
Abstract
Background:
Protective knee braces are used for rehabilitation or prevention. Due to poor patient compliance or slippage, the brace might be misaligned with the knee axis.
Objectives:
Does a misaligned knee brace stress the anterior cruciate ligament?
Study design:
It is an experimental study.
Methods:
A strain sensor was implanted on the anterior cruciate ligament in eight limbs. The limbs were mounted in a knee simulator, muscle forces were applied and a cyclic motion from 10° to 60° flexion was performed under three conditions: unbraced, braced and with a misaligned brace.
Outcome measures:
The outcome measures were anterior cruciate ligament strain and three-dimensional kinematics of the knee joint.
Results:
The correctly aligned brace significantly reduced the anterior cruciate ligament strain at 10° compared to the unbraced condition from 0% to −1.54% (standard deviation = 1.4). The misaligned brace neutralised the effect of bracing to −0.06% (standard deviation = 1.1) anterior cruciate ligament strain. At 60° flexion angle, bracing had no statistically significant effect on the anterior cruciate ligament strain compared to the unbraced knee: −2.58% (standard deviation = 0.8) versus −1.64% (standard deviation = 1.0). The anterior cruciate ligament in the misaligned braced knee at 60° flexion with a strain of −1.1% (standard deviation = 0.9) was significantly more stressed than in the correctly aligned condition. An effect of bracing on knee kinematics was not detected.
Conclusion:
A correctly aligned knee brace reduced anterior cruciate ligament strain. By contrast, a misaligned brace tended to increase the anterior cruciate ligament strain compared to the unbraced knee.
Clinical relevance
The correct alignment of the brace was identified as a key factor decisively influencing the effectiveness of bracing.
Background
Knee braces are frequently prescribed by physicians to prevent the knee joint from damage after surgery. This is particularly true following reconstruction of the anterior cruciate ligament (ACL), although the long-term effectiveness of bracing after ACL surgery could not be demonstrated in various studies.1–5 In addition, athletes participating in contact sports or sports with fast cutting may wear prophylactic knee braces to protect against ACL ruptures, one of the most prominent injuries in athletes.6–8 Studies about a protective effect of these braces against unphysiological loadings in sports are controversial.9–14 However, in vitro studies did demonstrate that bracing could protect the ACL and medial collateral ligament against lateral impacts.15,16 Furthermore, a study by Tomescu et al. 17 supported the use of a brace with a dynamic tensioning system for ACL-deficient knees.
Knee kinematics is complex, with six degrees of freedom, including flexion/extension, adduction/abduction and internal/external rotation. 18 After flexion and extension, tibial rotation is the most prominent rotation. This rotation is coupled to the flexion angle, 19 such that the knee performs an external rotation of approximately 10° when it is extended from 30° to 0° flexion angle. 20 As a result of this overlapping motion of flexion/extension and internal/external tibial rotation, the physiological finite rotation axis is skewed over a rotation of 30° to 0° flexion angle.
In contrast to the knee, brace kinematics is less complex. In general, braces consist of two rigid frames that are connected via a polycentric hinge and strapped around the thigh and shank, respectively. Because of the polycentric hinge, the tibial frame performs a translational movement relative to the femoral frame during flexion. In a pretest, we assessed the rotation axis of knee braces and found that the finite rotation axis moved translationally within the sagittal plane and did not tilt in contrast to the finite rotation axis of the physiological knee joint. This result could be expected, because of the simple brace-joint mechanics, which are equal on both sides. Therefore, it cannot mirror the tibial rotation of the knee, typically occurring between 30° and extension, so that the brace is misaligned during this specific motion (Figure 1).
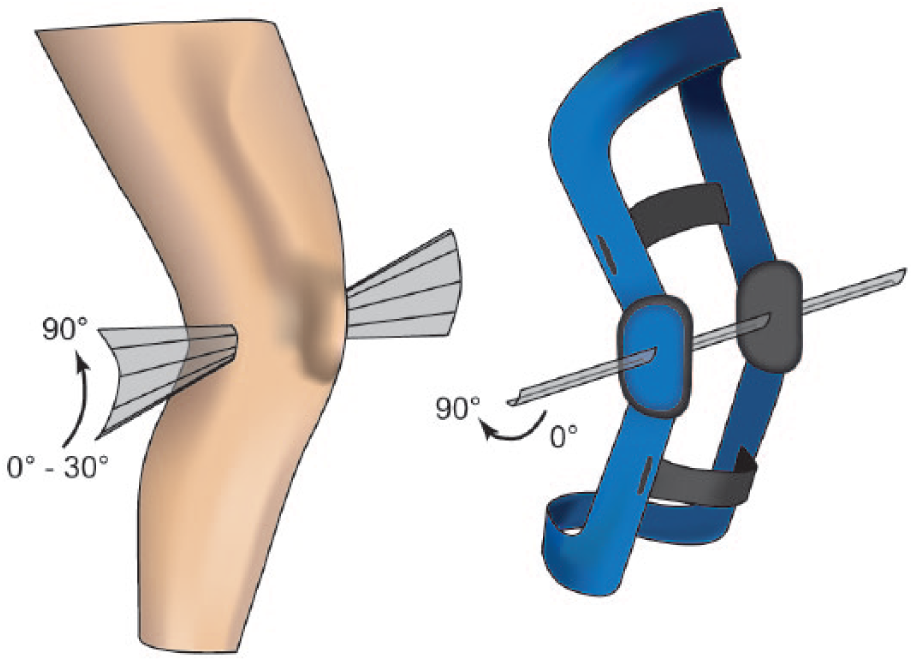
Exemplary scheme of the rotation axes of the knee joint (left) and a functional brace (right). The physiological rotation axes are slightly tilted in the vertical plane between 0° and 30° flexion angle, whereas the rotation axes of the brace are parallel throughout the entire flexion.
Another effect that causes misalignment and leads to discomfort issues is brace slippage. 21 A study by Brownstein 22 found a maximal migration of 11 mm after only 15 min of exercises. The misalignment of the rotation axes of knee and brace caused by the different kinematics and through brace slippage might influence structures within the knee. This research question was investigated by Regalbuto et al., 23 where the misalignment of brace and knee joint induced mechanical forces in the frame of the brace. The authors concluded that this could lead to adverse internal joint mechanics. Another study by Singer and Lamontagne 24 found no effect of brace migration on the kinematics or net joint moments.
However, the effect of brace misalignment on the inner knee structures, particularly the ACL, has not yet been specifically investigated. With the different kinematics of the physiological knee and brace in mind, we performed this study to answer the question if a misaligned knee brace stresses the ACL.
Materials and methods
ACL strain and knee joint kinematics were obtained in eight leg specimens (2 males, 6 females; age 70 ± 12 years; Science Care, Phoenix, AZ, USA) during five consecutive squats simulated in a knee simulator. Based on the results of another study investigating the ACL strain in the braced and unbraced knee, 25 an a priori power analysis was performed with type 2 error set to 5% and 80% power to calculate a sample size of seven, which was increased to eight specimens. This research was approved by the Ethics Committee at Ulm University (No. 207/16).
Preparation
Eight fresh frozen specimens were used for this study. Specimens were thawed overnight at room temperature. To measure ACL strain, a differential variable reluctance transducer (DVRT; Microstrain, Williston, VT, USA) was used. The knee capsule was opened, and muscles and fat tissue were carefully dilated. A notch plastic surgery was performed to avoid impingement of the DVRT with the intercondylar roof. The DVRT was then pinned on the anteromedial bundle of the ACL and secured with cross-stitches to avoid sensor slippage. To simulate muscle forces, two Bowden cables were pierced through the posterior and anterior soft tissue of the thigh, respectively. A steel cable was pulled through the anterior Bowden cable and crimped to a perforated metal plate. This plate was then sutured to the patella tendon to simulate the quadriceps muscles. Another cable was pulled through the posterior Bowden cable and anchored in the tibia 30 mm below the joint space to simulate hamstring muscles. During the entire preparation, the soft tissue was maintained intact as far as possible. Following placement of the sensors, soft tissue and skin were carefully sutured at the position of the insertion.
To assess knee kinematics, two Schanz screws were drilled one each into the tibial and femoral bone, respectively, and a lockable ball joint was mounted onto each pair of screws. A coordinate system with reflective markers was attached to the ball joint and aligned with the anatomical joint axes defined by Grood and Suntay. 26 Finally, both the tibia and femur were dissected at a distance of approximately 500 mm from the joint space. Both bones were cleared of soft tissue at the dissection cut, skin was laced up and the bare tibial and femoral bones were both cemented in polymethyl methacrylate (Technovit®; Kulzer, Wehrheim, Germany) (Figure 2).
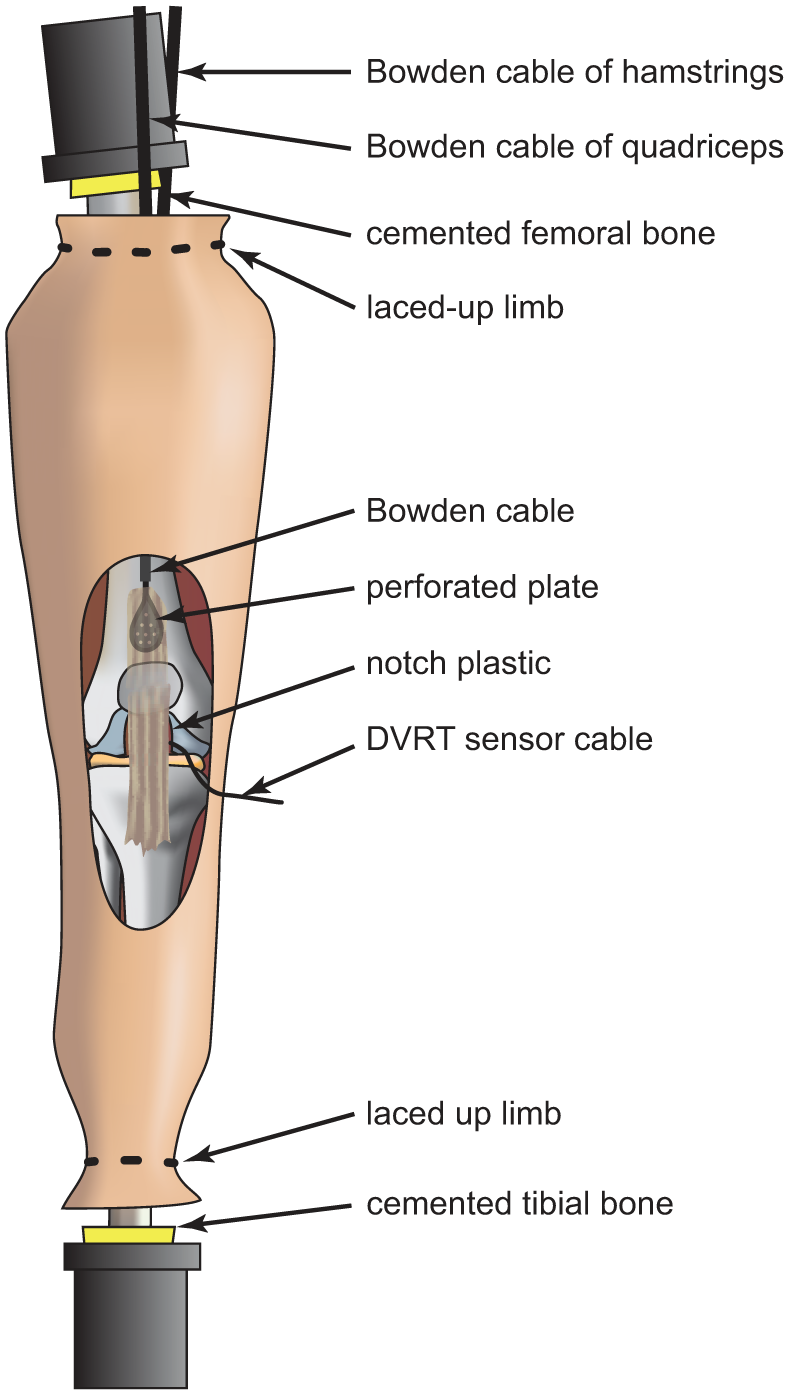
Prepared limb with the patella tendon sewn to a perforated metal plate that is crimped to a Bowden cable. The DVRT strain sensor is placed on the ACL while a notch plastic prevents the sensor from scratching the bone.
Test setup
The prepared limbs were mounted in a knee simulator. Moderate muscle forces were applied using the previously implanted steel cables with a force of 100 N simulating hamstring muscles and a force of 150 N simulating quadriceps muscles. The mechanical hip joint of the knee simulator consists of a Cardan angle that allows flexion/extension and abduction/adduction. The ankle is imitated by another Cardan ankle with all three rotational degrees of freedom.
The knee was flexed from 10° to 60° and back to 10° flexion angle, simulating the range of motion during normal walking, 27 for five cycles in unbraced, braced and braced but 20 mm distal migrated conditions with a speed of 20°/s (Figure 3). The brace (4TITUDE; DJO Global, Inc., Vista, CA, USA) was strapped according to the manufacture’s instructions.
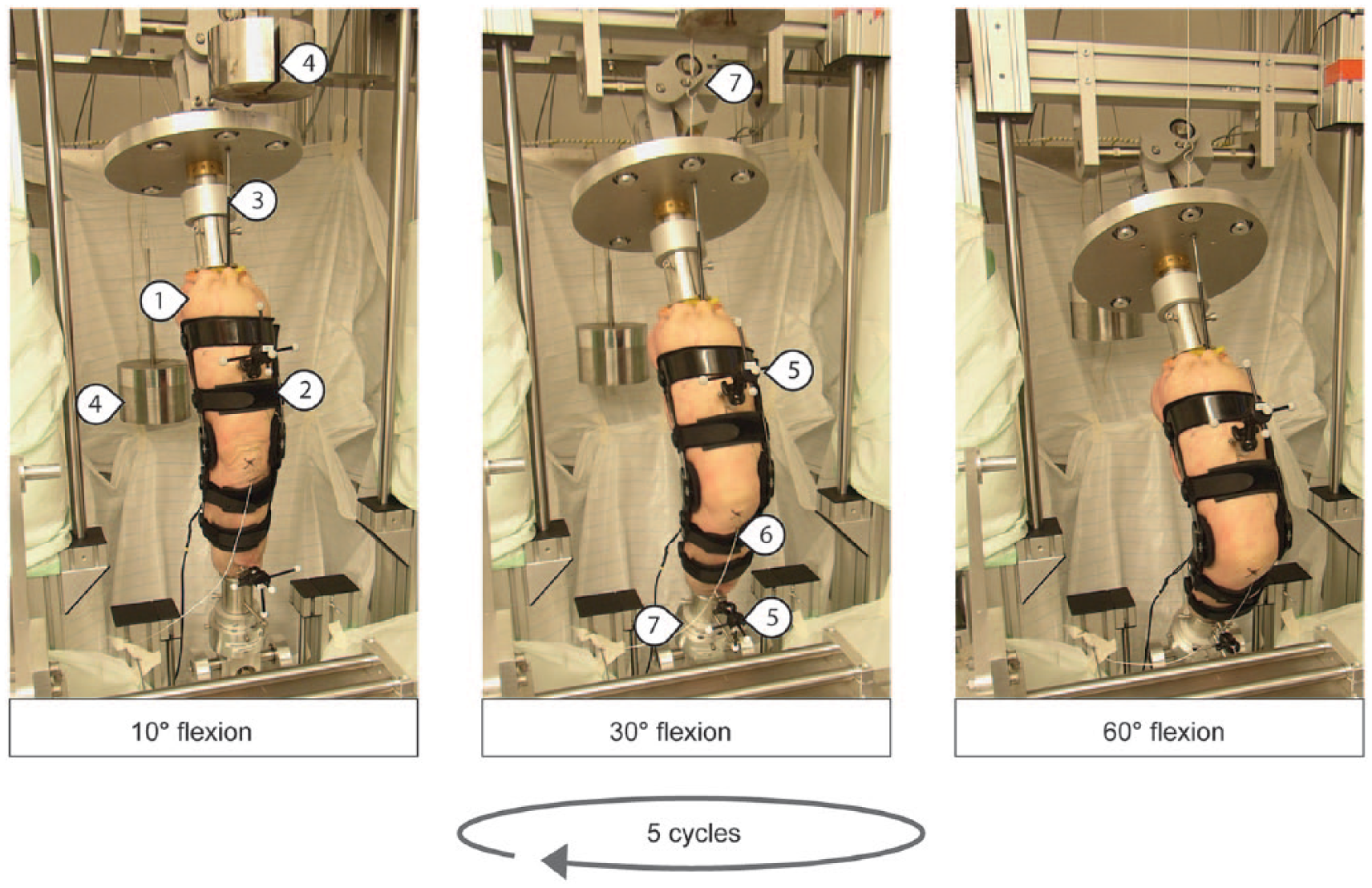
The limb (1) was mounted in a knee simulator and continuously moved from 10° to 60° and back to 10° flexion angle for five cycles, for the unbraced, braced (2) and 20 mm distally braced condition. Hamstring and quadriceps muscle forces are simulated with Bowden cables (3) and weights (4) that are pierced through the soft tissue along the physiological muscles. Two coordinate systems (5) with retroreflective markers were drilled in both the femoral and tibial bones to measure knee kinematics. The sensor cable of the DVRT (6) was carefully led through the skin and secured with cross-stitches. The hip and ankle were simulated with Cardan joints (7).
Data analysis
ACL strain was recorded at 1000 Hz using custom-developed software in LabVIEW (National Instruments; Austin, TX, USA). The kinematics was recorded using 9 three-dimensional cameras (Prime 13, Optitrack; NaturalPoint Inc., Corvallis, OR, USA) at 240 Hz with an error of <0.3 mm. The kinematics was computed as described by Grood and Suntay, 26 with a custom script in MATLAB 2017a (The MathWorks, Natick, USA).
The DVRT sensor continuously recorded the ACL length during five cycles, with only the final cycle used for data analysis. The ACL strain
Statistical analysis was performed in MATLAB with the built-in statistical toolbox. The data were analysed according to Beynnon et al.25,28 with a Student’s paired t-test and a level of significance of alpha = 0.05.
After the first two specimens were tested, we analysed the data and found that the pins of the DVRT that were pierced through the ACL were too long, causing an impingement of the pins with the tibia plateau. This influenced the DVRT accuracy and was consequently corrected for the following tests. For this reason, we decided to exclude the first two specimens from the ACL strain analysis. Therefore, all eight specimens were used for the kinematic analysis but only six for the ACL strain analysis. All data are presented as the mean and standard deviation (SD).
Results
ACL strain
The ACL strain at 10° flexion angle was significantly reduced by the correctly aligned brace to a mean of −1.54% (SD = 1.4, 95% confidence interval (CI) = −2.9% to −0.1%) (Figure 4). The misaligned brace slightly, but non-significantly, decreased the ACL strain at 10° flexion to a mean of −0.06% (SD = 1.1). The ACL in the unbraced condition at 60°, with a mean of −1.64% (SD = 1.0, 95% CI = −2.7% to −0.6%), was significantly more relaxed than at 10° flexion. Bracing did not significantly reduce the ACL strain compared to the unbraced condition at 60°, with −2.58% (SD = 0.8). In the misaligned condition, the ACL tended to be more stressed at 60°, with an ACL strain of −1.13% (SD = 0.9), compared to the unbraced knee. This effect was not statistically significant. The ACL strain in the misaligned condition at 60° was significantly higher than in the correctly aligned condition (95% CI = −2.1% to −0.1%).
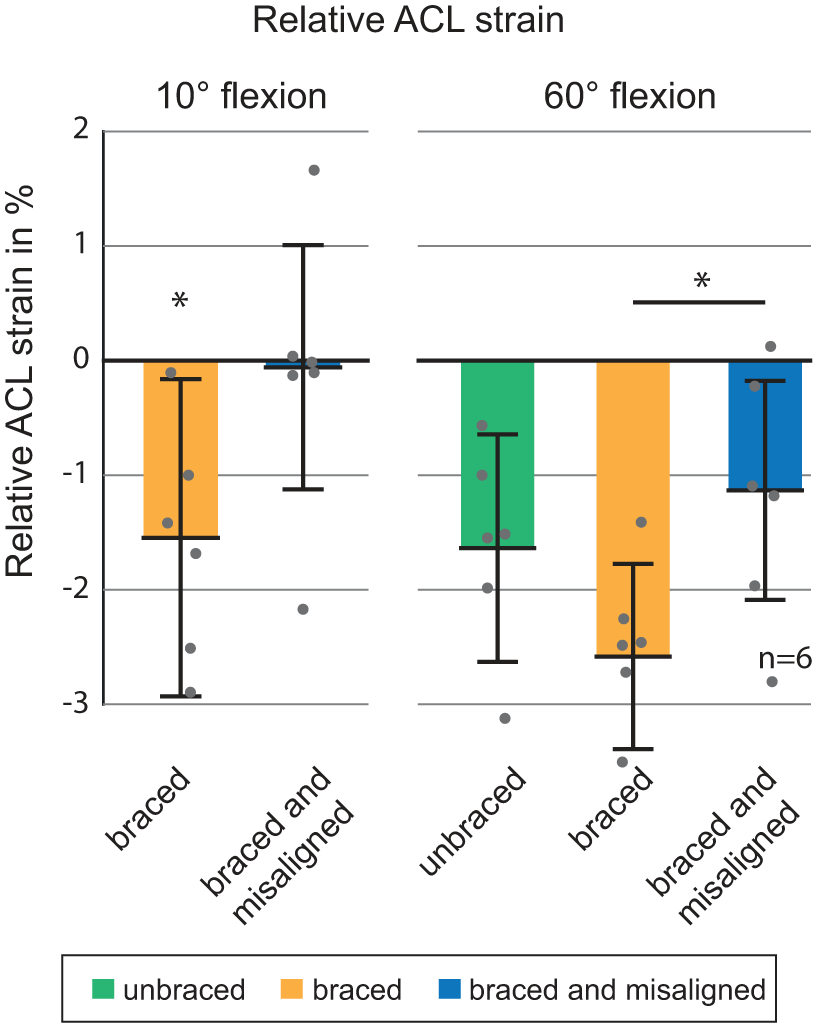
ACL strain at 10° flexion and 60° flexion for the three tested conditions: unbraced, braced and braced but 20 mm distally misaligned. The ACL strain at 10° flexion for the unbraced knee was defined as 0% baseline. Error bars represent standard deviation. *p < 0.05.
The ACL strain as a function of the flexion angle is presented in Figure 5. Bracing reduced the mean strain of the ACL during the complete cycle compared to the unbraced condition. By contrast, the misaligned brace tended to induce an increasing ACL strain and was significantly higher than the ACL strain with the correctly aligned brace from 50° to 60° flexion angle.
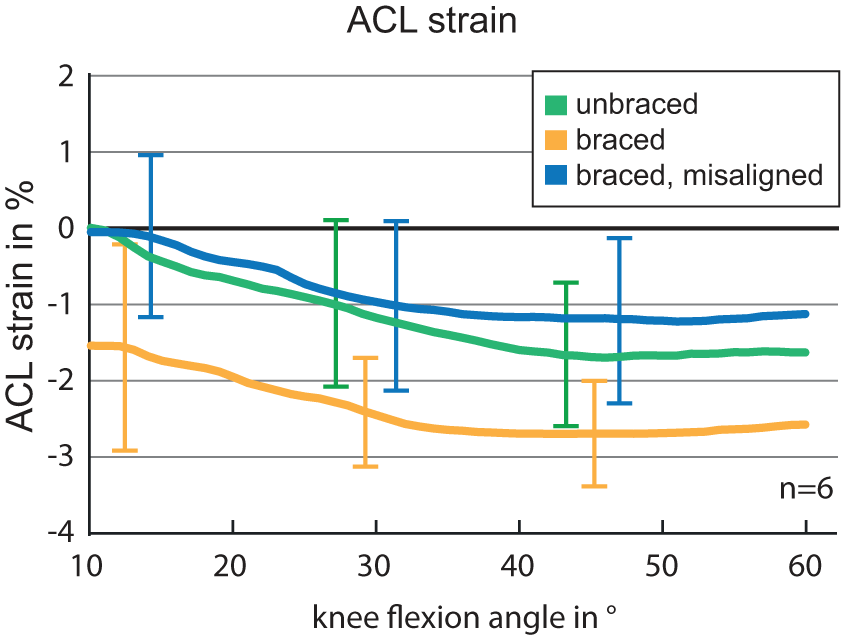
ACL strain as a function of the knee flexion angle for the three tested conditions: unbraced, braced and braced but 20 mm distally misaligned. Error bars represent the standard deviation at several data points.
Kinematics
The mean abduction angle during the squatting cycle was 6.8° (SD = 6.9°) for the unbraced, 7.2° (SD = 6.6°) for the braced and 7.4° (SD = 6.4°) for the braced and misaligned conditions (Figure 6). The unbraced knee performed a mean internal rotation from 10° to 60° flexion angle of 4.0°, the braced knee of 3.2° (SD = 7.4°) and the knee with a misaligned brace internally rotated 3.3° (SD = 6.6°). There were no statistically significant differences between the kinematics for any of the three scenarios.
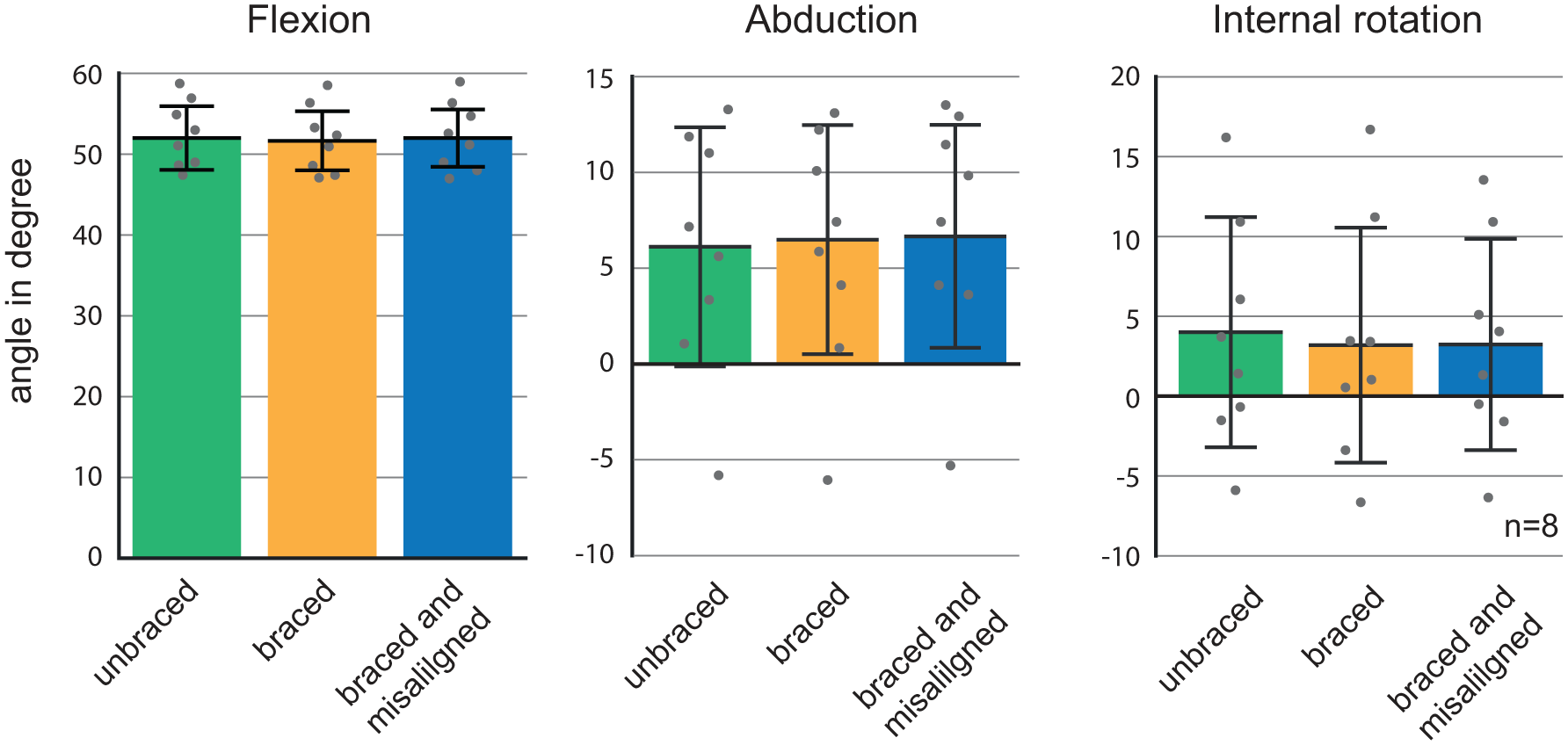
Kinematic analysis of the knee joint motion: flexion, adduction and external rotation for the three tested conditions. There are no statistically significant differences between the kinematics of each condition.
Discussion
In the present study, the ACL strain and kinematics were obtained in six and eight limb specimens, respectively, during five cyclic squats in the unbraced, braced and braced but 20 mm distally misaligned conditions. The overall gradient of the ACL strain versus flexion curve was similar to the in vivo findings of Beynnon et al., 29 with a decreasing ACL strain from 10° to 40° flexion and an almost constant strain from 40° to 60° flexion. However, the maximal stress release of the ACL during flexion in the unbraced condition was lower in the present study than that of Beynnon et al., with 1.5% versus approximately 4%. This might be explained by the applied muscle loads, which were most likely higher in vivo compared to the loads that we were able to simulate in vitro. However, our results are similar with the in vitro study of Dürselen et al., 30 who reported a linear strain release of 2% between 10° and 40° flexion without muscle forces.
In vivo studies by Beynnon et al. 25 and Fleming et al. 31 investigated the effect of bracing on the ACL strain during internal and external moments on the tibia and anterior–posterior shear load in patients undergoing arthroscopic surgery. Both found that a correctly aligned brace reduced the ACL strain when no external loads were applied, which is similar to our findings. In addition, our results are in line with those of Tomescu et al., 17 who found that bracing significantly reduced the ACL strain by 83% in a double-leg squat and 38% in single-leg squat in vitro.
Unfortunately, knee brace misalignment occurs frequently. This results from migration of the brace during daily exercises, as found by Brownstein, 22 or by poor patient compliance, such that the brace is already misaligned during placement of the brace when fastening the Velcro strips. For this reason, we investigated the effect of a brace that was 20 mm distally migrated during a normal gait cycle, simulating a worst-case scenario. Our results indicate that a misaligned brace neutralises the stress-decreasing effect on the ACL of a correctly aligned brace. Consequently, correct alignment of a knee brace was identified as a key factor that decisively influences the effectiveness of bracing.
Bracing had no effect on the kinematics of the knee. This might be explained by soft tissue movement, which compensated the effect of bracing for rotational degrees of freedom. Typically, ACL strain is induced by anterior translation or internal rotation of the tibia. Because the kinematic analysis showed no effect of the misaligned brace on internal/external rotation, we concluded that the higher ACL strain in the misaligned braced knee is most likely explained by the anteriorly directed shear force induced by the brace.
A limitation of this study are the small muscle forces compared to the physiological loading condition. However, we intentionally used this approach, so that the effects of bracing became more apparent as the muscle forces had only slightly stabilised the knee. In addition, because the change of the ACL strain during knee flexion is higher in vivo than in vitro, we also expect a larger effect of bracing in the living knee.
Another limitation is that the soft tissue in the present in vitro study was not as tensed as living tissue, even though we stretched the skin tightly to prevent wobbling. However, softer tissue can more effectively compensate misalignment than tensed tissue, and thus the negative effect of bracing might be even higher in the living.
Conclusion
Our results indicate that a correctly aligned knee brace does reduce ACL strain during squatting, particularly in a knee position close to extension. By contrast, a misaligned brace significantly increased the ACL strain compared to the correctly aligned brace. These findings emphasise the importance of educating patients and athletes how to place a knee brace correctly and to be aware of brace slippage. Non-compliance might result in a negative effect of bracing on the ACL.
Footnotes
Author contribution
SPH, FS and LD conceived and designed the experiments; SPH and FS performed the experiments; SPH, FS and LD analysed the data; and SPH, AI and LD wrote the publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
This research was approved by the Ethics Committee at Ulm University (No. 207/16).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the German Federal Ministry of Education and Research (BMBF) through the cooperative research project SE_BURG (Grant No. 16SV6313).