
Abstract
Summary
Reducing maternal mortality remains a global priority, particularly in low- and middle-income countries (LMICs). The Safer Anaesthesia from Education (SAFE) Obstetric Anaesthesia (OB) course is a three-day refresher course for trained anaesthesia providers addressing common causes of maternal mortality in LMICs. This aim of this study was to investigate the impact of SAFE training for a cohort of anaesthesia providers in Ethiopia.
We conducted a mixed methods longitudinal cohort study incorporating a behavioural questionnaire, multiple-choice questionnaires (MCQs), structured observational skills tests and structured interviews for anaesthesia providers who attended one of four SAFE-OB courses conducted in two regions of Ethiopia from October 2017 to May 2018.
Some 149 participants from 60 facilities attended training. Behavioural questionnaires were completed at baseline (n = 101, 69% response rate). Pre- and post-course MCQs (n = 121, n = 123 respectively) and pre- and post-course skills tests (n = 123, n = 105 respectively) were completed, with repeat MCQ and skills tests, and semi-structured interviews completed at follow-up (n = 88, n = 76, n = 49 respectively). The mean MCQ scores for all participants improved from 80.3% prior to training to 85.4% following training (P < 0.0001) and skills test scores improved from 56.5% to 83.2% (P < 0.0001). Improvements in MCQs and skills were maintained at follow-up 3–11 months post-training compared to baseline (P = 0.0006, < 0.0001 respectively). Participants reported improved confidence, teamwork and communication at follow-up.
This study suggests that the SAFE-OB course can have a sustained impact on knowledge and skills and can improve the confidence of anaesthesia providers and communication within surgical teams.
Introduction
More than half of global maternal deaths occur in sub-Saharan Africa, 1 with Ethiopia being one of six countries previously contributing more than half of these deaths. 2 The major pregnancy complications accounting for around 75% of maternal deaths are haemorrhage, infections, hypertensive disorders, delivery complications and unsafe abortion, 3 conditions often requiring anaesthesia, surgery and critical care.
The maternal mortality rate (MMR) in Ethiopia remains unacceptably high at 353 per 100,000 live births. 2 , 4 A publication from Ethiopia suggested the most common reasons for admission of obstetric patients to the intensive care unit (ICU) were eclampsia or uterine rupture secondary to obstructed labour, with a 42.9% mortality rate. 5
Deaths due to anaesthesia are higher in low-income countries,6–8 with shortages of skilled providers and lack of simple monitoring equipment contributing to anaesthesia-related maternal mortality. 9 The Lancet Commission on Global Surgery 10 highlighted the global deficiencies in surgery and anaesthesia provision, leading to the development of safe surgery programmes such as the GE Foundation Safe Surgery 2020 (SS2020; https://www.safesurgery2020.org).
Anaesthesia in Ethiopia is provided by physicians (physician anaesthesia providers (PAPs)), and non-physician anaesthesia providers (NPAPs), with only 0.05 PAPs per 100,000 population. 11 Anaesthesia training programmes for NPAPs vary from 18 months to over four years, with varied curricula and entry requirements. NPAP training includes: Anaesthesia Nurse Diploma, Level V Anaesthesia (18 months); Bachelor of Science Anaesthesia (BSc; three to four years, commonest form of anaesthesia training); and Master of Science Anaesthesia (MSc; BSc plus two years). PAPs undertake three-year residency programmes. There is little ongoing refresher training for all levels of provider. With this heterogeneous anaesthesia workforce, it is important to ensure all providers are equipped with the knowledge and skills to provide safe obstetric anaesthesia.
The Safer Anaesthesia from Education (SAFE) courses were developed as an educational initiative by the Association of Anaesthetists of Great Britain and Ireland (AAGBI) and the World Federation of Societies of Anaesthesiologists (WFSA). The SAFE Obstetric Anaesthesia (SAFE-OB) course is a three-day refresher course for trained anaesthesia providers to address essential obstetric anaesthesia and the most common causes of maternal death. 12 Since the first course in 2011 there have been 104 SAFE-OB courses in 40 countries, 3244 anaesthesia providers and 581 trainers trained (WFSA, personal communication, January 2020).
The aim of this mixed methods longitudinal cohort study was to investigate the educational impact of the SAFE-OB course in a cohort of anaesthesia providers who had attended training, by assessing knowledge and skills before and after training and at follow-up, and through structured interviews at follow-up.
Materials and methods
Ethical approval was obtained for this study from Bahir Dar University Institutional Review Board (protocol 02051/18-09). Multiple-choice questionnaires (MCQs) and skills tests were conducted as part of routine evaluation of the educational programme, with secondary analysis of anonymised data.
NPAP providers were invited to attend one of four SAFE-OB courses run between October 2017 and May 2018 (two courses in Amhara and two in Tigray) (Figure 1). Trainee anaesthesiologists sponsored by and due to return to these regions post-completion of training in Addis Ababa were also invited, as well as a small number of NPAPs from Afar, Dire Dawa and Southern Nations, Nationalities and Peoples (SNNP) regions. Training was in the English language and all participants had a good understanding of English.
Map illustrating the nine regions and two chartered cities of Ethiopia.
Courses were run in collaboration with the Federal Ministry of Health of Ethiopia, the Ethiopian Society of Anaesthesiologists (ESA), the Ethiopian Association of Anaesthetists (EAA) and Assist International. Participants were invited to attend from facilities selected by the Regional Health Boards of the Amhara and Tigray regions. A ‘Training of Trainers’ course was conducted alongside each SAFE-OB course, and 56 trainers trained.
Prior to training, all participants completed an anonymous behavioural questionnaire to establish baseline demographics and self-reported practice. This also included information on frequency of delivery of obstetric anaesthesia and neonatal resuscitation, and availability of required equipment. Participants were asked to rate on a Likert scale how often they would routinely perform a task. Scores of 0/10 were classified as never, 1–3/10 as rarely, 4–6/10 as sometimes, 7–9/10 as usually and 10/10 as always.
Multiple-choice questionnaires (MCQs) and structured observational skills tests were conducted immediately before and after training, and at follow-up. The MCQ comprised 50 ‘true–false’ statements related to obstetric anaesthesia. Participants completed one of four structured observational skills tests: neonatal resuscitation, maternal cardiopulmonary resuscitation, rapid sequence induction or eclamptic seizure. The same MCQ and skills test was then completed at the end of the course. Correct test answers or results were not shared with participants during the course or prior to follow-up repeat testing. MCQ examples are included in Appendix 1. Follow-up interviews explored the perceived impact of the SAFE-OB training and how this related to self-reported practice prior to training.
Three Ethiopian anaesthesiology residents who had taught on the SAFE-OB course followed up a convenience sample of participants in June, August or September 2018 during visits to the participants’ place of work. Follow-up included repeating the same MCQ and skills tests, and individual semi-structured face-to-face interviews. The skills test was scored against the same checklist utilised on the SAFE-OB course. Interviews were conducted in Amharic language. Interviews were audio-recorded, and later transcribed, anonymised and translated into English where required. Examples of interview questions are included in Appendix 2.
Participants from Afar, SNNP and Dire Dawa were excluded from follow-up due to travel distances. Participants from Addis Ababa University (AAU) who would be returning to work in Amhara or Tigray regions following training completion were eligible for follow-up.
Questionnaire responses were analysed quantitatively using MS Excel. Paired t-tests were used for subgroup analysis of paired complete data. Qualitative interview data were analysed thematically to identify key themes. These were subcategorised into non-clinical and clinical themes, with recurring sub-categories summarised and presented descriptively with examples as verbatim quotes. 13
Results
Demographics of course participants
A total of 149 participants attended the four courses, including nine anaesthesiology residents (all in training at AAU), 15 MSc level, 102 BSc level, 19 Level V and four Diploma Nurse providers. An additional 12 BSc students attended the courses but were excluded from the study. Participants on the courses were from 60 facilities, including both referral and district hospitals, primarily in Amhara (n = 59 participants) and Tigray (n = 70 participants), with a small number attending from the Afar (n = 5) and SNNP (n = 4) regions, and chartered cities of Dire Dawa (n = 2) and Addis Ababa (n = 9). There were 135 participants eligible for follow-up from Amhara and Tigray regions including those residents returning to these regions following anaesthesiology training.
Behavioural questionnaires
A total of 103 participants completed the behavioural questionnaire prior to training (69% response rate). Some participants did not complete the questionnaire due to late arrival and time constraints or chose not to complete or return it. Respondents had been in the anaesthesia profession for a median of two years (interquartile range (IQR) 2–5 (range 0–34 years)). In the two weeks prior to the course, the median number of Caesarean section cases performed by participants was six (IQR 4–10 (range 0–50)), and 81% respondents reported having all the equipment required for spinal anaesthesia available during those two weeks. More than half of respondents had performed neonatal resuscitation in the two weeks prior to the course (57%, n = 59). The median number of neonatal resuscitations that respondents had been involved in during those two weeks was one (IQR 0–2 (range 0–10)). Self-reported likelihood of performing specific tasks related to obstetric anaesthesia is illustrated in Table 1. No respondents answered ‘never’ to any actions.
Self-reported routine practices for Caesarean section (pre-course).
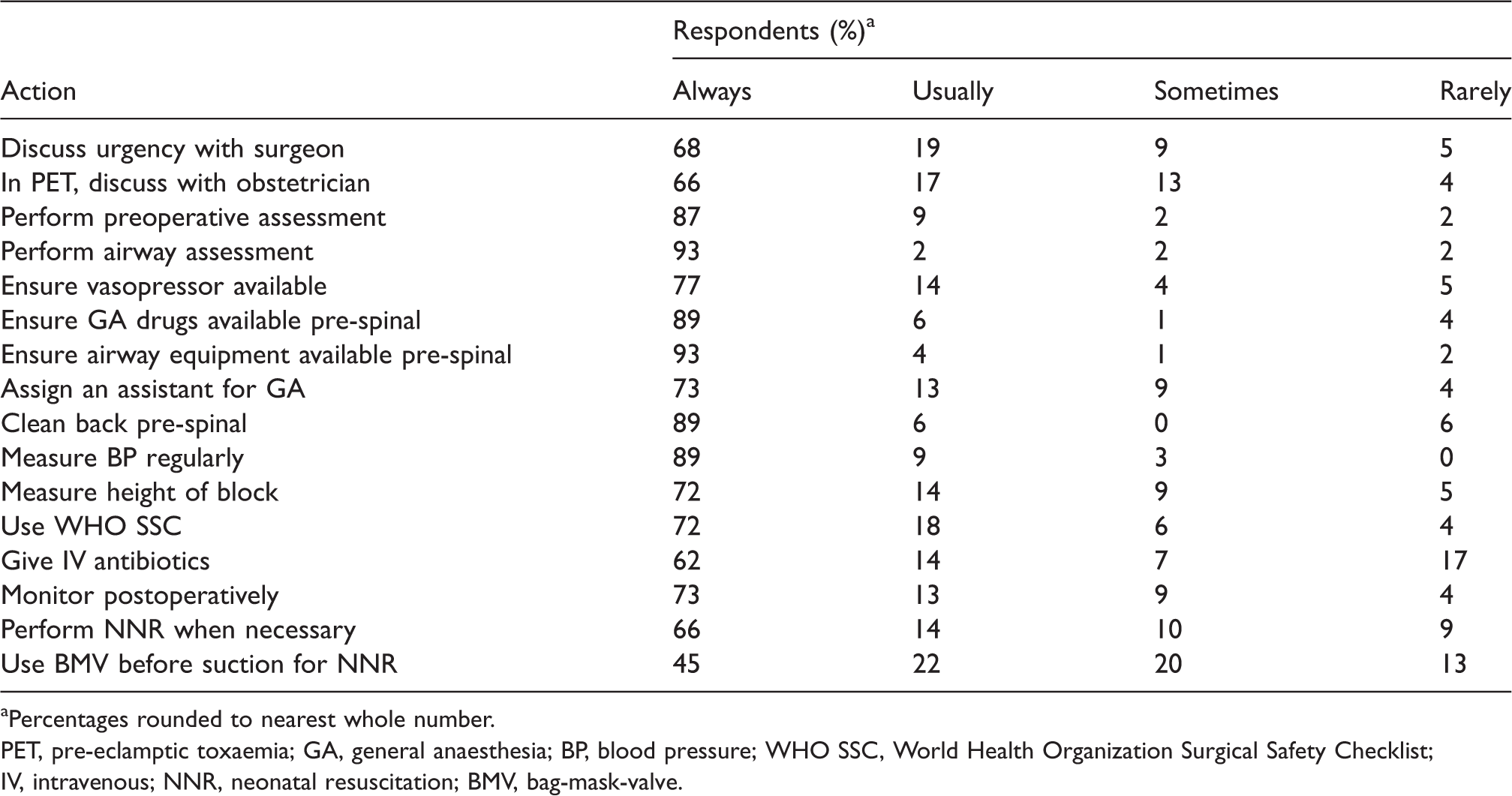
aPercentages rounded to nearest whole number.
PET, pre-eclamptic toxaemia; GA, general anaesthesia; BP, blood pressure; WHO SSC, World Health Organization Surgical Safety Checklist; IV, intravenous; NNR, neonatal resuscitation; BMV, bag-mask-valve.
Pre- and post-course knowledge and skills tests
A total of 121/149 (81%) and 123/149 (83%) participants completed the pre- and post-course MCQs, and 123/149 (83%) and 105/149 (70%) completed the pre- and post-course skills tests. A proportion of participants did not undertake the tests due to late arrival or early departure. MCQ scores for all participants improved from 80.3% to 85.4% (P < 0.0001) and the skills test improved from 56.5% to 83.2% (P < 0.0001) post-course. The summated pre- and post-course test results, and results from each individual course, are illustrated in Figure 2.
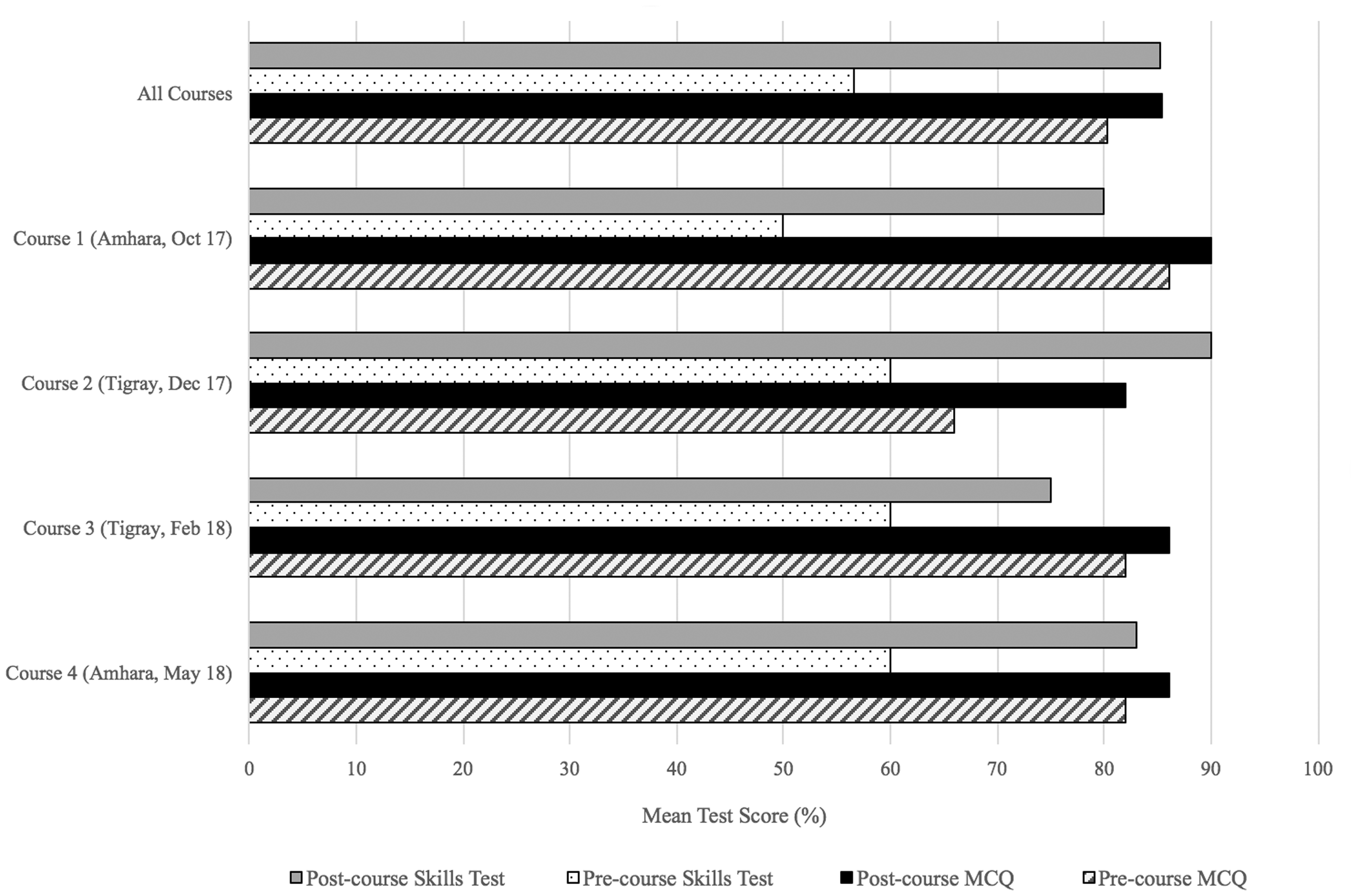
Mean scores (%) for pre- and post-course tests at each course.
Follow-up knowledge and skills tests
A total of 88 course participants (49 Amhara and 39 Tigray) completed follow-up MCQ tests and 76 completed skills tests. This cohort included six anaesthesiology residents, five MSc level, 68 BSc level, eight Level V and one Diploma Nurse. The mean follow-up MCQ score was unchanged from post-course at 85.2% (P = 0.8503) remaining higher than pre-course (P = 0.0006). Skills-test scores were unchanged from post-course at 80.2% (P = 0.2115) and maintained higher than pre-course (P < 0.0001). Scores are summarised in Table 2.
Summarised knowledge and skills scores in the subset followed up

MCQ: multiple-choice questionnaire.
For the 39 participants that completed all components of testing (pre-course, post-course and follow-up MCQ and skills tests), MCQ score increased from 81.8% pre-course to 84.6% post-course (P = 0.0473) and was not significantly different at follow-up at 86.3% (P = 0.1562) remaining significantly higher than pre-course (P = 0.047). In this group, the skills test score increased from 55.1% pre-course to 82.6% post-course (P < 0.0001) and was not significantly different at follow-up at 81.8% (P = 0.805), remaining significantly higher than pre-course (P < 0.0001).
Interviews
A total of 49 structured interviews were conducted during follow-up (33% course participants). Participants were asked to reflect on the course, and how it has impacted on their practice. All participants interviewed spoke positively of the training experience: ‘The SAFE teaching methodology, the materials they used in the course are new way of learning. The basic obstetric anaesthesia teaching was part of my University curriculum but SAFE taught me how to practise safely’ (Amhara region participant); ‘I expected the course to cover some topics of obstetric anaesthesia but once I was on the course it was so close to real life’ (Tigray region participant).
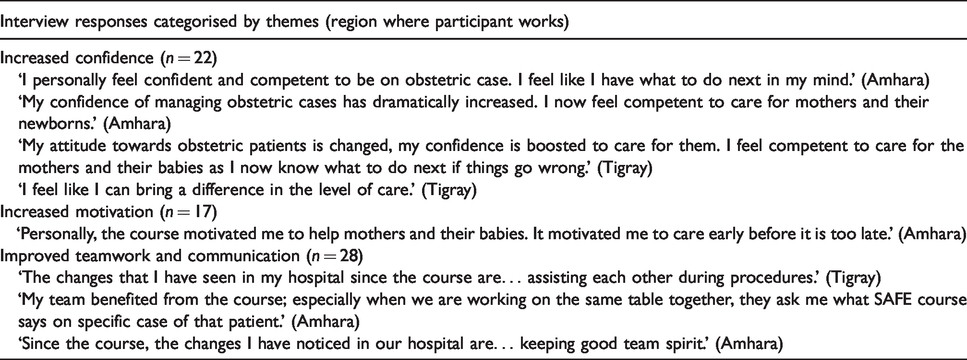
Emerging themes related to the impact of the course referred to: increased confidence (22 participants), building of teamwork and improved communication (28 participants) and feeling more motivated (17 participants). Of those interviewed, 28 noticed changes, citing improved teamwork and communication (28 participants) and increased use of the World Health Organization (WHO) Surgical Safety Checklist (10 participants). Examples are illustrated in Table 3.
Participant interview responses: effects on individual and teams.
Some participants commented on improved clinical care (nine participants). Twenty participants recalled cases that they managed differently after the course; 12 of these included a case where they had performed neonatal resuscitation effectively following the course. Examples are illustrated in Table 4.
Participant interview responses: effects on workplace.

WHO, World Health Organization; CS, Caesarean section; CPR, cardiopulmonary resuscitation.
Ongoing challenges included dissemination of material: ‘There were lots of challenges to accept some of the updated ideas from some of the colleagues who were not in the course’ (Amhara); and resources: ‘The challenges we have are [lack of] equipment … we are trying to solve those issues with the hospital’ (Amhara).
Discussion
This study provides a review of the educational impact of the three-day SAFE-OB course in two regions in Ethiopia. Our study highlights that the SAFE-OB course improves confidence, knowledge and skills of providers, and communication within surgical teams, with knowledge and skills maintained at follow-up. Understanding the impact of the course provides evidence for the SAFE-OB course as a potential means to improve knowledge, skills and practices in obstetric anaesthesia in Ethiopia.
Reducing maternal mortality remains a global priority, particularly in low- and middle-income countries (LMICs). Many of the causes of maternal mortality are preventable or treatable. It is estimated that in 2015, 303,000 maternal deaths occurred worldwide, equating to 830 per day. Around 99% of these occur in low-resource settings. 14
One in seven maternal deaths following Caesarean section in LMICs can be attributed to anaesthesia, with anaesthesia by non-physician providers identified as a risk factor. 15 There is, therefore, a need to ensure these providers are equipped with the knowledge and skills to provide safe obstetric anaesthesia.
Our study demonstrates that knowledge and skills, as well as confidence and teamwork, can potentially be improved through the SAFE-OB course. The SAFE-OB course was designed to focus on behaviours known to improve outcomes in obstetric anaesthesia. 12 Our baseline questionnaire suggested that tasks associated with preventable anaesthesia complications (for instance, measuring the height of a spinal block) were not always, and sometimes rarely, performed. Behaviours relating to communication, such as discussions with surgeon or obstetrician, were also not always performed. Infectious complications are known to be the single most important cause of perioperative morbidity and mortality in LMICs. 16 Our baseline questionnaire suggested that tasks associated with prevention of infection, such as cleaning the patient’s back before administering spinal anaesthesia and administering antibiotics, were not always, and sometimes rarely, performed.
Interviewed participants were positive regarding the knowledge and skills they gained from the course, and some felt that further improvements would be possible but were limited by resource availability. Many of those interviewed reported improved confidence, teamwork and communication following the course, particularly improved use of the WHO Surgical Safety Checklist, and reported positive consequences on clinical practice and case management.
These findings are relevant because there is reported high job dissatisfaction amongst anaesthesia providers in Ethiopia leading to high turnover rates, with a reported rate of 54.2% providers being dissatisfied in their role. Reasons for this included limited access to further education and dissatisfaction with in-service training. 17 A survey of practising anaesthetists from nine regions in Ethiopia conducted in 2012 reported up to 89% of respondents did not have routine access to safe conditions for provision of obstetric anaesthesia. This included limited access to utilities and resources. Lack of access to continuing professional development was reported as a barrier to service development and respondents suggested feelings of being marginalised and excluded from training. 18
In addition to improving knowledge and skills, our study suggests increased confidence and teamwork amongst those providers interviewed, as a consequence of the training. This, coupled with providing the desired additional education, could contribute towards improved job satisfaction and improved retention amongst anaesthesia providers.
There are currently few published studies analysing the impact of short educational initiatives in low resource settings. Systematic follow-up of the SAFE-OB course has been undertaken in Uganda, Rwanda, Bangladesh and Zambia and suggests the course is well received, and leads to both knowledge retention and positive changes in clinical practice. 12 , 19
A recent study from Congo and Madagascar reported sustained improvements in knowledge and skills at four and 12–18 months, and personal and organisational changes in practice. 20 In particular, participants reported improvements in neonatal resuscitation and airway management at four months, and management of emergencies, systematic ‘Airway, Breathing, Circulation’ (ABC) approach, and spinal anaesthesia at 12–18 months. In our study, participants reported fewer specific behavioural changes and focused more on feelings of improved confidence and motivation. These findings could fit with the reports from Ethiopia of low morale, poor job satisfaction 17 and providers feeling marginalised and excluded. 18
The three-day SAFE Paediatric course has also been demonstrated to lead to improved, and retained, knowledge and skills, following courses in Ethiopia, Kenya, Uganda, Zambia and Malawi, 21 , 22 with reported improvements in confidence, 21 and improved communication and positive behavioural changes. 22
Studies of other short courses run in LMICs also demonstrate benefits. A study of Primary Trauma Care (PTC) courses in East, Central and Southern Africa showed self-reported changes in practice at six months as well as effects on host institutions’ staffing, equipment and training. 23 A study of Lifebox one-day pulse oximetry training in Malawi led to improved knowledge, which was maintained for eight months. Pulse oximeters were distributed at the time of the training and the study found a reduced incidence of hypoxic events at follow-up. 24
The strengths of our study included inclusion of participants from a broad range of facilities and a mixed methods approach to follow-up. The faculty included Ethiopian trainers with local faculty members conducting skills tests and follow-up interviews to prevent miscommunication due to language barriers, impact on test scores, or translational difficulties during interviews. We recognise there are several limitations to this study. There was incomplete follow-up as some participants did not have email, and telephone communication was difficult with network problems and ineligible and incorrect phone numbers on record. Transportation of personnel and equipment to rural hospitals to conduct follow-up was difficult, and time constraints were a problem when trying to arrange follow-up around working patterns. Variation in the timing of follow-up between participants could mean an unmeasured difference between these participants.
Self-reporting is limited by the degree of honesty in responses. Interview responses could have been biased by a desire to please the interviewer or fear of consequences. Behavioural questionnaires would ideally be repeated at follow-up with direct observations to identify actual behaviours, and also to investigate any barriers to achieving these, such as shortage of resources or behaviours of other team members. We did not assess whether there were differences in impact between PAPs and NPAPs. The focus for training was in regions without PAPs, and due to the small number of PAPs attending the courses a valid comparison could not be made.
Although our study shows knowledge and skills are maintained at 3–11 months post-training, it is difficult to determine whether the improved knowledge and skills translates into improved clinical practice, or indeed to other environments. In particular, it is difficult to assess whether this type of training leads to a reduction in morbidity and mortality; this would require comprehensive surveillance of cases and root cause analysis. As highlighted in our study, there were reported difficulties with improving clinical care due to availability of resources and this reinforces that improving education is only one component of the wider system change.
It is important to consider both the impact and also the sustainability of the educational model. Burton et al. report that instilling local ownership was fundamental to implementing change in the local safety culture, when describing their programme of utilising visiting UK volunteers to help establish a postgraduate training programme at Jimma University Medical College in Ethiopia. 25 The SAFE-OB courses described in our study were run in collaboration with the Federal Ministry of Health of Ethiopia, the Ethiopian Society of Anaesthesiologists (ESA) and the Ethiopian Association of Anaesthetists (EAA) as part of the National Safe Surgery 2020 initiative. Courses have since been run independently by these organisations in Ethiopia, with local ownership driven by these national bodies.
A further aid to sustainability is through the incorporation of ‘Training of Trainers’ courses alongside the SAFE-OB courses. This enables a cohort of participants to become the in-country faculty of the future, thus reducing the need to rely on international faculty for course delivery. This programme of courses incorporated four one-day ‘Training of Trainers’ courses that trained 56 local trainers.
As the SAFE initiative expands, further models of training and methods to improve sustainability are being developed. SAFE-OB refreshers have recently been piloted in a neighbouring country (Tanzania). The modular nature of the course also enables course components to be incorporated into national anaesthesia curricula or other training programmes and this is also being piloted in neighbouring countries. This could also provide a cost-effective alternative where funding is limited, as well as broadening the numbers of providers trained.
It is also important to consider the context in which the course will be delivered. This is particularly relevant given that a main barrier to change appeared to be limited resources. Work is underway to adapt the SAFE-OB course to different provider groups, and for different settings, thus creating regional or country specific adaptations to the standard course.
In conclusion, our study provides evidence that the SAFE-OB course can have a positive short-term educational impact in a low-resource setting. Our article relates only to Ethiopia yet adds to a growing evidence base to support the SAFE-OB course in a variety of contexts. Further work will be required to assess the impact of SAFE-OB training in other countries and to establish its impact on clinical practice and patient outcomes. Work is ongoing to develop the SAFE-OB course for use in different contexts and to improve long-term sustainability.
Footnotes
Author contribution(s)
Acknowledgements
The authors wish to thank the following people:
Dr Mahder Kinfe and Dr Tirunesh Busha, for assistance with follow-up data collection. Dr Victoria White, for assistance with behavioural questionnaire data analysis. The Amhara and Tigray Regional Health Bureaus, Ethiopian Society of Anaesthesiologists, Ethiopian Association of Anaesthetists, the Federal Ministry of Health of Ethiopia and Assist International for their support with running the SAFE-OB courses.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors have roles within the WFSA and AAGBI Foundation, the organisations responsible for developing the SAFE Obstetric Anaesthesia course (JM: WFSA (UK) Trustee; WM: WFSA Director of Programmes; AA: Previously WFSA Head of Programmes; IW: AAGBI Foundation Trustee).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The SAFE courses and follow-up evaluation in this study were funded by GE Foundation.