
Abstract
Ocular hypotony can occur from many causes, including eye trauma, ophthalmic surgery and ophthalmic regional anaesthesia–related complications. Some of these patients require surgical intervention(s) necessitating repeat anaesthesia. While surgical management of these patients is well described in the literature, the anaesthetic management is seldom discussed. The hypotonous eye may also have altered globe anatomy, meaning that the usual ocular proprioceptive feedbacks during regional ophthalmic block may be altered or lost, leading to higher risk of inadvertent globe injury. In an ‘open globe’ there is a risk of sight-threatening expulsive choroidal haemorrhage as a consequence of ophthalmic block or general anaesthesia. This narrative review describes the physiology of aqueous humour, the risk factors associated with ophthalmic regional anaesthesia–related ocular hypotony, the surgical management, and a special emphasis on anaesthetic management. Traumatic hypotony usually requires urgent surgical repair, whereas iatrogenic hypotony may be less urgent, with many cases scheduled as elective procedures. There is no universal best anaesthetic technique. Topical anaesthesia and regional ophthalmic block, with some technique modifications, are suitable in many mild-to-moderate cases, whilst general anaesthesia may be required for complex and longer procedures, and severely distorted globes.
Introduction
Normal intraocular pressure (IOP) range is 10–21 mmHg, with a mean (standard deviation) of about 14.7 (2.8) mmHg. 1 ‘Hypotony’ refers to an IOP below the normal range; however, it lacks strict definition. Statistically, it is defined as an IOP of <6.5 mmHg, which is greater than three standard deviations below the population mean IOP. Clinically, it is described as the critical IOP, below which pathologic functional and clinically apparent structural changes occur.2–5 Eyes with clinically apparent hypotony will typically have an IOP below 7 mmHg, though many eyes may tolerate an IOP of 2–6 mmHg without vision loss.2,6 If ocular hypotony is left untreated, it can lead to deleterious effects, such as shallow anterior chamber, corneal changes, accelerated cataract formation, oedema of optic disc and optic nerve, cystoid macular oedema, choroidal folds, and choroidal effusion and detachment, resulting in temporary or permanent visual loss.4,5,7 The duration of hypotony directly affects the visual recovery; therefore, it is paramount to recognise and manage each case as early as possible.3,5
Surgical management of ocular hypotony is well described.2,4–6 However, the anaesthetic technique is seldom discussed. Most ocular surgery is performed under regional anaesthesia. A normal globe with intact scleral wall integrity usually provides certain ballottement and proprioceptive feedback during an ophthalmic block; however, this feedback may be lost partially or even completely in a hypotonous globe. This narrative review describes the physiology of aqueous humour and IOP; the aetiology, diagnosis, and management of hypotony; the risk factors associated with inadvertent ophthalmic regional anaesthesia–related causes and management strategies. Our aim is to better inform the choices of anaesthetic modality for the required surgery and issues and technique modifications that may influence the conduct of regional anaesthesia during surgical treatment of ocular hypotony.
Methodology
We conducted a literature review using a combination of keywords: ‘hypotony’ and ‘anaesthesia’ on PubMed, Google Scholar, Medline and Scopus published between January 1980 and December 2021. Other related articles were retrieved from references of key articles and a total of 50 articles were included in this review.
Physiology of aqueous humour dynamics and the normal IOP
Aqueous humour, the transparent fluid filling the anterior and posterior chambers of the eye, delivers oxygen and nutrients to the (avascular) cornea and lens, as well as maintaining the IOP and thence the shape of anterior and posterior chambers and the globe. It is produced by the ciliary processes at the rate of approximately 2.4 μl/min. 4 Most of it exits the eye through the trabecular meshwork and Schlemm’s canal (conventional route), with the flow driven by the hydrostatic pressure differential between the anterior chamber and episcleral veins. If the IOP falls below the episcleral venous pressure, conventional outflow ceases.4,8 About 10% of the aqueous humour leaves the anterior chamber by uveoscleral drainage (unconventional route) that is largely independent of IOP. An equilibrium exists normally between the rate of production and the rate of outflow of aqueous humour.4,8 This balance is represented by IOP.
Aetiology of ocular hypotony
Ocular hypotony can result from reduced aqueous humour formation, increased outflow, reduced episcleral venous pressure and aqueous humour loss from internal or external factors. It can be associated with an ‘open globe’ (resulting in complete breach of ocular wall integrity) from ocular trauma, penetrating injury, laceration or rupture, or after intraocular surgery. The list of rarer causes of ocular hypotony is extensive and beyond the scope of this review. 4
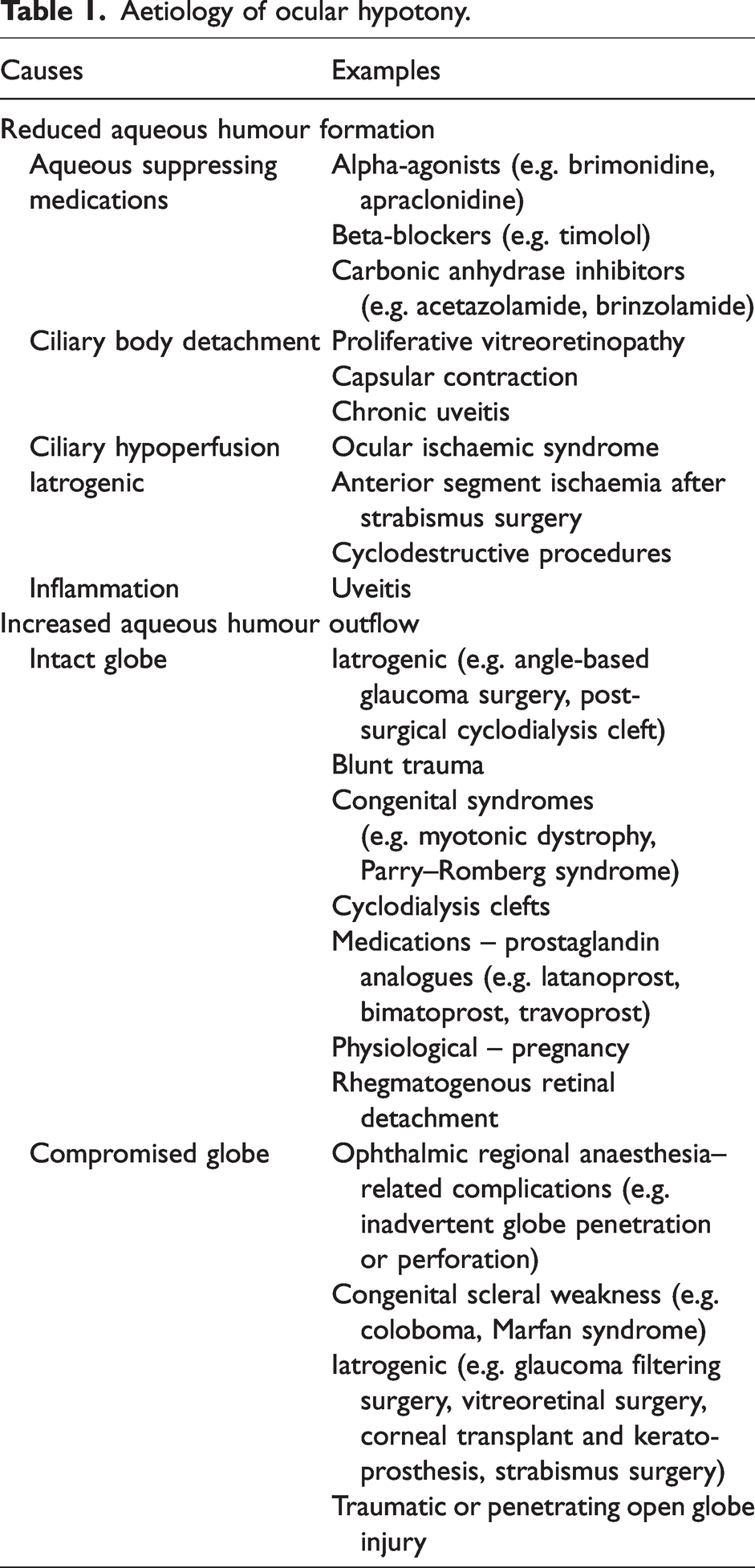
Table 1 contains causes of ocular hypotony which may be encountered in routine clinical practice. In most healthcare settings, the most common cause of hypotony is ocular trauma, which may be blunt or penetrating trauma. Different geographical areas may have differing frequencies and types of ocular trauma, depending in part on local customs and industries, usage of eye protection and personal safety measures employed, and road safety. Clinicians should look for associated additional trauma (e.g. brain, orbit) in cases of traumatic hypotony. The main cause of non-traumatic ocular hypotony in adults is iatrogenic related to intraocular surgery (where there is leakage from the intraocular wounds, excessive drainage following glaucoma filtering surgery or over-exuberant cyclodestructive procedures) and ophthalmic regional anaesthesia–related inadvertent complications. The incidence of iatrogenic hypotony is relatively uncommon and differs among institutions, depending on the types of surgery, regional anaesthesia routinely used and the skill of the clinicians involved.
Aetiology of ocular hypotony.
Ocular hypotony after ophthalmic surgery
Cataract surgery is the most common eye surgery worldwide. In small-incision phacoemulsification, the corneal incisions are usually sealed with stromal hydration, to give a watertight incision to maintain IOP and globe integrity and to minimise risk of infection. While this technique works in most cases, wound leakage may occur.9,10 This leakage usually resolves spontaneously within a few days but wound re-suturing may be required in some cases. 11 Extensive leak was also found in all the clear corneal wounds during vitrectomy in patients who have undergone recent cataract surgery. 12 Factors that potentially increase the risk of wound leakage include wound burn, prolonged surgical duration (e.g. complex surgery, mature cataract) and inadvertent eye rubbing/lid squeezing by the patients.
Glaucoma filtering surgery (e.g. trabeculectomy, implantation of aqueous shunt) often results in inadvertent over-filtering and may lead to hypotony. 13 The incidence of hypotony maculopathy is reported up to 20% when mitomycin C is used during filtration surgery. 7 Newer techniques of minimally invasive glaucoma surgery (MIGS) devices appear to have a lower risk of post-operative hypotony but suprachoroidal and subconjunctival MIGS devices have been associated with higher risk of early postoperative hypotony than Schlemm’s canal MIGS devices. 13
Cyclodialysis cleft results from a separation of ciliary muscle from the scleral spur forming a direct connection between the anterior chamber and suprachoroidal space. This accelerates the uveoscleral drainage pathway and reduces IOP; however, it may result in severe hypotony. 4
Iatrogenic scleral perforation has been reported with strabismus surgery, 14 buckle surgery for retinal detachment 15 and other periocular procedures (e.g. medial canthopexy 16 and endoscopic sinus surgery 17 ). In addition, anterior chamber ischaemia resulting from under-production of aqueous humour can occur after strabismus surgery. 4 Rare cases of spontaneous hypotony have been described, for example in Marfan syndrome 18 and congenital coloboma, 19 and as a consequence of uveitis. 15
Ocular hypotony resulting from ophthalmic regional anaesthesia
Inadvertent anaesthesia-related ocular complications, such as scleral penetration (entry wound only) and perforation (entry and exit wounds), are known to occur during needle-based regional block, leading to ocular hypotony. The reported incidence ranged from 0% to 0.75% in various studies. 20 Scleral lacerations, thence hypotony, can also result from glancing needle injuries (the needle is tangential to the globe).
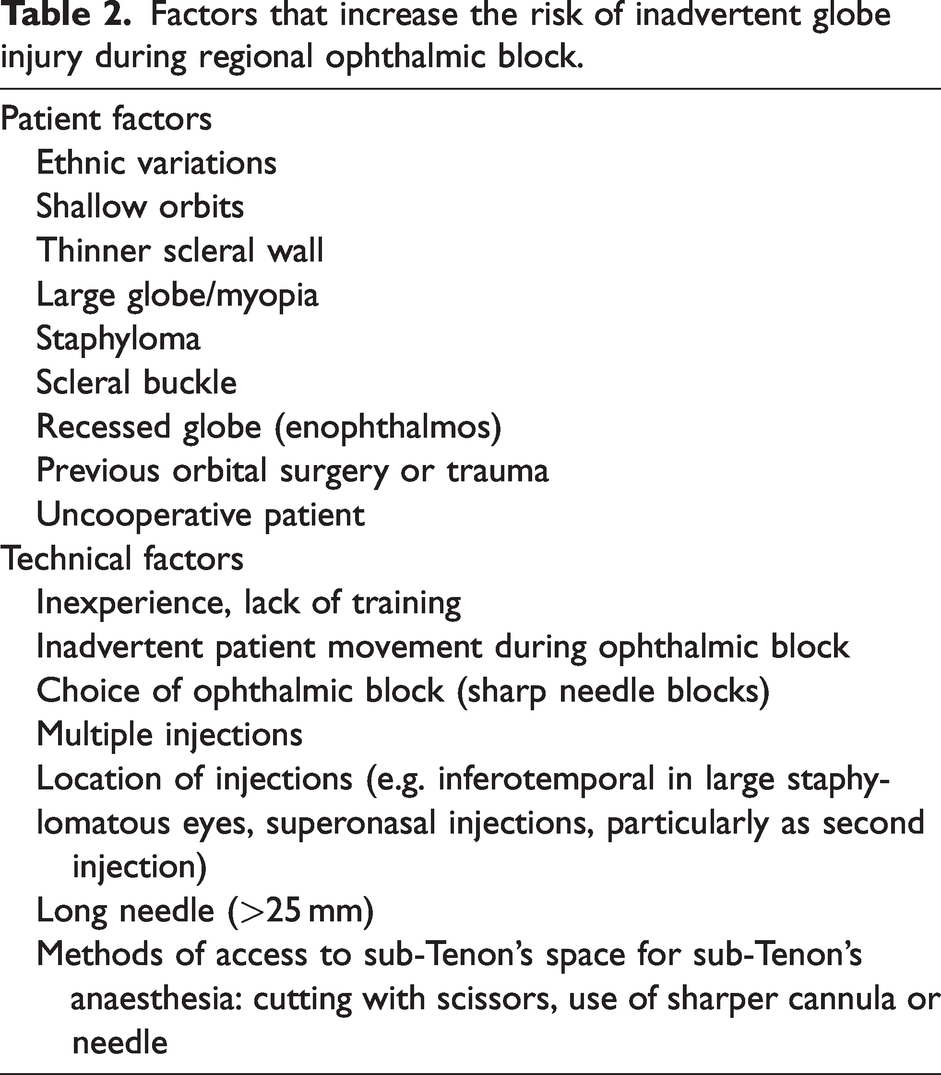
There are many factors that can potentially increase the risk of regional anaesthesia-related globe injury during routine clinical practice (Table 2). Patient factors include ethnic variations in orbital shape 21 and orbital depth, 22 shallow orbit, myopic eye, 23 recessed globe, scar and adhesions associated with previous ocular surgery or trauma, 24 presence of scleral buckle or staphyloma20,25 and lack of patient cooperation. 26 Technical factors include the skill and experience of the clinician performing the ophthalmic block,27,28 type of ophthalmic block employed,23,29 multiple injections,27,30 using a long needle (≥35 mm) for peribulbar block20,26 and using sharper cannula/needle or cutting with scissors to access sub-Tenon’s space.24,31
Factors that increase the risk of inadvertent globe injury during regional ophthalmic block.
Management of ocular hypotony
The management of hypotony involves a careful work-up by the ophthalmologist to establish the cause. Many cases are amenable to non-surgical management, for example, bandage contact lens to seal a small leak, 32 cycloplegic and steroid drops to manage uveitis, or slit-lamp—mounted laser treatment for some cyclodialysis clefts. Surgery is likely to be required for large leaks and/or more severe cases. Some cases may be treated with non-ophthalmic surgery (e.g. carotid endarterectomy in ocular ischaemic syndrome).33,34 Overall management strategies of hypotony are beyond the scope of this article and details can be found in other references.2,4,6,7,35 Traumatic hypotony usually requires urgent surgical repair, whereas iatrogenic hypotony may be less urgent and many cases can be scheduled for surgery as elective procedures.
Anaesthetic considerations for surgical management of ocular hypotony
Hypotonous eyes have varying degrees of severity and patient comorbidities. Preoperative discussion between the ophthalmologist and anaesthetist is critical, as there is no universal best anaesthetic method that is suitable for all cases. The surgical plan, severity of hypotony and estimated surgical duration are the main considerations in selecting anaesthetic modality. Coughing, bucking and forceful squeezing of the lids can precipitate extrusion of ocular contents. The following are general suggestions, based on the authors’ experience and published literature.
General anaesthesia
Basic principles of general anaesthesia for ophthalmic surgery apply in ocular hypotony, with some additional considerations. Most agents employed during general anaesthesia have minimal effect on IOP: volatile agents, nitrous oxide, thiopentone, propofol, benzodiazepines, opioids and non-depolarising muscle relaxants. 36 If there is continuous leakage, the case should be managed as an ‘open globe’. Facemask positioning is important because even mild pressure on a hypotonous eye could induce a choroidal (expulsive) haemorrhage. Increases in heart rate, blood pressure and IOP, resulting from sympathetic responses associated with laryngoscopy and intubation, 37 can be attenuated with pharmacological agents, including additional propofol and higher doses of fast-acting opioids. 38 However, their use should be balanced carefully against their unwanted side-effects, especially in the elderly and in cardiovascularly compromised patients. Depolarising muscle relaxants are best avoided in an ‘open globe’ as contraction of extraocular muscles may lead to extrusion of ocular contents. 39
Regional anaesthesia
Many cases of mild-to-moderate ocular hypotony may be amenable to topical anaesthesia or regional ophthalmic block9,40–42 and these are particularly useful in medically unwell patients.43,44 The authors are of the opinion that hypotony exacerbates pre-existing risk factors (Table 2) and further increases the risk of inadvertent globe injury with regional anaesthesia. If a hypotonous eye is considered suitable for an ophthalmic block, the techniques should be modified, and performed by experienced clinicians, to minimise further complications. In some cases, it may be appropriate to apply a bandage contact lens or adhesive glue initially to seal the wound prior to administering a block.32,45 Sufficient time should be allowed for the block to work while ocular compression should be avoided.
A blunt cannula technique (sub-Tenon’s block) is usually preferable over a sharp needle technique (peribulbar block). 31 If a peribulbar block is considered to be appropriate, then a carefully placed medial canthal approach may be safer than the traditional inferotemporal approach, especially in the myopic eye. 46 We recommend using a shorter needle (≤25 mm), smaller local anaesthetic volume, addition of hyaluronidase, slower injection and direct visualisation to monitor wound stability. A blunt needle tip (45° short bevel) may provide a false sense of security as it does not prevent globe perforation.23,26,27 It is important to avoid multiple injections but if it is necessary, a supplementary block should be administered after the globe has returned to its natural position. Avoid pushing or firm contact on the sclera, the use of a sharp or relatively sharp tip instrument, or the use of a more forceful action when performing a sub-Tenon’s block.
However, choosing an ophthalmic block may be inappropriate for several reasons. Administration of local anaesthetic into the orbit might further compress and squeeze the globe. A sharp needle block could be at increased risk of perforating the globe again. Administering a sub-Tenon’s block can also be dangerous in a very soft eye, because of difficulty finding the correct plane for injection, and the advancing cannula could provoke choroidal haemorrhage. Some trauma cases have an occult scleral rupture, meaning that a sub-Tenon’s cannula could potentially penetrate the globe. It may be necessary, for instance, to even alter the anaesthetic technique during surgery. Addition of adrenaline to local anaesthetic should be considered as an absolute contraindication when there is existing impaired ocular perfusion such as anterior chamber ischaemia.
Traumatic and penetrating open globe injury
The choices of anaesthetic modality and the controversy of suxamethonium in open globe injury have been well described, debated and documented.39–41,45,47 While general anaesthesia remains the mainstay technique, topical anaesthesia and ophthalmic block, with monitored anaesthesia care, have been used successful in many cases, especially in anteriorly located wounds and shorter wound length (<6.5 mm). In selected cases, it may be appropriate for the surgeon to perform an initial repair of the corneal wound using topical anaesthesia, then administer a gentle sub-Tenon’s block ‘on the table’ before dealing with any more posterior trauma.
The most challenging condition is the management of emergency repair for open globe injury in a non-fasted patient. The decision to proceed with urgency should be made after weighing up the risk of aspiration and the likelihood of preserving visual outcome. 36
Post-surgical leak
Early post-surgical leakage may be amenable to re-suturing under topical anaesthesia. However, more severe situations may need prolonged surgery on an ‘open’ eye, and thus would benefit from general anaesthesia. Revision of glaucoma surgeries may require extensive manipulation, including suturing to the sclera and/or conjunctival autografts: often the IOP is not particularly low, thus allowing for a sub-Tenon’s block or subconjunctival local anaesthesia.
Over-drainage after glaucoma surgery
Subconjunctival autologous blood can be injected using topical anaesthesia. Suturing conjunctiva to sclera would normally require subconjunctival local anaesthesia or an ophthalmic block. A formal revision procedure may require scleral patching: some can be performed under subconjunctival local anaesthesia, others may require sub-Tenon’s block, perhaps administered by the surgeon using the operating microscope.
Ocular injury from ophthalmic regional anaesthesia–related complications
Ophthalmic regional anaesthesia–related ocular complications can present with retinal haemorrhage and/or retinal detachment, in addition to ocular hypotony. Surgical management includes vitrectomy, air-fluid exchange, injection of gas or silicone oil, and scleral buckle surgery.20,23,25,26 Visual outcome is often significantly impaired; in two studies, >65% of the total patients achieved a final visual acuity of counting fingers or worse.23,26 General anaesthesia is, therefore, the preferred option in view of the potential medicolegal implications from the previous complication. 23
Ocular ischaemic syndrome
Ocular ischaemic syndrome, caused by severe common or internal carotid artery stenosis, can present with ocular hypotony. 33 Patients often have associated comorbidities, such as hypertension and diabetes mellitus. 34 The treatment is carotid endarterectomy or stenting and the anaesthesia for these procedures has been well described.48–50
Summary
In summary, ocular hypotony can occur for many reasons, with ocular trauma the most common cause. Intraocular surgery and inadvertent ophthalmic regional anaesthesia–related complications are the main reasons for non-traumatic ocular hypotony in adults. Some of these patients require surgical intervention(s) necessitating repeat anaesthesia. Traumatic hypotony usually requires urgent surgical repair whereas many cases of iatrogenic causes can be managed conservatively or as elective procedures. There is no universal best technique for all of these patients. Topical anaesthesia and ophthalmic block, with modified techniques, are suitable and amenable in many cases whilst general anaesthesia is more likely to be needed for complex procedures, longer surgical duration or severely distorted globes.
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the search, authorship and/or publication of this article.