
Abstract
Prophylactic cannula cricothyroidotomy is a recognised technique for actual or potential difficult airway management, where it confers a number of technical and non-technical benefits. Oxygenation with this technique is traditionally achieved by way of pressure-regulated, high flow jet ventilation and requires specialised equipment and considerable expertise for safe use, neither of which are always readily available. As an alternative, we describe the management of two patients with progressive upper airway obstruction in whom prophylactic cannula cricothyroidotomy and oxygen insufflation were performed using equipment which we consider is safer, widely available and already familiar to most anaesthetists throughout Australia.
Keywords
Introduction
Awake tracheal intubation is the gold standard in the management of the anticipated difficult airway. 1 When less invasive techniques are expected to fail or have already failed, primary tracheostomy under local anaesthesia is indicated. As an alternative to primary tracheostomy in this setting, prophylactic cannula cricothyroidotomy (PCC) for the purpose of jet ventilation facilitates awake or asleep tracheal intubation of the difficult airway. 2 By ensuring oxygenation and relieving time pressure, relatively unhurried attempts can be made at establishing a patent airway. Despite its appeal, safe use of this technique requires specialised equipment and significant expertise, both of which are unavailable in most settings. The aim of our report is to reintroduce this valuable approach to difficult airway management using equipment with a superior safety profile that is already widely available and familiar to Australian anaesthetists. Consent was obtained from both patients for publication of this report and the associated images.
Case presentation 1
A 71-year-old male presented to a district hospital with a six-hour history of progressive odynophagia and muffled voice. His past medical history included hypertension and emphysema. An ear, nose and throat (ENT) surgeon was approximately one hour away. On presentation, the patient was afebrile, in no respiratory distress and with normal vital signs. Mild anterior neck tenderness and inability to tolerate secretions were noted. Bedside upper airway examination was normal. Computed tomography (CT) of the neck (Figure 1) obtained by emergency department staff (prior to obtaining anaesthesia consultation) demonstrated severe swelling of the epiglottis with an epiglottic abscess and severe swelling of the posterior pharynx, arytenoids and aryepiglottic folds. Infraglottic structures were normal.
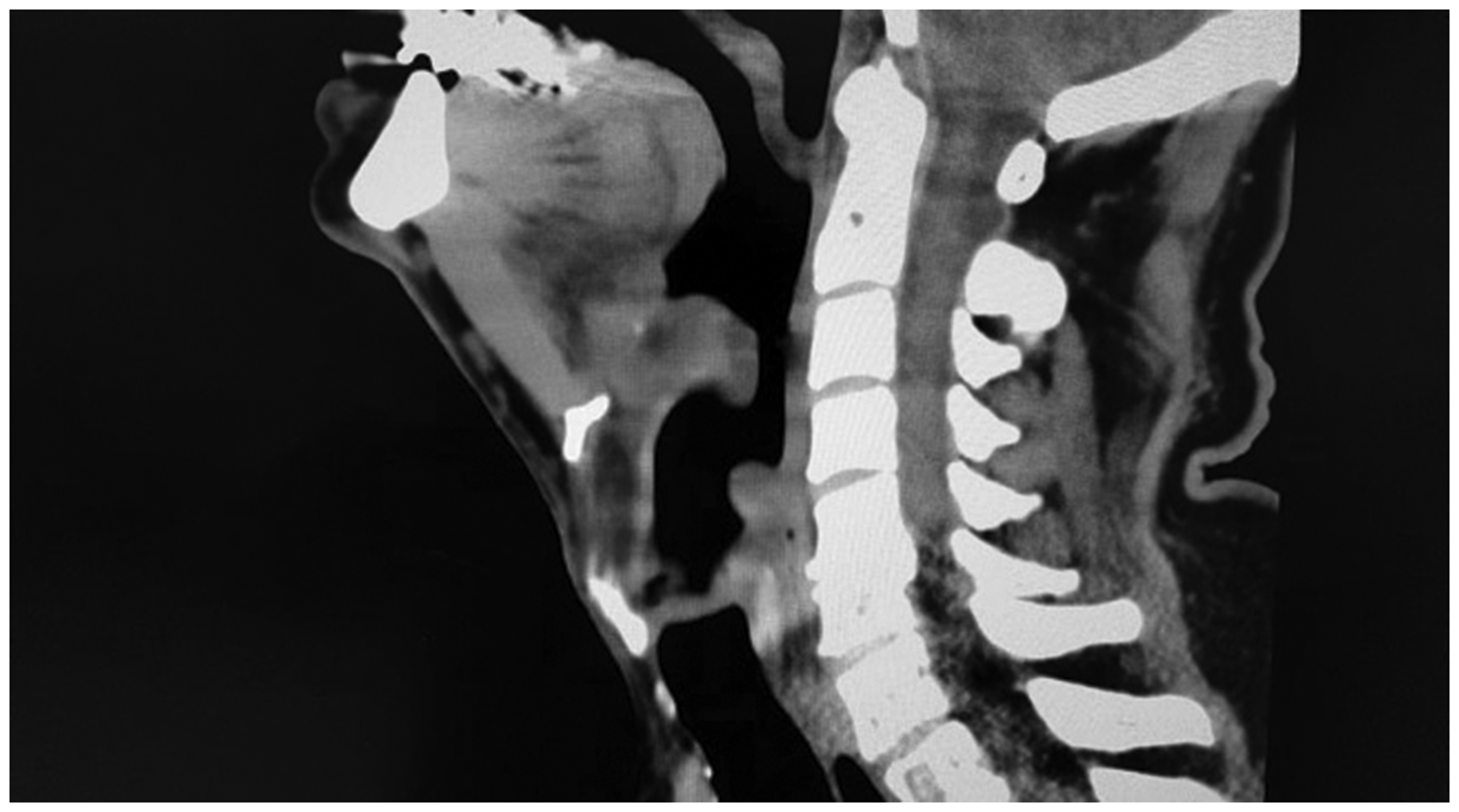
Computed tomography scan demonstrating supraglottic swelling and epiglottic abscess.
A provisional diagnosis of adult supraglottitis was made, and antibiotics and corticosteroids were commenced. Due to the lack of an intensive care unit and 24-hour ENT surgical support, the decision was made to transfer the patient to a tertiary referral centre (45 minutes away), and anaesthetic support was requested.
Nasendoscopy performed by the anaesthetist (S.W.) revealed severe swelling of the epiglottis and other supraglottic structures, with difficult and limited views of the glottic inlet (Figure 2 (a) and (b)).
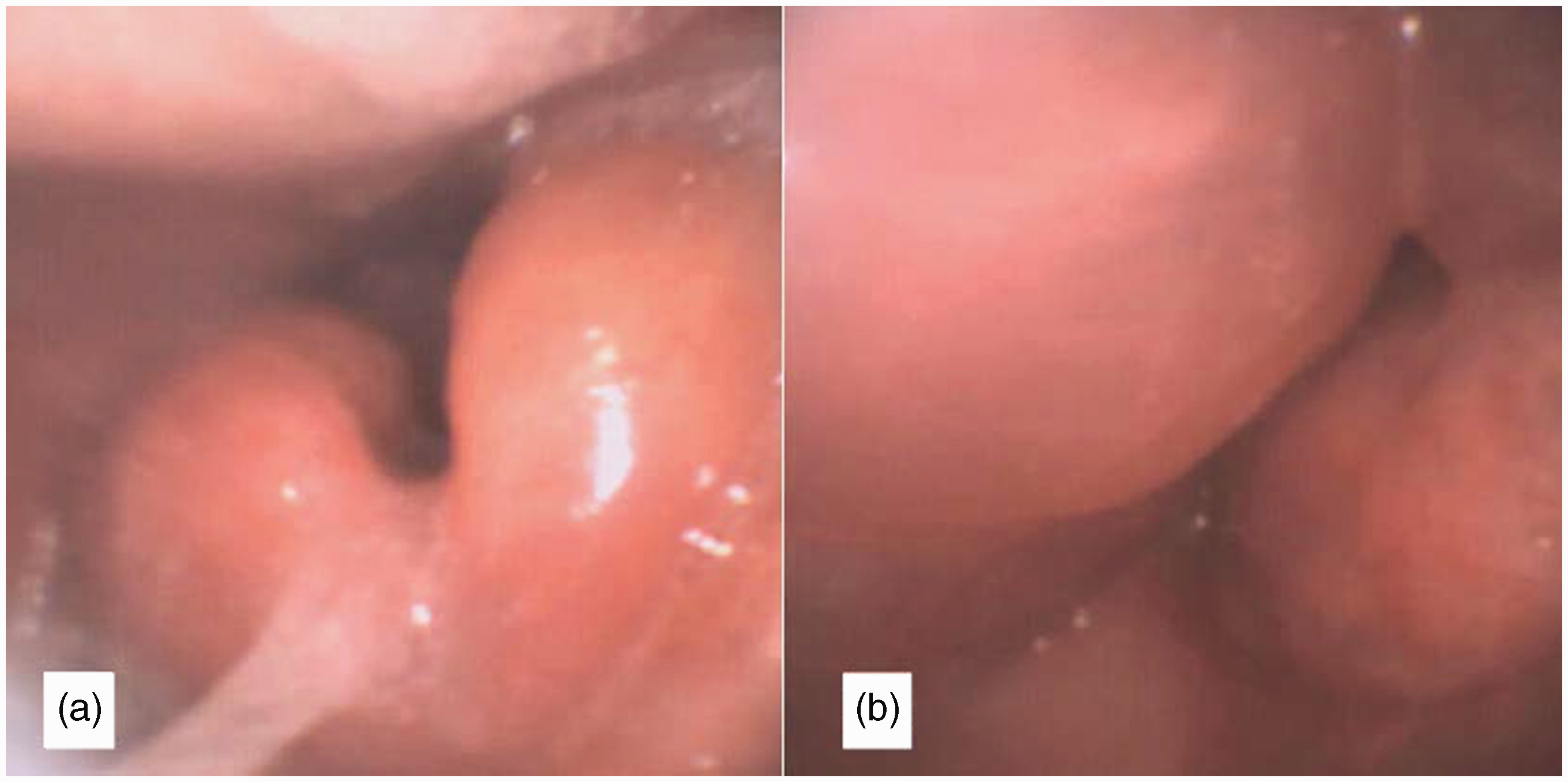
(a) Nasendoscopy findings demonstrating swollen epiglottis and (b) view of glottic inlet with markedly swollen arytenoids and aryepiglottic folds.
Given the nasendoscopy findings and clinical presentation, the senior anaesthetist decided to proceed immediately with endotracheal intubation. Despite the patient’s apparent stability, waiting for the ENT consultant—considered to be the only available surgeon proficient in tracheostomy formation—was deemed inappropriate, given the significant risk of disease progression and diminishing window of opportunity for successful intubation.
Nebulised epinephrine (adrenaline) was administered, and the patient was transferred to the operating room for awake nasal flexible bronchoscopic intubation (AFBI). Despite its intrinsic safety, however, the risk of AFBI failure was considered high due to grossly abnormal anatomy and poor glottic views on nasendoscopy. Additional risks included instrumentation-related trauma leading to a ‘can’t intubate/can’t oxygenate’ (CICO) scenario and failure to advance the endotracheal tube into the trachea due to tube hold-up on the swollen glottic structures. Therefore, to optimise alveolar oxygen delivery, a precautionary cannula cricothyroidotomy using a 14-gauge BD Insyte cannula (Becton Dickinson, Franklin Lakes, NJ, USA) was performed prior to attempting AFBI (using a technique previously described by Heard 3 ), its position confirmed by aspiration of air into a saline-filled syringe and positive end-tidal CO2. In the event of upper airway obstruction and oxygen desaturation, percutaneous oxygen insufflation (POI) would be delivered via the cannula using a Rapid-02® (Meditech Systems Ltd, Dorset, UK), which is a flow-regulated insufflation device that connects at one end to a standard oxygen flowmeter and at the other end to a Luer Lock cannula. Thumb occlusion of the T-piece allows for oxygen to flow from the flowmeter to the cannula (and delivery of a known volume of oxygen under low flow), whilst releasing the thumb allows for flowmeter gas to vent to the atmosphere, and passive expiration (Figure 3).
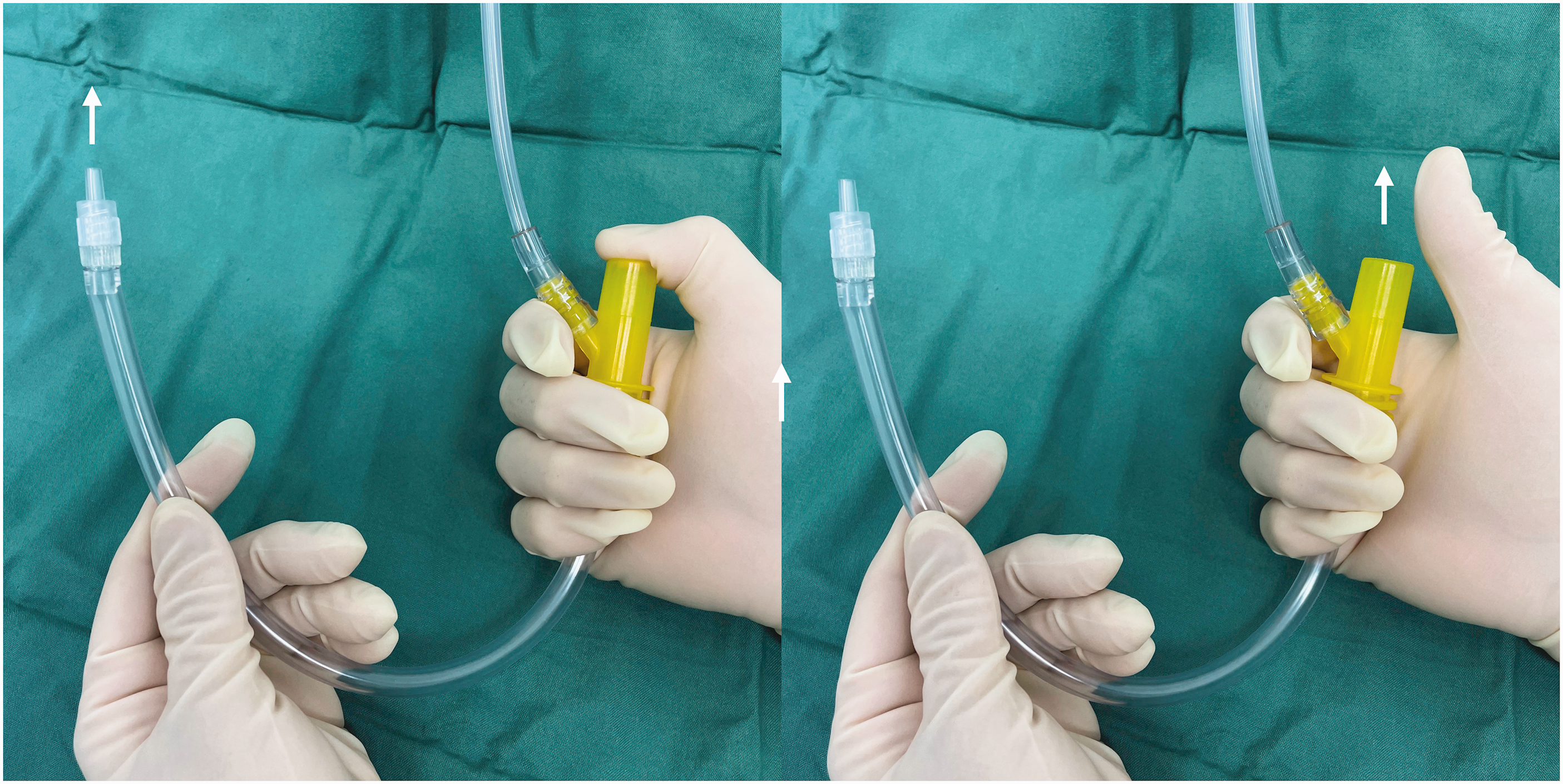
Rapid-O2® (Meditech Systems Ltd, Dorset, UK) oxygen insufflation device.
A Vortex approach was used to guide decision-making. 4 In this strategy, descent into the Vortex (no evidence of alveolar oxygen delivery) would trigger POI via the Rapid-O2. In the Green Zone, where more time would be available for decision-making, suitable courses of action would include further attempts at intubation, wire-guided conversion to a large bore cuffed airway using the Melker Cricothyroidotomy kit (Cook Medical, Bloomington, IN, USA) or awaiting the ENT surgeon. In the event of failure to re-enter the Green Zone using POI (e.g. displaced or kinked cannula), videolaryngoscopy would be attempted once, with immediate progression to scalpel-bougie cricothyroidotomy if immediate videolaryngoscopy proved unsuccessful.
Airway topicalisation was achieved using nasal lidocaine with phenylephrine, atomised lidocaine 2%, as well as transtracheal lidocaine 2% instilled via the cricothyroid cannula. Supplemental oxygen was provided via a modified Hudson mask. Throughout the encounter, correct cannula position was reconfirmed approximately every four to five minutes by oxygen insufflation (with lack of resistance on the occluding thumb for two seconds at 15 l/min).
Once the cricothyroid cannula was secure, AFBI without sedation was attempted. This proved both challenging and time-consuming (around 15 minutes) but was well tolerated and ultimately successful (standard endotracheal tube with an internal diameter of 7.0 mm), whereupon anaesthesia was induced uneventfully. The patient was transferred to a tertiary centre for microlaryngoscopy and drainage of an epiglottic abscess. He was successfully extubated on day 4 postoperatively and made a full recovery.
Case presentation 2
A 71-year-old male presented to a metropolitan cancer hospital with a three-month history of progressive symptoms of dysphagia and shortness of breath in the recumbent position. Eight years prior, he had undergone a partial glossectomy and temporary tracheostomy for oral squamous cell carcinoma. On examination, his breathing was unlaboured, and vital signs, including oxygen saturation, were normal. Nasendoscopy revealed a large obstructing mass at the base of tongue with no view of the glottic inlet. A CT scan demonstrated a large lobulated mass filling the vallecula and involving the epiglottis, with marked narrowing of the inferior oropharynx (Figure 4).
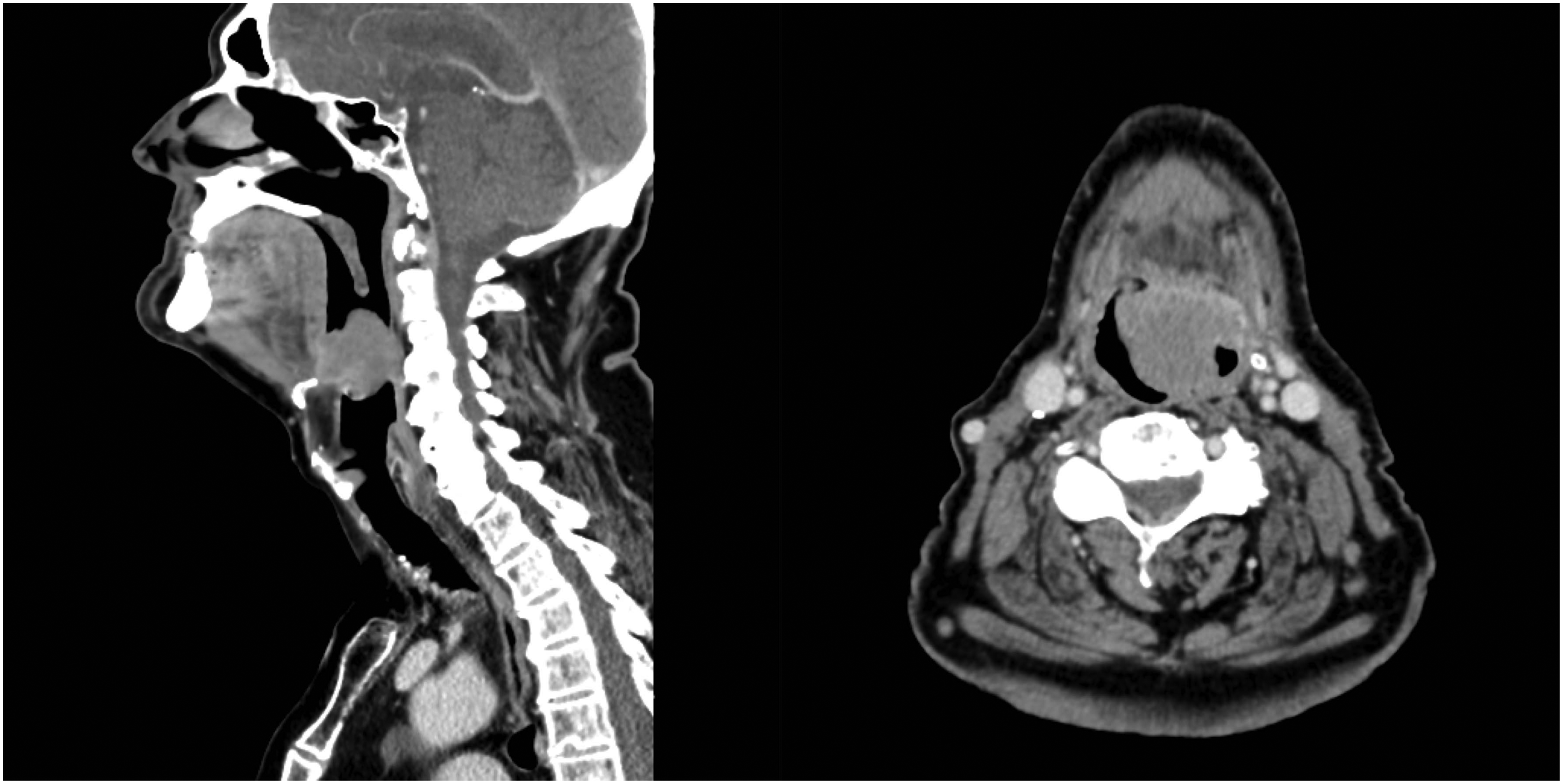
Computed tomography scan demonstrating obstructing vallecular mass with epiglottic involvement.
Given his progressive symptomatology and nasendoscopy findings, microlaryngoscopy and examination under anaesthesia was planned. Due to traumatic memories of the prior tracheostomy formation, the patient expressed significant reservations about having another tracheostomy. A shared decision between the patient, surgeon and anaesthetist was made to avoid tracheostomy, unless or until other alternatives to safe airway management were exhausted or deemed inappropriate.
Prior to airway instrumentation, equipment for surgical front-of-neck access was laid out. The patient was placed in the semi-recumbent position, and oxygen via high flow nasal cannula was supplied at 30 l/min. Using remifentanil sedation (effect site concentration 3.0 ng/l), the patient was maintained in a relaxed, awake and spontaneously breathing state. Airway topicalisation was achieved with a combination of nasal lidocaine with phenylephrine, lidocaine 10% spray to oropharynx and 2% lidocaine via an atomiser (MADgic laryngo-tracheal mucosal atomisation device; Teleflex Medical, Plymouth, MN, USA) to the hypopharynx. Awake videolaryngoscopy using a C-MAC® D-blade (Karl Storz Endoscopy, Slough, UK) was chosen for its potential to allow for visualisation of the introducer and endotracheal tube in relation to the tumour (thereby limiting trauma to the friable mass), as well as the increased upper airway space, potentially improving the glottic view. Upon advancing the videolaryngoscopy, a large, fixed mass was noted to obscure the glottic opening (Figure 5). Further attempts were made with a flexible bronchoscope nasally, then with a combined videolaryngoscopy/fibreoptic bronchoscope approach. Whilst successive attempts were well tolerated by the patient (who remained awake and cooperative), they were unsuccessful due to marked anatomical distortion and progressive airway bleeding and swelling.
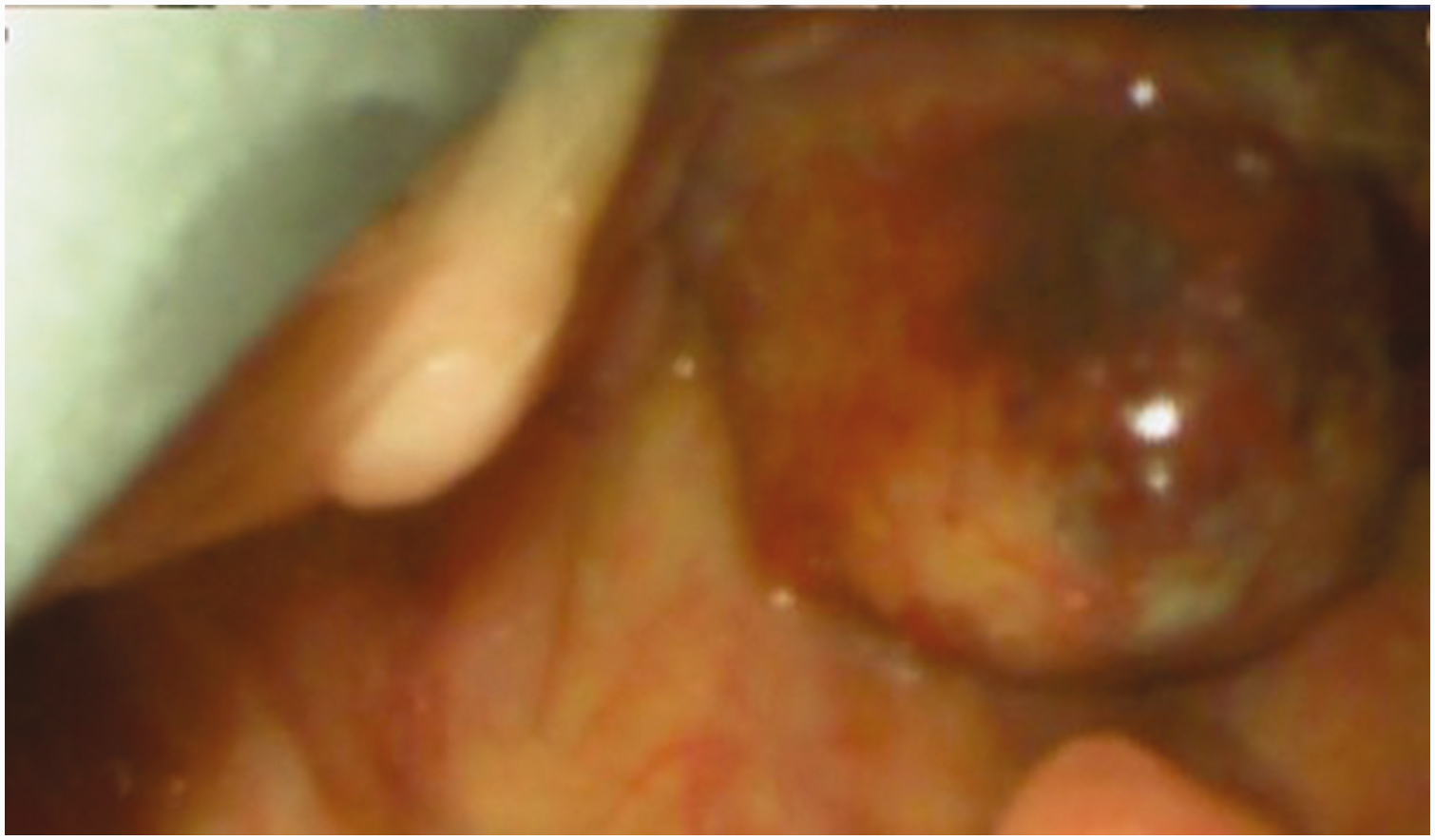
Optimal view on videolaryngoscopy.
After approximately 25 minutes, despite oxygen saturation maintained at 100% and no signs of psychological distress, the patient was noted to be slightly stridulous. This prompted the anaesthetist to shift team focus away from securing a definitive airway and towards ensuring oxygenation. Cannula cricothyroidotomy using the technique described in Case 1 was therefore performed. With establishment of a reliable conduit for oxygenation, we reviewed our available resources and our strategy for securing a definitive airway. Further attempts at intubation were made by the surgeon using an operative laryngoscope as well as a McCoy blade (Penlon Ltd, Abingdon, UK). As part of the strategy, introducer-guided videolaryngoscopy attempts were also undertaken, but these also proved unsuccessful. Throughout the encounter, oxygen was intermittently insufflated via the cannula using the Rapid-O2 (two seconds at 15 l/min every four to five minutes), and oxygen saturation was maintained above 98%.
At 45 minutes after commencement of instrumentation, the team elected to proceed to an awake tracheostomy. This was performed below the level of the cannula cricothyroidotomy, thus permitting use of the Rapid-O2 and the provision of oxygen at an FiO2 of 100% throughout the procedure. Anaesthesia was subsequently induced for microlaryngoscopy, during which the mass was debulked. Tracheostomy was removed on day 5, and the patient made an uneventful recovery with resolution of preoperative symptoms. He was referred for radiotherapy treatment.
Discussion
The role of prophylactic cannula cricothyroidotomy in difficult airway management is well described, where it has been used with pressure-limited, high flow jet ventilation.2,5 Safe use of jet ventilation, however, requires specialised equipment and significant expertise, 6 both of which are unavailable in many settings. In non-expert hands, the absence of tactile feedback, lack of an assured expiratory path and the risk of excessive intratracheal flows and pressures (resulting in impaired cardiac output, volume trauma and barotrauma 7 ) reduce the margin of safety for these devices. The Rapid-O2 offers several technical and non-technical benefits that could make its use in difficult airway management safer and more widely applicable (Table 1).
Potential technical and non-technical benefits of percutaneous oxygen insufflation using the Rapid-O2.
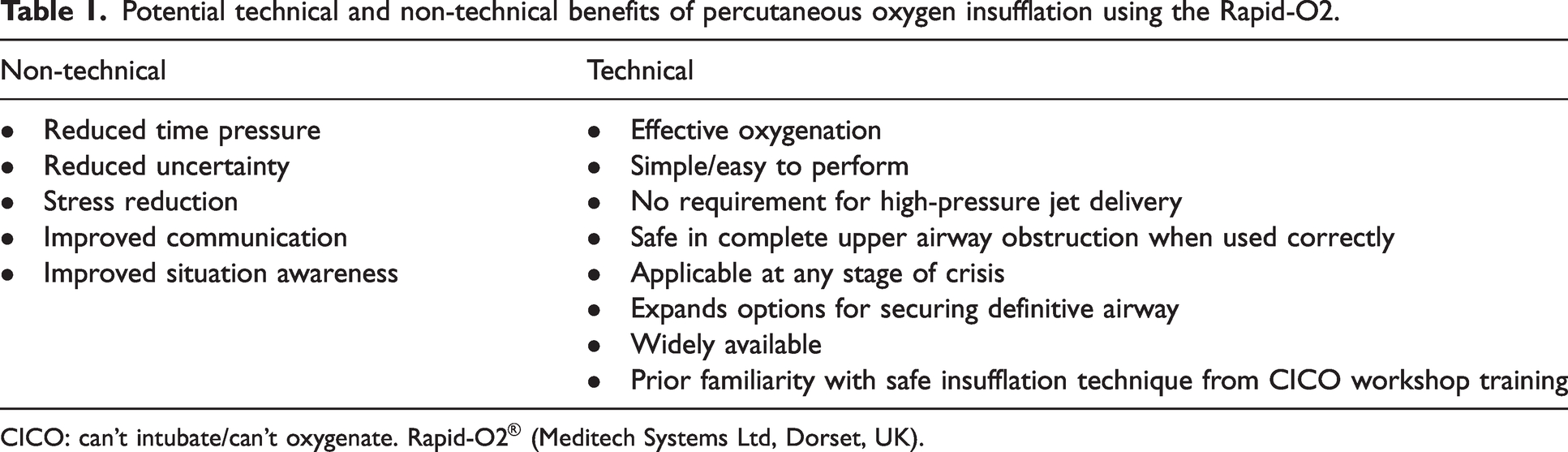
CICO: can’t intubate/can’t oxygenate. Rapid-O2® (Meditech Systems Ltd, Dorset, UK).
Pursuing an awake tracheal intubation in our patients was deemed appropriate and consistent with current guidelines.8,9 Considering their advanced airway pathology, however, they were also at risk of complications of instrumentation 10 (e.g. airway trauma, bleeding) and excessive sedation, and therefore at greater risk of failure to oxygenate. With each re-attempt at intubation, one would anticipate among the airway team an incremental increase in stress and fear, potentially degrading cognitive and technical performance further. We submit that establishing a prophylactic conduit for POI allowed us effectively to uncouple oxygenation from upper airway obstructive processes, permitting a shift from a maladaptive to an adaptive stress response. This in turn improved both technical and non-technical performance and created more cognitive space for creative and lateral thinking, which are essential skills for problem solving but which are often impaired under time pressure. 11 It allowed the team to be more methodical, mobilise resources, avoid ‘forced’ errors and better manage barriers to effective crisis management.
In the second case, despite the favourable outcome, the team did become fixated on making repeated awake intubation attempts despite evidence of increasing upper airway obstruction; this constituted a deviation from the usual standard of care, where failed awake tracheal intubation should be declared after a maximum of four attempts. 1 In complex, dynamic and tightly coupled settings characterised by novelty, time pressure and stress, several cognitive processes have been identified. 12 Expert decision-making deviates from prescriptive practice into contextually based patterns that are less well supported by checklists, algorithms and other procedural rules. Simultaneously, task and sensory overload predispose to cognitive errors. Our procedural violation serves as a reminder that, while acknowledging the evidence supporting guidelines and standardisation of practice, even highly motivated anaesthetic teams supported by the best guidelines may still struggle to perform optimally rule-related behaviour in a complex tightly coupled work environment. 13
PCC and POI were instrumental in mitigating the impact of fixation error in both cases. In the time-pressured setting of progressive airway obstruction and diminishing prospects of successful intubation, adhering to the traditional approach, 14 whose primary focus is on intubation and ventilation, can lead to fixation error as illustrated by our Case 2 and by the Elaine Bromiley case. 15 Incorporating POI into a traditional algorithm (prior to instrumentation in Case 1 and during instrumentation in Case 2) however, allowed us to shift focus from the process (intubation) to the goal (oxygenation). Nevertheless, it should be noted that PCC adds what should be regarded as a relative and not an absolute margin of safety; it should not be regarded with any confidence as a definitive airway. It is the duty of the airway team to remain mindful of the primary goal—oxygenation—and of the progressive risks of repeated attempts at intubation.
The ability to deliver intratracheal oxygen at an FiO2 of 1.0 is a distinct advantage over supraglottic methods of oxygen delivery (e.g. high flow nasal cannula), which carry a risk of fire given the proximity to the surgical site. Use of POI at an FiO2 of 1.0 with concurrent use of electrocautery is safe so long as the trachea is not entered surgically. Following tracheotomy, however, POI should be avoided if electrocautery is used. Close communication with the surgeon is therefore essential.
In Australia, 85% of teaching hospitals have visible point-of-care CICO rescue packs that include equipment for cannula-based techniques, and most (87%) include a flow-regulated device such as the Rapid-O2. 16 This visibility, coupled with the widespread teaching of POI in CICO workshops, encouraged our use of the rescue equipment in the non-CICO setting, and highlights how standardisation of equipment can facilitate good performance in difficult airway situations. 17 Additionally, the minimally destructive nature of cannula cricothyroidotomy18,19 and safety profile of the Rapid-O2 20 facilitated a lower threshold for considering PCC and POI early in the crises, despite the acknowledgment that, in hindsight, POI may not be needed. In our patients, the cannula was removed with minimal risk of morbidity but still provided the performance-enhancing non-technical benefits listed earlier.
Despite the benefits of PCC and the Rapid-O2, a number of safety and efficacy concerns exist (Table 2). Whilst pressures in an unobstructed 14G cannula are low (24–34 kPa) when using a wall-mounted flowmeter at 15 l/min, 21 pressures as high as 282 kPa are recorded when flows are increased beyond this limit. Furthermore, if resistance is increased (as would occur with cannula misplacement), the pressure at the tip of the cannula is limited only by pressure applied by the occluding thumb. Failure to detect this (in the case of an inexperienced operator or stress-related inattention) may result in delivery of dangerously high pressures (approaching pipeline pressures) into neck tissue with potentially catastrophic outcomes.
General risks of percutaneous oxygen insufflation.
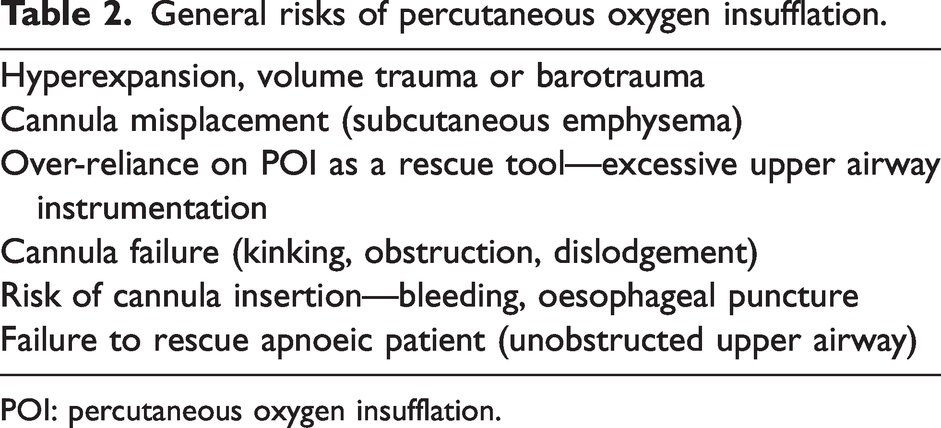
POI: percutaneous oxygen insufflation.
Reduced efficacy of the Rapid-O2 in lesser degrees of airway obstruction may constitute an additional limitation. In animal models with total or near-total airway obstruction, insufflation of 1 l oxygen followed by an additional 500 ml when oxygen saturation drops by 5% is effective and safe at achieving normoxia.18,19,22,23 Using a similar oxygenation regimen in the elective setting, the Rapid-O2 achieved normoxia in an obese adult with complete airway obstruction for up to an hour. 24 Only two other reports describe its successful use as a CICO rescue device in humans.25,26 When CICO is associated with lesser degrees of obstruction, however, POI may be less effective, as gas preferentially escapes out of the upper airway as opposed to expanding the lungs. 27
Compared with CICO rescue, prophylactic POI is not a widely recognised technique, but nevertheless served to increase the margin of safety in our patients in several ways. First, given that successful emergency rescue cannot be guaranteed, especially when attempted under stress, confirming the ability to rescue in advance is useful. Lack of resistance on the occluding thumb indicates lack of resistance to forward flow and, by extrapolation, a patent cannula with a tip that is positioned inside the lumen of the airway. Second, given that a patient may be in the Vortex (no evidence of alveolar oxygen delivery) despite normal oxygen saturation, 4 prophylactic POI minimises periods of hypoxia should alveolar oxygen delivery by supraglottic measures fail.
As POI is not without risk, it is reasonable to consider POI only when other measures (e.g. high flow nasal cannula) have failed or would otherwise be unsuitable. As in other areas of difficult airway management, the decision should be context dependent, with due consideration of other performance-shaping factors, such as operator experience with the Rapid-O2, risks of hypoxia, apnoeic reserve, and so on. Insufflation with Rapid-O2 can effectively be monitored with sidestream capnography, 24 thereby limiting the risk of breath stacking. Finally, given that continuous POI of 0.5 l/min is safe and effective in an apnoeic patient with total or near total obstruction, 28 our practice of prophylactically insufflating 500 ml every four to five minutes would therefore appear to be safe.
In summary, our report revisits the well-described technique of PCC in the awake patient prior to attempts at securing the airway either awake or asleep and the human factor benefits it confers on teams managing a difficult airway. In contrast to other reports, where oxygenation was achieved by means of jet ventilation, our proposed technique utilises the Rapid-O2, a device already familiar to anaesthetists and widely available in standardised, highly visible packs at sites of airway management across Australia. With the added safety profile and the minimal expertise needed for safe use, these features may lower the threshold for PCC, thereby potentially increasing the margin of safety in difficult airway management. As with any airway intervention, operators should be aware of the limitations and current knowledge gaps pertaining to the safety and efficacy of POI using the Rapid-O2.
Footnotes
Author Contributions
Declaration of conflicting interests
The authors declare no conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.