
Abstract
We conducted a survey of Australian and New Zealand anaesthetists to determine self-reported practice of perioperative oxygen administration and to quantify perceptions regarding the perceived benefits and risks resulting from liberal oxygen therapy delivered in a manner consistent with the current World Health Organization guidelines. In addition, we sought feedback on the acceptability of several proposed clinical trial designs aiming to assess the overall effect of liberal and restricted perioperative oxygen regimens on patient outcomes. We developed a 23-question electronic survey that was emailed to 972 randomly selected Australian and New Zealand College of Anaesthetists (ANZCA) Fellows. We received responses from 282 of 972 invitees (response rate 29%). The majority of survey participants indicated that they routinely titrate inspired oxygen to a level they feel is safe (164/282, 58%) or minimise oxygen administration (82/282, 29%), while 5% of respondents indicated that they aim to maximise oxygen administration. The mean value for targeted intraoperative fraction inspired oxygen (FiO2) was 0.41 (standard deviation 0.12). Of the survey respondents, 2/282 (0.7%) indicated they believe that routine intra- and postoperative administration of ≥80% oxygen reduces the risk of surgical site infection. Well-designed and conducted randomised trials on this topic may help to better direct clinicians' choices. A high level of willingness to participate (80% of responses) in a study designed to investigate the impact of differing approaches to perioperative oxygen administration suggests that recruitment is likely to be feasible in a future study.
Introduction
Despite almost every general anaesthetic involving the administration of supplemental oxygen intra- and perioperatively, the optimal approach to intra- and perioperative oxygen therapy is uncertain. The World Health Organization (WHO) and Centers for Disease Control and Prevention (CDC) guidelines for the prevention of surgical site infection (SSI) recommend administration of 80% oxygen (liberal oxygen therapy) during and for up to 6 h after surgery under general anaesthesia (GA) with tracheal intubation.1,2
SSI is the commonest complication of surgery and represents a significant healthcare problem worldwide.3 There are a number of potential mechanisms by which liberal oxygen therapy might reduce SSI. These include enhanced innate immune system function and bacterial killing, and augmented tissue healing.4–6
However, there are also potential mechanisms by which liberal oxygen therapy might cause harm. Specifically, excess reactive oxygen species may overwhelm reductive systems and cause cellular dysfunction and apoptosis.7 Moreover, sustained hyperoxia has been shown to cause atelectasis and lung injury,8,9 reduce cardiac output and reduce blood flow in the coronary, cerebral and peripheral circulations.10–14 A restricted approach to oxygen therapy that limits exposure to higher levels of inspired oxygen than is necessary by titration of oxygen to avoid abnormally low arterial oxygenation, might reduce the risk of such potentially toxic pulmonary effects of oxygen. Data from a recent systematic review and meta-analysis suggest that compared with a liberal oxygen strategy, a restricted oxygen strategy might reduce mortality risk when administered to critically ill patients across a wide range of acute conditions.15
The current WHO guidelines advocating for a liberal strategy of perioperative oxygen administration have attracted considerable criticism;16–19 however, the views of the Australian and New Zealand anaesthesia community about these guidelines have not been described. Accordingly, we undertook a survey to quantify the self-reported practice and perceptions of Australian and New Zealand College of Anaesthetists (ANZCA) Fellows regarding the risks and benefits associated with various approaches to perioperative oxygen therapy. In addition, we aimed to assess the acceptability of several proposed clinical trials designed to determine the overall effect of liberal and restricted perioperative oxygen therapy on important patient outcomes. We hypothesised that a minority of respondents would report administering oxygen liberally in accordance with the WHO guidelines.
Methods
A waiver of the requirement for full ethics review of this low-risk study was provided by the University of Otago, Wellington School of Medicine Ethics Committee. Subsequent approval was obtained under the ANZCA Clinical Trials Network (CTN) survey research policy to conduct this survey. The survey was constructed using the SurveyMonkey online survey platform. Questions were designed by the authorship group to meet study aims, and underwent peer review by the ANZCA CTN survey research review process. The survey consisted of four demographic and professional classification questions, and 19 questions addressing practice patterns and perceptions (see Appendix 1 in the online supplementary material).
The ANZCA CTN distributed the survey to a randomly selected group of 972 of the 5557 ANZCA Fellows practising in Australia and New Zealand at the time of dissemination of our survey. This is the standard sample size for ANZCA surveys. Sample size calculations were not performed. Participants were contacted during September 2018 via email, with a weblink to the online survey. A reminder email was sent after approximately two weeks to improve response rate, and the survey was closed three weeks after the first email. All data were collected anonymously; internet protocol (IP) addresses and other potentially identifying metadata were not recorded. Data were transferred to Microsoft Excel for analysis; chi-square tests were performed for comparison of selected characteristics of respondents with those of ANZCA Fellows overall, and mean and standard deviations (SD) or median and ranges calculated for survey responses where appropriate. ANZCA provided a summary of overall demographic data for all current Fellows. There was no imputation of missing data. The survey is reported here in accordance with published guidelines on survey research.20,21
Results
Demographics
The survey response rate was 29% (282 of 972); demographics of survey respondents and ANZCA Fellows overall are summarized in Table 1. There were minor geographical differences between the survey respondents and ANZCAs overall, and a significantly greater proportion of respondents with greater than 20 years of specialist practice than ANZCA Fellows overall. The majority of survey respondents’ primary work category was clinical work in a secondary or tertiary public hospital.
Demographics of survey respondents and Fellows of the Australian and New Zealand College of Anaesthetists overall.
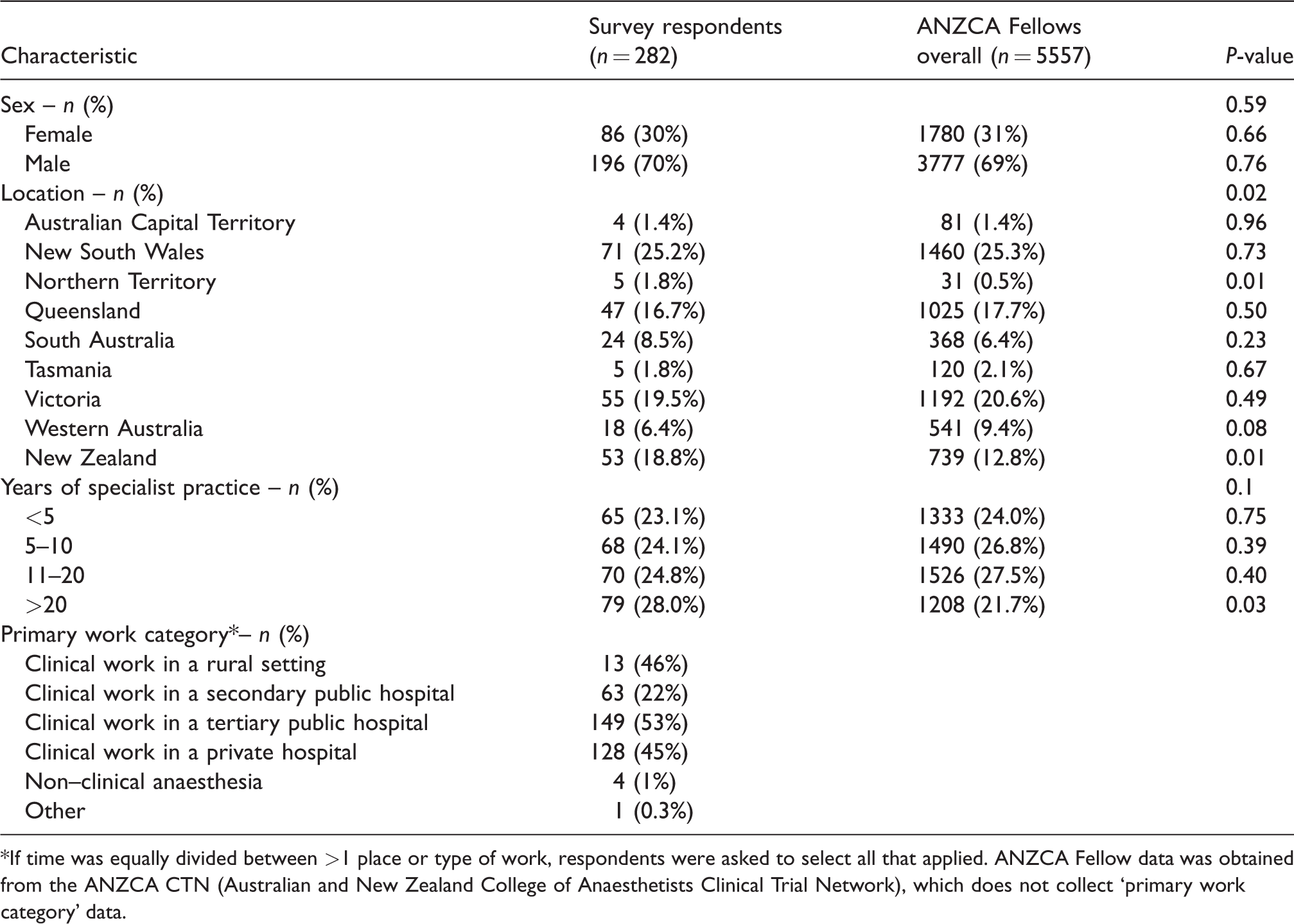
*If time was equally divided between >1 place or type of work, respondents were asked to select all that applied. ANZCA Fellow data was obtained from the ANZCA CTN (Australian and New Zealand College of Anaesthetists Clinical Trial Network), which does not collect ‘primary work category’ data.
Practice patterns
Titration of inspired oxygen fraction
The majority of respondents (164/282, 58%) aimed neither to routinely minimise nor maximise inspired oxygen intraoperatively, but instead preferred to titrate the inspired oxygen to achieve a desired SpO2 goal. A further 29% (82/282) aimed to minimise inspired oxygen intraoperatively when possible; however, only 5% (15/282) aimed to maximise inspired oxygen. Eight percent (21/282) indicated that they were inconsistent in their approach to intraoperative fraction of inspired oxygen (FiO2) administration, or unsure.
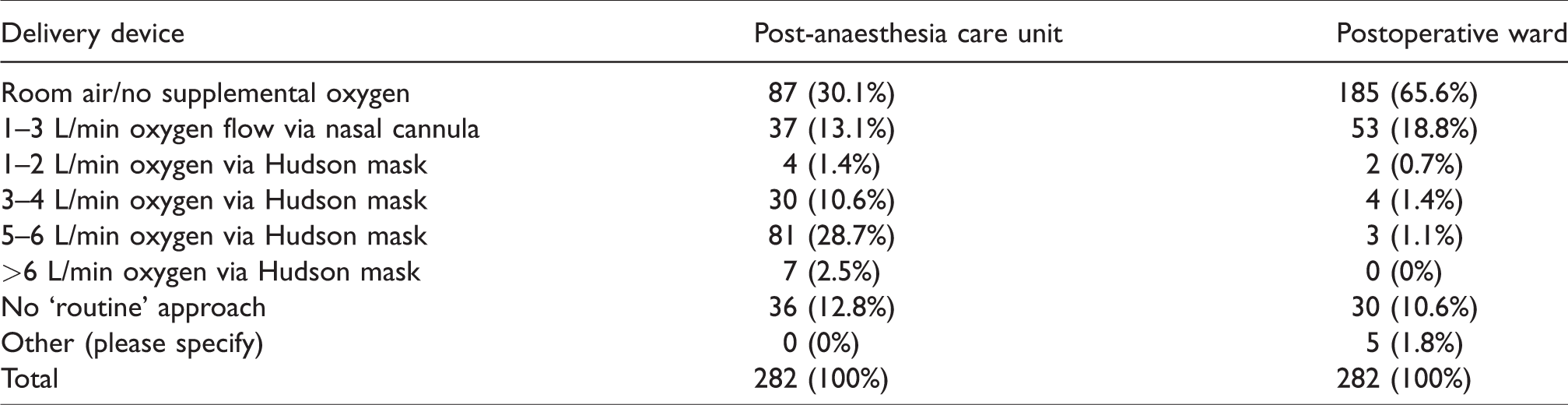
The reported mean and median FiO2 targets during the intraoperative phase for respondents managing a routine case in a patient with no specific need for increased FiO2 were mean 0.41 (SD 0.12); median 0.4 (range = 0.21–1.0). For the postoperative post-anaesthesia care unit (PACU) and postoperative ward phases, respondents were asked to select one from a list of options of oxygen delivery devices and flow rates that most closely resembled their practice. These data are displayed in Table 2.
Oxygen flow rate and delivery device utilised in the post-anaesthesia care unit and postoperative ward according to survey responses.
Saturation targets
The reported lower acceptable limit of sustained intraoperative SpO2 during the maintenance phase of a general anaesthetic in an elective surgical patient was mean 94.1% (SD 1.7%); median 94% (range 89%–98%). The lower acceptable limit of sustained SpO2 in the PACU was mean 93.8% (SD 1.6%); median 94% (range 89%–97%).
Perceived risks and benefits of liberal oxygen therapy
When asked to consider a hypothetical case of a patient with no specific indication for either high or low oxygen, 92.5% (259/280) of respondents stated that they did not believe that routine FiO2 ≥ 0.8 would confer any benefit. A further 2.9% (8/280) indicated that they believed there was a benefit to routine FiO2 ≥ 0.8 and 4.6% (13/280) were unsure. Underlying reasons cited to explain potential benefits of high FiO2 included an increased margin of safety in the event of an intraoperative crisis (6/280, 2%), reduced postoperative infection (2/280, 0.7%), and reduced cardiovascular (1/280, 0.4%) and neurocognitive complications (1/280, 0.4%). Conversely, 85% (239/280) of participants believed there was a risk of harm resulting from administering routine FiO2 ≥ 0.8 in this scenario, and a further 9% (25/280) stated that they were unsure. Perceived mechanisms of harm included increased likelihood of pulmonary complications (199/280, 71%), ‘as yet unquantified risks’ (106/280, 38%), increased neurocognitive (35/280, 13%) and cardiovascular (31/280, 11%) complications, and increased mortality risk (21/280, 8%). The percentage of respondents overall indicating benefit or harm from intraoperative administration of high FiO2 on various patient outcomes is displayed in Figure 1.
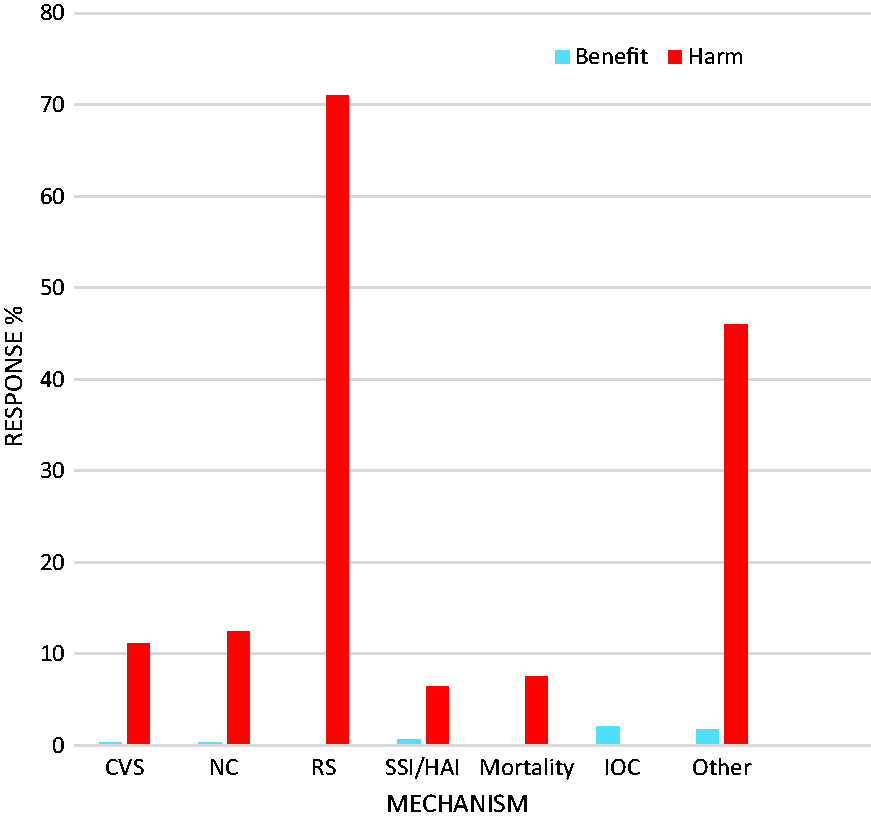
Percentage of respondents overall indicating perceived risk of benefit versus harm from liberal oxygen therapy on selected patient outcomes.
Specific indications for hyperoxia
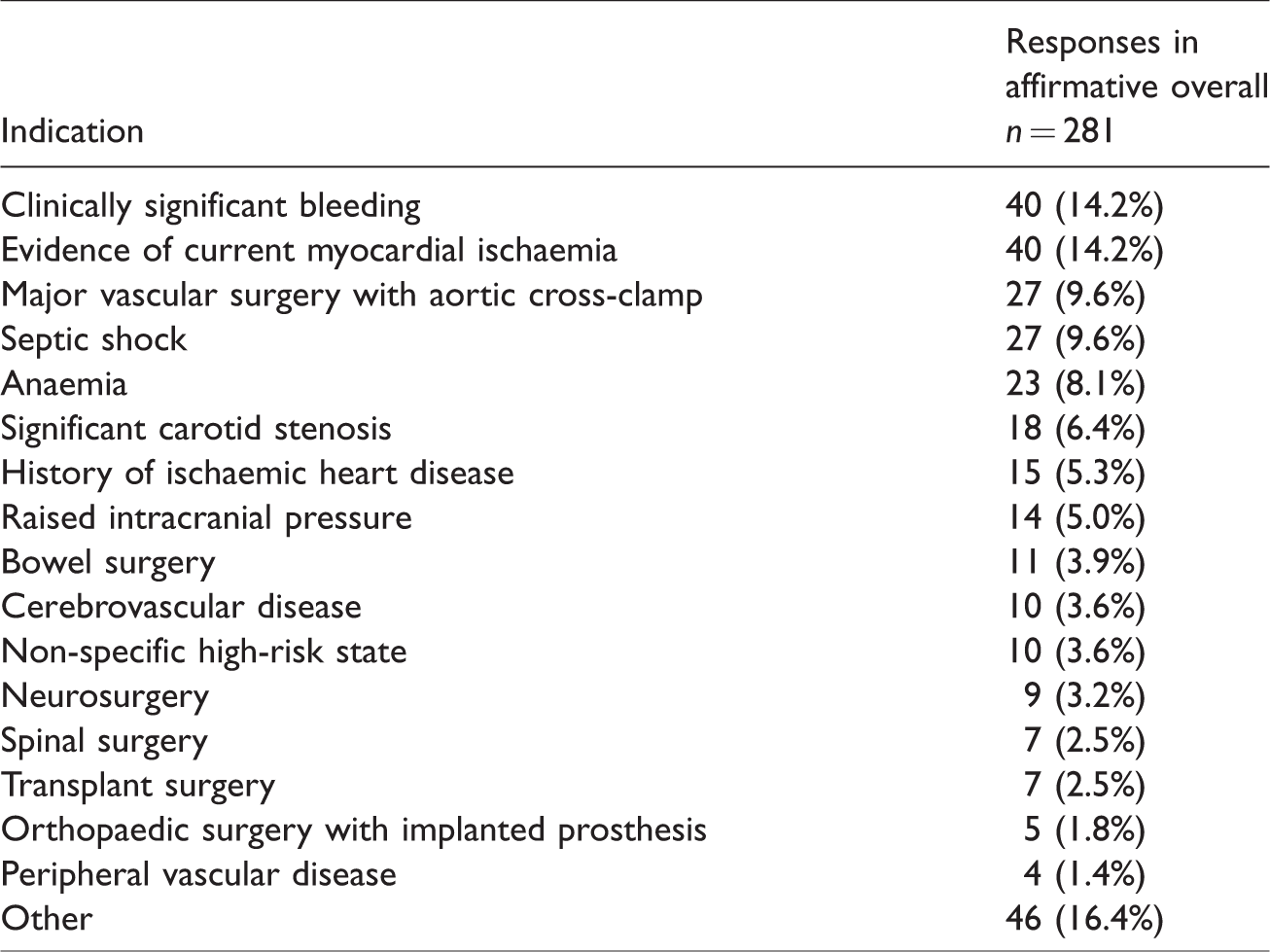
32% (90/281) of respondents believed that specific indications exist for intraoperative hyperoxia (PaO2 > 100 mmHg). Cited indications for hyperoxia under GA are displayed in Table 3. The most frequently cited indications were current evidence of myocardial ischaemia (40/90, 44%), clinically significant bleeding (40/90, 44%), septic shock (27/90, 30%), major aortic surgery with cross-clamping (27/90, 30%), anaemia (23/90, 26%) and carotid stenosis (18/90, 20%). The majority of respondents (149/281, 53%) did not believe that any specific indications exist for hyperoxia under GA, and 15% (42/281) were unsure.
Indications for arterial hyperoxia as indicated by survey respondents.
Future studies
The final three questions assessed the willingness of respondents to participate in a clinical trial aiming to address the impacts of perioperative oxygen therapy on postoperative patient outcomes. When asked to consider a proposed study that compared liberal oxygen therapy to standard care alone, or restricted oxygen therapy to standard care alone, 157/277 (57%) and 155/277 (56%) indicated they would be willing to participate in the respective study designs. When asked whether they would be willing to participate in a study comparing liberal with restricted oxygen therapy, 122/152 (80%) answered in the affirmative. The mean value for the lowest SpO2 that respondents felt should be defended to maintain participant safety in the restricted arm of an interventional trial was 93.2% (SD 1.7%); median 94%, (range 88%–96%).
Discussion
Summary of principal findings
In this survey of ANZCA Fellows’ practice and attitudes toward oxygen therapy in the perioperative period, we found that very few respondents reported following current WHO guidelines advocating for liberal oxygen therapy. Conversely, almost a third of respondents indicated that they aim to minimise exposure to supplemental inspired oxygen when possible, while the majority reported titrating intraoperative FiO2 to a SpO2 that they feel is safe. A minority of respondents thought that there were any specific indications for liberal oxygen therapy. Furthermore, few respondents indicated that routine liberal perioperative oxygen therapy was beneficial, and fewer still believed that high FiO2 reduced the risk of SSI. In contrast to this, a large majority of respondents thought that there was a significant risk of patient harm resulting from routine liberal oxygen therapy.
Comparison with previous studies
As far as the authors are aware no similar anaesthesia-specific surveys on perioperative oxygen therapy have been published to date. A survey of Australian and New Zealand intensive care specialists found marked heterogeneity in the attitudes toward and beliefs about oxygen therapy in mechanically ventilated intensive care patients.22 However, as in the present survey, 85% of respondent intensivists reported thinking that oxygen-related lung injury was a concern when placing a patient on mechanical ventilation. A survey distributed to 1523 members of the Australian College of Critical Care Nurses found that 36% of the 542 respondents thought that oxygen toxicity was a greater threat for lung injury than barotrauma in mechanically ventilated patients.23 A subsequent survey of intensive care nurses and doctors found that the majority of respondents considered oxygen-related lung injury to be a major concern.24 This appears to be aligned with the view of anaesthesia respondents in the present survey, that liberal oxygen therapy poses a substantial risk of respiratory system complications.
A 2010 survey of 524 United Kingdom emergency medicine, cardiology and ambulance staff on the practice and beliefs of oxygen use in acute myocardial infarction (MI) found that 61.3% of respondents thought oxygen therapy reduced the risk of death, while only 1.3% believed it could worsen mortality.25 Interestingly in the present study, an equal number of respondents thought that liberal intraoperative oxygen administration was indicated in the presence of acute myocardial ischaemia, as the number who thought that routine liberal intraoperative oxygen therapy increased the risk of cardiovascular complications. This may reflect more recent evidence that the routine provision of supplemental oxygen does not appear to improve outcomes following acute MI.26,27
The mean self-reported intraoperative FiO2 administered by specialist anaesthetists in the present survey is lower than the practice patterns suggested from international observational data. A recent observational study of British anaesthetists found that the mean intraoperative FiO2 administered to adult patients having non-cardiac surgery where an arterial cannula was placed by the treating anaesthetist, was 0.49.28 A North American retrospective registry study of 73,922 adult patients, undergoing non-cardiac surgery with tracheal intubation, showed an overall median FiO2 of approximately 0.52.29 Potential discrepancies between self-reported and actual practice are well known;30 however, no observational studies characterising intraoperative FiO2 among Australian and New Zealand anaesthetists have been published to our knowledge.
Strengths and weaknesses
Our survey response rate of 29% was comparable with previous ANZCA-facilitated surveys,31–33 and was a representative sample of the ANZCA Fellow population with respect of sex and years of specialist practice. There was a significant difference in geographical distribution between survey respondents and ANZCA Fellows overall. The survey had a high completion rate of the questions relating to practice patterns and attitudes to perioperative oxygen therapy. The final three questions on potential future studies had a lower completion rate.
Due to the diminishing number of responses to questions relating to the possible design of future trials, there may be some selection bias of respondents, with respondents who were more enthusiastic about the proposed studies being more likely to respond to the final three survey questions. We may therefore have overestimated the proportion of ANZCA Fellows willing to engage in a future study of perioperative oxygen therapy. Additionally, surveys of self-reported practice are vulnerable to responder bias, whereby survey invitees with the greatest interest in the survey content may be most likely to respond, thereby resulting in a non-representative sample.
Clinical implications
We found that the large majority of ANZCA specialist anaesthetists who responded to this survey did not think that there is any benefit from liberal perioperative oxygen therapy, and in particular did not think that liberal oxygen reduces the risk of SSI. The majority of respondents were however concerned about the potential for patient harm resulting from liberal oxygen administration, with a significant number indicating that it may be associated with an increased mortality risk. Similarly, the overwhelming majority of survey respondents do not appear to follow the current WHO recommendation advocating for ≥80% perioperative oxygen administration. This observation may be partially explained by limited translation of evidence into clinical practice and a perceived lack of benefit from routine liberal perioperative oxygen therapy.
The lack of consensus demonstrated in this survey mirrors the current lack of high-level evidence used to inform guidelines for perioperative oxygen therapy and suggests that conducting further studies addressing the impact of liberal and restricted perioperative oxygen therapy on patient outcomes is a priority. In addition, it is expected that engagement in such studies is likely to be high. The design of any future study should be informed by the findings that the greatest percentage of respondents in this survey indicated a willingness to participate in a study comparing liberal and restricted oxygen therapy, compared with either liberal or restricted versus standard care alone.
Supplemental Material
Supplemental material for Practice patterns and perceptions of Australian and New Zealand anaesthetists towards perioperative oxygen therapy
Supplemental Material for Practice patterns and perceptions of Australian and New Zealand anaesthetists towards perioperative oxygen therapy by Daniel R Frei, Richard Beasley, Douglas Campbell, Kate Leslie, Alan F Merry, Matthew Moore, Paul S Myles, Laura Ruawai-Hamilton, Tim G Short and Paul J Young in Anaesthesia and Intensive Care
Footnotes
Acknowledgements
We wish to thank the Australian and New Zealand College of Anaesthetists Clinical Trials Network for providing peer review and facilitating distribution of this survey.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.