
Abstract
Background:
Lower limb amputation due to workplace injury and motor vehicle accident is common in Bangladesh. Qualitative research may extend our understanding of how physical impairment and other factors, such as cultural norms, family roles and the built environment, facilitate or hinder work participation following lower limb amputation and prosthetic rehabilitation.
Objectives:
The aim of this study was to explore the experience of people in Bangladesh following lower limb amputation and prosthetic rehabilitation to understand the facilitators and barriers to their work participation.
Study Design:
Qualitative interviews with thematic analysis.
Methods:
The Worker Role Interview was used to guide semi-structured interviews in a convenience sample of 10 adults living in Bangladesh following lower limb amputation and prosthetic rehabilitation. Interviews were interpreted, and the themes that emerged were evidenced with first-person quotes.
Results:
Barriers and facilitators to work participation were synthesised into the following themes: spirituality, attitudes, meaning of work, planning for work participation, traditional gender roles, social support, mobility aids, environmental challenges and ergonomic adaptations.
Conclusion:
This qualitative approach identified barriers and facilitators to work participation, such as the role of spirituality and the effect of gender roles, that have not been well researched in this population. Being aware of their effects can help clinicians reduce barriers to work participation.
Clinical relevance
Greater awareness of the barriers and facilitators to work participation, such as the role of spirituality or the effect of gender roles, can assist clinicians to reduce barriers and help facilitate work participation for people living in Bangladesh following lower limb amputation and prosthetic rehabilitation.
Background
Of the 160 million people living in Bangladesh, more than half are of official working age (> 15 years) and there is no specific retirement age and a limited social welfare system. 1 Males account for over two-thirds of the workforce. 2 Jobs are most commonly in agriculture, construction and manufacturing where standards of workplace safety are generally poor, and accidents resulting in lifelong disability are common.
Lower limb amputation (LLA) is one such lifelong disabling condition affecting working-age people in Bangladesh. There are significant barriers to participation in the years following LLA given limited education and access to timely rehabilitation and prosthetic services, mobility challenges, difficulties accessing the physical environment and public transport, public attitudes to disability, poor mental health, social isolation and loss of roles within family and society that define a person and bring meaning and purpose to life.3–6
Our understanding of the impact of these factors on work participation is limited, given that most studies have used quantitative methods to examine the effects of demographic and amputation-related factors on work participation after LLA in countries with well-developed healthcare systems.7–10 Few studies have examined the effects of pain, level of mobility or the effect of comorbidities,11,12 or described the impact of the environmental or psychosocial factors on work participation following LLA.13,14
When work participation is considered with respect to contemporary models of function, disability and participation, such as the Model of Human Occupation (MOHO), the narrow focus of previous research becomes apparent. 15 For instance, MOHO describes that work participation is influenced by a person’s values, interests, motivation, roles, habits, capacity and skills, together with the physical and social environments in which they participate. 15
Given these factors have not been the focus of previous research, little is known about the extent to which they influence work participation following LLA. Similarly, little is known about the time and support required to establish new habits, skills or the self-belief and motivation needed to participate in work or the extent to which societal views on disability make it difficult to find employers willing to engage and support people with disability to participate in work.13,14
In this investigation, we are particularly interested to learn more about the barriers and facilitators to work participation for people in Bangladesh who have accessed prosthetic rehabilitation and are now living in the community. We are not aware of any research specific to this population, despite the importance of economic participation for people living with LLA and their families. It is important that we learn from people living with LLA following prosthetic rehabilitation about the issues that directly affect them now; particularly given the importance of their lived experience to inform the design of locally relevant programmes to improve occupational rehabilitation.
The aim of this study was to explore the lived experience of people in Bangladesh following LLA and prosthetic rehabilitation to understand the facilitators and barriers to their work participation.
Methods
Recruitment
A convenience sample was recruited using flyers, posters and the participant information statement from multiple CRP centres in Bangladesh. Those seeking rehabilitation and prosthetic services could self-refer or be referred for care regardless of their financial background and geographical location. Participants were eligible if above 18 years of age, with uni- or bilateral transtibial or transfemoral amputation, able to provide informed consent and willing to share their experiences of living with LLA in a face-to-face interview at a CRP centre.
Procedure
People interested in participation could contact the study coordinator who scheduled a face-to-face interview at a CRP centre. Each participant was provided a participant information statement in Bangla. The statement was read aloud as needed given the low level of literacy of many participants. Participants had the opportunity to ask questions, and their understanding of the purpose and procedures was confirmed by follow-up questions prior to providing signed consent.
During the interview, participants completed the demographic section of the Trinity Amputation and Prosthesis Experience – Revised (TAPES-R) 16 as well as the 7-item Prosthetic Limb Users Survey of Mobility (PLUS-M) 17 to characterise the sample. Questions were adapted where necessary, so the instruments would be appropriate for use in Bangladesh. For example, within the PLUS-M, the word ‘curb’ was changed given that roads in Bangladesh do not typically have curbs, with the word ‘doorstep’ used as an alternative as the front doorstep or lip of a home in Bangladesh is about the same height as a street curb in North America where the PLUS-M was developed and validated. The Worker Role Interview (WRI) is a semi-structured interview used to guide a conversation where people share their experience and thereby elicits details about an individual’s personal causation, values, interests, roles, habits and perceptions on environmental factors that influence work participation after injury.18–20 Originally designed to gather data from injured workers, the current version has been designed for anyone with disability 19 and widely used to gain insight into the past, present and future perspectives of work participation.21,22 In accordance with the user’s guide, 19 questions about the participant’s background and context were asked, sometimes being reordered or restructured to facilitate exploration of factors related to their work participation after LLA and prosthetic rehabilitation. While the WRI also includes a rating scale, this was not used as our intent was to elicit details about the individual’s experience through a meaningful conversation, not rate the extent to which an item supports or interferes with work participation. In this way, the WRI can provide an understanding of the ‘unique factors that affect a person’s success in assuming the responsibilities of work-related tasks and the worker role’. 23 The WRI was field-tested in a previous investigation involving people living with spinal cord injury in Bangladesh. 24
These three instruments (i.e. demographic section of the TAPES-R, PLUS-M and WRI) were translated from English to Bangla by one of the researchers (M.M.U.); a native Bangla speaker and allied health professional with undergraduate and postgraduate tertiary education in both Bangla- and English-speaking universities. Translations were checked by two bilingual professionals (i.e. a Bangladeshi rehabilitation counsellor at CRP and a Bangladeshi academic working in an Australian university) for verification and relevance for participants with diverse backgrounds, and changes made where required into simple and appropriate language. Translated copies were also approved by the Bangladeshi ethics committee.
Interviews were conducted in Bangla by one of the researchers (M.M.U.); a Bangladeshi national with many years of clinical experience working as a senior Occupational Therapist in acute and rehabilitation settings in Bangladesh. Interviews were audio-recorded for transcription and analysis. Handwritten notes were made during the interviews to supplement the audio recordings. A reflective journal was used to record the interviewer’s personal experience to allow them to become aware of any bias that might influence subsequent data analysis.
Each participant was reimbursed BDT3500 (about US$40) to cover the cost of attending the interview; an amount typically used by CRP to cover patient travel expenses.
Data analysis
Data from the demographic section of the TAPES-R describing the sample were summarised using descriptive statistics appropriate to the data type and tabulated. Survey responses from the PLUS-M were summed for each participant to produce a raw score, and the corresponding T-score were obtained from the appropriate conversion table. 25
Each interview was transcribed verbatim. Names of people and places were replaced with pseudonyms. Transcriptions were translated from Bangla to English by a bilingual research assistant and independently checked by the interviewer (M.M.U.) who listened to the audio recording and read the transcripts in tandem. Corrections were made to ensure that the transcription translation was a true reflection of each conversation. Each transcript was subsequently read by one of the researchers who was a native English speaker (R.S.), and phrases that did not make grammatical sense were queried and discussed with the interviewer (M.M.U.). Any corrections were made with reference to the Bangla transcripts to preserve the original meaning.
The subsequent analysis was undertaken by the interviewer (M.M.U.) and another researcher (R.S.) following the steps described by Liamputtong. 26 In summary, each transcript was independently reviewed by the interviewer (M.M.U.) and another researcher (R.S.) to get a sense of the participant’s responses. Margin notes identified thematic ideas which arose entirely from analysis of the participants data. Keywords or phrases were used to code the data to describe the facilitators and barriers to work participation. Codes were compared between the independent analyses undertaken by these two researchers, and variations resolved by discussion until consensus. Codes were grouped across interviews to synthesise similar experiences, and themes developed which were presented with supporting quotes that exemplified and supported the interpretation. Interview data were processed in this way until data saturation. 27
Results
Participants
Participants were relatively young (34.6 ± 12.3 years), mostly male (70%) with transtibial (50%) or transfemoral amputation (50%) due to road traffic or workplace accidents (80%) some years prior (4.9 ± 4.3 years), and had levels of community mobility typical of population norms (PLUS-M T-Score: 54 ± 10) (Table 1). 28 Prior to amputation, participants worked long hours each week in domestic work, office or retail jobs, or the ready-made garment industry (Table 2).
Study participants’ descriptors.

LLA: Lower limb amputation; RMG: Readymade Garment; RTA: Road traffic Accident; TTA: Transtibial amputation; TFA: Transfemoral amputation.
Bilateral LLA; # Participant was primarily a wheelchair user and utilised prostheses for cosmetic purposes in public.
Participants’ employment, training and support characteristics.
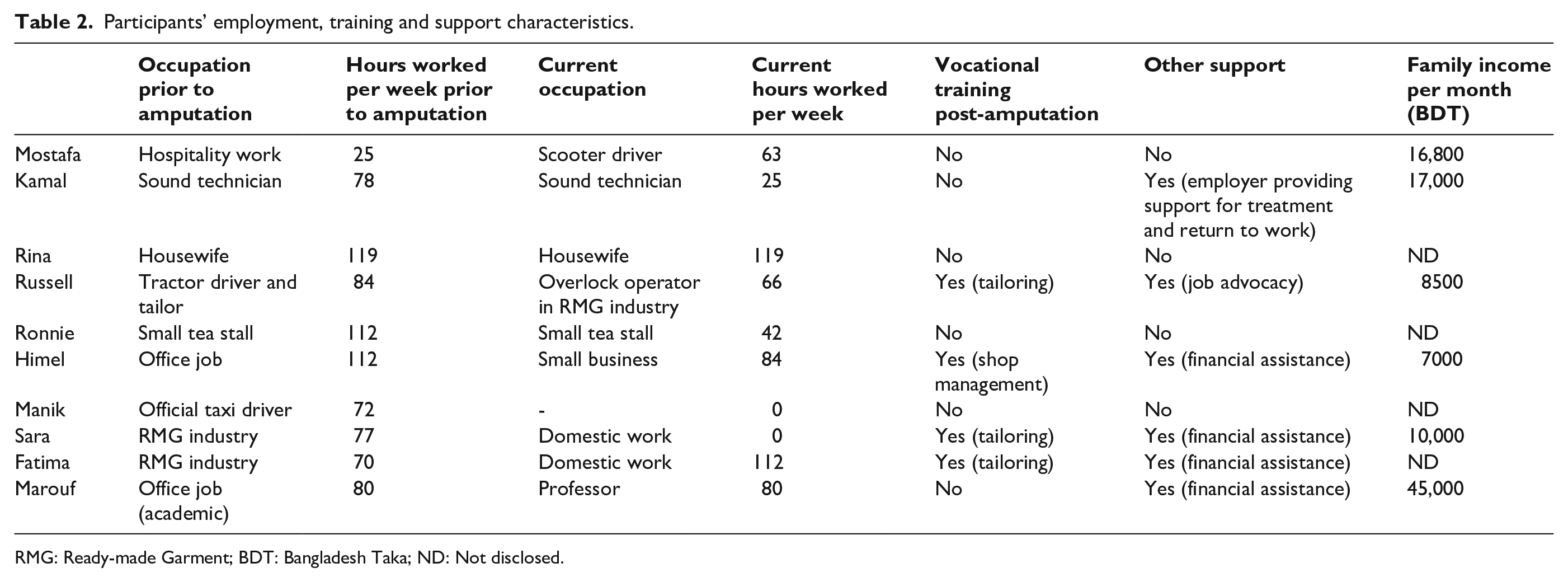
RMG: Ready-made Garment; BDT: Bangladesh Taka; ND: Not disclosed.
Thematic analysis
Commensurate with the aim of the study, barriers and facilitators to work participation derived from a thematic analysis were synthesised into eight themes (Figure 1); each of which is described in the following subsections.
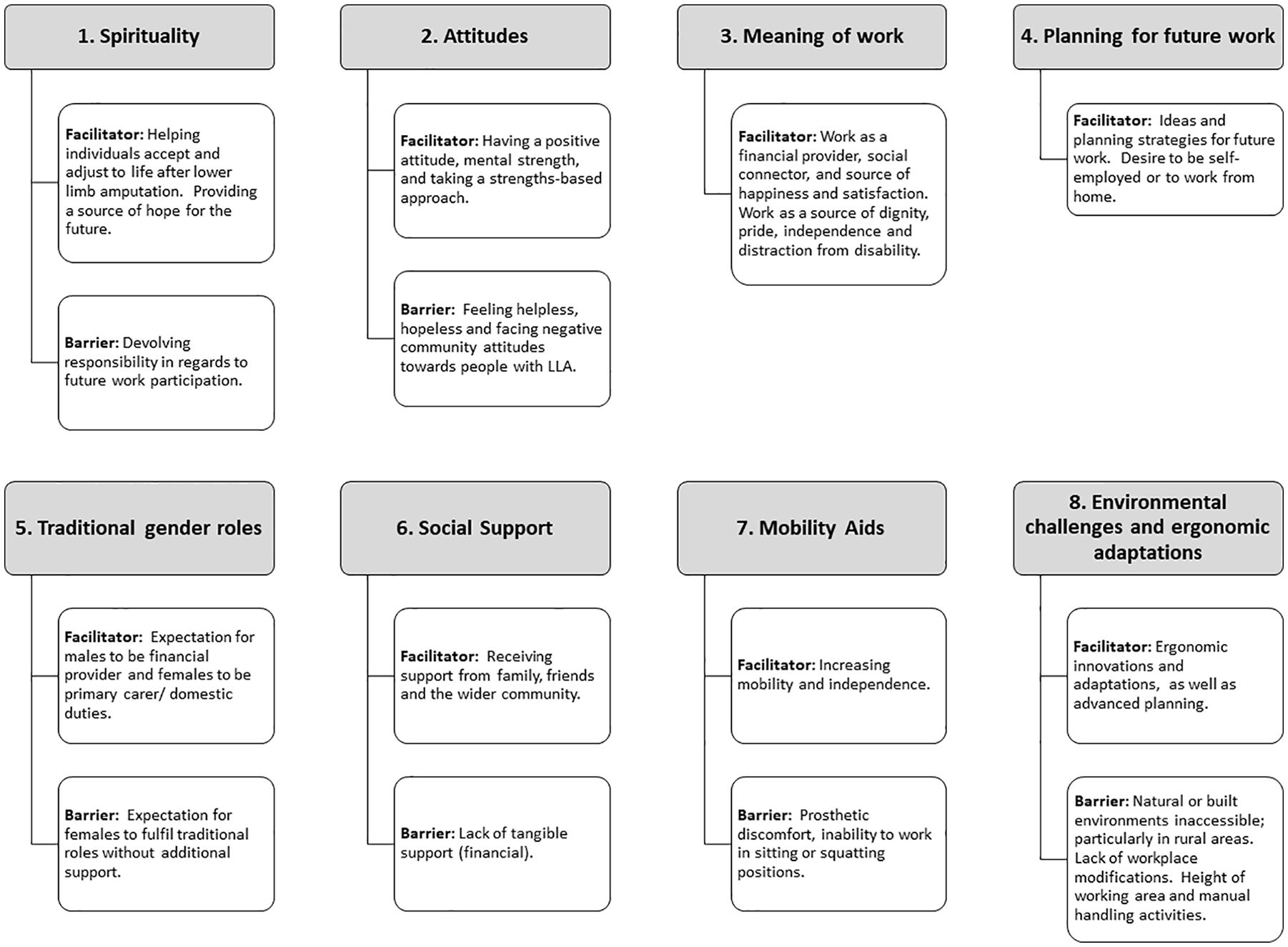
Themes related to work participation after lower limb amputation in Bangladesh.
Theme 1: Spirituality
The ability to participate in work was seen as a matter of fate given many participants devolved responsibility to Allah or the Almighty. This fatalistic view was often a barrier to work participation:
If I am meant to work, The Almighty will bless me to. He will make me fitter. I always pray to Him that He may shower His blessings and make me fit for work. – Kamal (M, 38)
By contrast, spirituality helped many participants deal with the grief of losing a limb, adjust to life after amputation and find meaning in what had occurred. These were important steps towards acceptance and work participation facilitated by faith in Allah:
I prayed to Allah that He keeps me happy whatever situation He wants me to live in. I want to live with that prayer. Since then I have never had such sadness. – Mostafa (M, 36) When I had the injury, I was very worried about my mobility and it hurt a lot. I am now adjusting to it. With the grace of Allah, everything comes to be a habit with time. – Sara (F, 24)
Theme 2: Attitudes
Attitudinal barriers to work participation were evident when participants reflected on their life prior to amputation, what they had lost, and the seemingly insurmountable limitations of living with LLA. Long-standing emotions – sadness, anger, helplessness and hopelessness – were a barrier to work participation for some:
It is not possible [to run my tea stall], because I am not as I was previously. Now I have one leg. Without the other leg it is not possible to do work. Now there is no hope. – Ronnie (M, 26) I had physical well-being and inner peace but, I have totally lost it now. So, there is no happiness in my life now. – Sara (F, 24)
Others’ attitudes towards people with amputation were often negative, lacked respect and reflected a limited understanding about what people with LLA could do:
. . .some people ask me whether I have a maid. . . They cannot imagine that I don’t need a maid. I can take care of my child. . .and do other activities by myself. – Fatima (F, 23)
Some participants described how community insensitivity and curiosity towards their amputation impacted their ability to participate in work as questions about their amputation were often distressing to relive:
I don’t want to let people see my amputation and acknowledge it. Because, when people acknowledge it, they start to ask questions. It felt difficult to deal with. – Himel (M, 33)
These cultural attitudes of low expectations and prejudice were a barrier to work participation.
Theme 3: Meaning of Work
The need to fulfil financial and other family responsibilities was a powerful impetus facilitating work participation. Typically, participants’ households included several generations, and many had financial and caring responsibilities for their spouse, children, parents or parents-in-law. Many faced economic hardship due to rehabilitation costs without access to structured systems of social welfare:
I have gone [back to work] because of my economic hardship. At present, I owe money to many people and interest on a loan. My accident cost me BDT 450,000. The rehabilitation centre costs me BDT 12,700. In total, I am in debt about BDT 500,000 [BDT 500,000 is about 2 ½ years’ salary based on average income of participants’ who disclosed their salary in this study]. – Ronnie (M, 26)
Work provided participants with an important means of connecting with the outside world and a source of happiness and well-being. Work participation was integral to many people’s identity and a source of dignity, pride and independence:
I enjoy my work very much. I feel free when I chat with those around me. I am well because of my work. – Himel (M, 33) There is no better food than that from one’s own hand. It is a psychological satisfaction for myself to work. Being dependent on others, even for food, cannot satisfy anyone. – Rina (F, 32)
Given the cultural stigma associated with unemployment or begging, many participants seemed driven to participate in work:
If I do not work they [customers] will think I am sitting at home, doing nothing. I will never beg…This is my love and I am proud of doing this. I have achieved many things through this work. I bought my land with this work [after the accident]. – Russell (M, 25)
Theme 4: Planning for Future Work Participation
For many participants, the type of work they wished to participate in changed after LLA. There was a strong desire for people to undertake work that aligned with their perceived abilities and to resolve related practical challenges. Many desired to work close to home or become self-employed. Planning practical strategies to achieve these goals was an important facilitator for work participation:
I will keep doing the same work [as an over locker operator in the ready-made garment industry]. If I am fortunate enough, and if I can make more money and save, I will set up a tailor shop at my home. – Russell (M, 25)
A number of participants used a strengths-based approach to focus on their current abilities, rather than limitations, to identify appropriate work:
. . . then I thought my left leg is not good, but to drive a ‘Hello Bike’ only requires the use of my right leg to push the brake. So, I thought I could drive a Hello Bike . . . I did not find any barriers. I can manage my Hello Bike easily. – Mostafa (M, 36)
This practical forward thinking assisted people to feel empowered, hopeful and optimistic and better able to navigate psychological and physical challenges to work participation.
Theme 5: Traditional Gender Roles
Traditional gender roles were an important factor influencing work participation for both men and women.
Women participants were highly motivated to fulfil their traditional role of homemaker with responsibility for cooking, cleaning and caring for elderly family or children. There was an expectation that they would maintain their domestic role after LLA, often without spouse or family support. Due to the physical demands of domestic work, women participants described they had little time or energy left for work outside the home. None of the women in this sample were in paid work after amputation, despite two of the three being employed in ready-made garment work before LLA (Table 2):
The reason for not being involved with any other [paid] work is time. I don’t get enough time after my domestic work. . . I need all day now for domestic work. Cooking and other things are time consuming. I have my child, parents and mother in-law [dependents]. – Sara (F, 24)
There was a reluctance to ask for support from their spouse or extended family – to not to be a burden; particularly given that failure to fulfil an expected role left some women feeling their spouse may leave:
If I ask someone [to help] it might be hard for them too. It becomes very difficult for my mother and sister-in-law when I go home. When I am dependent on them, this actually increases their workload. – Fatima (F, 23) Our kids are scared, because if I don’t continue my domestic responsibilities their father might get married for a second time. – Rina (F, 32)
By contrast, men who participated in this research identified with the traditional role of financial provider, their desire to fulfil this role being a strong motivator for work participation:
Everyone in my family depends on me . . . There are four people in my family. I need to take care of all of them, like food, and everything. I am bearing all the responsibilities for the income. – Mostafa (M, 36)
However, in a departure from traditional roles, many men who could not work following LLA received considerable support from their wives who increased their own work participation by adopting the non-traditional role of breadwinner in addition to their domestic roles:
My wife works very hard for me. She even does overtime duty in the garment factory to earn extra money. – Kamal (M, 38)
Theme 6: Financial, Practical and Social Supports
Most participants received some form of financial, practical or social support which facilitated work participation. Not having these supports was a real barrier to work participation:
XXXXX asked me to start a shop. . .I said I can start, but I have no capital. They asked me to start first and get support later. . .After I started, XXXXX gave me some goods [grocery and stationary items] and BDT 7000. . . I find that I am doing well, but if I had more capital, I would do better. – Himel (M, 33) I need 6000 Taka to get my driver’s license renewed. Once it is renewed I can work for the next five years. I am struggling to manage the family’s expenditure and cannot save money. If I stopped my family expenses I could renew my license. – Manik (M, 46)
While assistance with self-care activities was usually provided by family, support with domestic chores, such as cooking or collecting water, was often provided by neighbours or extended family:
My mother-in-law works very hard for me. I was at home for two years after the accident. She undertook all my care, like showering, toileting and even bed mobility. – Kamal (M, 38) Many people give their garment orders to me, and they give me a better rate for the same work, 10 taka to others, but 12 taka for me. My work is also good, and they supported me. – Russell (M, 25)
Some participants described other forms of support, including friendships, which brought reassurance and advice:
I had a neighbor, a police officer. He used to visit me and sat beside my bed and reassured me when I cried often. – Mostafa (M, 36)
Theme 7: Mobility Devices
While all participants reported that mobility devices were an important facilitator for work participation, there were barriers related to their use. Prolonged prosthesis use often resulted in discomfort and/or residual limb pain which negatively affected work participation:
The owner asked me to use the prosthesis in the workplace too. But I cannot keep wearing it for more than four hours. So he said to use it for four hours. If the prosthesis fitted the stump a little bit better, I could continue to wear it for more hours and work faster than now. – Kamal (M, 38)
Many participants would remove their prosthesis to prevent damage or to undertake activities, such as cooking, washing, toileting and prayer; tasks often performed in a squatting or kneeling position given traditional style homes with working areas located on, or close to, the floor:
I can’t do anything when squatting, I need to be standing. But it is not possible to place firewood into the burner while standing. The problem is similar with harvesting activities. . . and I face difficulty while washing clothes because I can’t wet the prosthetic limb. I can’t use the prosthetic limb when saying prayers, ablutions, sleeping and taking a shower. – Rina (F, 32)
Fatima, who had bilateral transfemoral amputations, chose to use a wheelchair rather than her prostheses to facilitate work participation:
I would never be capable of doing these activities if I didn’t have the wheelchair. A wheelchair allows me to move here and there. So, I think if I can go somewhere, I can do work there. – Fatima (F, 23)
Despite these barriers, many participants viewed their prosthesis as having a positive impact on their mobility and independence, allowing them to undertake work that would otherwise be impractical or impossible:
The artificial limb helps me a lot. I can perform every activity a non-amputee person can do except lifting the heavy sacks. . .I think it would not be possible to continue shop-keeping without the prosthesis. – Himel (M, 33) It is not possible to do this type of work without the prosthesis …I can take care of myself now, I couldn’t even go to the wash room when I didn’t have it. – Rina (F, 32)
For some participants, the prosthesis was a facilitator enabling participation in public. Sara, who had a transfemoral prosthesis and would remove her prosthesis while undertaking domestic duties stated,
It’s more about a cosmetic purpose, and still I have to use the crutch. -Sara (F, 24).
Theme 8: Environmental challenges and ergonomic adaptations
Almost all participants described situations that prevented work participation due to difficulties navigating the built or natural environment. For example, the combination of heavy rains and unmade roads – particularly in the monsoon season – were real barriers to work participation for those living in rural areas:
My house is distant from my shop, about half a kilometer. . . through bushes and trees. So, at night I cannot travel back up and down a muddy road. I might fall, so with this fear I go back earlier. – Ronnie (M, 26) I was supposed to go to the local market the day before yesterday. But, it was raining all the time and I had to stay home. . . when I had my real leg, I could go out even after getting drenched. – Sara (F, 24)
Traditional style homes and workplaces were often designed so work was done close to or at floor level. Participants either avoided or minimised work requiring squatting or repeated changing from standing to squatting:
It is not possible to keep working from a standing position and there is no scope for doing anything in the floor sitting position using the prosthesis, so the height of the working area is a challenge sometimes. Some activities related to cutting and cooking need to be done in both these positions. I cannot handle those activities. – Rina (F, 32)
While the ability to live in purpose-built accommodation helped overcome many of the environmental barriers and facilitated participation, so too did the ability to develop innovations, strategies or adaptations:
I generally face difficulty in lifting heavy weights. I have to carry the cooking pots to the burner. . . I have to complete that in stages with different repetitions of lighter lifting and carrying. – Sara (F, 24) I want to overcome the physical limitations by thinking and planning. If I can’t take the bus, I take the rickshaw instead. As I have difficulty getting up and down, I wear pants instead of a loin cloth. I worked these things out for myself … I faced a problem with the toilet. There is no high commode in the village, but I carry a rubber tire tube for sitting. – Mostafa (M, 36)
Discussion
This study described the lived experience of 10 adults with LLA in Bangladesh following prosthetic rehabilitation and points to a wide range of facilitators and barriers to work participation. Many of these experiences are consistent with the broader body of literature about the experience of disability in Bangladesh and highlight complex interactions between factors, such as perceptions of disability, gender roles, culture, access and the environment.29,30
Most participants in this sample were relatively young males with amputation at transtibial or transfemoral level, due to road traffic or workplace accidents many years prior, with either primary or early secondary school education. While these participants were typical of those who have accessed prosthetic rehabilitation in Bangladesh, 6 it is likely that the sampling method favoured those who found participation convenient given their proximity to the rehabilitation centres where the interviews were conducted.
Prior to amputation, participants worked long hours, not uncommon in Bangladesh, despite labour laws that cap work at 60 hours per week. 31 Given the limited oversight of these regulations, low pay rates and limited social welfare systems, it is not surprising that many work long hours.32,33
Our interviews highlight that when a male lost a limb, the female spouse assumed many of the occupational responsibilities, but this role reversal did not occur when a female lost a limb. A woman may have sought her first paid employment after their spouse had an amputation, thereby assuming a disproportionate amount of paid and unpaid work without the equitable exchange of work roles where their husband undertook domestic or childcare duties. This finding is consistent with previous studies examining the impact of disability on relationships and work roles29,30,34 and could be attributable to cultural norms where work roles are often defined by sex. Men may find the loss of their typical role difficult and be unable to adapt to work assumed to be the purview of women.
If individuals and their families are to successfully adapt to new work roles after LLA, it is important they are supported through complex issues, such as renegotiating notions of what is fair and equitable in relationships, new family roles and identities or the sense of obligation one partner has to the other.34–36 These sorts of discussions are necessary to help reduce the risk of relationship breakdown, exacerbation of disability impact and related risk of poverty, given the discrimination, exclusion and isolation that disproportionately affects women with disability in Bangladesh.29,30
Brokering these conversations can be difficult for many clinicians without training specific to this type of facilitation. As such, we encourage clinicians to work with those in the rehabilitation team with these skills.
Spirituality had a significant influence on how participants made sense of their LLA 37 and their ability to participate in work. 38 Those better able to participate assumed greater responsibility for their own destiny, including reaching out for help and creating opportunities. These findings point to the important role that spirituality has in peoples’ lives, and opportunities for clinicians to consider how an individual’s spirituality can help facilitate or hinder work participation.37,38 Some researchers have encouraged clinicians to initiate conversations with open-ended questions, such as ‘Is religion or spirituality important to you as you cope with. . .?’ that may help identify how spirituality might negatively or positively impact rehabilitation.37,39 In similarly disabled populations, this sort of spiritual screening has been linked to improving understanding between those living with disability and clinicians, and facilitation of life adjustment, satisfaction, coping and resilience.37,40
For all participants, some form of support was required for work participation. Some benefitted from practical assistance with domestic and self-care activities which may have also provided connection and emotional support, making participants feel loved and cared for despite their amputation. For others, changing occupation and assuming a different work role commensurate with their current physical ability, required financial support. While organisations, such as CRP, have schemes in place providing capital for new business ventures, support was contingent on already having established a business. Many participants, therefore, borrowed money to establish their business despite financial risks and lack of formal business training. Rehabilitation services could look to provide start-up funding without this need to have already established a business. It is also critical to have capacity building that empowers beneficiaries to manage their financial obligations and develop business skills for long-term economic independence. 41
While the provision of a prosthesis may have aided mobility, it was often a hindrance to work participation given the constraints of prosthetic design within the Bangladeshi built and natural environment. Many activities are undertaken on the ground while squatting, a position which can be difficult to achieve given that prostheses typically lack the necessary ankle range of motion and unimpeded knee flexion. The use of home or workplace modifications which could make prosthesis use more functional was rare in our interviews; therefore, many participants performed these activities without their prosthesis.
Given that workplace modifications have been found to be a deciding factor facilitating work participation after LLA,9,42,43 there are opportunities for clinicians to talk with prosthesis users and employers about simple ways to adapt the built environment or task to facilitate participation. Those participants who were empowered to adapt their tasks or environment found greater independence. This is particularly important as research indicates that most adaptations or assistive technology are not provided by a rehabilitation service but made by the user or family.13,44
Many participants described experiences of work participation barriers consistent with bias and discrimination. Many disguised their limb loss until after they were successfully recognised as competent in their new role by their managers or co-workers. These experiences are not uncommon in the experience of disability and work participation30,38 and highlight opportunities for rehabilitation services to help address negative stereotypes associated with disability and create an informed understanding of the abilities of people with LLA within their communities.30,38,41
Limitations
The experiences described in this study reflect those of people living with traumatic LLA who received their prosthesis and rehabilitation through a single Bangladeshi, multi-site, service provider. The convenience sampling methodology likely favours those who were younger, healthier and able to participate.
The insights reported in this investigation do not reflect those of people living with LLA who are not aware of, or unable to, access the assistive technology and rehabilitation they require due to poverty or remoteness.6,44 We hypothesise that for these people, there may well be very different barriers to work participation than for those living with an amputation who have access to rehabilitation.
Given the intervening years since amputation and prosthetic fitting, our cohort are likely to experience very different facilitators and barriers to work participation than those living with a recent amputation without rehabilitation. While the experiences described in this study may not be transferrable to different cultures and systems of social support, it is important to recognise that many people living with LLA reside in countries not dissimilar to Bangladesh. As such, the facilitators and barriers to work participation identified may be applicable to people living in countries with similar cultures, systems of social welfare and built environments.
While great care was taken to design methods to engender confidence in the trustworthiness of these findings, it was not possible to undertake member checking within the constraints of this project. Many of the mechanisms typically available to qualitative researchers, such as participants reviewing their written summaries, were not possible given the low literacy levels of many of these participants.
Conclusion
This study described the experience of 10 adults living with LLA in Bangladesh who have accessed prosthetic services and rehabilitation. Their experiences highlight a wide range of facilitators and barriers to work participation that have not been well researched in this population, including spirituality, traditional gender roles, social supports, planning to overcome environmental and other challenges and ergonomic adaptations. Being aware of the complex interactions between such factors and the impact of physical disability, social supports and cultural norms can help clinicians reduce barriers that facilitate work participation. Given that many people living in Bangladesh with lower limb amputation do not have access to necessary rehabilitation and prosthetic services, there are opportunities to conduct similar research to identify barriers to work participation not identified in this research.
Footnotes
Acknowledgements
The authors thank the International Society for Prosthetics and Orthotics for their leadership in supporting research that can positively impact the quality of life for all those living with disability that require assistive technologies. They also thank the support of the Centre for Rehabilitation of the Paralysed, who collaborated in this research by supporting the researchers while in Bangladesh and facilitating access to participants. They thank the many participants who shared their experiences so as to help illuminate the barriers and facilitators to work participation following lower limb amputation and prosthetic rehabilitation.
Author contribution
All authors contributed equally in the preparation of this article.
Ethics review and approval
The study was approved by the La Trobe University Research Ethics Committee (S15/218) and the Centre for the Rehabilitation of the Paralysed (CRP) Ethics Committee (CRP-R&E-0401-151).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a research grant awarded to M.M.U., A.S.M.B., M.P.D., R.S. and E.F. by the International Society for Prosthetics and Orthotics, Australian National Member Society.