
Abstract
Regional anaesthetic techniques for patients undergoing laparotomy have been shown to provide optimal postoperative analgesia and allow early mobilisation, and thus, enhance recovery. The serratus anterior plane block, first documented in 2013, has been suggested as a potential alternative to thoracic paravertebral and central neuraxial blockade for chest wall and upper abdominal incisions as it can provide analgesia from T2 to T9. Although there are published cases of this block being used for chest wall analgesia, there are currently no published cases of this block being used for abdominal incisions. We report our experience with two patients, using ultrasound-guided serratus anterior plane blockade with catheter insertion following laparotomy.
Introduction
Bowel resection is a commonly performed surgical procedure. Despite advances in surgical and anaesthetic techniques, morbidity after abdominal surgery is still high. 1 Enhanced recovery after surgery pathways recommend that pain management should be multimodal, evidence-based, and procedure-specific. The aim is to produce optimal analgesia with minimal side-effects and to facilitate early mobilisation and oral feeding. 2 For patients undergoing open abdominal surgery, thoracic epidural analgesia is the gold standard for postoperative pain control. 3 Other regional anaesthetic techniques include abdominal trunk blocks such as transversus abdominis plane (TAP) block and rectus sheath block.
The serratus anterior plane (SAP) block, was first documented by Blanco et al. in 2013. 4 Paraesthesiae from T2 to T9 were demonstrated, and it was proposed that this technique could be a viable alternative to thoracic paravertebral and central neuraxial blockade for chest wall and upper abdominal incisions. SAP blocks have been documented in the literature only a handful of times since and mostly for chest wall analgesia.
We report two cases of ultrasound-guided SAP block with catheter insertion providing effective analgesia following upper abdominal laparotomy. Both patients gave verbal consent for publication of their case histories. Consent for non-specified regional analgesia was elicited preoperatively from both patients.
Case report 1
A 48-year-old male patient weighing 130 kg (body mass index, BMI, 41.3 kg/m2) was admitted to hospital with a one-day history of fever and right upper quadrant abdominal pain. He was diagnosed with acute calculous cholecystitis. After initial resuscitation he proceeded to laparoscopic cholecystectomy. There was difficulty obtaining adequate visibility of the surgical field via the laparoscope, so the procedure was converted to an open cholecystectomy. As this was not the original plan an epidural had not been placed preoperatively. The decision was made to perform an ultrasound-guided SAP block with catheter insertion prior to extubating the patient. Using a sterile technique, the block was performed in the mid-axillary line at approximately T6–7 level (Figure 1). A 100 mm 18G Tuohy (SonoLong Echo NanoLine, Pajunk®, GmBH, Geisingen, Germany) needle was placed with ultrasound guidance into the plane deep to serratus anterior (Figure 2 (a), (b)). A bolus dose of 0.75% ropivacaine 20 mL with dexamethasone 4 mg was injected and a catheter was inserted. An intermittent bolus of 0.2% ropivacaine 30 mL was delivered every 3 h through the catheter.
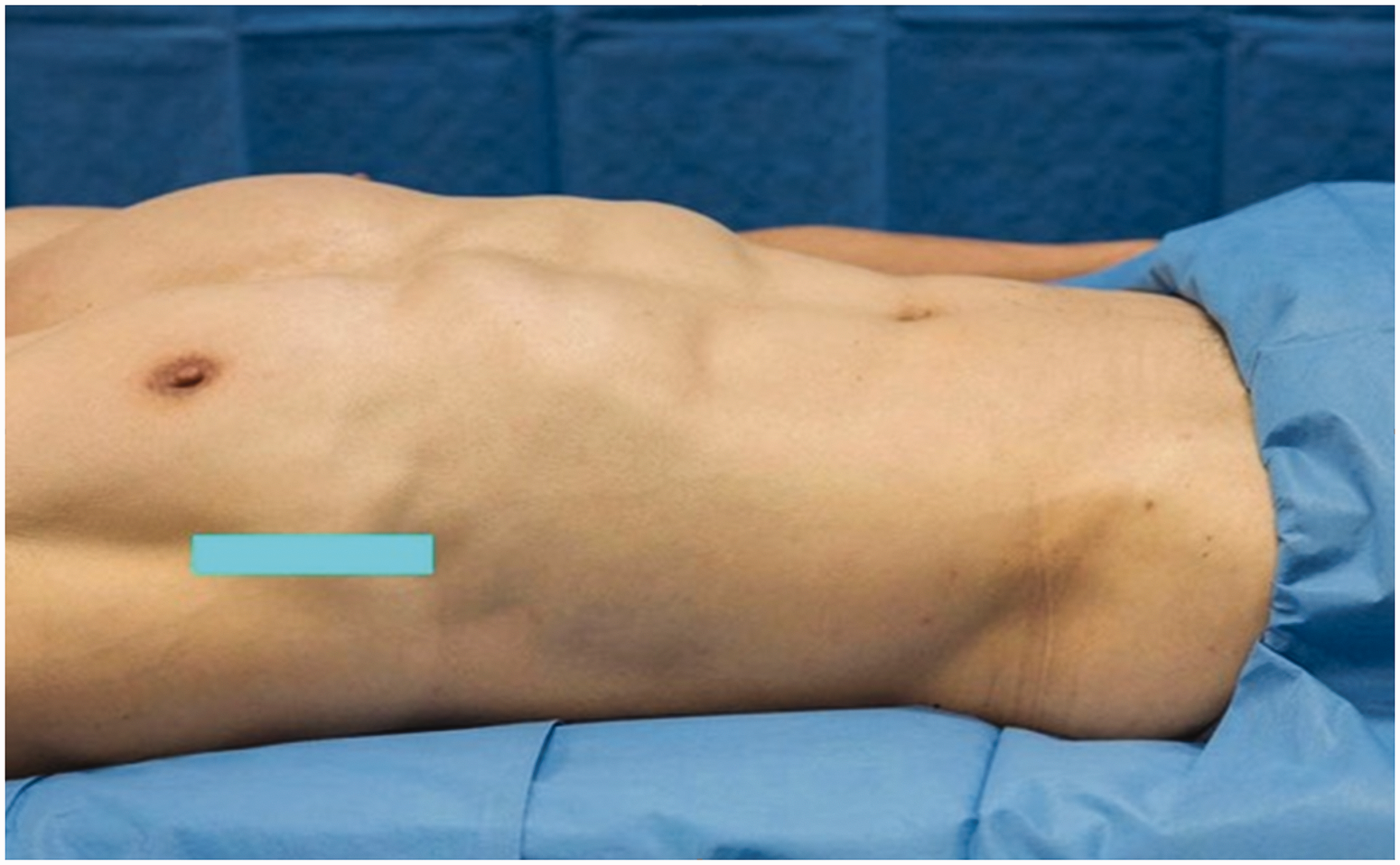
Graphic representing probe position (model used for demonstration purposes and not the actual patient).
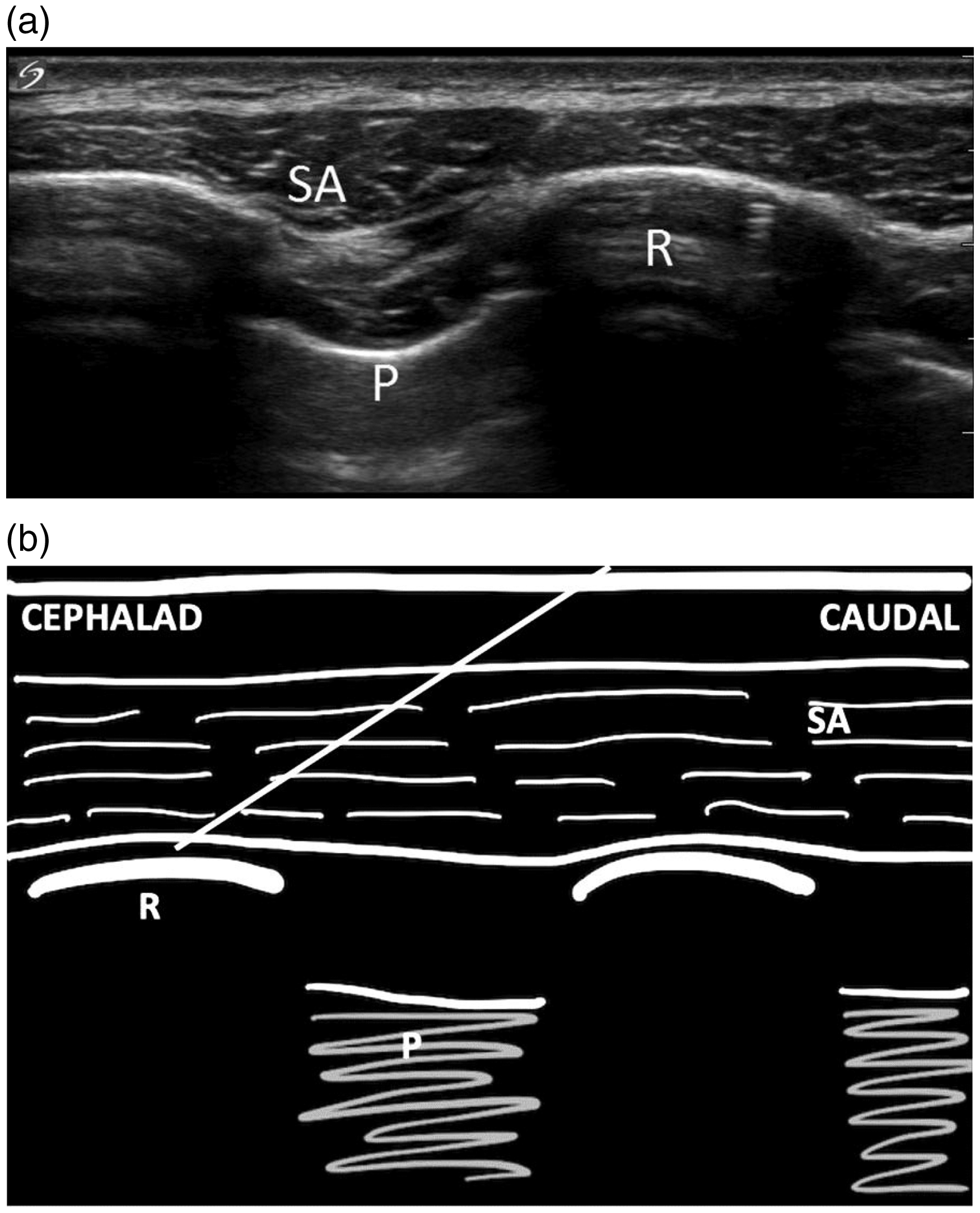
(a) Ultrasound image of serratus anterior and surrounding structures. (b) Graphic representing needle position for the serratus anterior plane block. SA: serratus anterior; R: rib; P: pleura and lung.
The patient was reviewed daily by the Acute Pain Service (APS) team. On day 1 postoperatively, the SAP catheter infusion was working well with the patient reporting a static pain score of 4 out of 10 (using the Numerical Pain Rating Scale). In addition, the patient could mobilise and participate in physiotherapy with adequate pain control. In the 48-h period following surgery, the patient received only 50 mg of oral oxycodone for breakthrough analgesia. The SAP catheter infusion was continued for three days after initial insertion and was removed on the morning of the patient’s discharge from hospital. Subsequent follow-up was performed five weeks postoperatively with the patient reporting no pain and that the wound had healed well.
Case report 2
A 65-year-old female weighing 100 kg (BMI 38 kg/m2) presented to hospital with acute onset right-sided abdominal pain. This was on a background of recently diagnosed malignant caecal adenocarcinoma (T4aN2b), with the patient awaiting a right hemicolectomy. Her medical history also included Barrett’s oesophagus. A computed tomography scan of the abdomen was performed which showed free fluid in the pelvis and a small caecal perforation. The patient was taken to theatre for an emergency right hemicolectomy through a right-sided transverse incision.
A preoperative epidural catheter was avoided because of suspected underlying sepsis and raised white cell count. Prior to extubating the patient, an ultrasound-guided SAP block with catheter insertion was performed. The block was performed in the mid-axillary line at approximately T6–7 level in the plane deep to serratus anterior using a 100 mm 18G Tuohy needle. An initial bolus of 0.75% ropivacaine 20 mL and dexamethasone 4 mg was used. The patient subsequently received an intermittent bolus of 0.2% ropivacaine 20 mL every 3 h. The patient also received intravenous morphine via patient-controlled analgesia (PCA). Only 4 mg of morphine was used within the first 24-h period and, hence, the PCA was ceased on day one postoperatively after review by the APS team. The patient reported static and dynamic pain scores of 4 out of 10 (using the Numerical Pain Rating Scale). Loss of cutaneous sensation to cold was demonstrated near the wound. However, mapping specific dermatomes was not possible due to dressings. The SAP catheter remained in situ for a total of 34.5 h. On further follow-up there were no noted complications.
Discussion
Ultrasound-guided SAP blocks have been reported in the literature as an effective regional anaesthetic technique for breast and thoracic wall surgeries and to provide analgesia for rib fractures.4,5 Given that innervation of the upper abdominal wall is derived from T6 to T10, blockade of these sensory nerves in the thoracic region should offer some degree of analgesia for upper abdominal incisions. 4
Mayes et al. investigated the anatomical basis of the analgesic effect of ultrasound-guided SAP blocks on six soft-fix embalmed cadavers. 6 On one side, methylene blue was injected, to assess the upper limit of spread. On the contralateral side, liquid latex, which had been coloured black to aid identification, was used to assess the lower limit of spread. Subsequent dissection was performed and showed that the lateral cutaneous branches of the intercostal nerves contained methylene blue and latex on all occasions. This suggests that SAP blocks are mediated through blockade of the lateral cutaneous branches of the intercostal nerves.
Strengths of the ultrasound-guided SAP block include the ability to perform the block with the patient in the supine position, and lack of the sympathetic nervous system blockade and associated hypotension common with neuraxial techniques. Limitations include a lack of familiarity with the technique, the possibility of causing a pneumothorax with incorrect needle positioning, and the unilateral effect of the block.
We report on two cases where SAP blocks were used for upper abdominal analgesia following laparotomy with good effect. In both cases, no adverse outcomes were encountered. The SAP block technique has fewer side-effects and fewer potential risks than thoracic epidural and paravertebral block techniques. 4 The ultrasound-guided SAP block with catheter can be easily and safely inserted with the patient in the supine position at the end of surgery. We suggest this new technique could be a useful addition to multimodal analgesia following unilateral upper abdominal incisions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.