
Abstract
In the absence of upper airway patency, supraglottic methods of oxygen delivery become ineffective. We present two semi-elective difficult airway cases where oxygenation via the supraglottic route was deemed impractical due to upper airway obstruction. In order to facilitate safe airway management, apnoeic oxygenation was delivered via a narrow bore transtracheal cannula using a flow-regulated oxygen insufflator. The potential for safely prolonging apnoea time with this technique in both elective and emergency settings is discussed.
Keywords
Introduction
Airway management techniques in laryngeal surgery include endotracheal intubation as well as tubeless techniques, such as jet ventilation or apnoeic oxygenation (e.g. Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE)). The latter afford unobstructed views of and surgical access to the glottis and periglottic structures whilst satisfying the primary goal of oxygenation. Additionally, their use may limit the risk of trauma-related airway complications by obviating the need for instrumentation of an already compromised airway. Both techniques require a patent upper airway for safe gas exchange as a prerequisite. Where endotracheal intubation is deemed unsafe or impractical for surgical reasons, and upper airway patency cannot be assured, an awake surgical tracheostomy is typically advised. However, this approach carries the risk of serious short- and long-term complications. We describe a safer alternative to tracheostomy whereby apnoeic oxygenation is delivered via a small-bore transtracheal cannula using a flow-regulated oxygen insufflator (Percutaneous Oxygen Insufflation (POI)) and discuss implications for elective and emergency airway management. Patient consent for this publication was sought and given.
Cases
Case 1
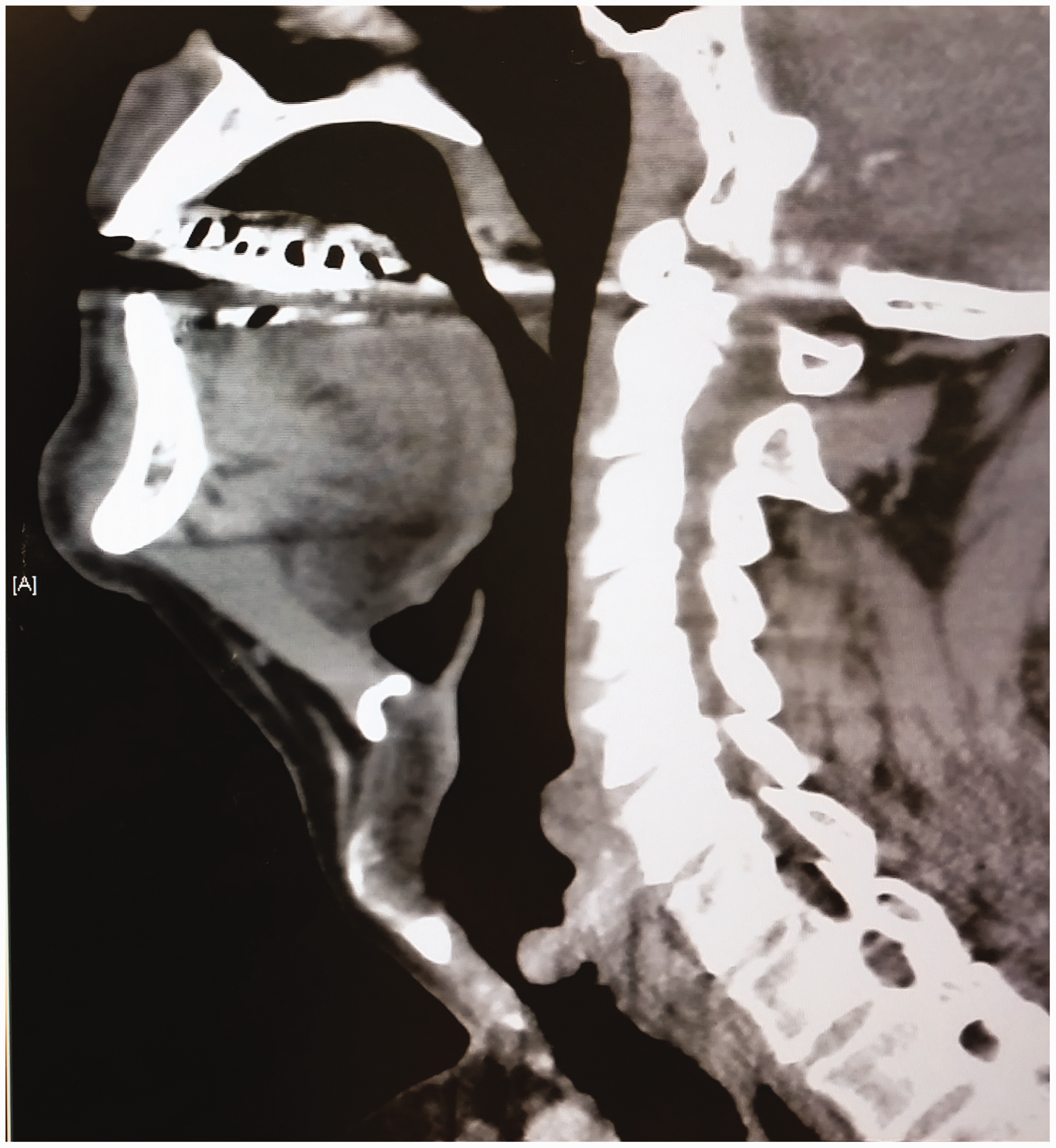
A 65-year-old obese male (body mass index 40 kg/m2) presented with a large base of tongue cancer causing near total airway occlusion (Figure 1). Progressive symptoms of shortness of breath, dysphagia and voice change were noted over a period of six months. On examination, he was breathing comfortably, and his vital signs were normal. Due to advanced disease, palliative radiotherapy was offered, with pre-radiotherapy tumour debulking in anticipation of post-radiation swelling. As nasendoscopic findings (Figure 2) indicated extreme difficulty with intubation and because an unhindered surgical field was deemed necessary, an awake tracheostomy was advised, but the patient adamantly refused this. Transtracheal jet ventilation (TTJV) was then considered as the primary airway management technique. However, TTJV is contraindicated in complete upper airway obstruction, which would almost certainly have occurred with induction of anaesthesia given the extensive tumour burden on computed tomography and nasendoscopy. Therefore, as a bridge to safe TTJV, transtracheal apnoeic oxygenation using a Rapid-O2™ oxygen insufflation device (Meditech Systems Ltd, Dorset, UK; Figure 3) was planned until surgical debulking of the tumour achieved sufficient upper airway patency. Conversion to a cuffed airway via wire-guided Seldinger technique was planned if required. Additionally, anterior neck landmarks were identified and marked in preparation for Can’t Intubate/Can’t Oxygenate (CICO) rescue in the event of cannula failure and failed laryngoscopy. As the cricothyroid membrane was easily palpable, timely emergency surgical front-of-neck access was considered feasible.

Computed tomography demonstrating a large base of tongue cancer.
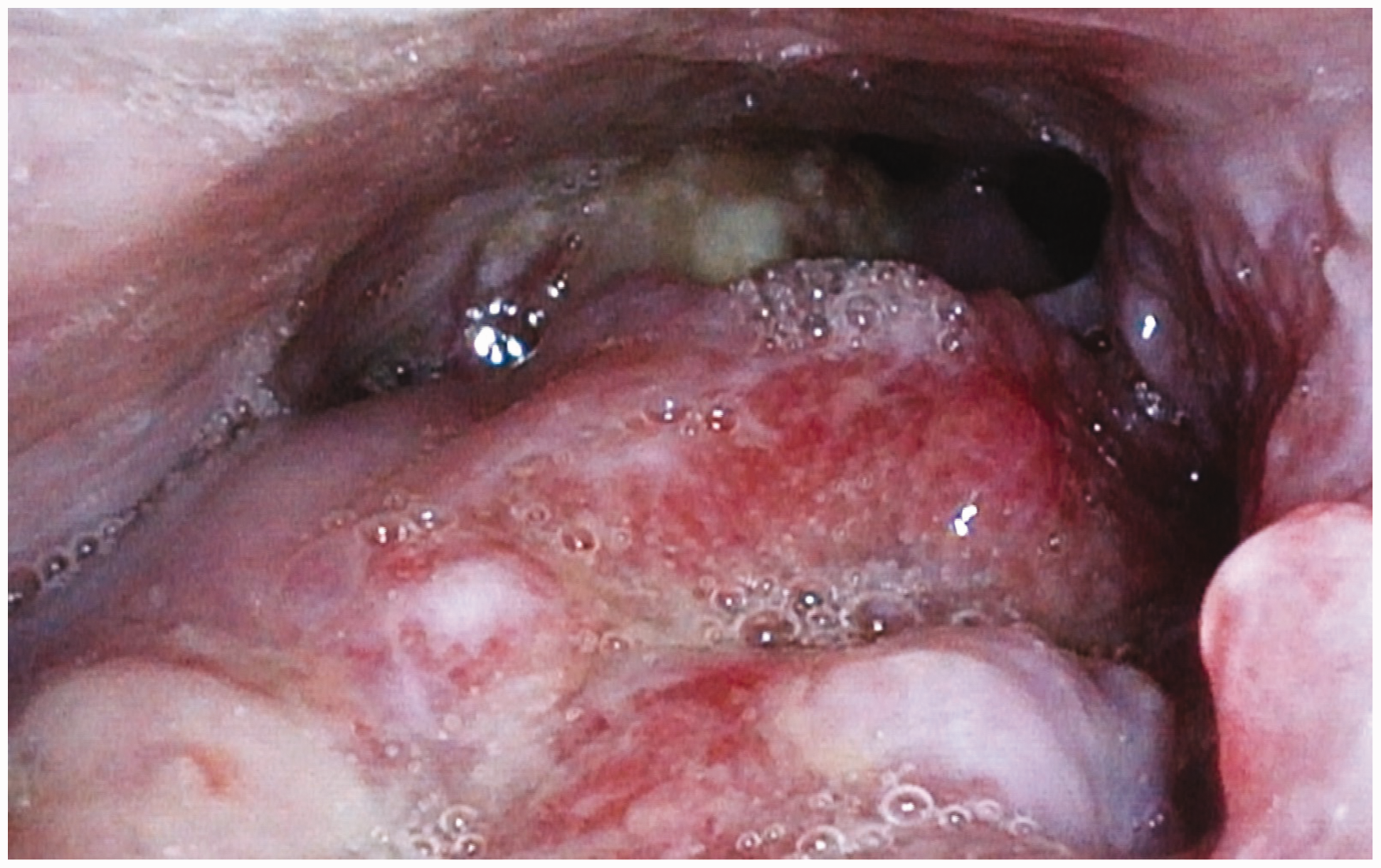
Large base of tongue cancer with limited view of glottic inlet as seen on nasendoscopy.
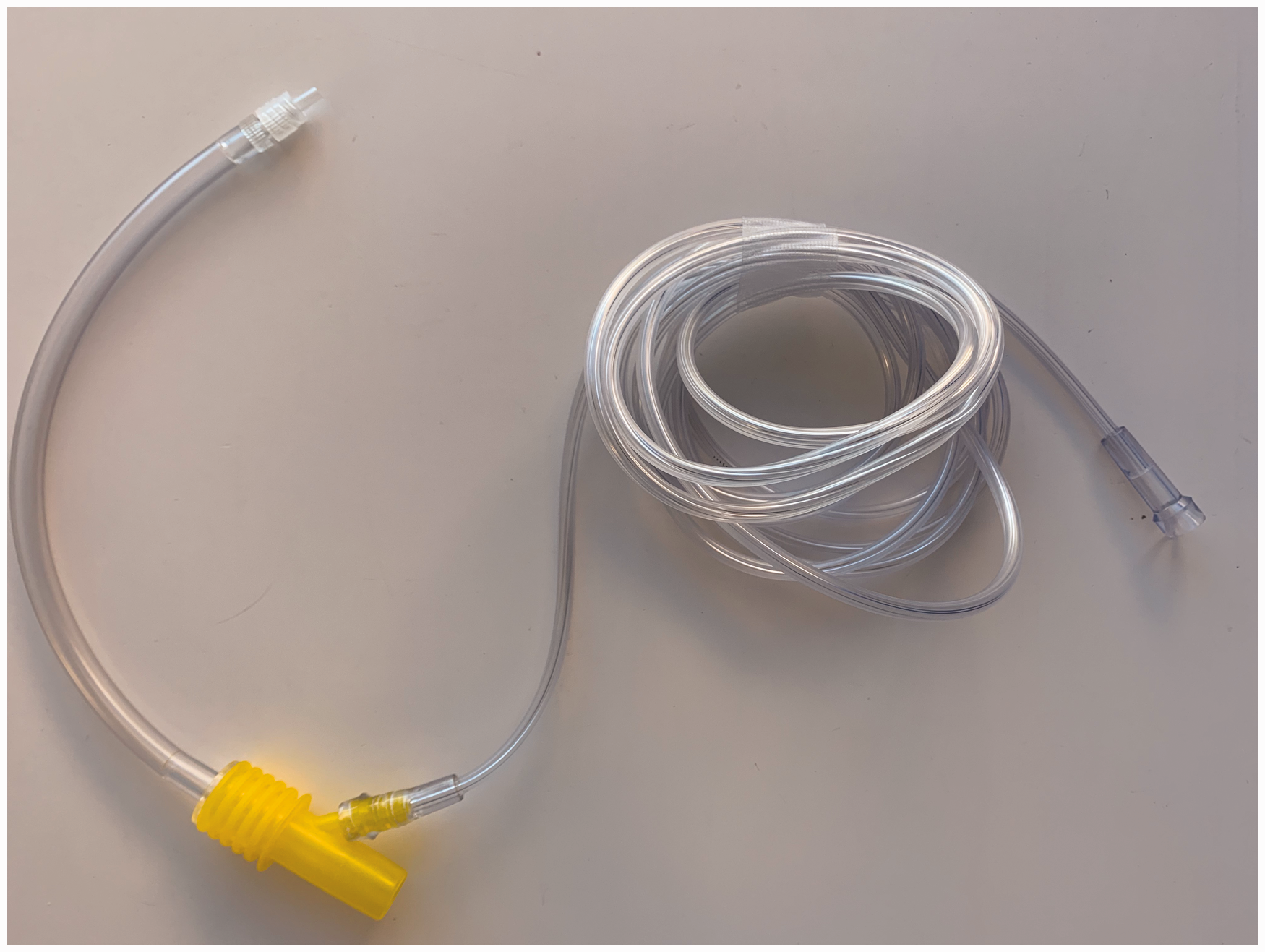
Rapid-O2 oxygen insufflation device (Meditech Systems Ltd, Dorset, UK).
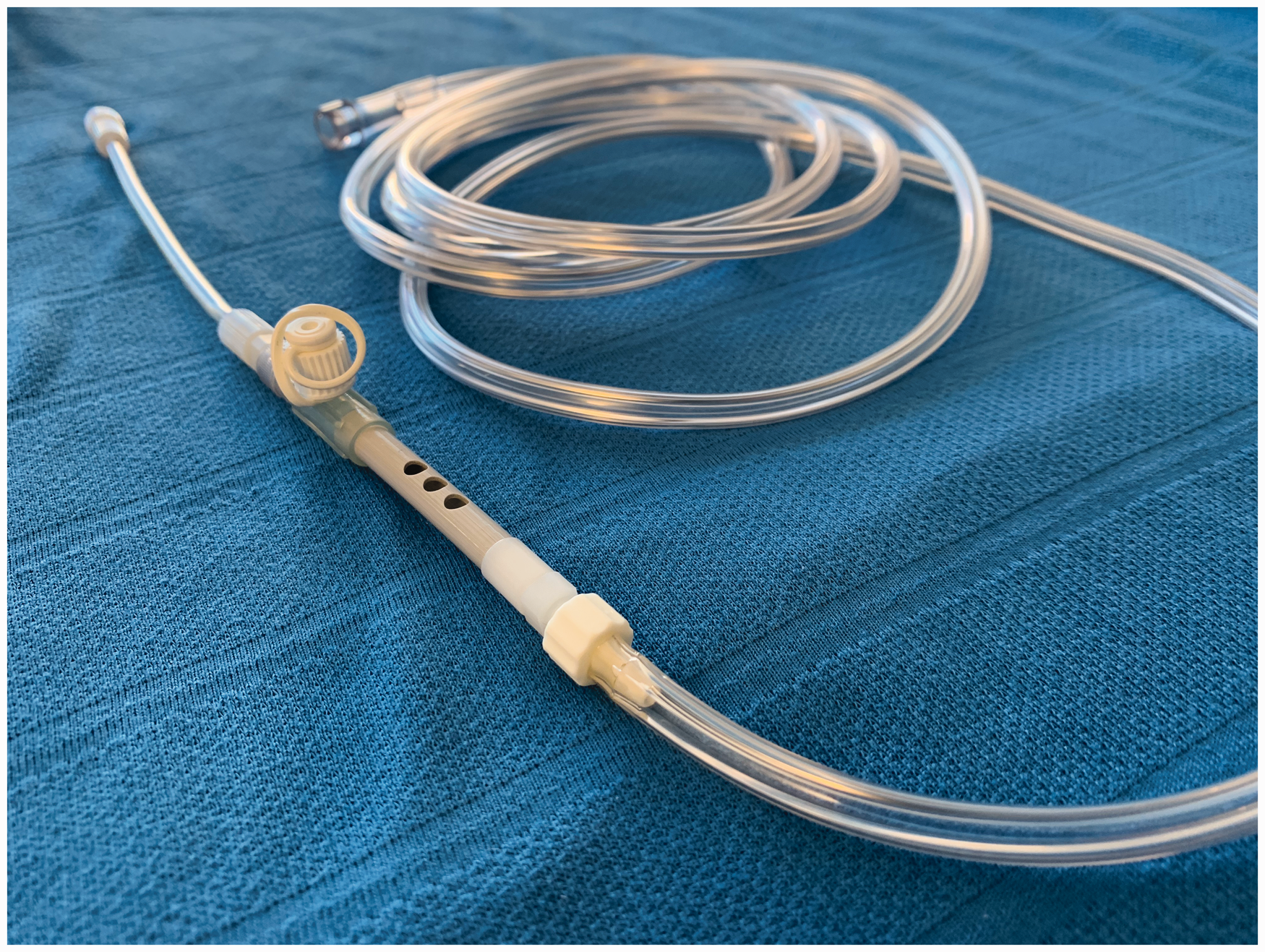
After application of standard monitoring, midazolam 2 mg was administered and the skin and subcutaneous tissue overlying the cricothyroid membranes were infiltrated with lidocaine 2%. Awake cricothyroidotomy using a 6Fr Cook Transtracheal Catheter (Cook Medical Inc., Bloomington, IN, USA) was performed with the catheter sutured to the skin. While still awake, gentle application of TTJV using the Manujet III ventilator (VBM, Sulz am Neckar, Germany) and oxygen insufflation using the Rapid-O2 were performed to test functionality and safety of the equipment prior to induction. Anaesthetic induction and maintenance were achieved with infusions of propofol and remifentanil, and rocuronium boluses. Once the patient was anaesthetised, debulking was achieved with radiofrequency Coblation (Smith & Nephew, London, UK) with the patient maintained in a Trendelenburg position to prevent passage of irrigation fluid and blood into the lower airway. Oxygenation technique involved delivery of 1 L O2 (4 s at 15 L/min) via the Rapid-O2 when oxygen saturation reached 93% (approximately every 6–8 min). This typically resulted in a prompt rise of saturation to 100% within 25–30 s. Sidestream capnography added to the Rapid-O2 via a three-way tap (Figure 4) provided immediate confirmation of alveolar oxygen delivery prior to a rise of saturation with a corresponding end-tidal carbon dioxide (ETCO2) waveform lasting 14 s.
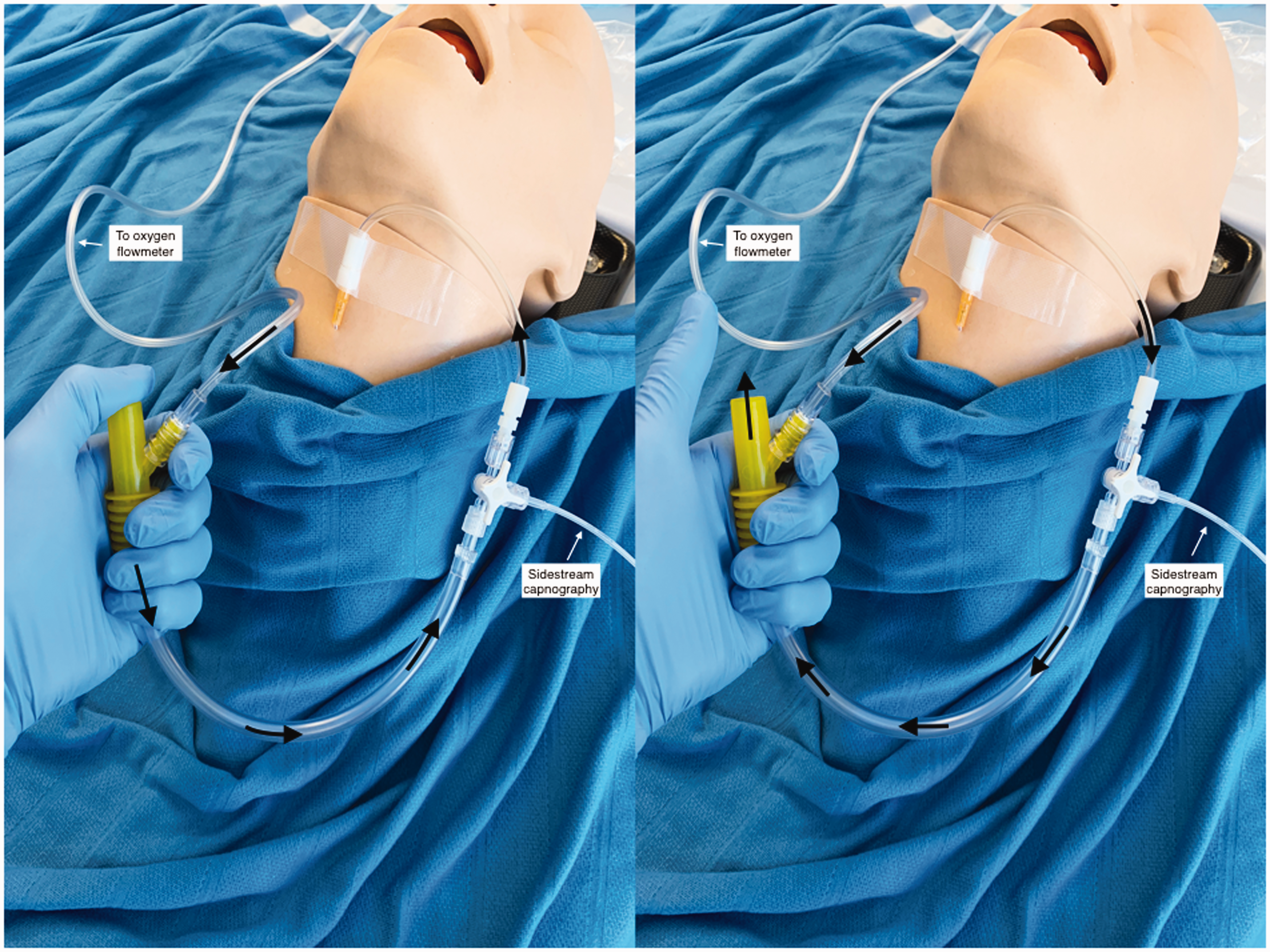
Rapid-O2 (Meditech Systems Ltd, Dorset, UK) with sidestream capnography.
At 60 min, upper airway patency was achieved by debulking allowing for safe conversion to transtracheal jet ventilation. The peak ETCO2 was 115 mmHg, pH 7.27, with stable haemodynamics. Due to the unanticipated extent of debulking required, endotracheal intubation and overnight mechanical ventilation were deemed necessary in order to allow for a reduction in airway swelling prior to resumption of breathing via the natural airway. Identification of the glottic inlet by videolaryngoscopy, however, remained difficult due to anatomical distortion. Air bubbling at the glottis inlet from TTJV assisted bougie placement for endotracheal tube insertion. The patient was extubated the following day and made an uneventful recovery.
Case 2
A 60-year-old male presented for microlaryngoscopy and resection of a subglottic mass on a background of increasing shortness of breath of several weeks’ duration. His significant past medical history included a prolonged intensive care unit stay three years prior to admission due to a massive pulmonary embolus requiring tracheostomy formation. Computed tomography obtained on admission revealed a posteriorly-based subglottic mass causing 80%–90% narrowing of the tracheal lumen (Figure 5). On nasendoscopy intermittent glottic occlusion was noted on exhalation due to the subglottic mass acting as a ball-valve, with a normal glottic and supraglottic airway.
Computed tomography demonstrating a large, posteriorly-based, subglottic mass.
Avoidance of endotracheal intubation was considered desirable in order to both provide an unhindered surgical field and avoid the risk of intubation-related trauma of the tumour. TTJV was therefore chosen as the primary ventilatory management plan. However, jet ventilation below the level of the ball-valve posed the significant risk of obstruction to exhalation causing baro- and volutrauma. To avoid these risks, transtracheal apnoeic insufflation of oxygen was planned until a patent airway for exhalation could be visualised and secured. In the event of failure of the primary airway management plan, timely rescue by either laryngoscopy and intubation or emergency cricothyroidotomy were deemed feasible given the patient’s normal supraglottic anatomy and palpable cricothyroid membrane.
After application of standard monitoring, midazolam 2 mg was administered and the skin and subcutaneous tissue overlying the lower cervical trachea were infiltrated with lidocaine 2%. Awake transtracheal cannulation was then performed using a 6Fr Cook Transtracheal Catheter. Anaesthetic induction and maintenance were achieved with infusions of propofol and remifentanil, and rocuronium boluses. Once the patient was anaesthetised, apnoeic oxygenation was provided via the Enk Oxygen Flow Modulator (Cook Medical Inc., Bloomington, IN, USA) (Figure 6) with a technique similar to that described for Case 1. Total apnoeic time was 20 min, after which a patent expiratory path could be visualised, thereby allowing for safe TTJV. Haemodynamic and respiratory parameters remained normal throughout the surgery. Once surgical resection was complete (via electrocautery) the patient was allowed to emerge from anaesthesia with resumption of spontaneous respiration. After a period of observation in the recovery unit, the transtracheal cannula was removed and the patient transferred to the ward. He was discharged home the following day and made an uneventful recovery.
Enk Oxygen Flow Modulator (Cook Medical Inc., Bloomington, IN, USA).
Discussion
Transtracheal catheterisation with TTJV is a well-established airway management technique in routine upper airway surgery, allowing for adequate ventilation whilst providing for an unhindered surgical field. 1 In the urgent setting, when faced with an anticipated difficult airway, this technique is also established as a means to facilitate a secondary intubation technique and avoidance of a tracheostomy. 2 Despite its appeal, safe use of this technique is limited to practitioners experienced in TTJV in the elective setting and the availability of specialised high-pressure source equipment, neither of which can be guaranteed in most settings. Crucially, while gentle test ventilation with TTJV can be performed in an awake patient who is maintaining some upper airway patency without obvious distress, an absolute requirement for utilising this technique under general anaesthesia is the assurance of a patent expiratory path via the supraglottic airway. The aim of our report is to highlight the utility of POI as an alternative oxygenation technique to both TTJV and THRIVE, and which utilises equipment which is simple, cheap and increasingly stocked in operating theatres in Australia and New Zealand. 3 Most important, the technique is safe and effective even in complete upper airway obstruction.
Devices available for POI include the Rapid-O2 oxygen insufflation device and the Enk Oxygen Flow Modulator (Figures 3 and 6). These simple devices connect at one end to a standard oxygen flowmeter and at the other to a Luer Lock cannula. Finger occlusion of the T-piece in the former and a set of holes in the latter allows for oxygen to flow to the cannula, whilst finger release allows for flowmeter gas to vent to the atmosphere and passive expiration.
Features of the Rapid-O2 which make it the ideal rescue oxygenation device in CICO events 4 include the need to occlude only one hole by using the thumb (intuitive and simple), and delivery of a known volume of gas under very low pressure (negligible risk of barotrauma). As a true on/off device, passive expiration occurs, and flowmeter oxygen can vent to the atmosphere when the thumb is removed from the jet oxygenation hole. The risk of breath stacking is therefore limited. Additionally, feedback with regard to cannula kinking or misplacement is manifest as palpable resistance against the thumb, allowing for early detection of technique failure. From a cost viewpoint, the Rapid-O2 is inexpensive and therefore its frequent use is affordable. All these features are equally advantageous in the non-CICO setting.
As insufflation pressures are low, 14G angiocatheters may be used and offer the advantage of availability, familiarity and safety. Our preference, however, is for the 14G non-safety Insyte™ cannula (Becton Dickinson Infusion Therapy Systems Inc., Sandy, UT, USA) (Figure 7), as it requires a lower insertion pressure and has a stronger memory for re-forming a patent lumen after kinking. 5 Alternatively, dedicated airway cannulas may be used such as the 6Fr Cook Transtracheal Catheter (Figure 7), which offers the advantages of greater kink resistance and added length (7 cm), which reduces the risk of dislodgement. Additionally, a groove on the metal hub facilitates suturing of the catheter to the skin.
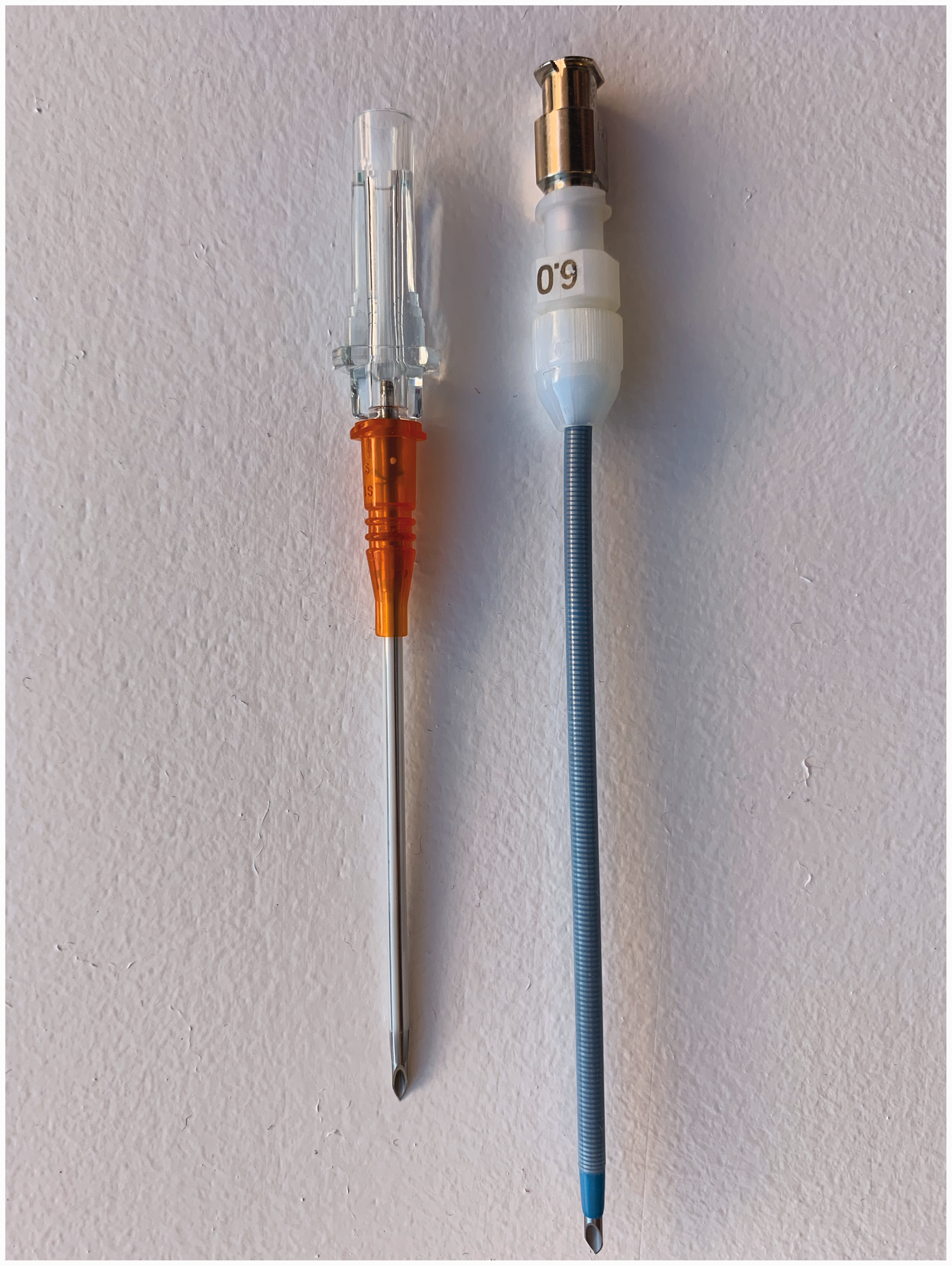
14G non-safety Insyte™ cannula (Becton Dickinson Infusion Therapy Systems Inc., Sandy, UT, USA) (left), and 6Fr Cook Transtracheal Catheter (Cook Medical Inc., Bloomington, IN, USA) (right).
Efficacy of the Rapid-O2 for rescue oxygenation in the CICO setting has already been described. 4 Ours is the first report on its efficacy in achieving normoxia in the non-CICO setting in a human. Ours is also the first report on use of sidestream capnography in conjunction with flow-regulated oxygenators for confirmation of alveolar oxygen delivery. Using an oxygenation strategy based on the data from wet lab studies by Heard et al. 6 we were able to provide effective oxygenation over an apnoea time of 1 h in an obese patient in the Trendelenburg position. With each insufflation of 1L oxygen, saturation increased from 93% to 100% within 20–30 s.
The rationale for using the oxygenation strategy advocated by Heard et al., whereby re-insufflation is provided only when oxygen saturation drops, is to avoid over-insufflation with its deleterious effects. In Case 1, re-insufflation was provided every 6–8 min and return of ETCO2 trace to baseline occurred at 14 s. After 60 min of apnoea, the peak ETCO2 of 115 mmHg and pH of 7.27 seem lower and higher respectively than the levels that would be predicted by other studies of apnoeic insufflation, 7 suggesting that even at such low frequency of oxygen insufflation, there was some evidence of ventilation. Using a return of ETCO2 to baseline as the trigger for re-insufflation, rather than an oxygen saturation value, may allow the operator to safely increase insufflation frequency. The addition of sidestream capnography to POI therefore raises the possibility of extending the use of such devices from mere oxygenators to devices capable of safe ventilation, thereby extending safe apnoea time.
In addition to facilitating safe oxygen insufflation and ventilation, the addition of sidestream capnography to the oxygenation strategy allows for immediate confirmation of alveolar oxygen delivery after thumb release, thereby obviating the need to wait 20–30 s for a rise in oxygen saturation as confirmation. Under the stressful conditions of a CICO situation, the immediate presence of an ETCO2 trace would provide immediate confirmation of successful rescue and the confidence to wait for a saturation response, whilst its absence would allow for early recognition of failure and timely forward progression. Further simulation studies are needed in order to demonstrate the impact of adding capnography to the Rapid-O2 on team performance in CICO situations.
The utility of high flow nasal oxygenation in management of the difficult airway in both elective and emergency situations is well established.
8
Extending the apnoeic window reduces and often obviates the need for repeated rescue facemask ventilation and airway instrumentation under time pressure,
9
converting what might otherwise be a hurried and hazardous task of securing the airway into a safer and smoother event. Additionally, for patients undergoing surgery on the upper airway, apnoeic oxygenation using THRIVE is effective at maintaining oxygenation and limiting excessive hypercapnia whilst providing for an unhindered surgical field.
10
A limitation of this technique, however, is the absolute requirement for a patent upper airway, which may not be present when critical obstructive pathology exists or when surgical equipment and/or manipulation obstruct the upper airway. In such circumstances, where upper airway patency cannot be assured, POI is an effective, simple, and minimally invasive method of oxygenation, with a number of potential advantages in both emergency and elective airway management:
Prolongation of safe apnoea time. In elective upper airway surgery, POI allows for significant prolongation of safe apnoea time prior to establishing a more definitive airway, which may include endotracheal intubation or commencement of safe jet ventilation as in our report. Alternatively, the entire procedure may be performed using POI, allowing the patient to regain control of their airway at case completion. POI may therefore be considered a safe alternative to tracheostomy when the risk of airway soiling is low and where postoperative tracheostomy is not required or is refused. Avoidance of airway instrumentation. POI may obviate the need for instrumentation of an at-risk airway thereby limiting or avoiding the associated risk of airway trauma. Safe extubation strategy. A transtracheal or transcricothyroid cannula may be left in place whilst the patient is observed in the recovery ward or intensive care unit with reapplication of POI in case of oxygen desaturation. Priming for CICO rescue. In the emergency setting, a risk of progression to a CICO situation can usually be identified in advance of critical desaturation.
9
In this setting, prophylactic cannula cricothyroidotomy (PCC) with a view to performing POI ensures that the team is primed to perform CICO rescue with zero delay when CICO is declared. This proactive strategy, whereby supraglottic and infraglottic approaches are integrated as opposed to being viewed as separate events in the course of an evolving airway crisis, is a departure from the reactive approach that teams commonly use to manage an airway crisis, that is, to wait until critical hypoxia triggers preparation for CICO rescue.
A number of alternatives to the Rapid-O2 currently exist for POI via narrow-bore cannulae. Jet ventilation using pressure-driven devices such as the Manujet is well established in both elective and emergency airway care but requires expertise and specialised equipment. With misuse, high airway pressures may cause significant harm or death and thus jet ventilation is absolutely contraindicated if passive expiration cannot be assured. 11 Automatic ventilators featuring a pressure monitor and automatic cut-off when airway pressure is raised may limit the risk of pressure-related complications in this setting but are not widely available. The Ventrain® (Dolphys Medical BV, Eindhoven, Netherlands) allows for oxygen insufflation under low pressure like the Rapid-O2, but with the substantial benefit of active expiration (termed Expiratory Ventilatory Assistance). 12 Safer normal minute ventilation is therefore possible, even in total upper airway obstruction. However, compared with the Rapid-O2, the Ventrain is currently more expensive, less well-known and its availability less widespread. Its design, which requires two-finger operation as opposed to a single thumb, is somewhat less intuitive.
POI carries with it a number of potential limitations. First, as passive expiration via the percutaneous cannula is limited by its small diameter, normal minute ventilation is unachievable. The resulting hypercapnia may therefore limit the duration of safe POI. In Case 1, we chose to commence ventilation at an ETCO2 of 115 mmHg (apnoea time 60 min) with no intra- or postoperative adverse events. Whilst there is currently no evidence to suggest an absolute level above which the partial pressure of CO2 should not rise we nevertheless acknowledge this degree of hypercapnia may be considered excessive by some practitioners. Based on a large number of case reports and series, however, severe respiratory acidosis under general anaesthesia can be tolerated under apnoeic normoxic conditions with complete recovery (ETCO2 and apnoea time approximately 100 mmHg and 30 min respectively). 10 Second, the efficacy of POI may deteriorate once a previously obstructed upper airway becomes patent. In Case 1 we found that as surgical debulking created a more patent upper airway, maintaining stable oxygenation through POI became more difficult. This may have been because POI establishes a high oxygen content reservoir in the upper airway below the obstruction, but once this obstruction is relieved, insufflated oxygen preferentially escapes via the upper airway. Third, the efficacy of POI may be limited by extensive atelectasis caused by obesity or pulmonary disease, which may necessitate positive pressure ventilation for adequate oxygenation. Fourth, cannulae may kink, obstruct or dislodge during an operation. Finally, airway needling may be associated with inadvertent vascular, nerve or oesophageal injury. Use of ultrasound to guide percutaneous cricothyroidotomy or tracheotomy, however, increases placement accuracy and reduces puncture-related complications. 13 Ultrasound may be particularly efficacious in patients with abnormal neck anatomy. 14
In keeping with current trends, prioritising oxygenation over ventilation is the key to successful airway management in extreme situations. In the absence of upper airway patency, however, supraglottic methods of oxygen delivery become ineffective. Our cases highlight the efficacy and safety of re-establishing and maintaining normoxia with POI via small-bore cannula in the elective setting, even in complete upper airway obstruction. The benefits of prolonging safe apnoea time in this setting include facilitation of a primary or alternative airway management technique (awake or asleep), avoidance of upper airway instrumentation and provision of an unhindered surgical field. In the appropriate patient, POI may also obviate the need for tracheostomy formation. In the emergency setting, where many potential CICO scenarios can be anticipated in advance, an opportunity often exists for performing PCC. POI in this setting is a simple and efficacious method of maintaining normoxia, whilst attempts at securing a definitive airway are carried out safely. Moreover, the addition of sidestream capnography to POI provides immediate confirmation of alveolar oxygen delivery, signifying that the patient is no longer at imminent risk of critical hypoxia and providing the team with time to mobilise resources, devise an airway management strategy and execute an airway intervention. Capnography may also allow for a safe increase in insufflation frequency, thereby enhancing CO2 elimination and further prolonging safe apnoea time.
In summary, POI is an effective and safe oxygenation technique for prolonging safe apnoea time when timely supraglottic methods of oxygenation are ineffective or impractical, and requires equipment that is simple, intuitive and increasingly available.
Footnotes
Author contributions
SW: concept, background research, main author, manuscript revision, manuscript final approval. SNP: manuscript revision, manuscript final approval. TAS: manuscript revision, manuscript final approval.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.