
Abstract
The oxygen concentration (FiO2) and arterial oxygen tension (PaO2) delivered in patients undergoing major surgery is poorly understood. We aimed to assess current practice with regard to the delivered FiO2 and the resulting PaO2 in patients undergoing major surgery. We performed a retrospective cohort study in a tertiary hospital. Data were collected prospectively as part of a larger randomised controlled trial but were analysed retrospectively. Patients were included if receiving controlled mandatory ventilation and arterial line monitoring. Anaesthetists determined the FiO2 and the oxygenation saturation (SpO2) targets. An arterial blood gas (ABG) was obtained 15–20 minutes after induction of anaesthesia, immediately before the emergence phase of anaesthesia and 15 minutes after arrival in the post-anaesthesia care unit (PACU). We defined hyperoxaemia as a PaO2 of >150 mmHg and included a further threshold of PaO2 >200 mmHg. We studied 373 patients. The median (interquartile range (IQR)) lowest intraoperative FiO2 and SpO2 values were 0.45 (IQR 0.4–0.5) and 97% (IQR 96–98%), respectively, with a median PaO2 on the first and second ABG of 237 mmHg (IQR 171–291 mmHg) and 189 mmHg (IQR 145–239 mmHg), respectively. In the PACU, the median lowest oxygen flow rate was 6 L/min (IQR 3–6 L/min), and the PaO2 was 158 mmHg (IQR 120–192 mmHg). Hyperoxaemia occurred in 82%, 73% and 54% of participants on the first and second intraoperative and postoperative ABGs respectively. A PaO2 of >200 mmHg occurred in 64%, 41% and 21% of these blood gases, respectively. In an Australian tertiary hospital, a liberal approach to FiO2 and PaO2 was most common and resulted in a high incidence of perioperative hyperoxaemia.
Introduction
Approximately 2.5 million patients undergo general anaesthesia per year in Australia. 1 All receive oxygen therapy during general anaesthesia, and many receive oxygen postoperatively. Avoidance of hypoxaemia during and after surgery is important. 2 Some evidence in studies of patients at risk of hypoxaemia (critically ill patients) has raised concerns that supraphysiological oxygen tension (‘hyperoxaemia’) may be undesirable, although there is inconsistency in these findings.3–18 A recent systematic review of 16,000 critically ill patients (including patients who had undergone emergency surgery) suggested that liberal oxygen therapy might be associated with increased hospital mortality. 19 In addition, guidelines by the British Thoracic Society suggest a target pulse oximetry reading (SpO2) of 94%–98% in the perioperative period. 20 However, at this time, there have been no studies that have confirmed that intraoperative hyperoxaemia in non–critically ill patients is associated with adverse effects.
Despite the above concerns, evidence and guidelines, there is little information about the current practice of oxygen administration and partial pressure of oxygen in arterial blood (PaO2) levels achieved during and after surgery. The values for resulting PaO2 are not well documented, and the decision-making around this is not well described. In a recent Japanese study, oxygen therapy was liberal, and 80% of patients had oxygen saturation levels in excess of 98%. 21 However, high oxygen saturation levels are not informative about the degree of hyperoxaemia, and neither the Japanese study nor any other studies have measured PaO2 levels during or shortly after surgery. This is unfortunate because such information would provide a clearer understanding of the magnitude of exposure to hyperoxaemia and guide the planning of randomised controlled trials of oxygen therapy targets during anaesthesia.
Accordingly, we performed a retrospective cohort study of current oxygen therapy practice during major surgery in a university teaching hospital. Data were collected as part of a larger randomised controlled trial and were analysed retrospectively for the purposes of this sub-study. We hypothesised that anaesthetists would pursue a liberal approach to oxygen administration and that intraoperative and postoperative hyperoxaemia would be common.
Methods
After Human Research Ethics Committee (HREC approval number HREC/14/Austin260) and written informed consent, we performed a retrospective cohort study of patients undergoing major surgery at the Austin Hospital in Melbourne, Australia. This study was undertaken as a sub-study of an ongoing randomised controlled trial focusing on patients receiving controlled ventilation and its effects on postoperative clinical outcomes (Australia New Zealand Clinical Trials Registry no. 12614000790640, 19 July 2014). The protocol and statistical analysis plan of this overarching trial have recently been published. 22 Eligible patients were older than 40 years of age and undergoing major surgery with planned endotracheal intubation and controlled mandatory ventilation. Patients were included only if an arterial line was inserted as part of routine care and if the expected duration of surgery was more than two hours. The aim of these inclusion criteria was to enrol a cohort with higher risk of respiratory complications and in whom there would be a significant time of exposure to both controlled mechanical ventilation and oxygen therapy.
We excluded patients undergoing cardiac surgery (due to the need for cardiopulmonary bypass), patients undergoing procedures involving one-lung anaesthesia, intracranial neurosurgery and liver transplantation surgery due to potential concerns with exacerbation of intracranial pressure or pulmonary hypertension due to high partial pressure of carbon dioxide in arterial blood (PaCO2). Pregnant patients were also excluded. For the purpose of the present sub-study, we included participants randomised to the control arm of this trial from August 2014 to May 2017. The participants were ventilated with a mandatory volume control mode according to a ‘conventional’ ventilation strategy of 10 ml/kg ideal body weight and positive end-expiratory pressure (PEEP) of 5 cmH2O as defined by previous observational studies of mechanical ventilation during anaesthesia in Australian hospitals. 23 The study hospital is a tertiary hospital in Melbourne, Australia, with a wide surgical case mix, and is affiliated to the University of Melbourne. This manuscript adheres to the Strengthening of Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Details of ventilation and oxygenation and timing of data collection
All cases were undertaken under the supervision or direct care of a consultant anaesthetist. Participants underwent intravenous induction, neuromuscular blockade and tracheal intubation. A volatile agent was used to maintain anaesthesia. The primary trial protocol dictated only the tidal volume and the PEEP that needed to be applied. All other aspects of clinical care (including oxygen treatment) were at the discretion of the treating anaesthetists. 22 This sub-study had not been conceived at the time that surgery occurred. Therefore, anaesthetists were unaware of this sub-study and determined the inspired fraction of oxygen (FiO2), respiratory rate (RR) and the management of oxygen therapy according to their clinical judgement and preference. As part of the study protocol, the treating anaesthetists were requested to obtain a ‘post-induction’ arterial blood gas (ABG; 15 minutes after induction of anaesthesia) and a second ‘pre-emergence’ ABG (15 minutes before the estimated completion of surgery). These timepoints were chosen to assess oxygen therapy during the maintenance phase of anaesthesia and to avoid the induction and emergence phases where an increased FiO2 is typically used to prevent hypoxaemia. 2 The results of these ABG analyses were presented to the treating anaesthetists by operating-room nurses, and management was dictated according to their clinical judgement. In addition, anaesthetists recorded the lowest FiO2 and SpO2 during the intraoperative course. Postoperatively, in the post-anaesthesia care unit (PACU), oxygen was administered as directed by medical staff. PACU staff members were requested to obtain an ABG approximately 15 minutes after arrival in the PACU.
Measurement of PaO2 in the arterial blood was completed on an ABL 800 Blood Gas analyser (Radiometer, Copenhagen, Denmark) with a fully automated micro-mode adjustment, attenuating the risk of user-induced error and loss of accuracy with very small samples.
Details of data collected
Data were extracted from the participant’s electronic medical records and Austin Hospital’s computerised laboratory results by two independent study investigators. Austin Health utilises Cerner® (CERNER Millennium, Kansas City, KS) electronic medical records that allow comprehensive electronic data capture and access to participant health information in the perioperative setting. We collected data including participant characteristics such as age, sex, body mass index, American Society of Anesthesiologists Physical Status (ASA PS) score and type of surgery. We also collected data with regard to the presence of comorbidities, including the presence of previously diagnosed chronic obstructive pulmonary disease (COPD). Intraoperatively, the highest and lowest measured oxygen saturation from the pulse oximeter (SpO2) and the highest and lowest FiO2 during the maintenance phase of anaesthesia were recorded by the treating anaesthetist. Anaesthetists were instructed not to include the FiO2 administered specifically during the induction and emergence phases. We also recorded the PaO2 from the intraoperative ABG samples. In the PACU, we collected the highest and lowest SpO2 from the pulse oximeter and the PaO2 from the ABG.
We defined hypoxaemia as a PaO2 of <60 mmHg or a SpO2 from the pulse oximeter of <91%, as previously described. 2 Given the variability of previous definitions of hyperoxaemia in the literature, we identified two thresholds which are consistent with previous clinical studies. We defined hyperoxaemia as a PaO2 of >150 mmHg and a further threshold of a PaO2 of >200 mmHg.4,21 These thresholds were defined prior to initiation of the study. In addition, we separately assessed a preplanned subgroup of patients with COPD as documented at the pre-anaesthesia assessment.
Finally, we assessed whether the treating anaesthetists modified the oxygen level up or down after the first intraoperative ABG by assessing the differences in the FiO2 and PaO2 between the first and second intraoperative blood gas.
Statistical analysis and data handling
Recorded data were entered into an electronic database by staff blinded to the purpose of the study. Data were checked for validity by a third party also blinded to the purpose of the study. Data are presented as median (interquartile range (IQR)). Categorical data are presented as numbers and percentages. In cases where data were missing or not recorded, the data are presented as a proportion of complete cases, and no assumptions were made about missing data. Differences in distributed data were evaluated using the Mann–Whitney U-test. In all statistical tests, a two-sided P-value of <0.05 was taken to indicate statistical significance.
Results
Participant characteristics and surgical procedures
Between August 2014 and May 2017, 750 participants were randomised to our study of tidal volume and its effects on major surgery. We included 373 participants from the control group. The demographic details and type of surgery represented in our cohort are summarised in Table 1. Most patients were male (61%), with an ASA PS classification of 2 or 3. Comorbidities were common, affecting >10% of patients. In addition, 222 patients (60%) patients underwent major abdominal surgery.
Characteristics of study patients undergoing major elective surgery.
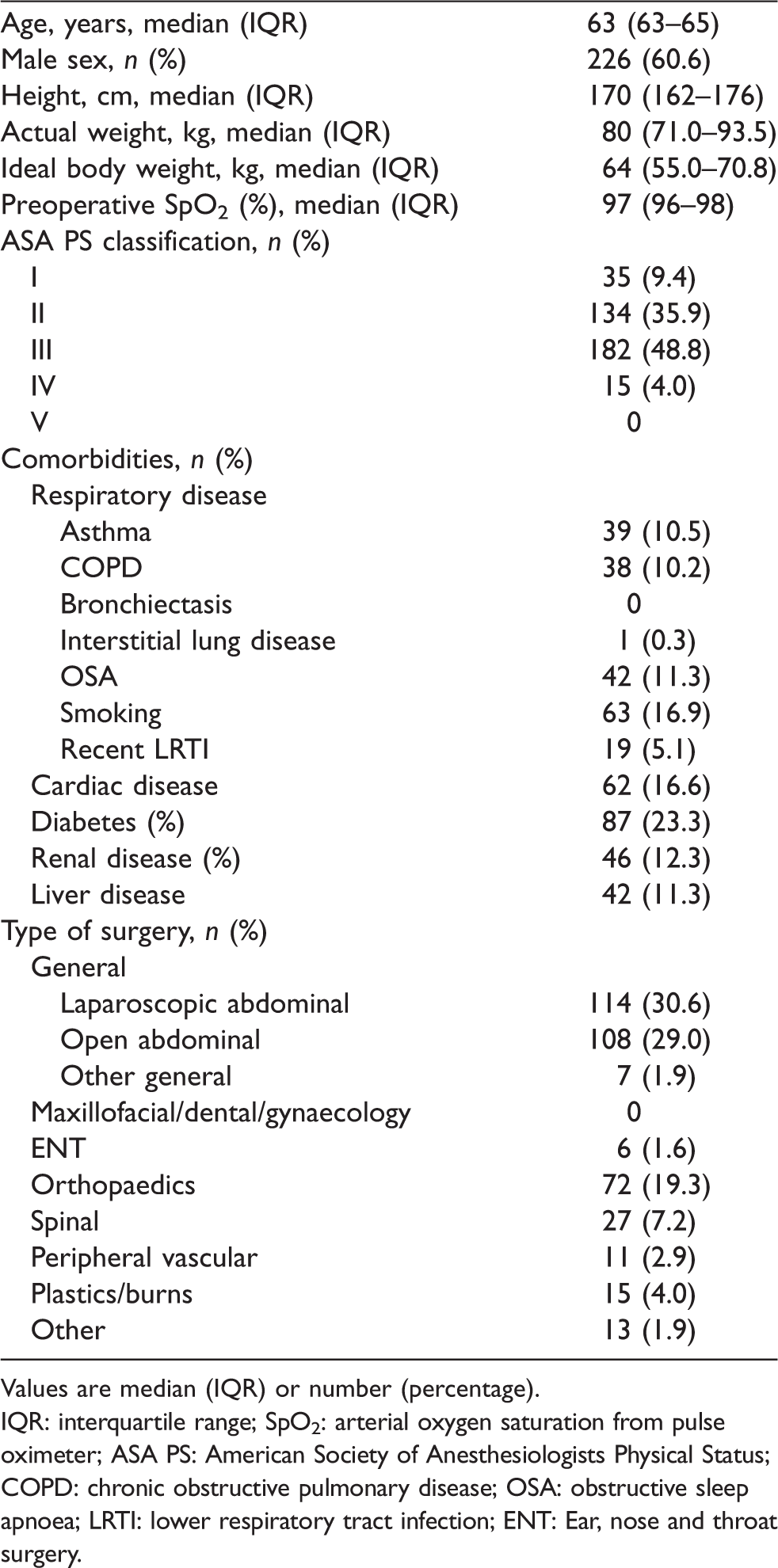
Values are median (IQR) or number (percentage).
IQR: interquartile range; SpO2: arterial oxygen saturation from pulse oximeter; ASA PS: American Society of Anesthesiologists Physical Status; COPD: chronic obstructive pulmonary disease; OSA: obstructive sleep apnoea; LRTI: lower respiratory tract infection; ENT: Ear, nose and throat surgery.
Intraoperative and postoperative FiO2 and oxygenation
As shown in Table 2, intraoperative FiO2 administration was initially high, with a median lowest FiO2 and SpO2 of 0.45 (IQR 0.40–0.51) and 97% (IQR 96–98%), respectively. Similarly, the median post-induction and pre-emergence median PaO2 were 237 mmHg (IQR 171–291 mmHg) and 189 mmHg (IQR 145–239 mmHg), respectively. In the PACU, the median PaO2 was 158 mmHg (IQR 120–192 mmHg; Table 2 and Figure 1).
Intraoperative and postoperative oxygen therapy and resultant oxygenation for patients undergoing major elective surgery.
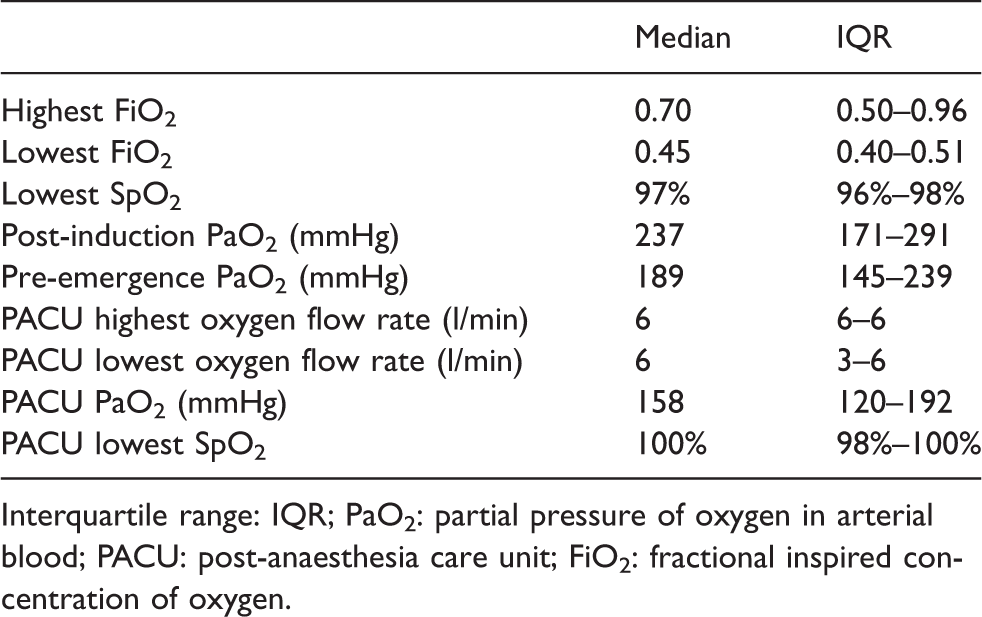
Interquartile range: IQR; PaO2: partial pressure of oxygen in arterial blood; PACU: post-anaesthesia care unit; FiO2: fractional inspired concentration of oxygen.
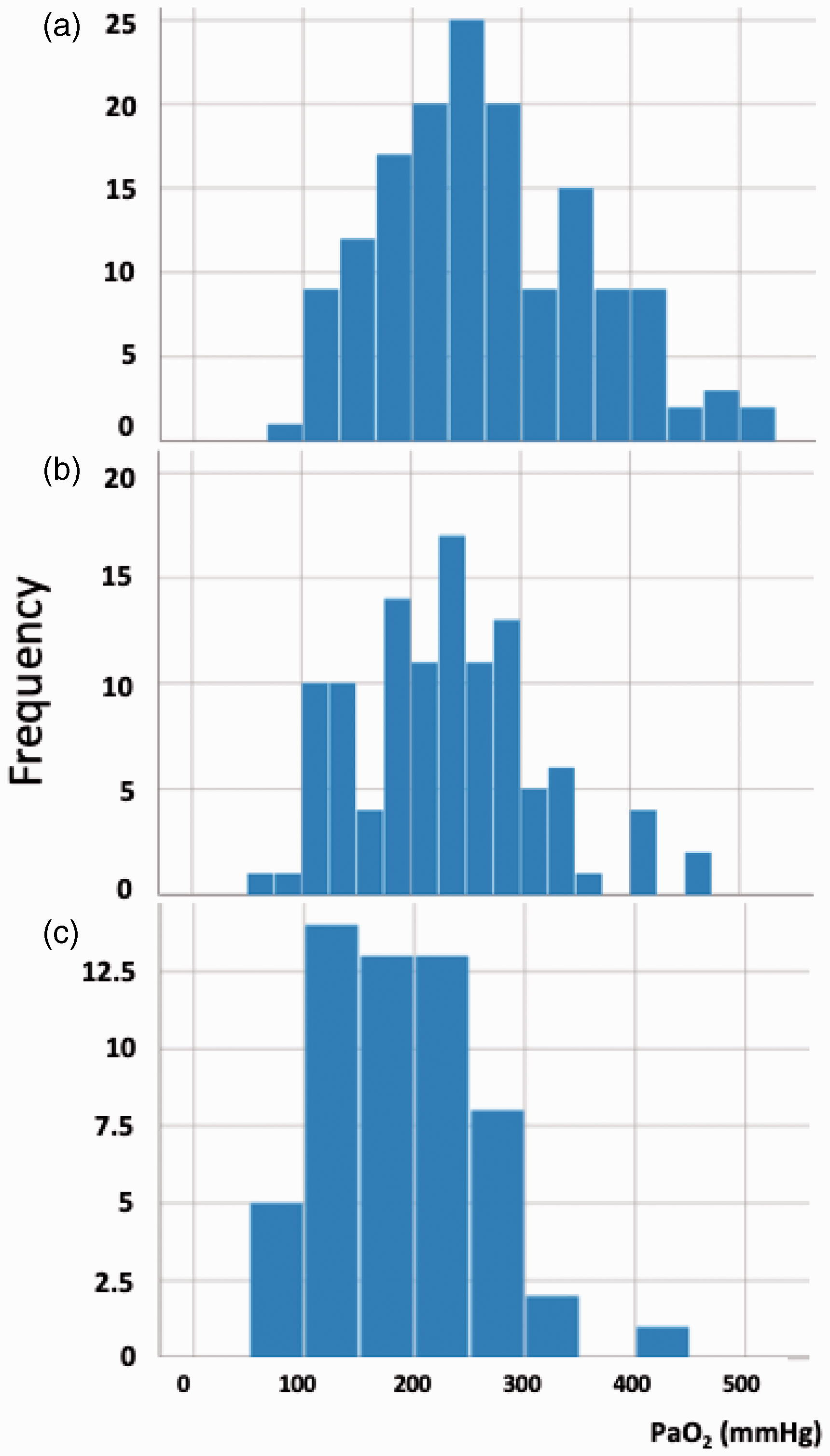
Frequency distribution of partial pressure of oxygen in arterial blood (PaO2; mmHg). (a) Distribution of PaO2 on the first arterial blood gas. (b) Distribution of PaO2 on the second intraoperative gas. (c) Distribution of PaO2 values in the post-anaesthesia care unit (PACU).
Titration of intraoperative FiO2
Paired data on FiO2 were available from the first and second intraoperative ABG in >90% of participants. In 35%, the FiO2 was unchanged, and in 48% of participants, the FiO2 decreased. In the remaining 58 participants (17%), the FiO2 increased by a median of 10% (IQR 4.8–21.3%)%. The distribution of the initial PaO2 from the first intraoperative ABG according to such FiO2 titration is shown in Figure 2.
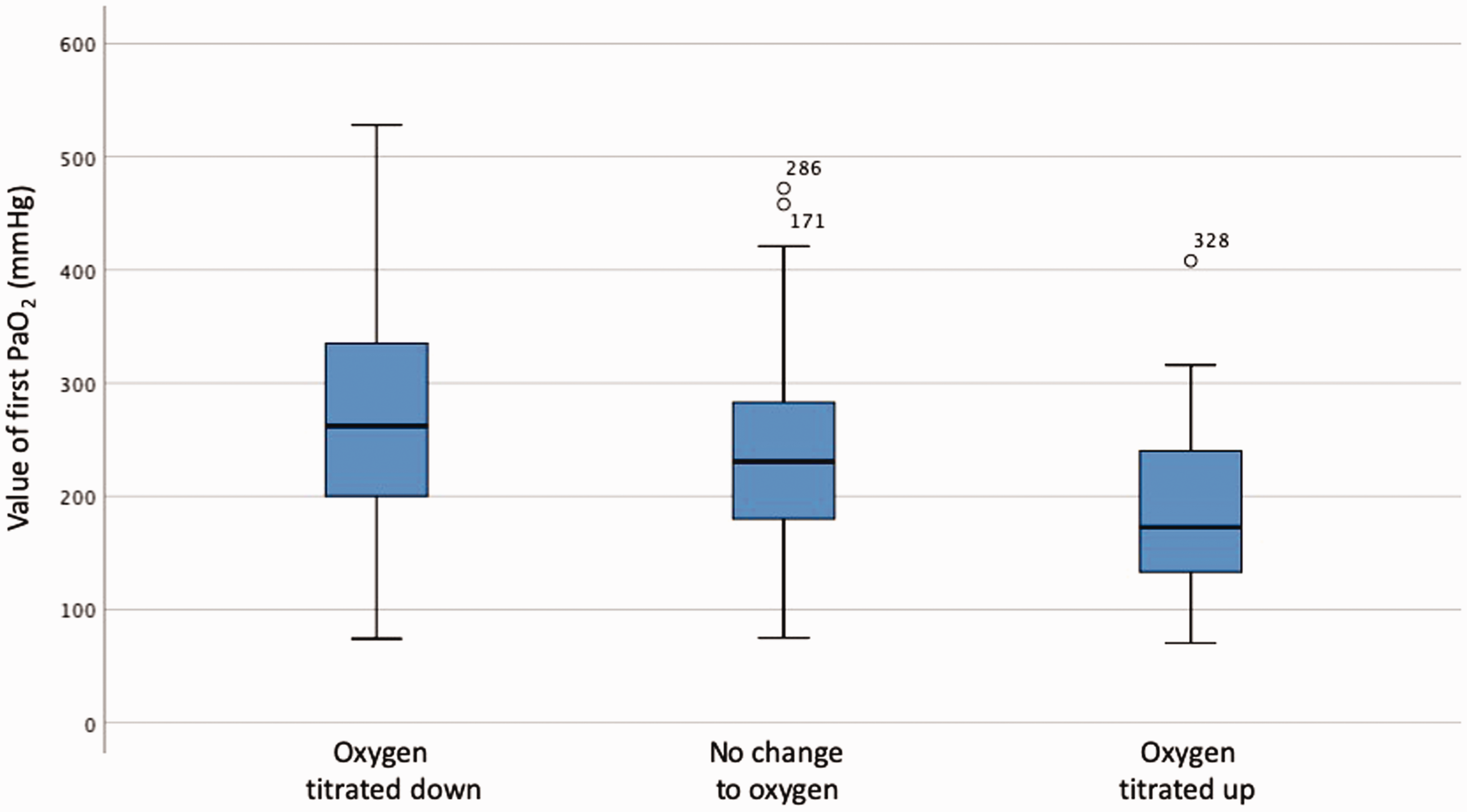
PaO2 of the first intraoperative arterial blood gases (ABG) according to oxygen titration response.
Incidence of hypoxaemia and hyperoxaemia
Based on pulse oximetry, hypoxaemia (SpO2 < 91%) occurred in seven (1.9%) participants intraoperatively and seven (1.9%) participants postoperatively. Based on ABG analysis, hypoxaemia (PaO2 < 60 mmHg) did not occur in any participants intraoperatively nor did it occur on postoperative ABG analysis.
Overall, 70% of the ABGs analysed in this study demonstrated hyperoxaemia (PaO2 >150 mmHg). Intraoperatively, a PaO2 >150 mmHg and a PaO2 >200 mmHg were seen in at least 64% and 41% of ABGs, respectively. In the PACU, a PaO2 >150 mmHg and a PaO2 >200 mmHg were seen in 54% and 21%, respectively (Table 3). The details of oxygen therapy in specific subgroups of patients are shown in online Supplemental Table S1. In patients with known COPD, oxygen administration remained liberal, and the resulting PaO2 was similar to that of patients without COPD.
Incidence of hyperoxaemia in patients undergoing major elective surgery.

ABG: arterial blood gas.
Discussion
Key findings
In this retrospective study of oxygen practice by a large number of anaesthetists during major surgery, a ‘liberal’ oxygen strategy was most common and was frequently associated with hyperoxaemia. Moreover, despite documented hyperoxaemia, anaesthetists decreased FiO2 in less than half of patients, and such hyperoxaemia continued into the immediate postoperative period.
Relationship to previous studies
Our study describes all the components of oxygen therapy and the incidence, severity and duration of hyperoxaemia during and after anaesthesia for a large number of patients and anaesthetists.
Other studies, however, have addressed one or more aspects of such therapy. In a large retrospective study, investigators assessed a large cohort of patients undergoing anaesthesia in the USA and found that FiO2 and SpO2 were consistently high. 12 However, they did not report PaO2 values, or the incidence, severity and duration of hyperoxaemia, or its presence or absence in the PACU. A large retrospective Canadian study of all recorded pulse oximetry readings during surgery from more than 95,000 electronic anaesthesia charts reported a 56% incidence of SpO2 readings of 99% and 100%, and only 0.2% of values in the range of 90%–92%. 2 However, the associated FiO2 and PaO2 were unknown.
More recently, Suzuki et al. performed a multicentre observational study of 1498 patients undergoing general anaesthesia in Japan. They found that >90% of patients received an FiO2 of between 0.31 and 0.6, only 1% of patients received a FiO2 of < 0.31 and >80% of patients were exposed to an arterial oxygen saturation >98%. However, PaO2 values and changes in FiO2 therapy were unknown. 21
Study implications
If our hospital is typical of broader Australian practice, it suggests that many Australian anaesthetists apply a liberal approach to oxygen therapy and deliver supra-physiological PaO2 levels during major surgery. They also imply that such levels are maintained after surgery. Finally, they suggest that they typically do not adjust FiO2 to achieve lower PaO2 levels.
Study strengths and limitations
This study assessed the incidence, severity and duration of hyperoxaemia using ABG analysis during and immediately after major surgery. It also reported on whether anaesthetists modify FiO2 in response to intraoperative PaO2. It included data from several hundred patients treated by more than 100 attending anaesthetists, lending a degree of robustness and face validity to such findings. Whilst we accept that our hospital may not represent broader Australian practice, we do believe, given they have many features consistent with other large hospitals, that our findings are likely to be generalisable to similar centres. Given that this sub-study had not been conceived at the time the parent study was executed, treating anaesthetists could not have modified their practice with regard to oxygen administration during this study, mitigating selection and ascertainment bias and increasing internal validity. By measuring ABG analysis at specific timepoints distinct from the induction and emergence phases of anaesthesia, our study was able to assess practice specifically during the maintenance phase of anaesthesia. The use of ABG added further precision compared to previous work, which had relied solely on arterial saturation from a pulse oximeter.20,21,23,24 Furthermore, mechanical ventilation and PEEP were standardised according to recently described current practice to allow the focus to be only on FiO2 titration and the resulting systemic oxygenation. 23
Despite the above strengths, our study also carries several limitations. Our definition of hyperoxaemia was a PaO2 of >150 mmHg. This definition is consistent with previous studies.25 However, hyperoxaemia has been variably defined in the clinical literature as > 100 mmHg and in other reports as > 300 mmHg. Our inclusion criteria aimed to capture patients who were exposed to oxygen therapy for a significant period of time (i.e. more than two hours) and also those in whom the treating anaesthetists had decided to place an arterial line. This implies that our cohort had a higher level of acuity. We measured oxygen tension via an ABG at three predefined points during surgery, and we are therefore unable to comment on oxygen tension between these timepoints. Notably, we did detect episodes of apparent hypoxaemia based on SpO2 traces. This may have been due to artefactual readings or hypoxaemia that occurred between the scheduled ABGs, and thus was not detected on ABG analysis. However, our ABG intervals were not intended to capture episodes of hypoxaemia. Approximately 5% of ABGs were missing. However, it is unlikely that such missing values would materially alter the study findings. The described practice is at variance with the British Thoracic Society Guidelines. 20 However, these guidelines are in contrast to those from the World Health Organization (WHO), which recommend an inspired fraction of oxygenation of 0.8 and no oxygenation targets (SpO2 or PaO2), which remains a source of controversy.26–29 We also did not record other factors that may have influenced the anaesthetists’ practice with regard to FiO2 administration such as major haemodynamic instability or haemorrhage, anaemia or dyshaemoglobinaemia. In the interpretation of our findings, we assumed that changes in oxygen administration would most likely occur in response to interpretation of the ABG result. We further recognise that it is also possible that in some cases, oxygen titration may have occurred for reasons other than in response to the ABG result obtained. Finally, our study is retrospective and single centre in nature, with all the inherent limitations of such studies. However, it describes the practice of what we believe to be a typical tertiary hospital in a developed country and of more than 100 different anaesthesiologists, suggesting a degree of generalisability. There are no departmental policies or directives with regard to oxygen therapy in our hospital, and the large number of anaesthetists participating in this study are likely to represent a large cross section of practice. Furthermore, given that our practice at the Austin Hospital has been shown to be consistent with a number of other metropolitan and rural centres in Victoria with regard to the approach to controlled mechanical ventilation, when this was previously investigated by our group, we suggest it would be unlikely that our practice with regard to oxygen therapy would not be representative of other Victorian hospitals as well. 23 We acknowledge that given anaesthetists were aware of participation in a trial regarding mechanical ventilation; such knowledge may have influenced their management of oxygen administration. However, there was no directive given to the anaesthetists with regard to the management of oxygen during conduct of the trial, and therefore oxygen administration was managed at their discretion. We also acknowledge that a given anaesthetist may have been involved in the parent trial more than once. Thus, it is possible that management related to oxygen administration may have been modified with subsequent exposures to the trial. Finally, the clinical meaning of the hyperoxaemia that we describe is unclear and cannot be addressed by our study. It remains unclear whether the inspired oxygen fraction administered by anaesthetists in this study was optimal or suboptimal. We also acknowledge that it is still possible that the high FiO2 observed may prove to have better outcomes than lower FiO2. However, previous reports in critically ill patients have reported a higher incidence of atelectasis, with higher fractional inspired oxygen concentrations and arterial oxygen tensions. 30 Further studies focusing on the incidence of atelectasis or other lung complications specifically in operating room patients potentially affected by high FiO2 and PaO2 levels are necessary to assess the possible clinical consequences of hyperoxaemia during anaesthesia, if any exist, and to identify outcome measures that are potentially directly relevant to oxygen therapy.
Conclusions
In our retrospective cohort study of oxygen therapy during and after major surgery, we found that anaesthetists adopted a liberal approach to oxygen therapy. Consistent with our hypothesis, we found that anaesthetists delivered a high FiO2, and this approach resulted in a high incidence of intraoperative and early postoperative hyperoxaemia. Further studies are now required to evaluate the feasibility, safety and efficacy of a restrictive approach to oxygen administration and of how the targeting of a physiological PaO2 influences outcomes perioperatively.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X20905320 - Supplemental material for Frequency of hyperoxaemia during and after major surgery
Supplemental material, sj-pdf-1-aic-10.1177_0310057X20905320 for Frequency of hyperoxaemia during and after major surgery by Dharshi Karalapillai, Laurence Weinberg, Philip J Peyton, Louise Ellard, Raymond Hu, Brett Pearce, Chong Tan, David Story, Mark O’Donnell, Patrick Hamilton, Chad Oughton, Jonathan Galtieri, Anthony Wilson, Glenn Eastwood, Rinaldo Bellomo and Daryl Jones in Anaesthesia and Intensive Care
Supplemental Material
sj-pdf-2-aic-10.1177_0310057X20905320 - Supplemental material for Frequency of hyperoxaemia during and after major surgery
Supplemental material, sj-pdf-2-aic-10.1177_0310057X20905320 for Frequency of hyperoxaemia during and after major surgery by Dharshi Karalapillai, Laurence Weinberg, Philip J Peyton, Louise Ellard, Raymond Hu, Brett Pearce, Chong Tan, David Story, Mark O’Donnell, Patrick Hamilton, Chad Oughton, Jonathan Galtieri, Anthony Wilson, Glenn Eastwood, Rinaldo Bellomo and Daryl Jones in Anaesthesia and Intensive Care
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding supplied by the Australian and New Zealand College of Anaesthetists Australian and New Zealand College of Anaesthetists grant no: 16/008.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.