
Abstract
Background:
Alongside physical impairment, psychosocial health issues may arise after amputation, impacting quality of life. Traditional psychosocial care models provide services in a linear fashion, with limited supports upon discharge. A novel program entitled Amputees Unanimous is a 12-step program provided for amputees by amputees.
Objective:
To shape the final content of Amputees Unanimous by identifying personal beliefs and opinions of healthcare professionals and amputees.
Study Design:
Qualitative design utilizing a phenomenological approach.
Method:
Five focus groups were held: four with amputees and one with healthcare providers. A phenomenological approach shaped the inquiry of the lived experience of limb loss in relation to the content of Amputees Unanimous.
Results:
Three themes emerged: (1) accepting limb loss, (2) peer inspiration, and (3) regaining prior level of function.
Conclusion:
Limb loss may alter one’s self-image, both physically and psychologically, having a profound effect on how an individual copes throughout his or her lifetime. The content and delivery format of Amputees Unanimous could be tested for effectiveness as a program tailored to facilitate coping after limb loss and to provide encouragement, support, and hope for the future of amputees.
Clinical relevance
A dynamic, amputee-led, mutual help program may provide individuals with limb loss a place for encouragement, support, and optimism for the future.
Background
An estimated 1.6 million Americans are living with limb loss. 1 Trauma is the leading cause of limb amputation globally. 2 Approximately 2% of combat causalities sustain limb amputation, 3 with battle-related explosive events accounting for 93%. 4
Psychosocial health issues may arise after amputation, impacting quality of life. The Amputee Coalition of America 5 surveyed 954 amputees and 30% (286) reported a depressed mood, half of whom were not receiving behavioral health services. Obstacles cited involved financial burden and being uninformed on available services. 5 A study comparing combat amputees to individuals with extremity injury found those with limb loss were more likely to have a mental health diagnosis consisting of nonorganic sleep disorders, pain disorders, and post-concussion syndrome. 6
Distinct features have been correlated with poor adaptation to amputation. For example, female amputees reportedly experience more distress 7 and negative associations with body image anxiety. 8 Younger amputees demonstrated increased levels of post-traumatic stress disorder and depressive symptoms, 7 which correlated with poor adjustment to a prosthesis and restriction of activities. 8 Upper limb amputees experienced increased rates of depression, anxiety, adjustment to a prosthesis, activity restriction, and body image anxiety. If an individuals’ dominant hand was affected, these rates increased, further impairing social interactions and functioning. 8 One study reported those who required late amputation after failed limb-salvage attempts experienced significantly worse emotional well-being and body image concerns. 9 Individuals who sustained limb loss from complications related to diabetes expressed “feelings of helplessness,” with reported lack of knowledge provided by healthcare professionals on their condition and associated risks. 10
Conversely, protective factors for adjustment and coping after limb loss include a positive attitude, social support, problem-solving abilities, personal courage, humor, and meaning making.11–13 Social support acts as a “buffer” toward psychological distress, decreasing the patient’s likelihood for social isolation, depression, and anxiety. 12 Peers who have experienced the loss of a limb are considered to be the strongest source of encouragement,2,14–17 a benefit deemed greater than advice provided by physicians. 18
Psychosocial supports for amputees typically exist in a traditional provider–patient educational format, commonly with a provider who has never personally experienced limb loss. In this classic teacher-student role, participants are passive beneficiaries asked to follow a structured, linear path for recovery. Given that peer support from fellow amputees and time since amputation 18 are factors in adjustment and acceptance, a dynamic, amputee-led program could positively impact recovery after amputation.
12-step program
One example of a dynamic, participant-led program is Alcoholics Anonymous (AA). No similarity is implied between an alcoholic and amputee; rather, the participant-led approach used in AA is explored in how it may benefit adults coping with limb loss. Group involvement is voluntary and members delineate when, where, and how often they attend. It is a mutual-help association following a 12-step model for recovery. Members “work” the 12 steps, practicing tools for recovery and taking control of their actions. 19 As a dynamic model, the design allows for members to move forwards, backwards, and progress at a personal pace, ultimately reaching the 12 step of “service to others.”
AA membership is estimated at over two million across 180 countries, 19 with the fourth edition of “Alcoholics Anonymous” having been translated into 69 languages. 20 Researchers continue to explore the effectiveness of the program’s participant-led 12-step model compared with standard psychosocial treatment methods. Expansion of the AA model within other disorders (e.g. narcotics anonymous, gamblers anonymous, food addicts anonymous, etc.) demonstrates the unique support possible for individuals, by individuals coping with the same experience. One group yet to be aided through a participant-led 12-step model is amputees.
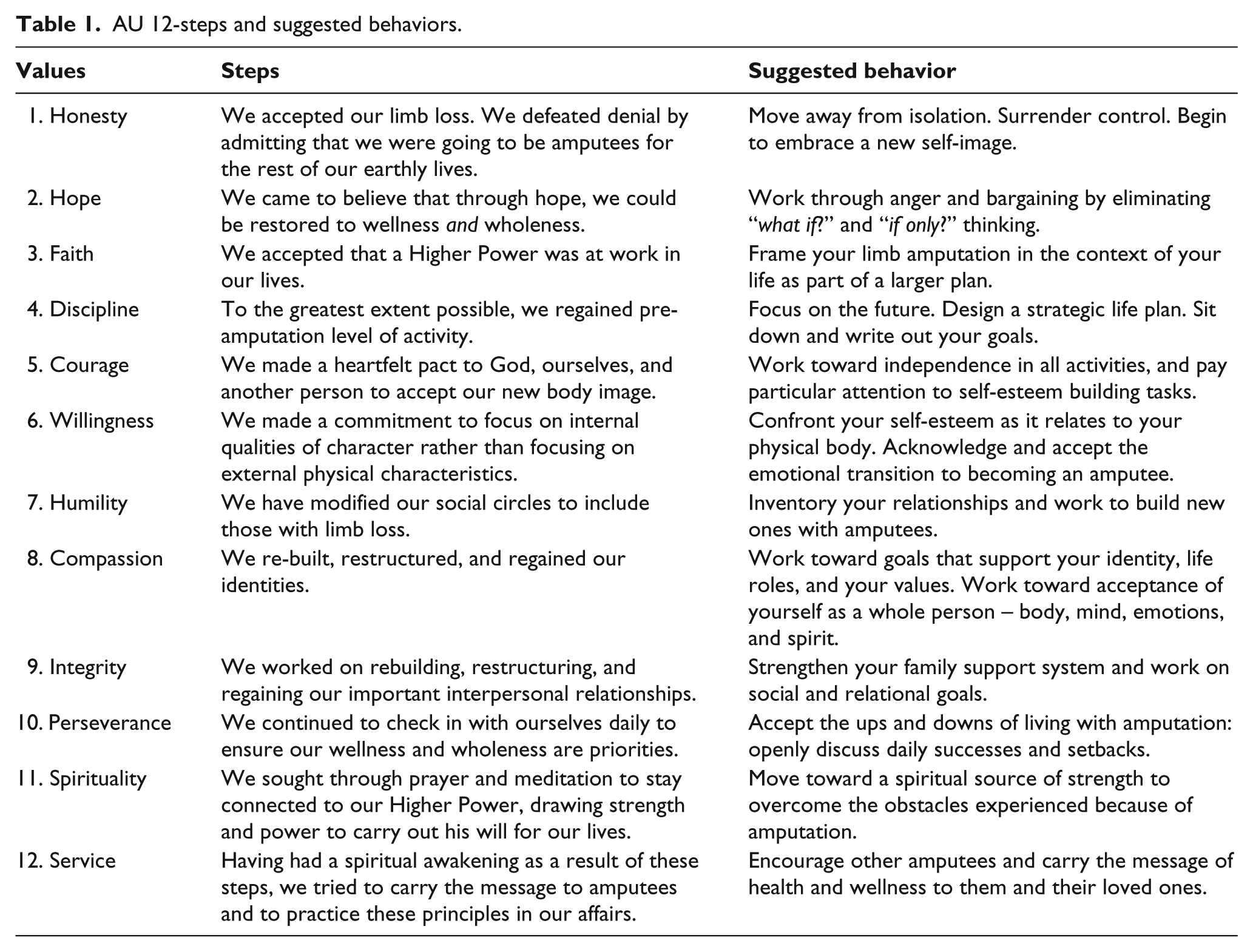
Amputees Unanimous
A recovery program entitled Amputees Unanimous (AU) was developed by Kathleen Yancosek, PhD, Occupational Therapist Registered/Licensed (OTR/L), Certified Hand Therapist (CHT) to facilitate coping with limb loss for the general, adult amputee population regardless of mechanism of injury or military affiliation. The program is based on the model and structure of AA, modified to address the particular needs of the amputee population. The 12-steps of AU progress from accepting and embracing a new self-image to providing encouragement and service to fellow amputees throughout the recovery process. Each step is supplemented with a “suggested behavior” to further elaborate what individuals may experience (see Table 1). AU is a dynamic program allowing for personal advancement and re-examination of prior steps, as necessary. It is a 12-step program led by amputees, to the benefit of amputees, with the primary purpose of helping those still in need, conveying the message of acceptance, courage, and service to others. Due to the program’s purpose of being for amputees by amputees, it was essential that the proposed 12-steps be evaluated by a subset of the amputee population to explore the value of such a novel program. The aims of this study were to (1) examine the content of the AU program by adults who have lived through the experience of recovery after limb loss, (2) examine the content of the AU program by healthcare professionals experienced in amputee rehabilitation, and (3) discover beliefs, opinions, and attitudes regarding AU’s value for the limb loss community. This research will inform the final content and future clinical research to examine the effectiveness of AU in the community.
AU 12-steps and suggested behaviors.
Methods
Study design
A qualitative design utilizing a phenomenological approach was used to understand participants’ beliefs and attitudes toward AU. In phenomenology, participants are believed to be the most knowledgeable on the delineated topic and are asked to describe their personal involvement with the phenomena. 21 Focus groups gather in-depth knowledge of individuals’ personal beliefs relating to a shared common experience. 22 In this study, four focus groups were held with amputees and one with healthcare providers experienced in amputee care. Group discussions averaged 70 min, and in-depth knowledge was gained through semi-structured interviews. Permission to audio tape discussions was provided by all participants.
Participants
Ethical approval to conduct the study was obtained through the local institutional review board. Informed written consent and Health Insurance Portability and Accountability Act (HIPAA) forms were completed prior to focus group engagement. Participants were selected through purposeful sampling. Inclusion criteria included the following: (1) military service members, beneficiaries, veterans, or local, non-military citizens who gained proper military approval to receive care at the local hospital and/or affiliated amputee rehabilitation center, or healthcare professionals experienced in amputee care; (2) 18 years of age or older; (3) sustained major limb amputation(s) (defined as “amputation proximal to the carpals or tarsals of a limb” 4 ); (4) fluent in English to be able to understand instructions, provide informed consent, and engage in focus group discussion; and (5) willing to participate in a focus group discussion with subsequent survey on a designated day and time for an estimated 2 hrs. Participants actively attending a support group for psychological relief for issues related to amputation were excluded. Participants were placed in one of five focus groups: (1) upper extremity amputees, (2) lower extremity amputees, (3) trauma-related amputation, (4) illness-related amputation, or (5) healthcare professionals experienced in amputee care.
Focus group procedure
Focus groups were held in a private conference room. For confidentiality and anonymity, nameplates with pseudonyms were positioned in front of each participant. A brief overview of AU was provided at the beginning of each focus group. For the four amputee focus groups, a mock AU meeting was conducted during the first half to provide an understanding of how the 12-step program would be conducted. Amputee participants shared personal experiences with a selected step and/or suggested behavior. Upon completion of the mock AU group, a 10-min break ensued, followed by the associate investigator (second author (K.Y.)) asking open-ended questions on opinions and beliefs regarding the value, structure, and content of AU in relation to limb loss. A “moderators guide” developed by the primary investigator (first author (C.A.)) was utilized. Amputee focus groups concluded with completion of a study-specific survey to gather additional descriptive statistics. The healthcare provider focus group began with an educational overview of the AU program, followed by open-ended questions to capture opinions regarding the value of AU. Immediately after each focus group, the primary and associate investigators discussed observations, participant interactions, overall group experience, and potential themes while maintaining objectivity through reflexivity. All avenues of interpretation of focus group content was explored, supplementing data analysis through audio recordings.
Data analysis
Data from audio recordings were transcribed and coded utilizing NVivo 11 software (NVivo 11 for Windows, QSR International, Version 11.1.0.411, Burlington, MA). Data were analyzed through Colaizzi’s phenomenological method. Significant statements were identified and coded throughout transcriptions, with subsequent reduction into formulated meanings, theme clusters, and finally emergent themes. 23 Following identification of themes by C.A. and K.Y., the last author independently reviewed the analysis and validated the themes. Member checking was performed through follow-up conversations (phone or in person) with 23/27 participants. Four were lost to follow-up. Data from the study-specific survey were entered into a Microsoft Excel (Microsoft Office 365, Redmond, WA) spreadsheet and descriptive statistics calculated.
Results
Of the 45 eligible people invited to the study, 27 participated. Our 10 were healthcare professionals with 126 years of combined amputee care experience. Professionals were occupational therapists, physical therapists, social workers, physicians, and orthotists and prosthetists who worked at the amputee rehabilitation center. Of the participants with limb amputation, 11 had unilateral lower-extremity amputations, four had unilateral upper-extremity amputations, one had bilateral lower-extremity amputations, and one had amputation of all limbs (see Table 2). The majority of amputee participants were male (88%) and had lived with limb loss for over 3 years (41%). Accidents and combat-related events were the leading cause of amputation. Prior experience with support groups either in relation to limb loss or another condition was reported by 71% of amputee participants; however, only 12% had experienced a 12-step program. All amputee participants reported experience with at least one AU step, with an average of 7.6 steps encountered throughout recovery. When reviewing steps individually, 76% of participants reported personal experience with steps one, six, eight, and ten. Participant feedback regarding the program’s structure and utility centered around (1) removing language in suggested behavior number one: “surrendering control,” (2) modifying spiritually content throughout, and (3) recognizing the need for AU within the limb loss community. A complete list of recommendations and feedback provided by participants on the AU program is recorded in Table 3.
Demographics of participants with limb amputation.
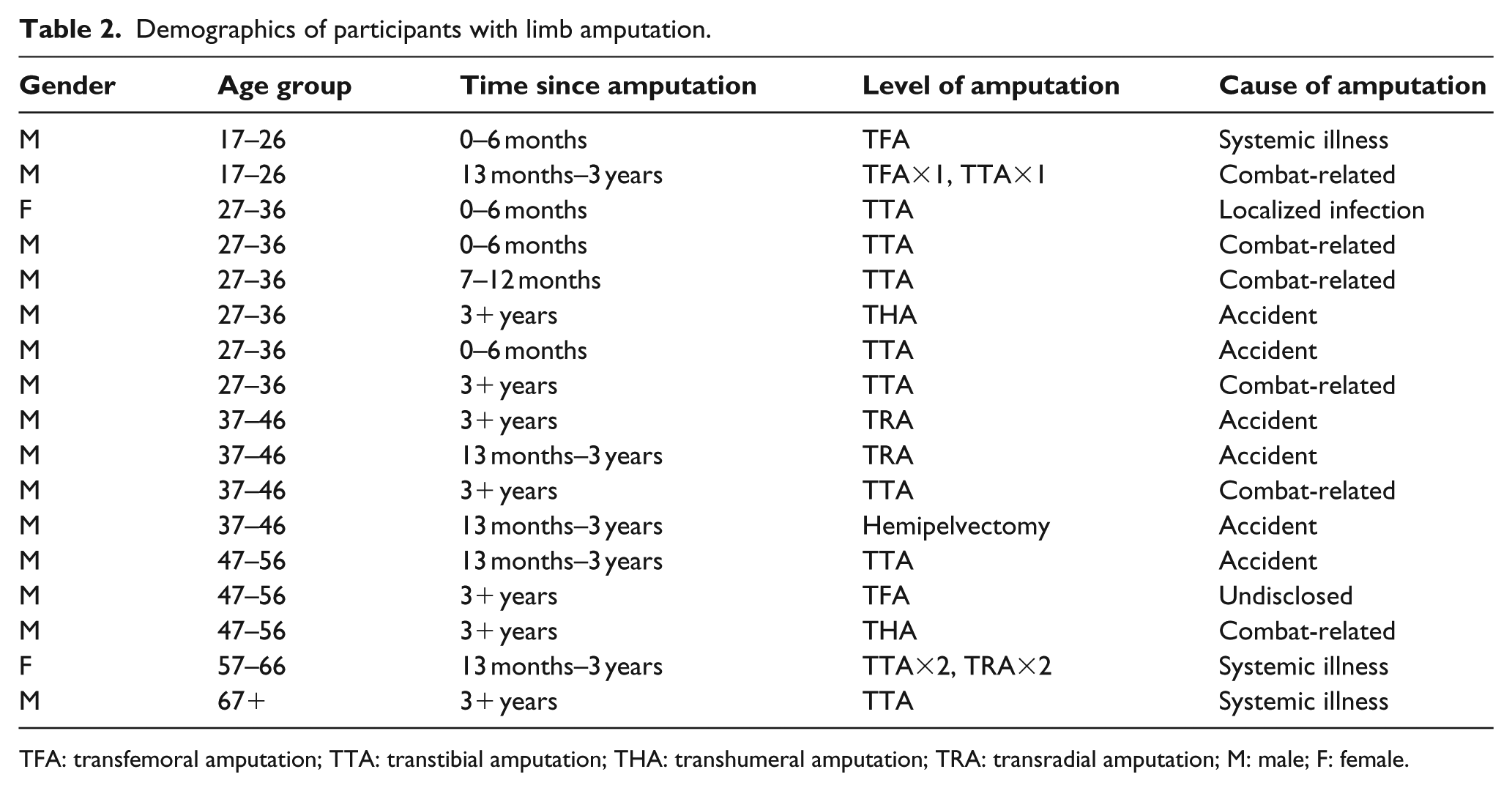
TFA: transfemoral amputation; TTA: transtibial amputation; THA: transhumeral amputation; TRA: transradial amputation; M: male; F: female.
Program modifications and feedback from participants.
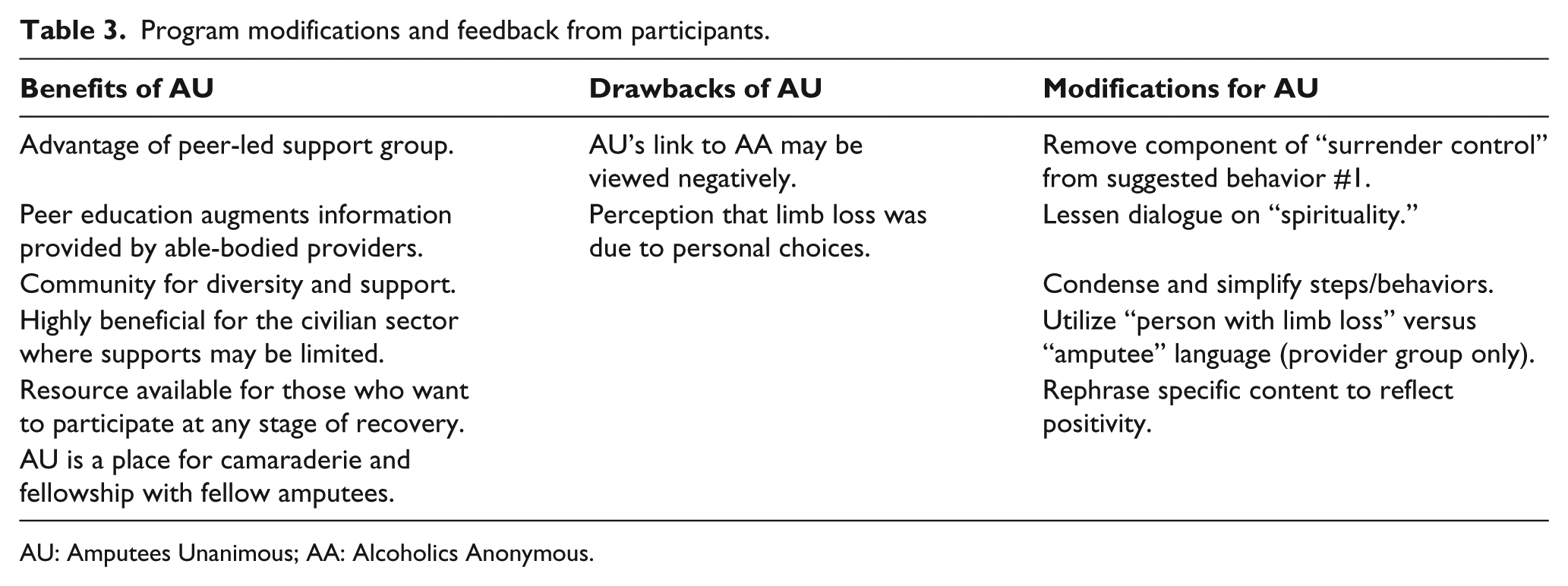
AU: Amputees Unanimous; AA: Alcoholics Anonymous.
Themes
Three themes emerged from data analysis of the focus group discussions: (1) accepting limb loss, (2) peer inspiration, and (3) regaining prior level of function.
Accepting limb loss
Acceptance of limb loss was the primary theme. Participants viewed acceptance as an essential stage to psychological recovery, expressing a belief that recovery may be prolonged when the amputated limb is not mourned. Cause and length of time to amputation were reported to alter the acceptance process. Specifically, having the opportunity to prepare for a shift in body image, obtain knowledge, and acquire support can facilitate acceptance. If the amputation was necessary to save the individual’s life, acceptance was easier. For three participants, military training and the mind-set to never quit were factors in overcoming adjustment to limb loss.
Nothing changed. The world didn’t change, stairs didn’t change, the elevator didn’t change, door knobs didn’t change, your wife didn’t change, your kids didn’t change, you changed. Now you have to adapt. It wasn’t a harder journey for me because I already accepted it … I’m missing bones … they’ve been crushed beyond [repair]. My body’s killing me; and let’s see what amputation is gonna do? I know what it’s gonna do, it’s gonna keep me alive.
Healthcare providers spoke more of adaptation than acceptance for the amputee patient throughout the recovery process. Two providers felt the adaptation process was continuous, evolving as one ages, while another two viewed it as a learning process.
It’s not so much adapting as learning … They adapt at an early stage, hopefully acutely, and then have to be a lifelong learner to see how to maximize their function lifelong versus continuing to adapt. I mean, once you’re an amputee you’re an amputee. You do adapt to being an amputee. The process usually takes about two years, but you are adapting to what you are now. You adapt to being an amputee at age thirty, but when you’re age fifty, you’re a different amputee … Now other parts of your body are decompensating also so you are a new amputee in a sense … You do have to re-adapt to being an amputee.
Maintaining a viewpoint of purpose, perspective, and faith were highlighted as supports to acceptance by amputee participants. Furthermore, medical staff, rehabilitation specialists, family, and peers were viewed as aids in developing a sense of structure and direction onto the path of recovery and wellness.
Peer inspiration
Peer support and inspiration throughout the recovery process emerged as important elements. Participants remarked on how meeting a fellow amputee and hearing his or her story provided optimism for the future. Three individuals gained encouragement simply by observing fellow amputees engaging in activities that the participant had once enjoyed prior to limb loss, providing a sense of hope. One participant was inspired to live his life in honor of a friend, reminding himself of the fragility of life. Another commented on how simply living and being authentic to oneself was enough to inspire peers.
One of the biggest and most helpful things for me throughout all of this has been when people have given me, ya know, input on their experience and what they needed to overcome. Some of the biggest, best, visits I had at the hospital were from Vietnam veterans. When you see a guy, from another generation, who fought a war from before you were even born, and they’re living with injuries … amputations, and all kind of other things, and you see they’ve done it. They have a quality of life, and they’re living like nobody’s business. That said to me, right there in the hospital bed, I can be like that guy. Whenever a new amputee came in, it always appeared like all the guys put their issues aside, and everybody kind of jumped in, and some of it was educational, some of it was just answering questions for the new guy … helping the new guy along.
One participant reflected on the absence of peer support during his time of recovery from limb loss.
No, I did not have any sort of peer group, and it would have been helpful.
Five participants remarked on how they choose to be a source of inspiration for new amputees, visiting hospitals and sharing their personal stories of triumph.
One of my goals from the very beginning was when I get home I want to go to hospitals and volunteer to talk to people in similar situations that I’m in and tell them that it’s not the end of the world. Tell them, “Yeah, listen, you’re going to have hardships. Things aren’t going to be as easy as they once were, but as long as you just pick yourself up, stay motivated, stay positive, and keep moving forward, everything will work out.” I think it’s really something that you help out with a new amputee, because you can help motivate them and give them a lot of knowledge on how to deal with the issues of losing a limb.
Peer support offered hope, fostered determination, and inspired re-engagement in daily activities.
Regaining prior level of function
Step 4 of AU was a popular topic for discussion, addressing the challenge of regaining pre-amputation level of activity. A total of 10 participants remarked on how they viewed their new physical limitation not as a disadvantage, but as an obstacle to overcome.
I try to be [as] normal as possible after the amputation, trying to do everything that I did before. I don’t look at it as a limitation. I just overcome it. It was just, you gotta do this stuff, so do it. There wasn’t really anything that was impossible to do. So like I said, to the greatest extent possible, I got back to doing just about everything I could.
Engagement and successful completion of an activity without the assistance of others was seen as a high accomplishment within recovery. A positive outlook combined with perseverance was a key factor in regaining independence. For four participants, goal-setting was a means of motivating oneself to regain functional performance. One participant remarked on how he pushed himself to engage in activities he never attempted prior to amputation.
For me personally, I’ve done a lot of things. You know, getting out there and doing things that I haven’t even done when I did have legs. Like kayak, fishing, golfing … a whole bunch of stuff and bowling. That’s what it means to me. Just getting out there and doing your best. I accept that I’m, to a certain extent, crippled or broken or whatever, but I’m going to focus on that number [Step] 4 there, and I’m going to get back my independence, and I’m going to get back to doing what I do … for me, that was the biggest challenge. I know for me … I didn’t want to be that guy who was just sitting there. You know, come hell or high water, I want to be out moving again whether it’s in the military, hiking, swimming, biking, whatever. I just kinda made it a purpose so that’s what I’m going to do.
Discussion
This study examined the content of AU by adults living with limb loss as well as by inter-disciplinary healthcare professionals who work in amputee rehabilitation. Adjustment after limb loss, both physically and psychologically, was expressed as a personal journey and evolving process. No matter the cause, level, or time since amputation, each participant identified a connection to the AU program. Participants recommended similar modifications to the program enhancing the structure of the AU program for the amputee population.
In the traditional five-stage grief model, acceptance is often recognized as the last phase. 24 For focus group participants, numerous factors played a role in achieving acceptance. One participant expressed accepting the injury immediately, with difficulty experienced in regards to proposed recovery time to regain pre-amputation level of activity. Limb-salvage participants who lived with a painful, non-functioning limb for years expressed an ease into the transition to acceptance, discovering improved physical performance after amputation. Although acceptance has typically been described as the final stage of grief, amputees experience a dynamic array of emotions after limb loss. 25 A rescaled model consistent with this theory was proposed by researchers, supporting continual negotiation of acceptance throughout the recovery process instead of experiencing it as a final step. 26
Peer support is an element discussed frequently within amputee literature. Inspiration is discovered through various means, from observing those ahead in the rehabilitation process to comparing personal situations to those of past amputees, when supports and technological advances were limited. 14 Four study participants commented on the camaraderie and fellowship discovered while rehabilitating next to fellow patients with limb loss. Communicating with peers who understood the struggles of living with limb loss has been cited as providing comfort 2 as well as emotional and psychological wellbeing. 17 Peer support and education has been viewed as a greater benefit than physician instruction 18 or practical support from healthcare professionals. 14 Fellow amputees are regarded as role models and foundations for encouragement to regain functional independence.11,14,15,17,18 The literature on peer support and inspiration was confirmed by participants’ stories.
Focus group content revealed narratives of personal goals to regain prior level of function, some revolving around work-related tasks, while others involved re-engagement with family members. Hamill et al. 14 performed semi-structured interviews with amputees 18 months after limb loss, discovering a theme of “renegotiation of self-identity to new ‘disabled’-identity.” Participants expressed frustration with loss of independence post amputation, and that assistance from able-bodied peers was at times overwhelming. Goal setting was used by these participants as a means to regain independence. 14 Senra et al. 27 also found that 38 of 42 amputee participants they interviewed expressed the desire to obtain independence through establishing goals, with desired skills ranging from basic daily activities to work-related tasks. Overall, function in daily life has been related to emotional well-being and psychosocial outcomes. 9
AU program modifications expressed during focus group discussion relating to powerlessness and spirituality within the 12-step model have been reported in prior research.28,29 A study conducted to evaluate patient and clinician attitudes toward 12-step groups found several obstacles to participation, with the emphasis on powerlessness and religious implications as factors of resistance to treatment.28,29 Although 12-step programs are formatted as spiritual programs, the utilization of words such as “higher power,” “prayer,” and “God” may be viewed as religiosity. 29 Conversely, the 12-step models’ ability to generate a sense of belonging, cohesiveness, hope, and fellowship among members are cited as beneficial aspects to attendance.28,30
Accepting limb loss, inspiration by one’s peers, and regaining prior level of function were identified as important factors for psychosocial recovery and wellness. This evolution was both personal and dynamic, with varying accounts of the challenges faced after limb loss.
As healthcare providers involved in amputee care are elected as rehabilitation guides, it is vital that these professionals identify when patients need psychological assistance, being holistic in their evaluation and treatment. Knowledge of support systems which may compliment physical rehabilitation can be an additional tool for clinicians to utilize throughout therapy, as providers are a gateway for information exchange. Recommending support systems and programs which incorporate key protective factors highlighted within the literature should be carefully selected and evaluated for appropriateness.
Participants identified with the AU 12-step program and discussed the benefits of a peer-led support group. Emphasis was placed on the need for AU within the civilian sector, due to a lack of “ready-made community [supports] to walk into.” This is in contrast to military treatment facilities for wounded military members who are provided the opportunity to rehabilitate alongside fellow amputees, with ample support possibilities. AU provides a platform for knowledge exchange between amputees, bridging the gap exposed by able-bodied healthcare providers leading an education (content-focused) group. The absence of a professional for execution of groups allows for enhanced availability throughout the community, 31 bringing amputees together and providing an additional resource for familial support.
Limitations of the study may include self-selection bias because participants could have adapted better to limb loss than those who chose not to participate. In addition, lack of understanding questions posed during the focus groups may have influenced data collected. Despite attempts made to stratify across limb amputation types and mechanisms of injury, the small sample size may not be representative and generalizable, particularly because of the large number of military members in the group which may not represent the general population. This is highlighted as a limitation because the AU program was designed to be utilized by adults with limb loss across all strata; however, the majority of study participants were young males who sustained limb loss from an accident or combat-related incident. Finally, the focus group format may have deterred participants from discussing personal stories, limiting honest feedback.
Conclusion
Overall, participant feedback on the content and suggested modifications for the program mirrored that found in AA literature, assisting in the revision of the program. The results of this study revealed helpful suggestions to modify AU content, as well as explore the value of such a program. Research is thus necessary to test the clinical effectiveness of the AU program within the community of adults with limb loss. This participant-led 12-step program was written to facilitate coping after limb loss by providing individuals with encouragement, support, and optimism for the future. This study was the first step in the line of research to assess its ultimate utility.
Footnotes
Acknowledgements
The authors would like to thank all participants of the study and acknowledge the support of Jill Cancio, OTD, OTR, CHT for her guidance and support. The view(s) expressed herein are those of the author(s) and do not reflect the official policy or position of Brooke Army Medical Center, the US Army Medical Department, the US Army Office of the Surgeon General, the Department of the Army and Department of Defense or the US Government.
Author contribution
All authors contributed equally in the preparation of this article.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: K.Y. holds a copyright of the AU materials but provides open-access to all content via the Internet.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.