
Abstract
Background and aim:
It is unknown whether prophylactic knee braces can reduce the strain in the anterior cruciate ligament during dynamic activities.
Technique:
An athlete, who had characteristics of high anterior cruciate ligament injury risk, was chosen. A motion capture system (Optotrak Certus; Northern Digital, Waterloo, ON, Canada) was used to record dynamic trials during drop-landing activity of this subject with and without the knee brace being worn. A musculoskeletal model was used to estimate the muscle forces during this activity. A dynamic knee simulator then applied kinematics and muscle forces on a cadaver knee with and without the brace mounted on it. The anterior cruciate ligament strain was measured.
Discussion:
The peak strain in the anterior cruciate ligament was substantially lower for the braced (7%) versus unbraced (20%) conditions. Functional knee braces could decrease the strain in the anterior cruciate ligament during dynamic activities in a high-risk subject. However, the reduction seems to be a result of altered muscle firing pattern due to the brace.
Clinical relevance
Prophylactic knee brace could reduce the strain in the anterior cruciate ligament of high-risk subjects during drop-landing through altered muscle firing pattern associated with brace wear. This could help reduce the anterior cruciate ligament injury risk.
Background and aim
Knee braces have a multitude of uses including stabilization of the knee joint, prevention of injury to the knee, or helping the rehabilitation of the joint following injury. A brace is called a prophylactic brace if it is used to prevent injury. Studies have attempted to investigate the effects of prophylactic bracing on anterior cruciate ligament (ACL) injury incidence with inconclusive results.1,2 Biomechanical studies have reported no consistent reductions in anterior tibial translation (ATT) between braced and unbraced conditions.3,4 Researchers have also reported that knee braces offer some resistance to ATT under low static anterior tibial loads.5,6
The above studies offer no conclusive understanding of the effects of prophylactic knee braces (PKBs) on the ACL as the loads used do not reflect the knee loading during high-risk dynamic activities such as drop-landing. No biomechanical study to date has evaluated PKB for their capability to reduce the strain in an intact ACL during dynamic activities7,8 and tried to distinguish the mechanical restraint of the PKB from neuromuscular effects of brace wear.
The objective of this study was to investigate the effectiveness of a PKB in reducing ACL strain in an athlete who was identified to have high risk of ACL injury, during a highly dynamic activity.
Technique
This research has been approved by the office of research ethics at University of Waterloo, ensuring the ethical and humane principles of research. Written informed consent for participation and publication has been obtained.
Inclusion criteria
A motion capture system (Optotrak Certus; Northern Digital Inc., Waterloo, ON, Canada) was used to record jump-landing trials on 10 recreational athletes (5 females and 5 males with following mean ± standard deviation (SD) characteristics: age 21.5 ± 2.4 years; height 1.77 ± 0.12 m; mass = 75.8 ± 16.1 kg) using a 12-sensor motion capture system. Participants were outfitted with five rigid body marker clusters (each with four Optotrak smart markers) placed on the right foot, right shank, right thigh, low back and upper back. Additionally, 36 relevant bony anatomical landmarks were digitized on the right lower limb, pelvis and trunk. The participants were asked to land with their dominant leg on a force plate (OR6-7-1000; AMTI, Watertown, MA, USA) after stepping off a 0.45-m platform. Five trials were performed for each subject. Kinematic data were sampled at 100 Hz, while ground reaction force (GRF) was sampled at 3000 Hz. Kinematic and GRF data were filtered with a dual-pass second-order low-pass Butterworth filter at cutoff frequencies of 15 and 100 Hz, respectively. The trial with minimal missing markers was used for further analysis.
Outcome variables that have previously been associated with ACL injury risk, such as GRF during landing, plantar flexion angle, knee flexion angle and knee abduction angle, hip flexion angle, trunk flexion angle, and ankle plantar flexion angle, were calculated.9–11 A subject who showed most of these traits was identified as our high-risk participant. This subject (23-year-old female, 1.55 m tall, 50 kg body mass) demonstrated the greatest knee abduction during landing (10°), the highest peak GRF/body weight (BW) ratio (4.9), highest peak knee abduction angle (15°), and least plantar flexion angle at initial ground contact (IGC) (15.5°). A PKB (CTi-Custom; Ossur Inc., Richmond, BC, Canada) was custom made for the participant. The participant repeated five landing trials with and without wearing the PKB. Trials with minimal missing markers were used for further analysis.
Biomechanical modeling
The kinetic and kinematic data from the motion capture trials were input into a rigid musculoskeletal model created in AnyBody modeling software (AnyBody Technology, Aalborg, Denmark). 12 Time-varying muscle force profiles of quadriceps, hamstring, and gastrocnemius muscles were estimated and were input into our in vitro test procedure explained below.
In vitro testing
A fresh frozen cadaver knee (23-year-old male, 1.83 m tall, 95 kg body mass) was procured from a tissue bank. The mold of the frozen knee was prepared using polymer casting tape and sent to a brace manufacturer (Ossur Inc.). A PKB (model CTi-Custom) was made for the cadaver knee. The knee specimen was then thawed and carefully dissected to remove all skin and muscle tissue while keeping the joint capsule intact. Stainless steel cables were attached to the patella, hamstring muscle insertion site, and gastrocnemius muscle insertion site as explained in Cassidy et al. 13 A differential variable reluctance transducer (DVRT; LORD Miscrostrain Inc., Burlington, VT, USA) was placed on the distal section of the anterio-medial bundle of the ACL.
In order to facilitate mounting of PKB on cadaver knee, a foam compound that had similar stiffness as a stiffened muscle was used. A custom-built indentation device (25-mm-diameter indenter) was used to measure the compressive stiffness for the thigh of a live person (22-year-old male, 165 lb, 1.77 m) at nine different locations by applying 180 N compressive force, during a maximum voluntary contraction. The average stiffness was measured to be 19.3 ± 7.95 N/mm (mean ± SD). Liquid foam having a similar compressive stiffness of 17.6 N/mm (Sunmate; Dynamic Systems Inc., Leicester, NC, USA) was prepared and was cast around the dissected knee within the mold that was prepared from the undissected knee.
A dynamic knee simulator system was developed in our lab to study the biomechanics of the knee. The simulator uses six electromechanical actuators to move a cadaver knee in the sagittal plane and to apply quadriceps, hamstring, and gastrocnemius muscle forces and the net moment at the hip joint. The cadaver knee specimen inside the foam cast was mounted on the simulator (Figure 1). Four different combinations of single-leg drop-landing (five trials each) simulations were performed in the following order: (a) unbraced specimen with braced muscle firing pattern/kinematics, (b) braced specimen with braced muscle firing pattern/kinematics, (c) braced specimen with unbraced muscle firing pattern/kinematics, and (d) unbraced specimen with unbraced muscle firing pattern/kinematics. ACL strain data were collected using a custom written LabVIEW program (National Instruments, Austin, TX, USA). The total time of the simulation lasted for 300 ms (100 ms before IGC to 200 ms after IGC). ACL elongation data from the DVRT were collected at a sampling rate of 1000 Hz. Parametric unpaired student t-test (alpha = 0.05) was used to compare the difference in peak ACL strain between the test conditions.

Knee brace mounted on the foam material that encapsulates the cadaver knee. The knee brace assembly is mounted on the dynamic knee simulator.
Discussion
In this study, ACL strain during drop-landing from a height of 0.45 m, with and without brace, was investigated. Researchers have used different heights ranging from 0.2 to 0.6 m to study knee biomechanics during landing. The height in this study was chosen based on study by Yeow et al., 14 which resulted in GRF approximately four times the BW. The quadriceps, hamstring, and gastrocnemius muscle forces for this high-risk subject, derived from the AnyBody modeling system for the braced and unbraced trials, are shown in Figure 2. The peak hamstring muscle force was 3052 N in unbraced trial versus 1930 N in braced trial. The peak quadriceps muscle force was 5653 N in unbraced versus 4666 N in the braced condition. Furthermore, wearing the brace substantially reduced the estimates of the peak net hip extensor moment from 314 to 211 Nm.
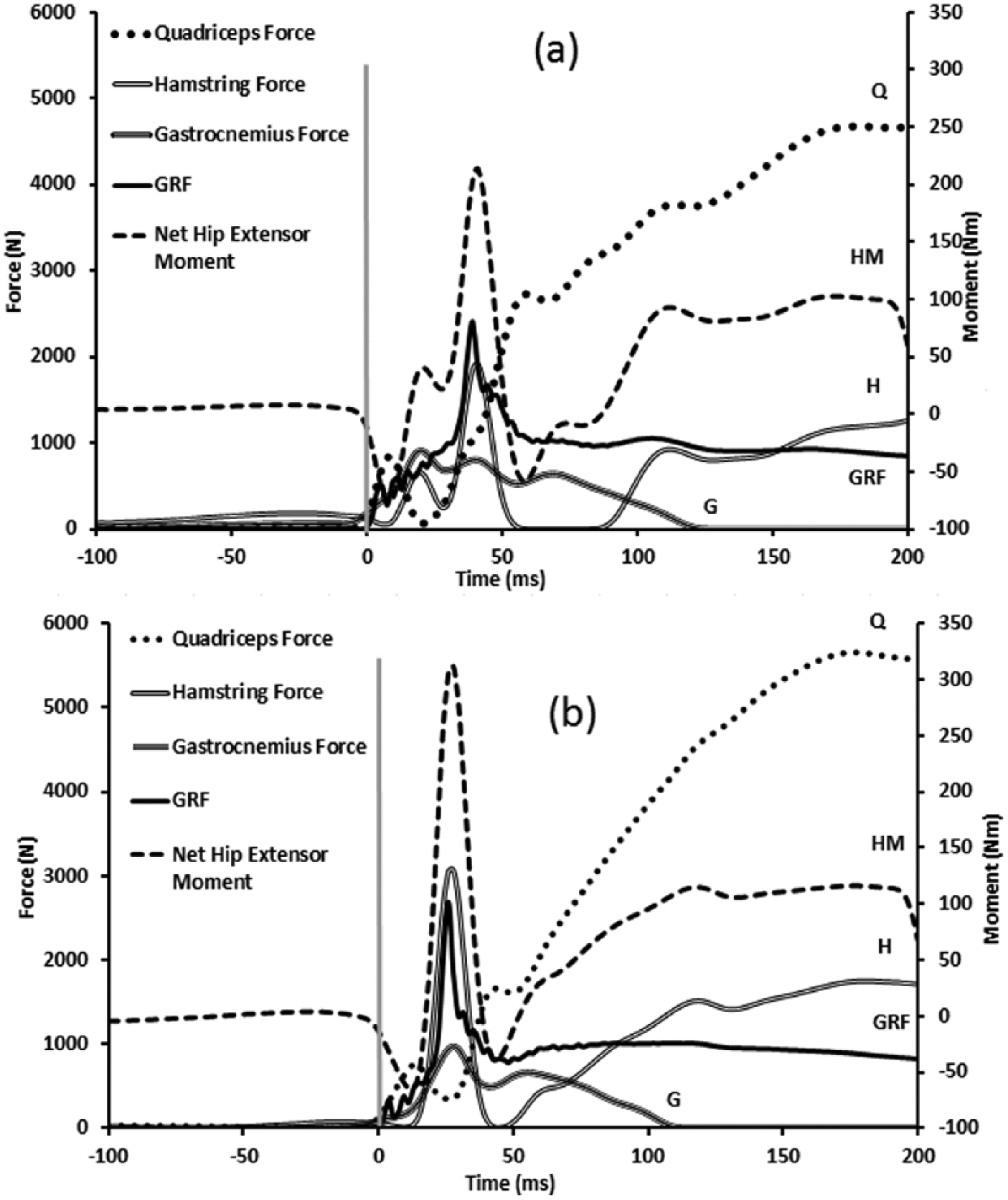
Muscle forces derived from the AnyBody Modeling system for (a) unbraced and (b) braced landing. Vertical component of ground reaction force (GRF) is also given. The gray vertical line at 0 ms represents the initial ground contact. The curve labels are as follows: quadriceps force (Q), hamstring force (H), gastrocnemius force (G), vertical component of GRF, and hip extensor moment (HM). Peak GRF is at 26 ms for braced and 40 ms for unbraced conditions.
Figure 3 represents the average ACL strain curves for each of the test conditions. Additionally, the peak ACL strain for each of the conditions is presented in Table 1. Unbraced condition (d) resulted in significantly (p < 0.01) higher strain (20%) than the braced condition (7%). However, there was no statistical difference between the conditions with similar muscle firing patterns (p > 0.05).
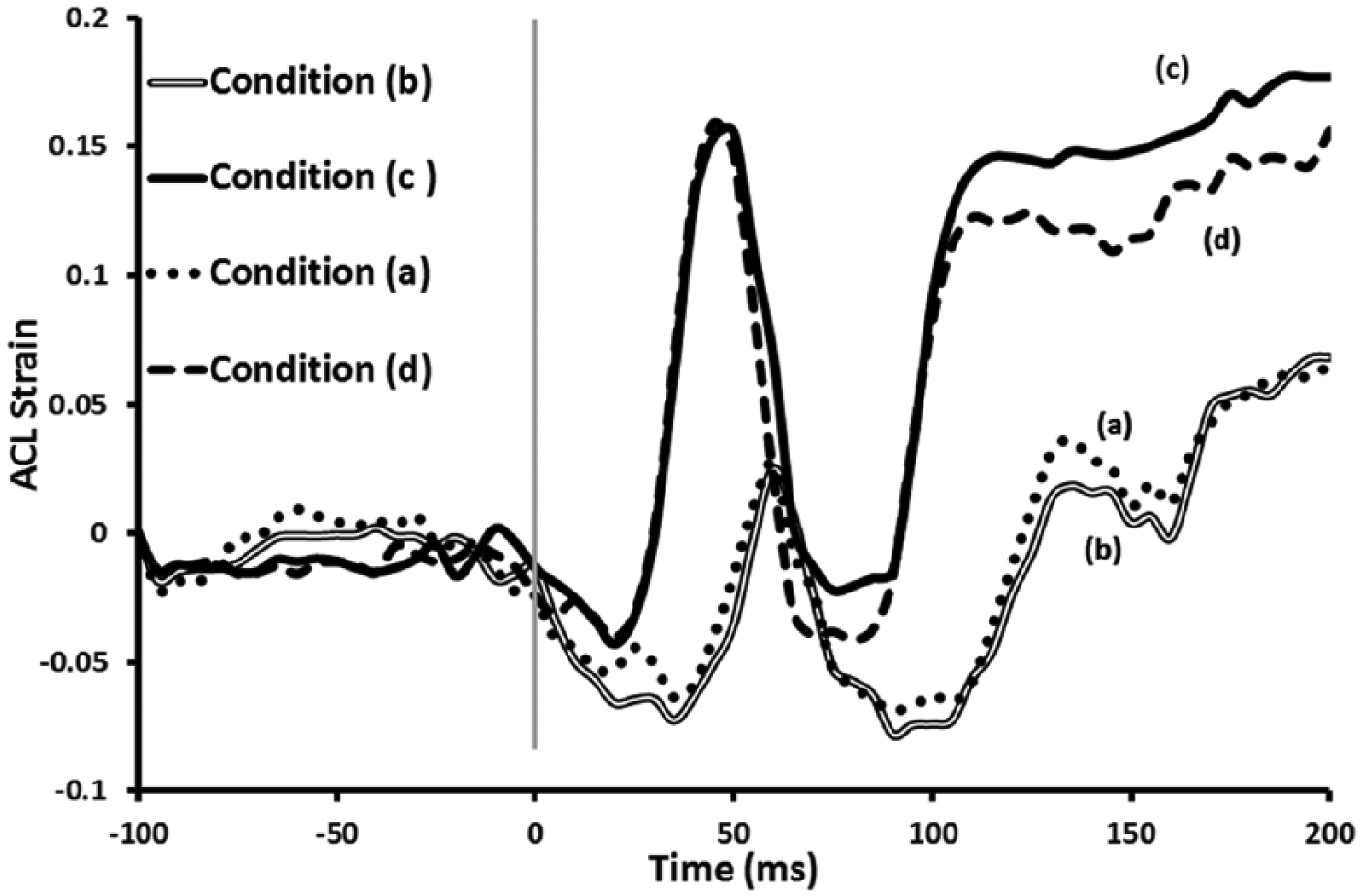
ACL strain plots for each of the simulation conditions. Each curve represents an average of five trials. The gray vertical line at 0 ms represents the initial ground contact. (a) Unbraced specimen with braced muscle firing pattern/kinematics, (b) braced specimen with braced muscle firing pattern/kinematics, (c) braced specimen with unbraced muscle firing pattern/kinematics, and (d) unbraced specimen with unbraced muscle firing pattern/kinematics.
Peak ACL strain under different experimental test conditions based on five trials each.
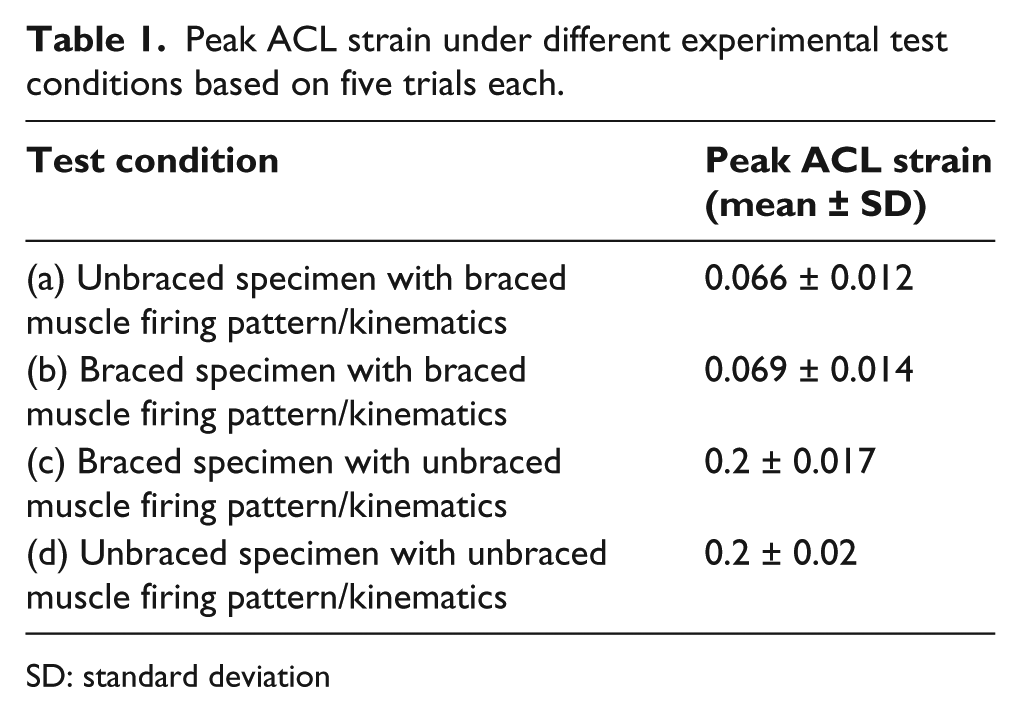
SD: standard deviation
Our results clearly demonstrate the effect of wearing PKB. Comparison between the ACL strain of braced and unbraced conditions showed that wearing the knee brace resulted in a 55% reduction in peak ACL strain (Figure 3). There are two acceptable explanations for the reduction of ACL strain in braced drop-landings. The change in the muscle firing pattern between braced and unbraced conditions could reduce the ACL strain. Alternatively, the PKB could have offered some mechanical restraint to ATT. However, our results showed that the peak ACL strains between conditions that had similar muscle firing patterns, between (a) and (b) and between (c) and (d), were similar. This suggests that the reduction in the peak ACL strain we observed between braced and unbraced conditions with their native muscle firing patterns (conditions (b) and (d)) was not because of the mechanical contribution of the PKB, but rather was caused by the difference in their muscle firing patterns.
From Figure 2, it can be seen that the PKB decreases the hip extensor moment and the quadriceps muscle forces which are well known to be antagonist to the ACL. Furthermore, the peak GRF was reduced in the braced condition. Kinematic analysis of braced and unbraced condition indicates that the hip and knee joints were in a more extended position in the braced condition at initial contact compared to the unbraced condition. The range of motion of the hip, knee, and ankle joints in the sagittal plane between touch down and peak GRF was found to be higher in the braced condition. Furthermore, the time taken to reach the peak GRF was increased from 26 ms during unbraced condition to 40 ms during braced condition. This indicates that PKBs contribute in attenuating the GRF which may offer a protective mechanism by decreasing the absolute force experienced by the lower limb.
The reduction in ACL strain in spite of the lower forces in ACL hamstrings is probably because the increase in the hip extensor moment in unbraced trials overshadows the effect of increased hamstring forces. The ACL strains reported in this study are higher than the ones reported in the literature 5 probably because a high-risk participant was used for simulation.
Beynnon et al. 5 showed that knee braces could protect the ACL only under low anterior shear load but does not offer resistance under high anterior shear load. The major differences between our study and previous studies are that we used realistic kinematics and muscle forces and directly measured ACL strain on cadaver knees. Other studies such as that of Beynnon et al. 5 studied the effect of knee braces under static conditions. While our study showed that the PKB does not offer any mechanical restraint in an ACL intact knee, it does not necessarily mean that that brace would not prevent ACL injury by offering mechanical restraint. In addition to changing the muscle forces and their firing pattern to favor the protection of the ACL, it may mechanically reduce ATT during loading scenarios that might create ATTs larger than those associated with our simulation.
Mounting a PKB on a cadaveric knee is a challenge as the muscles are not stiff as experienced in vivo. Therefore, we substituted the muscles with foam that had similar geometry and stiffness properties compared to activated muscle. The resulting cadaver knee assembly was a closer approximation to the real knee compared to previous approaches. 6
A male cadaver knee, from a person much larger than the female high-risk participant, was used in this study. This was because, based on some pilot studies, it was found that smaller female cadaver knees usually have less strong bones. Such cadaver knees cannot sustain repeated loading on the simulator and usually fail at the patella or muscle insertion sites. Therefore, it was inevitable that a bigger and heavier male cadaver knee was used to ensure experimental feasibility. However, since both braced and unbraced conditions are tested on the same knee, it is unlikely the results would have been affected. While the absolute strain values might be different if a female knee was used, effect of braces would be same irrespective of any knee used as long as same set of loading conditions were simulated. Furthermore, any anatomic variability between the knee sizes of the subject and cadaver is removed by matching the knee moments through adjusting the muscle forces. 13
Currently, PKBs are not widely used as preventive interventions due to an absence of direct evidence of their effectiveness. Our biomechanical case study demonstrates that a PKB can result in reduced ACL strain in an intact knee. This supports the development of additional studies aimed at improving the effectiveness of new brace designs and enhancing the evidence base to assist with clinician and consumer decisions.
The most important limitation of this study is that only one cadaver specimen, which was not of the same gender as the subject, was used. Furthermore, muscle stiffness used for the foam casting was based on muscle stiffness of a subject other than the high-risk subject chosen. Future directions for this research involve replicating the study on multiple participants and cadaveric knee specimens to verify our findings in a wider population.
Footnotes
Key points
Prophylactic knee braces (PKBs) could decrease the strain in the anterior cruciate ligament (ACL) during dynamic activities in a high-risk subject. The reduction is primarily due to the change in muscle firing pattern due to bracing. More research is needed to investigate the effectiveness of brace on a wider population.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
One of the authors, Micah Nicholls, is employed at Ossur Inc. The authors verify that no other conflicts of interest exist.
Funding
This study was funded in part by Ossur Inc., Natural Science and Engineering Research Council Canada, Canada Foundation for Innovation, and Ontario Research Fund.