors including anxiety, depression and post-traumatic stress disorder (PTSD) contribute to high dropout rates from follow-up as well as non-compliance with the therapeutic interventions being trialled. 102
It is important to keep in mind that nociception and pain (and suffering) are different and distinct phenomena. In the management of burn pain a focus on nonpharmacological interventions has become even more important in the face of the emerging opioid epidemic, with a growing recognition that the treatment of patients with opioids and other pharmaceuticals with misuse potential has contributed to tolerance, hyperalgesia, addiction and death. Despite the growing awareness of the dangers posed by opioids, there is evidence to suggest increases in both the number of opioid prescriptions and in doses following discharge from burn centres. 103 With the particular distress associated with burn injury, the risk for abuse through euphoric effects may be more important for some patients wanting to escape their reality. 104 Risk for misuse has also been noted to be increasing for gabapentinoids, 105 and accidental overdoses have occurred when combined with opioids. 106
Evidence is emerging for alternative nonpharmacological adjuncts for managing procedural pain, with trials showing positive results using hypnosis, 107 virtual reality and interactive gaming consoles, music and transcranial direct current stimulation. 108
Distress during the acute event resulting from pain and insomnia can contribute to worse psychological outcomes with the likelihood of chronic depression, suicidal ideation and poorer quality of life measures found to be increased out to two years. 109 Sleep dissatisfaction can occur in up to 50% of young adult burn survivors for several years following discharge from the burn unit. 110 Early identification of patients with insomnia and appropriate pharmacological 111 and nonpharmacological therapy may therefore lead to improved pain outcomes. PTSD that is diagnosed after burn injury--related pain may be due to hyperarousal which has been associated with misperception, catastrophising and intrusive thoughts, and anticipation of pain. 112 Acute stress disorder as well as PTSD is very common amongst major burn patients.
Coping style affects the acute pain experience as well as long-term outcomes in terms of both pain and stress disorders, and quality of life measures. Early identification of patients with avoidant coping styles and low levels of coping self-efficacy allows early intervention to address dysfunctional beliefs about the future physical and functional problems. This group of patients may benefit from increased self-control during painful procedures, 113 perhaps through a combination of anxiolysis and use of patient-controlled analgesia (PCA) modalities.
Reinforcement learning models postulate that patients try to predict future experiences by calibrating to their last pain experience. In this model opposite effects of controllability and uncertainty exist, where pain can be modulated through a sense of control and this could be exploited for benefit by the use of PCA or predictable administration of analgesia. 114
Some patients experience flashbacks to the event with negative emotional responses including anxiety, anger and depression, frustration from perceived loss of control, and catastrophic thinking leading to increased focus on pain behaviour. One potential approach to changing this thought pattern is known as ‘explaining pain', which includes a range of educational interventions to change the pattern of thinking from pain as a marker of tissue damage to an alert for protection against damaged tissue. This is a pragmatic approach to the biopsychosocial model of pain which includes teaching the patient about the biological process underpinning the pain, helping them to understand that pain avoidance can be overprotective, the hypersensitised nature of the sensory pathways, and that the brain and thoughts are able to act in a way that allows the signalling to be perceived as pain or alert signals. 115 In the acute setting this needs to be a continuous effort by all clinicians in contact with the patient and their family to facilitate long-term behaviour change and potential benefit.
Pain and itch both persist for years following recovery. 116 , 117 Post-burn itch is often a bigger problem than pain, 118 sharing features of neuropathic nociception such as hyperalgesia or hypoaesthesia in injured areas, worsening in the evening or when at rest, and with an overlapping time course following the injury. 119 Effective treatment for itch remain elusive in many patients, but proposed approaches include using a stepwise regimen starting with oral antihistamines and emollients, then psychologist input, then massage, silicone sheeting, hypnosis, transcutaneous electrical nerve stimulation, topical crystalline silver or capsaicin, and then consideration of topical steroids, topical lidocaine or gabapentin as the last approach. An alternative approach has been to link the therapy to the phase of wound healing with the same escalation pattern as above. 120
Alteration of the gut microbiome occurs early following burn injury, 121 theoretically contributing to the development of inflammation, acute and chronic pain, opioid tolerance, depression and anxiety, 122 and suggesting potential utility from probiotics, prebiotics, fermentable oligo-, di-, mono-saccharides and polyols (FODMAP) or faecal transplantation in pain management for burn patients. There is thus a developing understanding of the role of the microbiome in both acute and chronic pain, as well as the links with depression and anxiety. 123
Opioid hyperalgesia seems to occur more commonly in burns than other forms of trauma, probably related to the duration and dose of opioid therapy. 124 Various cellular mechanisms have been described as having a role in the development of opioid hyperalgesia. These include functional interactions with other G-protein coupled receptors including β-arrestin which mediates both acute tolerance and hyperalgesia. Other proposed mechanisms include µ-receptor variants, opioid metabolites including morphine-3-glucuronide, 125 increased NMDA receptor expression in the central glutaminergic system, and neuroinflammatory mechanisms, with evidence that blocking immune activation reduces hyperalgesia. 126 There are sex differences with animal studies showing females to be at higher risk. Lipid soluble opioids are more likely to induce acute tolerance. 127
Approaches to mitigate opioid hyperalgesia include using standardised pathways to encourage intermittent therapy and avoiding infusions when possible, avoiding lipid soluble opioids such as remifentanil, minimising overuse of benzodiazepines, avoiding massive dose increases, and addition of methadone to attenuate opioid tolerance through its action at NMDA receptors. The use of non-opioid analgesics such as ketamine for both pain management and ICU sedation, α-2 agonists (clonidine and dexmedetomidine) and gabapentinoids has also become standard practice in many centres. Opioid rotations and tapering of opioid doses when hyperalgesia is recognised are also recommended. 128
Opioids change the brain reward and affect pathways as shown by dose-related volumetric increases in the right hypothalamus, left inferior frontal gyrus, right ventricular posterior cingulate, and right caudal pons, and a decrease in the right amygdala. These changes are associated with the regulation of reward-related learning processing in the nucleus accumbens and may lead to long-term behaviour change, in some individuals increasing the risk for addiction. 129 Our understanding of the biology of pain becoming persistent has improved in recent years, 130 but more research is needed to establish reliable interventions to restore maladapted neural networks and the thought processes of the patient suffering pain during their recovery from severe burn injury.
Two apparently conflicting approaches to pain therapy exist; one being the use of standardised guidelines, which has been shown to have advantages, 131 and on the other hand individualised pathways that take into account the variability in opioid pharmacogenomics. 132 Early recognition of coexistent depression and anxiety traits should lead to early consideration of anxiolytics as well as psychological interventions for pain management. 133 Currently, despite recognised shortcomings, standardised pathways are probably still the best approach available. 134
Pain management in burn-injured patients remains challenging despite our increased understanding of the mechanisms involved in the various phases of recovery, and our understanding of the chronification of pain, and the effect of pain and suffering on the long-term outcomes for the burn patient.
Footnotes
Declaration of conflicting interests
The author(s )declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: F Stapelberg serves on the Board of the Australian and New Zealand Burn Association (ANZBA) as the Chair of the Education Committee. The views expressed in this article are his own and do not necessarily represent those of ANZBA.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.