
Abstract
We conducted a survey of Australian and New Zealand anaesthetists designed to quantify self-reported use of cricoid pressure (CP) in patients presumed to be at risk of gastric regurgitation, and to ascertain the underlying justifications used to support individual practice. We aimed to identify the perceived benefits and harms associated with the use of CP and to explore the potential impact of medicolegal concerns on clinical decision-making. We also sought to ascertain the views of Australian and New Zealand anaesthetists on whether recommendations relating to CP should be included in airway management guidelines. We designed an electronic survey comprised of 15 questions that was emailed to 981 randomly selected Fellows of the Australian and New Zealand College of Anaesthetists (ANZCA) by the ANZCA Clinical Trials Network on behalf of the investigators. We received responses from 348 invitees (response rate 35.5%). Of the 348 respondents, 267 (76.9%) indicated that they would routinely use CP for patients determined to be at increased risk of gastric regurgitation. When asked whether participants believed the use of CP reduces the risk of gastric regurgitation, 39.8% indicated yes, 23.8% believed no and 36.3% were unsure. Of the respondents who indicated that they routinely performed CP, 159/267 (60%) indicated that concerns over the potential medicolegal consequences of omitting CP in a patient who subsequently aspirates was one of the main reasons for using CP. The majority (224/337; 66%) of respondents believed that recommendations about the use of CP in airway management guidelines should include individual practitioner judgement, while only 55/337 (16%) respondents believed that routine CP should be advocated in contemporary emergency airway management guidelines.
Keywords
Introduction
Gastric regurgitation (GR) and subsequent pulmonary aspiration (PA) in patients under general anaesthesia (GA) has been identified as a significant source of patient morbidity.1 Although numerous techniques have been employed to reduce the incidence of PA, high-level evidence to support these interventions is lacking. Cricoid pressure (CP) has historically been described as standard care to reduce GR during rapid sequence induction (RSI). Research into the efficacy of CP is hampered by the large sample sizes required, given the rarity of clinically significant pulmonary aspiration, or other patient-oriented surrogate endpoints such as visible gastric contents in the hypopharynx, observation of anatomical occlusion of the oesophagus and micro-aspiration assessed radiologically or biochemically.2–4 This was demonstrated in a recent 3472-participant prospective randomised study, which failed to show non-inferiority of a sham cricoid procedure compared with CP.5 An international effort with a global database has been proposed to capture more information into the practice and prevention of clinically significant pulmonary aspiration.6 However, to date, there is no high-quality controlled trial evidence demonstrating that the use of CP results in a clinically significant reduction in pulmonary aspiration.7
Conversely, it is known that CP is often taught ad hoc and that correct and consistent application is not universal.8–13 Although the risk of serious harm resulting from the application of CP is likely to be low, the potential for increased difficulty of laryngoscopy and increased time to intubation has been recognised among a range of potential complications.5,14–16
The disputed efficacy and inconsistent recommendations for the routine use of CP in patients determined to be at increased risk of GR has generated significant controversy in contemporary anaesthesia practice, and there is a lack of consistency regarding the use of CP during RSI in international guidelines.9,17–21 The Difficult Airway Society guidelines for emergency management of unanticipated difficult intubation advocate for the routine use of CP, with the recommendation to release CP if initial attempts at laryngoscopy are difficult during RSI.22 This contrasts with other contemporary guidelines, for example the Scandinavian clinical practice guidelines on general anaesthesia for emergency situations, which assert that the use of CP to reduce GR cannot be recommended on the basis of scientific evidence, and that while anaesthesiologists may use CP on individual judgement, they must be ready to release CP if necessary to optimise the glottic view on laryngoscopy.14,23–25
The views of Australian and New Zealand specialist anaesthetists regarding the effectiveness of CP have not previously been quantified. We have therefore undertaken a survey of anaesthesia specialists registered with the Australian and New Zealand College of Anaesthetists to quantify self-reported practice and attitudes towards the use of CP for the prevention of GR and PA during RSI and in patients at increased risk of GR, and to explore the potential impact of medicolegal concerns on clinical decision-making with regard to the use of CP.
Methods
Ethical approval for the study was obtained from the Victoria University of Wellington Human Ethics Committee (000002734). Subsequent approval was obtained under the Australian and New Zealand College of Anaesthetists (ANZCA) Clinical Trials Network (CTN) survey research policy to conduct and distribute this survey. The survey interface was designed using the SurveyMonkey online platform. The survey consisted of four demographic and professional classification questions, including whether participants identified as paediatric anaesthetists. Respondents were asked to indicate whether they identified as paediatric subspecialists or having a special interest in paediatrics in order to determine whether specific recommendations for the use of CP in paediatric practice affected its use in adults amongst those respondents. There were a further 11 questions addressing practice patterns and perceptions of participants relating to the use of CP, including specific questions relating to the impact of medicolegal concerns on practice. All questions were multiple-choice style, with the ability to choose either only one answer or multiple answers, as appropriate for the question, with space for optional free-text responses (see Appendix 1). Survey questions were prepared by the study authors to answer the specific questions outlined in the study aims, and underwent peer review by the Wellington Department of Anaesthesia and Pain Medicine Research Committee and subsequently the ANZCA CTN survey research review process, which involved a process of independent review by an anonymous anaesthetist with no involvement in this research.
The survey was distributed via email to a randomly selected sample of 1000 of the 5557 ANZCA Fellows practising in anaesthesia or pain medicine in Australia or New Zealand at the date of distribution. Random sampling was achieved by running a randomisation script through the ANZCA database. This is the current standard maximum sample size for ANZCA CTN--facilitated surveys. Sample size calculations were not performed. Participants were contacted by email during June 2019, with a web link to the online survey. A subsequent email was sent after two weeks to encourage maximal response rate. The survey was closed four weeks after the first invitation to participate. All data were collected anonymously; no internet protocol addresses or any other potentially identifying metadata were collected. The ANZCA CTN provided a summary of demographic data for all current Fellows at the time the survey invitation was sent in order to enable a qualitative demographic comparison between survey respondents and ANZCA specialists overall. Data were analysed using Microsoft Excel 2016 (Microsoft Corp., Redmond, WA, USA). Mean and standard deviation (SD) were calculated for survey responses where appropriate. There was no imputation of missing data. The survey is reported in accordance with published guidelines on survey research.26,27
Results
Demographics
The survey was successfully distributed to 981 of the 1000 randomly selected anaesthetists registered with ANZCA. There were 348 (35.5%) responses, with participation similar to the population of ANZCA Fellows in each jurisdiction. Demographics of survey respondents and ANZCA Fellows overall are summarised in Table 1. Baseline characteristics were similar across geographical location and number of years in specialist practice. The majority of survey respondents’ primary place and type of work was clinical work in a tertiary public hospital.
Demographics of survey respondents and Australian and New Zealand College of Anaesthetists Fellows overall.
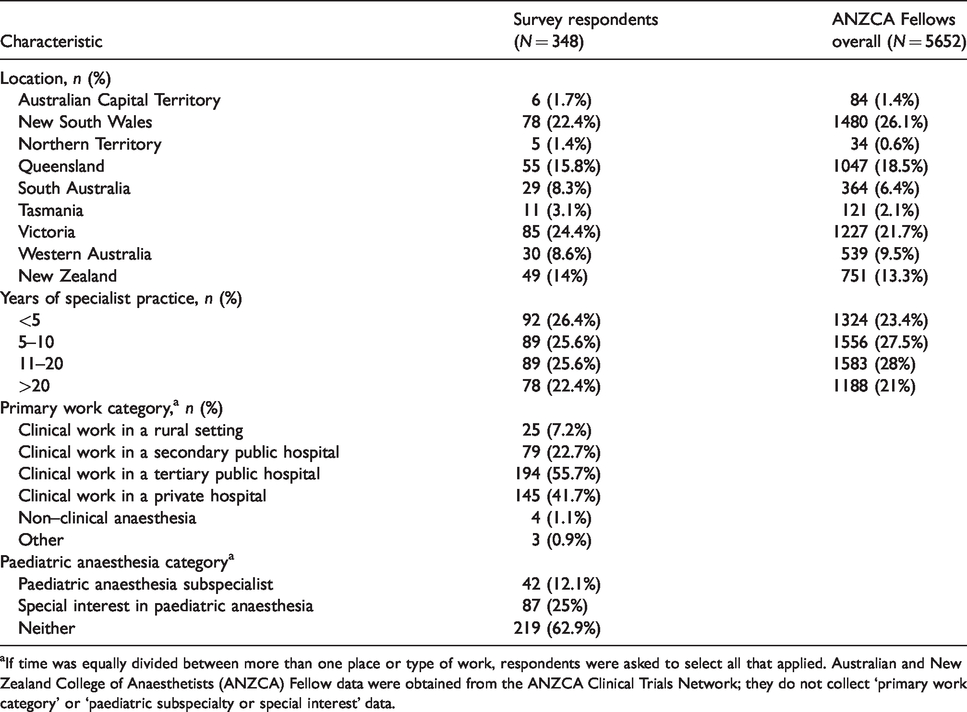
aIf time was equally divided between more than one place or type of work, respondents were asked to select all that applied. Australian and New Zealand College of Anaesthetists (ANZCA) Fellow data were obtained from the ANZCA Clinical Trials Network; they do not collect ‘primary work category’ or ‘paediatric subspecialty or special interest’ data.
Practice patterns
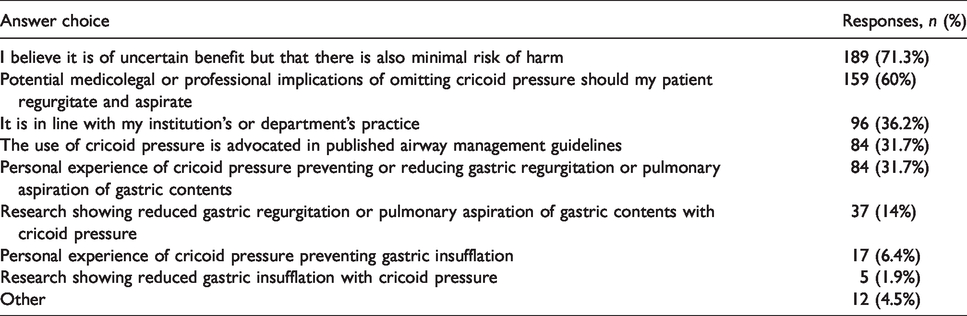
Of the 348 survey respondents, 267 (77%) indicated that they routinely use CP prior to tracheal intubation in a patient who the respondent perceives to be at increased risk of GR or in whom they have decided that RSI or modified RSI is indicated. Underlying reasons selected for those who routinely utilise CP as part of RSI are shown in Table 2.
Reasons cited by respondents for the routine use of cricoid pressure (in the subset who routinely use cricoid pressure).
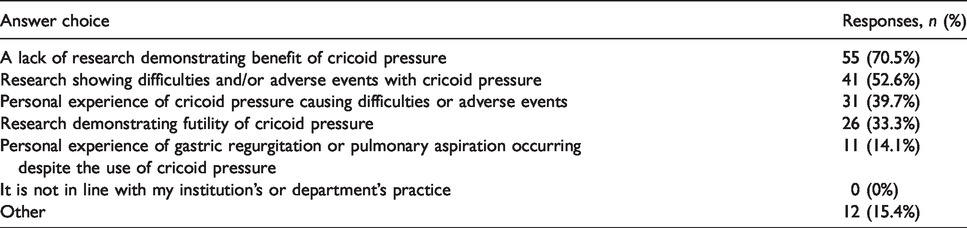
The underlying reasons selected by those who do not routinely use CP as part of the RSI technique are displayed in Table 3.
Reasons cited by respondents for not using cricoid pressure (in the subset who do not routinely use cricoid pressure).
Perceived efficacy and harms of cricoid pressure
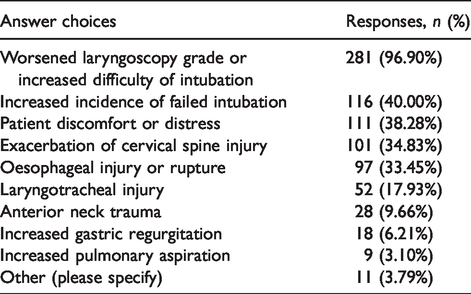
When respondents were asked whether they believe that the use of CP reduces the risk of gastric regurgitation, 39.8% indicated they believed that it does, 23.8% believed it does not and 36.3% were unsure. Similar responses were obtained when asked whether CP reduces the risk of clinically significant pulmonary aspiration; 40.7% agreed, 23.6% disagreed and 35.8% were unsure. Conversely, 86.3% of respondents thought that CP can result in difficulties or adverse events. The types of harm resulting from CP that were selected by respondents are shown in Table 4.
Concerns selected by respondents related to using cricoid pressure.
When asked to consider the overall potential benefit and harm of CP, 16.3% thought that it is much more likely to confer benefit than result in adverse conditions or harm, 45.4% thought that it is modestly more likely to confer benefit than harm, 19.9% thought it is equally likely to confer benefit or harm, while 18.4% thought it was modestly or much more likely to result in harm than benefit.
Medicolegal concerns
The distribution of responses when respondents were asked to indicate if and how strongly they agreed or disagreed that medicolegal concerns had a greater influence on their practice than their interpretation of the available evidence regarding the benefits and harms of CP is displayed in Figure 1. A higher proportion of responders who indicated that they routinely perform CP agreed or strongly agreed that they were concerned with potential medicolegal concerns of omitting cricoid (49%) than those who indicated that they do not routinely perform CP (21%).
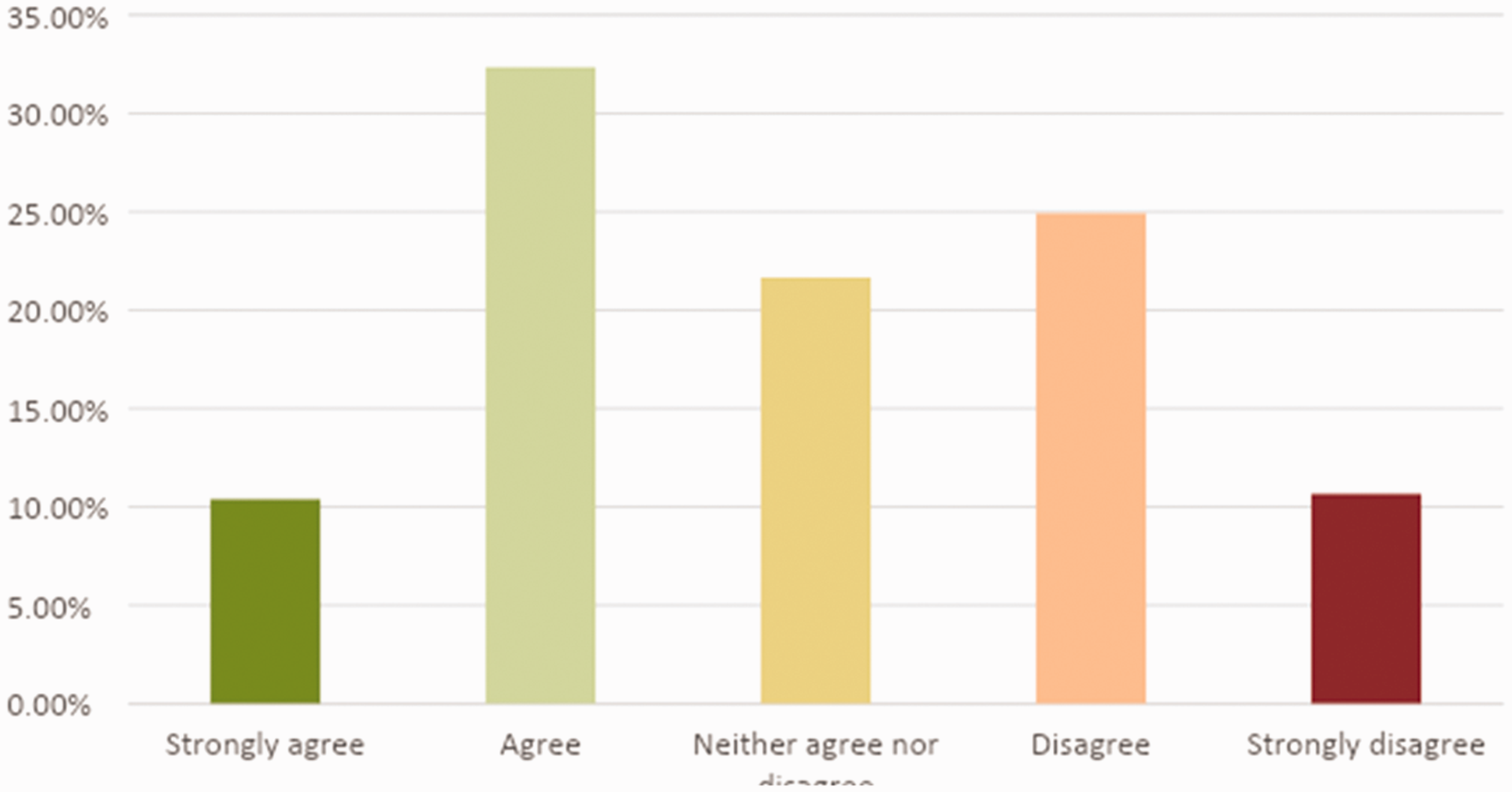
Indicate whether you agree or disagree with the following statement: ‘The possible medicolegal or professional consequences of omitting cricoid pressure in the event of pulmonary aspiration influences my practice more than my interpretation of the available evidence’.
Emergency airway management guidelines
When asked about the inclusion of CP recommendations in contemporary emergency airway management guidelines, 66.5% (n = 224) of respondents thought that guidelines should encourage individual clinician judgement about use of CP. A further 7% (n = 24) thought CP should be discouraged, and 6.2% (n = 21) thought that guidelines should omit any recommendations on the use of CP. Conversely, 3.9% (n = 13) thought that guidelines should strongly advocate for the routine use of CP, and 16.3% (n = 55) thought that CP should be encouraged in emergency airway management guidelines.
Paediatric subspecialists
A similar proportion of paediatric subspecialists (32/42; 76%), respondents with a special interest in paediatric anaesthesia (65/87; 75%) and respondents who were neither subspecialists nor special interest paediatric subspecialists (170/219; 78%) indicated they would routinely use CP for patients considered to be at increased risk of GR.
Discussion
The majority of respondents to our survey of ANZCA registered specialists reported routinely performing CP in patients with an increased risk of GR or in whom they have decided that RSI is indicated. The majority also believed there is likely to be more benefit than harm resulting from CP use during RSI. Whilst medicolegal concerns were identified as one of the main reasons for performing CP by the majority of respondents, attitudes about the relative risks and benefits of the inclusion of CP as part of the RSI technique varied widely. Similar response rates were obtained from respondents identifying as paediatric versus non-paediatric anaesthetists with respect to their adult anaesthesia practice.
Comparison with previous studies
The prevalence of self-reported CP use amongst the respondents is similar to a recently published large international survey of anaesthetists and airway experts from other jurisdictions which reported that CP would be used by 71% and 50% of anaesthetists for a hypothetical patient with and without intestinal obstruction, respectively.28 The use of CP in Europe was reported in a survey of trauma instructors, noting that overall use was lower than our study (50%), though use in the UK was similar to our findings (83%) in comparison with the rest of Europe with the UK excluded (39%).29 The frequent use of CP in anaesthesia in the UK has been previously noted in a survey of National Health Service anaesthesia trainees and consultants (92%) and in a survey comparing UK (96%) to Swiss and Austrian practice (52%).30,31 In contrast to previous surveys, the present survey did not describe a hypothetical patient on which to base responses, but instead was intentionally ambiguous about the indications for RSI by asking the respondent about their view on the inclusion of CP in a scenario where they had determined that the patient was at increased risk of GR or that RSI was indicated. This approach was chosen in order to avoid responder uncertainty about the indications for RSI. However, the authors acknowledge that due to this intentional ambiguity, the influence of the perceived degree of risk in different clinical scenarios on individual responses cannot be assessed.
There was strong representation of views from survey respondents who thought that CP is effective for reducing GR and PA, those who thought it is not effective and those who were unsure. It is probable that the variation in views reflects the absence of high-level patient-centred evidence to either support or discourage the use of CP. In addition, individual clinician experience of PA events and local departmental practice and teaching may impact beliefs on the effectiveness of CP.
While almost all respondents believed that CP could result in adverse conditions or harm, overall more respondents thought there was likely to be more benefit than harm from the use of CP during RSI. There are a number of potential explanations for this finding. First, it is possible that respondents thought that although a wide range of harms are possible, these are unlikely to occur, or are less likely to cause more serious morbidity than PA. Furthermore, as stated in the Difficult Airway Society guidelines, increased difficulty in laryngoscopy may be able to be resolved by removing CP. Respondents were not asked to indicate how likely or harmful they thought each potential complication of CP could be. Second, given the prevalence of the concern from respondents about negative medicolegal repercussions from omitting CP, the authors speculate that participants may have considered their professional self-interest in pursuing medicolegally defensive practice amongst the ‘benefits’ of performing CP.
Previous studies have also suggested that the popularity of CP may reflect the potential legal repercussions of avoiding CP use in patients with an elevated risk of PA.28 However, the present survey is the first to document that potential medicolegal implications are identified as a reason for the use of CP in contemporary anaesthesia practice by the majority of respondents.
Most survey respondents expressed a view that airway management guidelines should encourage clinicians to exercise individual judgement about the use and utility of CP, which it could be speculated may reflect an awareness among respondents of the lack of evidence supporting the use of CP for reducing GR and PA. Nonetheless, the inclusion of CP in published airway management guidelines is likely to be an important factor in determining clinicians’ practice.
Clinical implications
The findings of this study suggest that the majority of respondents report performing CP in patients perceived to be at increased risk of GR and believe that the potential benefits outweigh the potential harms. However, the majority also believe that airway management guidelines should encourage individual clinical judgement about the inclusion of CP in patients who are perceived to be at increased risk of GR and in whom RSI is thought to be indicated. Clinicians may wish to have the freedom to use CP selectively for a particularly high-risk situation, use cricoid routinely for all RSI patients or omit the use of CP altogether, whilst maintaining other components of the RSI technique. Many survey respondents indicated that one of the main reasons for their practice of CP is concern about potential medicolegal or professional implications should their patient regurgitate or aspirate, despite a belief held by the majority that CP is either ineffective or of uncertain benefit for reducing PA in at risk patients (Tables 2 and 3). Despite the finding that the majority of respondents believed that CP is ineffective or of uncertain benefit for reducing PA, the majority felt that overall CP is more likely to provide net benefit than harm.
Strengths and weaknesses
Our survey was distributed to a randomly generated representative sample of anaesthetists in Australia and New Zealand. Although the study achieved a survey response rate consistent with previous ANZCA-facilitated surveys,32–34 and a high survey completion rate, there remains a risk of responder bias, with those invitees who possessed a particular view either in favour of or in opposition to CP possibly being more or less likely to participate. In addition, questions relating to practice by their nature relied on self-reporting, which is prone to response bias and may not accurately reflect practice.
We acknowledge that the medicolegal climates of Australia and New Zealand are not the same (with New Zealand clinicians protected by the state-provided no-fault accident cover by the Accident Compensation Corporation). However, in order to protect anonymity, we did not distinguish views from separate jurisdictions.
Given the limitations on the maximum number of ANZCA Fellows able to be surveyed through the ANZCA CTN survey process, we accept that the sample size representing just over 6% of the population of anaesthetists in Australia and New Zealand is vulnerable to selection bias. However, comparisons of demographic data between survey respondents and Fellows overall would support the notion that this survey achieved a relatively representative sample of anaesthetists.
Amongst patients determined to be at risk of GR, there is a spectrum of illness severity, between which this survey did not differentiate in order to minimise survey fatigue and to maximise response rate. As already outlined, this was a deliberate survey design choice to avoid confusion between the question of determining the indications for RSI and determining the utility of CP as a part of an RSI technique, only the latter of which was the purpose of the present study.
Conclusion
The findings of this study suggest that the majority of Australia and New Zealand specialist anaesthetist survey respondents use CP when performing intubation in patients considered to be at increased risk of GR, or in whom they believe RSI is indicated. The two reasons most commonly selected by study respondents were the belief that CP is of uncertain benefit but there is also minimal risk of harm, and concerns about medicolegal or professional implications of omitting CP should a patient regurgitate or aspirate.
Most respondents in this survey thought that contemporary emergency airway guidelines should recommend that clinicians exercise individual judgement about the use of CP with RSI, rather than encourage or discourage the use of CP as a routine component of RSI. This may indicate that existing guidelines on airway management may benefit from an update and a reappraisal of the evidence supporting routine CP use in patients considered at risk of GR.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X20968841 - Supplemental material for A survey of self-reported use of cricoid pressure amongst Australian and New Zealand anaesthetists: Attitudes and practice
Supplemental material, sj-pdf-1-aic-10.1177_0310057X20968841 for A survey of self-reported use of cricoid pressure amongst Australian and New Zealand anaesthetists: Attitudes and practice by Ravi Mistry Conceptualization Formal analysis Investigation Methodology Writing original draft Writing review editing Daniel R Frei Conceptualization Formal analysis Investigation Methodology Writing original draft Writing review editing ChrisBadenhorst Formal analysis Investigation Methodology Writing original draft Writing review editing James Broadbent Formal analysis Methodology Writing review editing in Anaesthesia and Intensive Care
Footnotes
Acknowledgements
We wish to thank the Australian and New Zealand College of Anaesthetists Clinical Trials Network for providing peer review and facilitating distribution of this survey.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.