
Abstract
Background:
The Trinity Amputation and Prosthesis Experience Scales—Revised assesses adjustment to amputation and to using a prosthesis and considers psychosocial adjustment, activity restriction, satisfaction with the prosthesis, and other aspects related to health and physical activities, including residual and phantom limb pain.
Objectives:
The aim of this study was to assess the semantic equivalence of the Trinity Amputation and Prosthesis Experience Scales—Revised when translated into Brazilian Portuguese.
Study design:
Qualitative study.
Methods:
The process was conducted in five stages: translation of the questionnaire into Brazilian Portuguese; development of a first consensual version in Brazilian Portuguese; appraisal of the translation by an expert committee; back-translation; and semantics assessment of the instrument. For semantic evaluation, the translated and adapted Brazilian Portuguese versions were applied to a convenience sample of 10 individuals.
Results:
The translated instrument showed a high degree of comprehension within the target population, as it was observed all questions from Part I and II were score 4 or higher on an Ordinal Scale ranging from 0 to 5.
Conclusion:
The Brazilian version of Trinity Amputation and Prosthesis Experience Scales—Revised has a satisfactory verbal comprehension and is now ready for assessment of its psychometric properties.
Clinical relevance
The process of semantic evaluation of the Brazilian version of the Trinity Amputation and Prosthesis Experience Scales—Revised makes available to health professionals and researchers who work with people with amputations initial information on cross-cultural adaptation and degree of comprehension of this scale.
Background
Amputation is a public health problem that affects many countries and its etiology differs according to conditions of development of a country, because in developed countries vascular causes of amputation prevail and in developing countries traumatic causes predominate. 1 After the removal of a diseased limb, people with amputation may use a prosthesis, which can help improve body image, self-esteem, physical skills, and quality of life.2,3 In addition to physical adaptation, psychological and social adaptations are also needed to deal with multiple issues arising from lower limb amputation and the functional use of a prosthesis. 4
These issues associated with amputation should be considered important factors in the process of rehabilitation. According to Kageyama et al., 5 available instruments have different forms of evaluation, which makes comparing results difficult. Moreover, many researchers use scales or questionnaires designed for other clinical populations and adapt them to their studies, such as the Functional Independence Measure (FIM), Reintegration of Normal Living (RNL) Index, and Barthel Index; others develop instruments and evaluate their psychometric properties, such as the Prosthetic Profile of the Amputee (PPA), Prosthesis Evaluation Questionnaire (PEQ), Functional Measure for Amputees (FMA) Questionnaire, and the Trinity Amputation and Prosthesis Experience Scales—Revised (TAPES-R).4,5–11 However, studies on people with amputation in the Portuguese language of Brazil are lacking, due to an insufficiency of instruments that provide information about quality of life, physical activity 12 and satisfaction, fit, and use of the prosthesis. 13
The TAPES is an instrument used to evaluate the satisfaction and fit of the prosthesis, as well as the quality of life and physical activity of people with amputation. TAPES was developed by Gallagher and MacLachlan 4 in Ireland and had its initial version revised in 2010 by Gallagher et al., 14 creating the TAPES-R. The TAPES-R scale can be used to evaluate the quality of life during rehabilitation of those with limb amputation through several domains, which consider physical and psychosocial aspects that can have an effect on the individuals’ well-being. 15 These aspects represent a great benefit for this population since health professionals who interact with these individuals are able to understand their functional needs. While this scale has been validated and translated in several countries,16,17 it has not been translated for Brazil.
Therefore, considering that TAPES-R provides important information regarding the conditions associated with amputation, the lack of studies in Brazil with this population, and that this scale is not currently available in the language and culture of Brazil, it is believed that translation and semantic equivalence of TAPES-R is important in order to better understand the population of people with amputation in Brazil. Thus, the aim of this study was to assess the semantic equivalence of the TAPES-R when translated into Brazilian Portuguese.
Method
The study was submitted for consideration to the local Ethics Committee Research and was approved from National Research Ethics Commission. All subjects who participated in the study provided a written informed consent.
Instrument
The TAPES-R is divided into two parts, the first part refers to the psychosocial adjustment to use of a prosthesis, the limitations imposed by the use of a prosthesis and the satisfaction or dissatisfaction with a prosthesis. In the second part, the questions concern health, physical abilities, residual pain, phantom pain, other medical problems, and other types of pain with which the person with amputation may present. Beyond this, the instrument also includes some sociodemographic questions in relation to the amputation and prosthesis. The answers are summed and divided by the number of questions answered or applied in each of the three subscales. Higher scores are indicative of better psychosocial adjustment. 14
The subscale of activity restriction questions the subject regarding the limitations imposed by the prosthesis in performing activities that could be done during a normal day. Higher scores indicate greater limitation. The questions regarding satisfaction with the prosthesis are divided into aesthetic satisfaction and functional satisfaction. The subject is questioned about how satisfied he is in relation to color, shape, appearance, weight, confidence, fit, and comfort. Higher scores indicate a better satisfaction with the prosthesis.14,15
Translation and cross-cultural adaptation process of TAPES-R
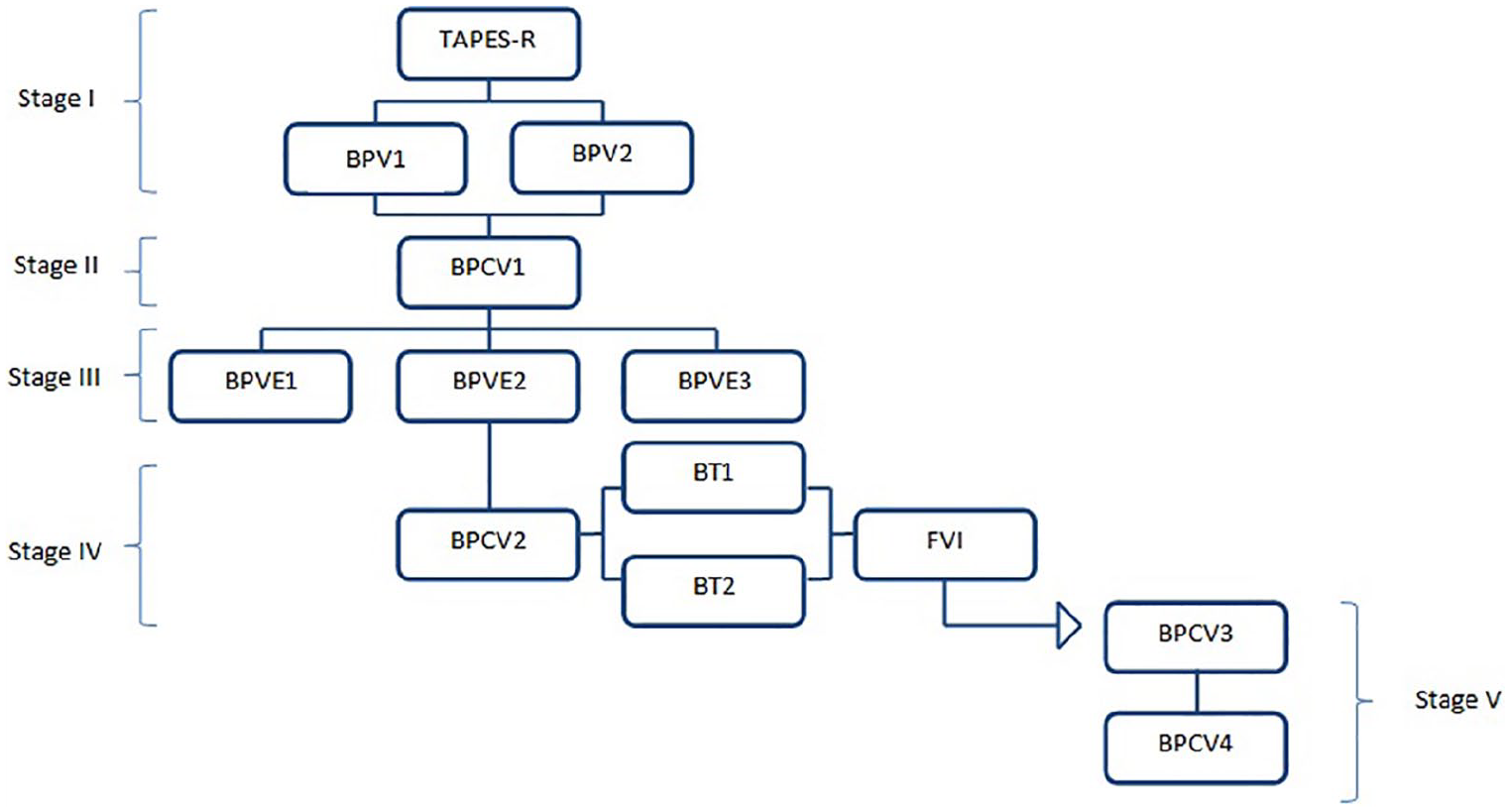
The translation and cross-cultural adaptation process of TAPES-R was performed according to the methodology proposed by Beaton et al. 18 (Figure 1), as described in the following paragraphs.
Stage 1. Translation of the questionnaire into Brazilian Portuguese: Two Brazilian nationals, fluent in the English language, translated the questionnaire into Brazilian Portuguese. One of the translators was a health specialist and the other was a layperson, that is, a translator with no experience translating medical or clinical documents. The layperson was included as they were likely to be less influenced by the research goal and would offer a translation that reflected the language used by the general “lay” population. Each translator independently produced a translation into Brazilian Portuguese, and this stage was completed with two versions of the questionnaire in Brazilian Portuguese (Brazilian Portuguese Version 1 (BPV1) and Brazilian Portuguese Version 2 (BPV2)).
Stage 2. First consensual version in Brazilian Portuguese: In order to obtain the first consensual version in Portuguese, those involved in the research met with the translators and evaluated the two translations produced in stage 1 (BPV1 and BPV2). The translated versions were compared, in order to identify any discrepancies in meaning and context. After analyzing these differences, a single translation was produced, in which the expressions chosen were those which were considered best suited to the population, with no interference in the meaning of the scale. This stage was completed by obtaining a consensual version in Brazilian Portuguese (Brazilian Portuguese Consensual Version 1 (BPCV1)) approved by all professionals involved (i.e. translator from the health sector, lay translator, and researchers).
Stage 3. Appraisal by an expert committee: This stage involved submission of the BPCV1 to an expert committee for appraisal of the adaptation process. The criteria for the selection of the committee included knowledge of the subject in question (limb amputation and prostheses) and fluency of Portuguese and English. The committee was composed of three experts, who were informed of the objective of the study, namely, to assess the semantic equivalence of the TAPES-R when translated into Brazilian Portuguese. The professionals had no access to the original instrument—only the consensual version 1—in order to avoid being influenced by the expressions used in the original scale. Each practitioner provided their own considerations regarding the semantic, idiomatic, cross-cultural, and conceptual equivalence of BPCV1. Thus, an individual appraisal (BPVE) of the translated instrument from stage 2 was obtained from each member of the expert committee. After considering and discussing the three BPVE, the researchers produced a second consensual version in Brazilian Portuguese (Brazilian Portuguese Consensual Version 2 (BPCV2)). All members of the expert committee also reached a consensus on face and content validity by discussing the BPCV2. In order to verify face validity, whether the translated version of TAPES-R evaluated what it proposes to measure was discussed and, regarding content validity, how much the scale items represented the entirety of its content was discussed.
Stage 4. Back-translation: The second consensual version (BPCV2) was independently translated back into English by two translators for whom the source language (English) was their first language. These translators were not informed about the scale and respective objectives. After back-translation, two versions in English (Back Translation 1 (BT1) and Back Translation 2 (BT2)) were produced. In a new meeting of the researchers and translators, the objectives of the study and analysis of the translations were discussed and a final English version (FV1) was produced through consensus, which was compared with the original instrument in the English language. Finally, the committee compared BPCV2 with FV1, to obtain a third consensual version of TAPES-R (Brazilian Portuguese Consensual Version 3 (BPCV3)) which was agreed to by all the researchers and translators.
Stage 5. Semantic assessment of the instrument: Semantic analysis was performed through the presentation of the scale to 10 persons with amputation, who were chosen in an intentional non-probabilistic manner. The inclusion criteria for subjects consisted of individuals using a lower limb prosthesis (unilateral or bilateral), of at least 18 years of age, of both genders, and who took part in the programs conducted by the Rehabilitation Center of Santa Catarina or the Sport and Health Sciences Center of Santa Catarina State University (CEFID/UDESC). Individuals who could not provide informed consent or complete the questionnaire due to cognitive issues or other physical issues beyond the lower limb amputation, were not included in the study.
Cross-cultural adaptation process of TAPES-R.
Initially, a form with sociodemographic data related to amputation was completed in order to characterize the participants. Afterward, each subject was individually questioned by the researcher regarding their degree of verbal comprehension of each item of the Brazilian version of TAPES-R with a standardized question “Do you understand what is being asked?” This question was applied for each item of the TAPES-R and the response options were evaluated according to a six-point ordinal scale, shown in Figure 2. The questionnaires were administered by the researches in interview form.

Ordinal scale—degree of comprehension of each item of the instrument.
The subjects were informed of the objective of this stage, namely, to assess the clarity and understanding of the scale items and to suggest possible changes. To be considered acceptable, each question was required to have a degree of understanding of 4 points or more on the scale, questions with comprehension scored less than 4 on the scale were modified.
The data obtained in this step were entered into an Excel® (2010, Microsoft, Redmond, WA, United States) spreadsheet, and descriptive statistical analysis was performed using the Statistical Package Social Science (SPSS) version 20.0 (IBM, United States). For analysis, mean and standard deviation, absolute frequencies, and relative frequencies were applied to characterization of subjects and to the items of semantic evaluation. After the BPCV3 was assessed with the participants with amputation and its results analyzed, a new meeting was held between the researchers in order to evaluate the degree of comprehension of the subjects in each TAPES-R question and the need for any other changes to the instrument in order to facilitate their understanding, reaching the end of this stage with the consensual version number 4 (Brazilian Portuguese Consensual Version 4 (BPCV4)).
Results
The sample consisted of 10 Brazilian individuals with lower limb amputation (7 men and 3 women, mean age of 45.30 ± 14.20 years, ranging between 26 and 66 years, average of 11.57 ± 10.43 years since amputation, average time of use of prosthesis of 11.46 ± 10.48 years, and average of 3.5 ± 4.8 years of current prosthesis use). The education levels of the subjects were as follows: illiterate (n = 1), incomplete basic education (n = 4), complete basic education (n = 2), complete secondary education (n = 2), and incomplete higher education (n = 1). The characteristics related to the cause of amputation, level of amputation, general health, and physical capabilities according to gender are shown in Table 1.
Characteristics related to the cause of amputation, level of amputation, and classification of general health and physical capabilities of subjects by gender (male and female).
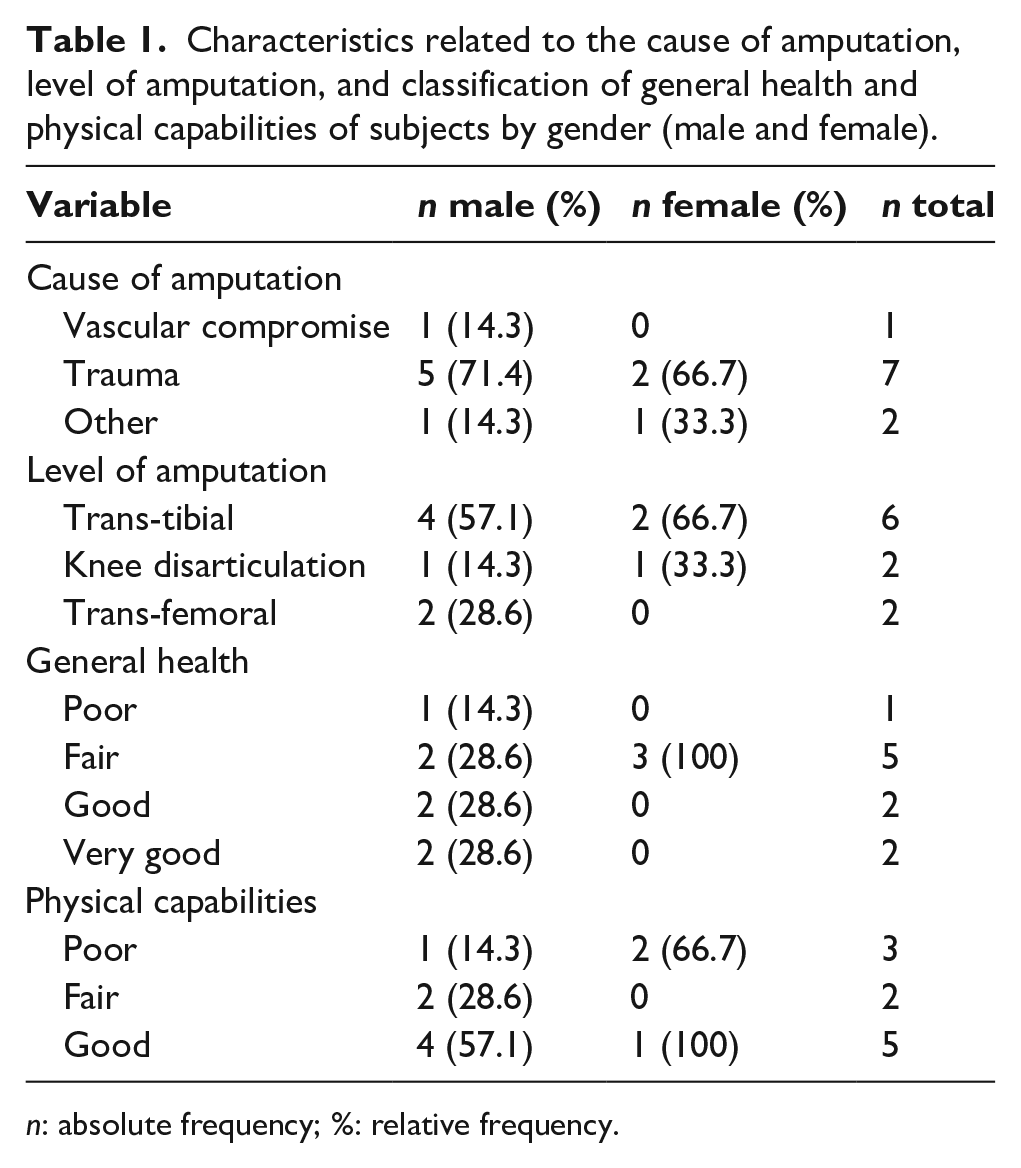
n: absolute frequency; %: relative frequency.
Small changes identified in the process of translation, back-translation, and definition of the consensual version in Portuguese were necessary, to facilitate understanding of subjects who would respond to the instrument. Minor changes were also made in the semantic evaluation, as described in Table 2.
Modifications performed in the scale to increase the level of understanding.
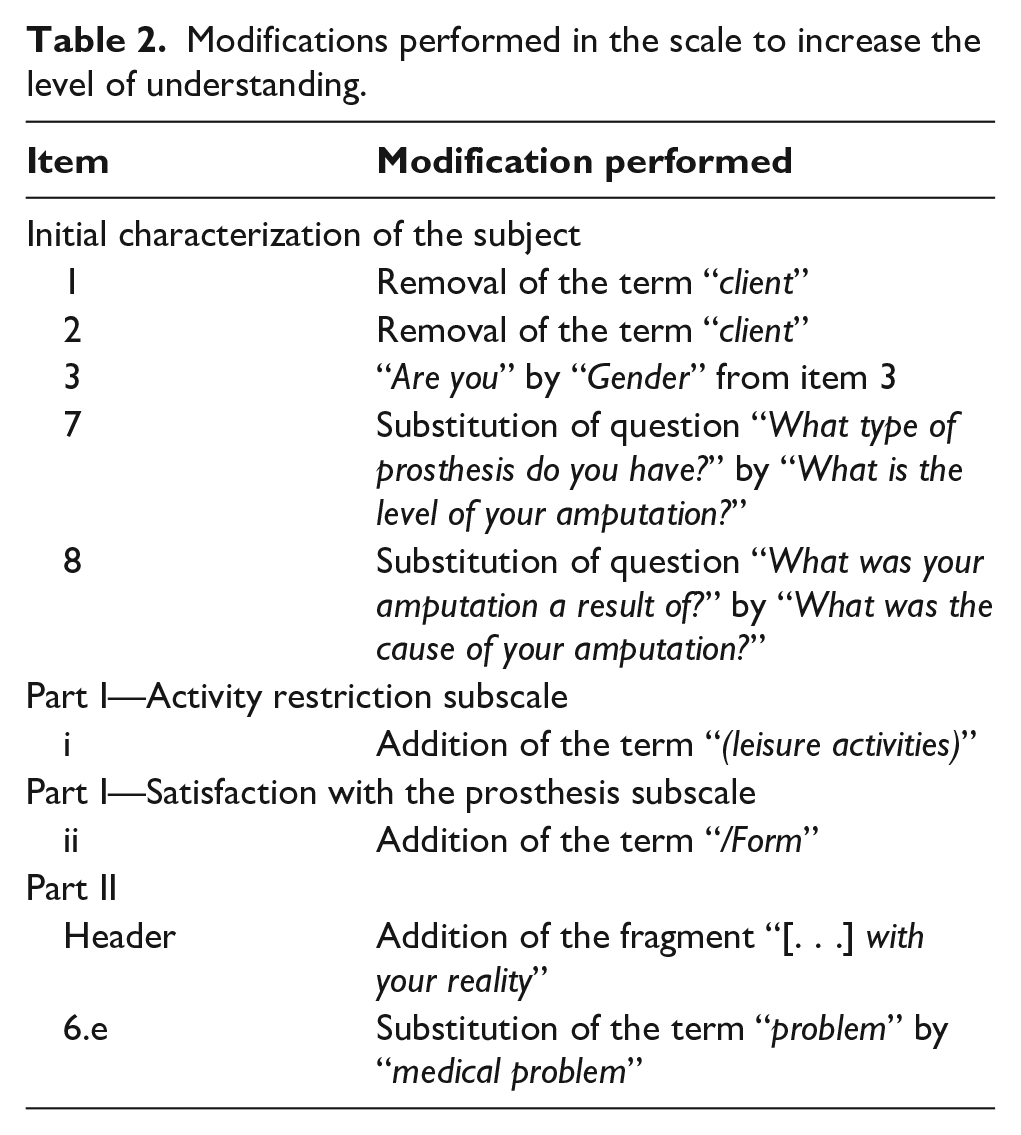
Some words were changed during the translation and back-translation process (stages 1–4), so as to facilitate the understanding of the subjects and make the instrument comprehensible in the Brazilian language. Item “Part I—11” where it says “A prosthesis interferes with the ability to do my work” was adapted to “The prosthesis interferes with my capacity to work.” In item 12, there was modification of the original version “Having a prosthesis makes me more dependent on others than I would like to be” to the back-translation version “Using a prosthesis makes me more dependent on others than I would like to be.” Another item was also clarified through back-translation by modifying “Being an amputee means that I cannot do what I want to do” to “Being an amputee means that I cannot do what I would like to do.” Other words were changed throughout the translation process, but were changed without any modifications in the sense of the phrase, as occurred in item 13: “Having a prosthesis limits the kind (type) of work that I can do.” In the original version the word “kind” was used, and in the backward version it was replaced by “type.” No further modifications were necessary for translation into Portuguese.
In the semantic evaluation (stage 5), it was observed that, for Part I and Part II, all questions obtained a degree of understanding of 4 points or more on the scale. It wasn’t observed questions with a comprehension score less than 4 on the scale (Tables 3 and 4).
Evaluation of verbal comprehension of the items of Part I from the Brazilian Portuguese version of the Trinity Amputation and Prosthesis Experience Scales—Revised (TAPES-R) (BPCV3).
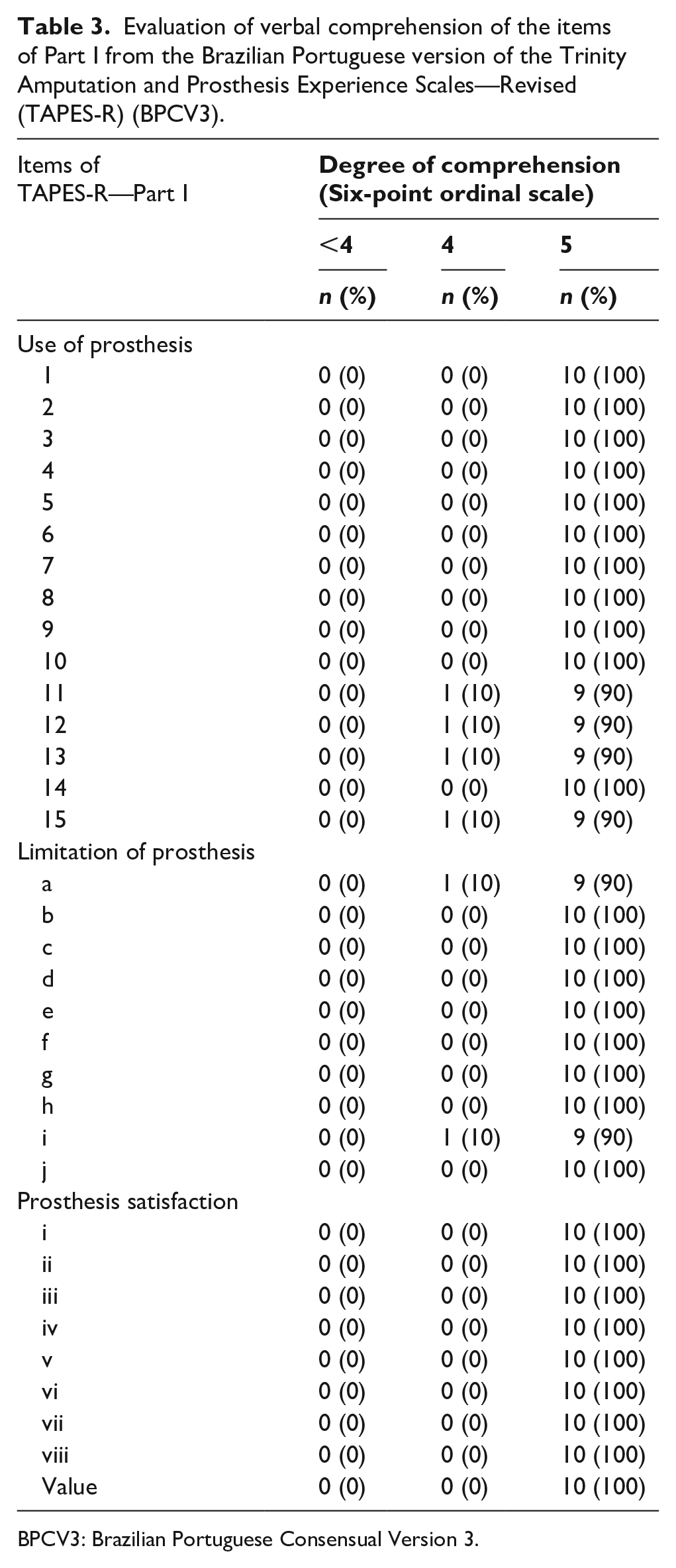
BPCV3: Brazilian Portuguese Consensual Version 3.
Evaluation of verbal comprehension of the items of Part II from the Brazilian Portuguese version of the Trinity Amputation and Prosthesis Experience Scales—Revised (TAPES-R) (BPCV3).
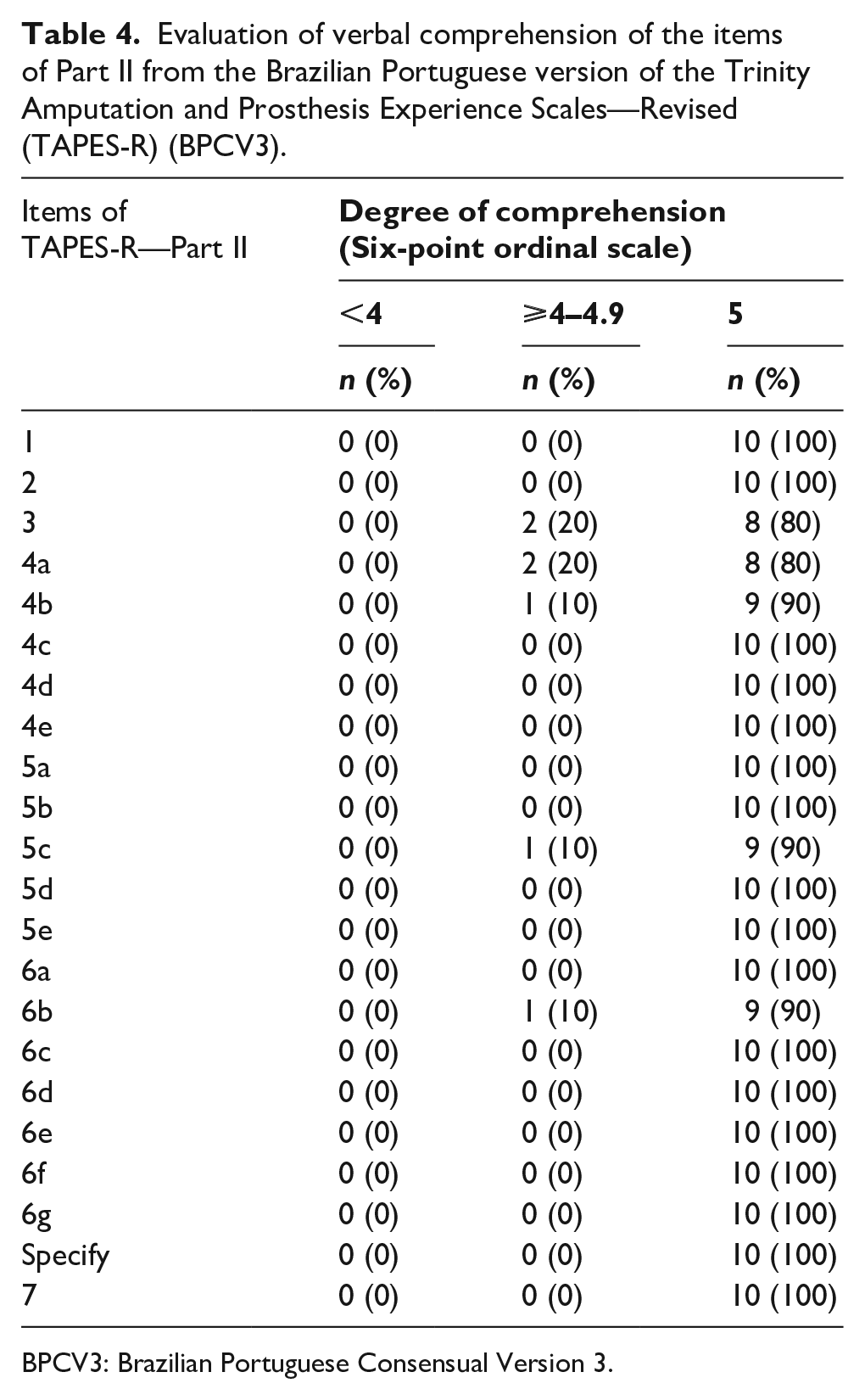
BPCV3: Brazilian Portuguese Consensual Version 3.
Discussion
The aim of this study was to evaluate the semantic equivalence of the Portuguese–Brazilian version of the TAPES-R scale. It was observed that the Brazilian version of TAPES-R was comprehensible to a sample of persons with lower limb amputation with different age, sex, and level of education. The translation process aimed to replicate the intent of the original wording but in a way that the terms used in the adapted version reflect the reality of the country in which the instrument will be applied. To do this, the recommendations by Beaton et al. 18 were used, who suggested that in the first stage, at least two translations be made of the instrument from the source language into the target language. After this process, the evaluation by a committee of experts was recommended by Beaton et al. 18 to ensure identification of errors or comprehension problems, which could be modified in the translated version before being back-translated. Finally, alterations in the translation were compared to the source language of the instrument, with the goal of maintaining the fundamental characteristics of the concepts found in the original version.
Even though no consensus exists on strategies for cross-cultural adaptation, studies advocate the operational stages used in this study for the adaptation of instruments.19–21 The assessment of semantic equivalence is one of the stages of cross-cultural adaptation of instruments that allows researchers to verify whether the concepts of an original instrument have been replicated for another culture, so that they can be equally understood in both cultures. 21 When two terms have the same meaning referenced in the original instrument, we conclude that they have semantic equivalence. 21
The analysis of semantic equivalence was based on the degree of verbal comprehension of persons with lower limb amputation, which was considered to be satisfactory. Therefore, this confirmed that the translation of the scale showed high level of semantic equivalence for the target population. Silva et al., 22 who checked the semantic equivalence of the Brazilian version of the Online Cognition Scale, also found a satisfactory comprehension for this scale following a similar methodology as our study.
As in the study by Amaral et al., 23 in our study no items of the scale were excluded. In our study, the objective was that there would be no modification of the intention of the original instrument beyond the necessary changes of some words. In order to achieve this goal, some words were changed during the translation and back-translation process (stages 1–4), so as to facilitate the understanding of the subjects and make the instrument comprehensible in the Brazilian language. Similar wording changes were observed in a study conducted by Lins et al., 20 who performed the translation, cultural adaptation, and validation of the celiac disease DUX (CDDUX) for Brazil. They adjusted expressions of the original instrument according to the needs of the Brazilian population, emphasizing the importance of these adjustments in the cross-culturalization process.
Cross-cultural studies not only allow us to verify differences between individuals and cultures, but to also understand similarities and common characteristics. In this way, every translated instrument can be adapted to the culture for which it is being used, in this case for the Brazilian population, but hopefully resulting in the same effect that the original instrument was intended to have in the context in which it was created. Lack of transcultural equivalence compromises the validity of the information collected, making it impossible to use an instrument to study a concept correctly. 24 Therefore, it is necessary to have more and more instruments undergo a rigorous process of adaptation and evaluation of the semantic characteristics of the translated instrument, to ensure that the instrument is able to be used adequately in the new social and cultural context. 24
This study only describes the first stages of the process of translation with cross-cultural and semantic equivalence. Future studies are needed to verify psychometric properties of the translated instrument. The findings of this study suggest that the translated TAPES-R has sufficient semantic equivalence to be understood by Brazilian people who have lower limb amputation.
Conclusion
It may be concluded that the Brazilian version of TAPES-R has satisfactory verbal comprehension and is ready for additional study of its psychometric properties in Brazilian Portuguese speaking people with lower limb amputation.
Footnotes
Author contributions
All authors contributed equally in the preparation of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was submitted for consideration to the local Ethics Committee Research and was approved under CAAE protocol number: 24550114.3.0000.0118 from National Research Ethics Commission from Ministry of Health of the Brazil. All subjects who participated in the study provided a written informed consent.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.