
Abstract
Background:
There are several kinds of scoliosis-specific and general physiotherapeutic exercise methods used in scoliosis rehabilitation. But there is need for comparable studies on the effectiveness of different exercise approaches for the treatment of adolescent idiopathic scoliosis.
Objectives:
Comparison of the effects of combined core stabilization exercise and bracing treatment with Scientific Exercises Approach to Scoliosis and bracing treatment in patients with moderate adolescent idiopathic scoliosis.
Methods:
Thirty females with adolescent idiopathic scoliosis, who have moderate curves (20°–45°), were randomly divided into two groups. In addition to brace wearing for 4 months, one group received core stabilization exercise therapy, while the other received scientific exercises approach to scoliosis exercise therapy. The outcome measures were based on Cobb angle, angle of trunk rotation, body symmetry, cosmetic trunk deformity, and quality of life.
Results:
Thoracic and lumbar Cobb angles and trunk rotation angles, body symmetry, and cosmetic trunk deformity improved for both groups. Quality of life did not change in either group. The pain domain of the Scoliosis Research Society-22 questionnaire improved in the core stabilization group only.
Conclusion:
Both treatment conditions including core stabilization with bracing and scientific exercises approach to scoliosis with bracing had similar effects in the short-term treatment of moderate adolescent idiopathic scoliosis.
Clinical relevance
This study showed that when scientific exercises approach to scoliosis (SEAS) and core stabilization (CS) exercises were administered with equal intensity, the effects of the two treatment protocols including CS and bracing and SEAS and bracing were similar in the treatment of patients with moderate adolescent idiopathic scoliosis (AIS).
Background
AIS is a three-dimensional deformity of the spine and rib cage. The aims of AIS rehabilitation are primarily to keep the curve magnitude below 30° if possible and to avoid progression 1 and, secondarily, to prevent potential complications, such as postural asymmetry, cosmetic trunk deformity, back pain, and psychosocial effects. 2
For moderate curves (Cobb angle 20°–45°) 3 , the conservative treatment is combined spinal braces and exercise approaches with the aim of preventing curve progression. 4 The mechanism of the spinal brace reducing curve magnitude is to change the patient’s posture by keeping the trunk in a fixed (corrected) position, whereas the aim with exercises is to create behavioral and automatic changes of movement and posture through the use of different motor control strategies. 5
Scoliosis-specific exercise approaches are commonly used in scoliosis treatment, which consist of different active self-correction strategies of the spine (based on curve location, pattern, and magnitude) and individually adapted exercises. The scientific exercise approach to scoliosis (SEAS) is one of these commonly used scoliosis-specific exercise approaches in scoliosis rehabilitation. 6 SEAS provides functional stimulation of muscle contraction for search of the best realignment of the spine and spinal stability in order to counteract curve progression. This muscle contraction is provided by autocorrection of the patient. 5 SEAS exercises are based on three-dimensional active self-correction and stabilization of the correction in different functional movements. 7 The effectiveness of SEAS therapy in AIS in preventing curve progression has been demonstrated.7,8 Negrini et al. 8 reported short-term efficacy of SEAS exercises (for 5-month intervention) in subjects with moderate curves. Reduced risk of progression for mild curves with SEAS intervention is shown in the study by Romano et al. 9
On the other hand, there are general physiotherapeutic exercises, like CS exercises, Pilates, and yoga, which have recently been used in the conservative treatment of idiopathic scoliosis.10,11 These exercises focus on spinal stability and core strength training. 12 Increasing spinal stability is one of the primary therapeutic goals of the CS approach in scoliosis. 11 CS exercise therapy includes training the deep trunk muscles by controlling the position of the trunk in static postures and in functional activities. 13 Improvement in curve magnitude, pain, and postural control due to CS exercises has been shown in adult subjects with mild scoliosis. 10 We previously found that CS exercises are more effective in reducing the angle of lumbar trunk rotation and pain than traditional exercises in moderate AIS. 11
The most effective exercise method for the treatment of AIS remains controversial. There is a need for comparative studies on different methods of exercise for recommendation in clinical practice. In addition, there have been no studies reporting on the efficacy of scoliosis-specific exercises in the improvement of cosmetic issues, quality of life, back pain, and psychological issues. 14 After documenting the efficacy of CS exercise training in AIS, 11 with this study we aimed to establish whether SEAS and bracing intervention are more effective than CS and bracing intervention for treating moderate AIS. The aim of the study was to compare the effects of the combined CS and bracing approach with the SEAS method of scoliosis-specific exercise and bracing on curve magnitude, trunk symmetry, cosmetic deformity, and health-related quality of life in brace wearer individuals with AIS.
Methods
Study Design
This randomized prospective intervention study was approved by the university ethics committee (GO 16/82 on 22 March 2016). All patients gave written informed consent before the study. Eligible subjects were randomly assigned using stratified block to one of two study arms: CS group or SEAS group. Patients were stratified according to age, skeletal maturity, and curve pattern including single (thoracic, lumbar, or thoracolumbar) and double (both thoracic and lumbar) curves. The randomization schedule was known by only one investigator, who was not involved in recruiting participants.
There were 124 females with AIS assessed for eligibility, of which 70 were excluded from the study for not meeting the inclusion criteria, and 24 patients refused to participate in the study. Familial economic problems and patients’ intensive schoolwork were cited as reasons for not participating. Thirty patients agreed to participate in the study. All patients completed the 4-month intervention process and attended the final assessments. The enrollment process is shown in Figure 1.
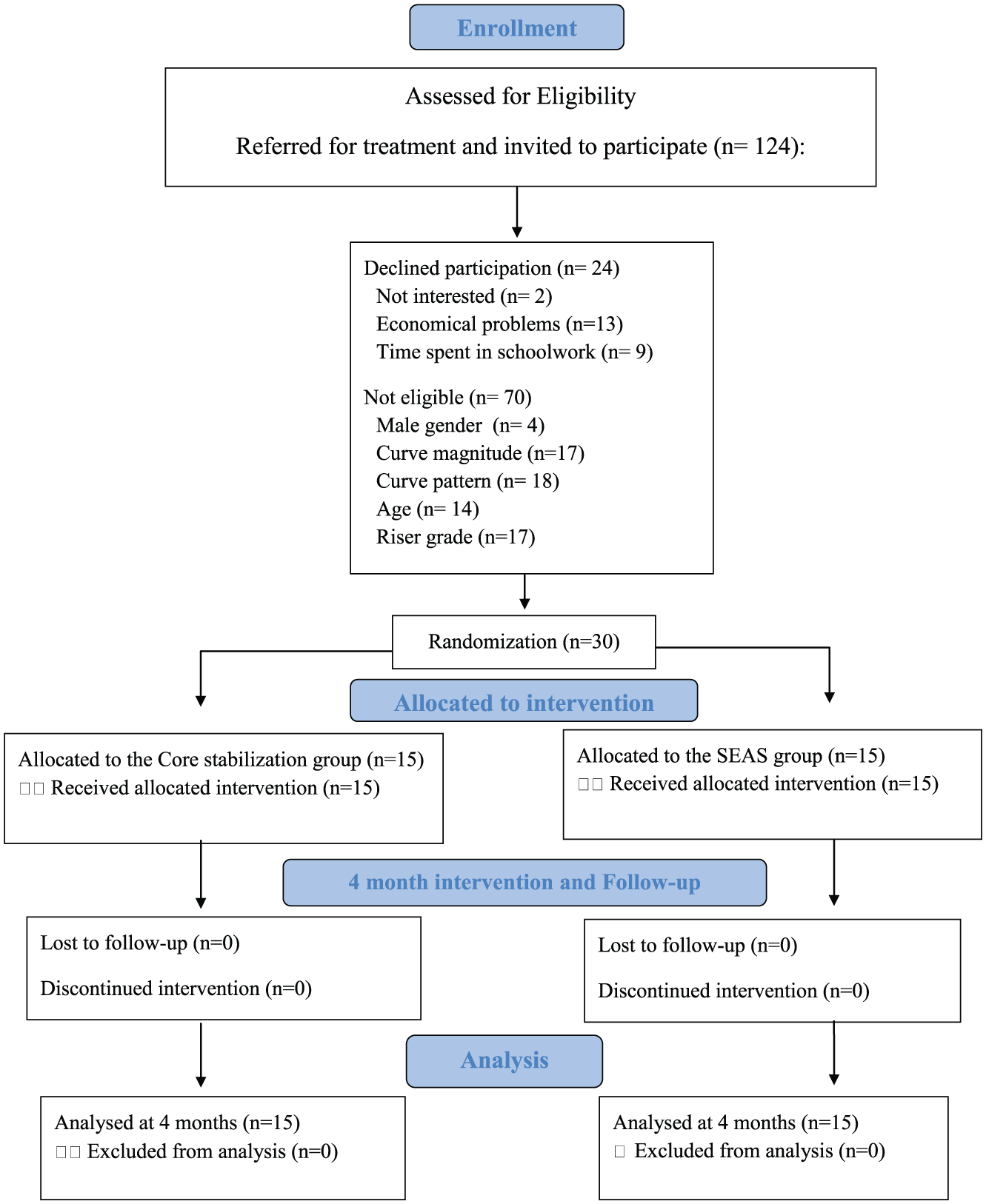
Flow diagram for participant enrollment, allocation, follow-up, and analysis.
Participants
Included patients were adolescents with idiopathic scoliosis seen in our department who were prescribed brace and exercise treatment by the physician between November 2015 and October 2016. Additional inclusion criteria: female sex; at least 12 years old; primary curve magnitude 20°–45° Cobb angle; 3 double curve (right thoracic–left lumbar) or single thoracolumbar curve having an apex in the thoracic region; Risser 2–3; 15 and no previous treatment. Exclusion criteria for both groups: evidence of congenital curve; neuromuscular, rheumatologic, renal, cardiovascular, pulmonary, or vestibular diseases; or surgical correction history.
Outcome measures
The patient general characteristics collected at baseline included age, sex, body weight, height, body mass index, curve pattern (double curves or single thoracolumbar curves), and Risser grade for skeletal maturity.
Assessments were undertaken at baseline and after the 4-month treatment period for each patient by the second investigator, who was blind to the allocation of the participants, throughout the study. Final measurements were taken after the brace has been removed for 6 h. The CS exercise and SEAS exercise intervention groups were compared using the following measures for treatment outcome: curve magnitude with Cobb angle on anteroposterior standing radiograph, 3 angle of trunk rotation with scoliometer in forward bending, 16 trunk asymmetry with the Posterior Trunk Symmetry Index (POTSI), 17 cosmetic deformity with the Walter Reed Visual Assessment Scale (WRVAS), 18 and quality of life with the SRS-22 questionnaire. 19 Furthermore, initial in-brace corrections were calculated for the primary curve, and the correction rate was reported in percentages in order to assess the clinical success of the brace as part of the bracing protocol. Initial mean in-brace correction was recognized as at least 30%, or more as necessary, as previously reported. 20
The Risser grade for determining skeletal maturation was obtained from a frontal-plane radiograph and an index of maturity rated on a scale of 0–5 (where grade 0 indicates no ossification center at the level of iliac crest apophysis and grade 5 indicates complete ossification and fusion of the iliac crest apophysis). 15
Cobb angle is considered the gold standard for determining the magnitude of spinal curve on the frontal-plane radiograph. 3 All patients’ curves were measured, and the score was recorded in degrees. Moderate curves (20°–45°) based on the Cobb angle of the primary curve 4 were included in this study. Thoracolumbar and right thoracic-left lumbar curves were included in this study.
The most common clinical approach used in the measurement of the angle of trunk rotation is the scoliometer of Bunnell measurement in the standing forward-bending position. 16 This method has been reported to have high intraobserver reliability. 21
The POTSI includes the sensitive assessment of the frontal-plane asymmetry of trunk deformity as a two-dimensional surface topographic method in scoliosis. The index based on assessing trunk asymmetry with regard to C7 plumb line, shoulder, and hip asymmetry based on back surface photograph of patient. The ideal POTSI score is zero, which represents full symmetry of the back surface. Higher scores indicate an increasing asymmetry of the trunk. 17
The WRVAS assesses the patient’s cosmetic trunk deformity with a set of figures representing seven visible aspects of spinal deformity: spinal deformity, rib prominence, lumbar prominence, thoracic deformity, trunk imbalance, shoulder asymmetry, and scapular asymmetry. Each item is scored from 1 to 5, with higher scores reflecting worsening deformity. Results are presented as the sum of the seven items. 18 WRVAS was completed by the physiotherapist.
SRS-22 is widely used to evaluate the efficacy of several treatment regimens for idiopathic scoliosis from the patient’s perspective of his or her condition. It consists of 22 items exploring five domains related to psychophysical wellbeing: function/activity level, pain, mental health, self-image, and treatment satisfaction. For each item, the score ranges from 0 (worst) to 5 (best). The summary score is obtained by summing the score of each domain. 22 The Turkish transcultural adaptation of SRS-22 was found to have good consistency and concurrent validity for individuals diagnosed with idiopathic scoliosis. 19
Evaluation of patient compliance with the spinal brace-wearing and home exercise program was done with a daily follow-up diary that was given to patients, to be completed by them, with help from the parent when needed. Patients were required to keep a record of how many hours they wore their spinal brace daily (necessary for 23 h) and how many times they performed home exercises daily (20 min daily). Sums of compliance scores are expressed as percentages.
Interventions
Patients attended an individual exercise program consisting of one 40-min individual session in the clinic per week for 4 months. Patients were instructed to continue performing the same exercise approach for 20 min daily at home. They were taught the exercises individually in the sessions and advised of the intensity at which they should exercise at home. Patients were also given a booklet outlining the movements for visual reference. In this 4-month period, the CS exercise group received CS exercise training, while the SEAS group received SEAS exercises. Both exercise programs were given by the first author, a certified provider of SEAS and CS training methods.
Along with exercises, a spinal brace was applied. 23 Patients were instructed to wear the brace for 23 h daily 23 and to take it off while exercising and during personal hygienic activities for 1 h per day. The treatment was classified as a success or a failure, with failure defined as >5° Cobb angle progression within a 4-month period. 24
In this study, we used a custom-made thoracolumbosacral spinal brace that was adapted according to the curve patterns of the individual patients. The brace was prescribed by the physician as a part of standard care of patients with moderate scoliosis and then fabricated by the same orthotist. The brace was based on the symmetric, patient-oriented, rigid, three-dimensional, active concept of bracing. 23
SEAS consist of individually adapted exercises based on active self-correction. Active self-correction is defined as active movement performed to achieve the maximum possible correction. The approach aims for the stabilization of active self-correction in functional movements; strengthening of the tonic antigravity muscles; and improvement in balance, postural control, and coordination. 8 Supervised SEAS exercise training lasted 40 min in this study. Patients performed seven exercises at home for 20 min, with 3 min spent on each exercise. Exercises gradually progressed based on the participant’s ability each month.
The purpose of the CS method in scoliosis is to develop the ability of the core muscles to restore the dynamic control of external and internal forces over the spine and increase spinal stability. This approach integrates respiratory control, neutral spinal position, rib cage placement, scapular position, and neck-head position. 11 The CS exercise supervised session lasted for 40 min. CS training gradually progressed from the stability of local core muscles (transversus muscles, multifidus, and diaphragm) in static positions to global muscle stability training (internal and external oblique abdominal muscles, psoas major, m. quadratus lumborum, and pelvic floor muscles), global muscle mobility, and strength training (m. rectus abdominis, back extensor muscles, and hamstring muscles) in dynamic body positions. Home exercises were designed to be done for 20 min daily.
Statistical analysis
Sample size was determined based on a pilot study with nine patients using a power of 0.80 and α = 0.05. It was calculated at a minimum of 12 participants per group considering primary outcome of Cobb angle. After confirming the normal distribution of data (using the Kolmogorov–Smirnov test) and homogeneity of variances (using Levene’s test), the effects of the interventions were compared using an independent-sample t-test for continuous variables and Pearson’s chi-square test for categorical variables of outcome measures. The paired t-test was used to test changes from baseline within each treatment group. Data were expressed as means (X) and standard deviations (SDs; 95% confidence intervals (CIs)). p values < 0.05 were considered statistically significant. Analyses were done with SPSS for Windows, version 11.0 (SPSS Inc., Chicago, IL).
Results
The patient groups were similar at baseline in terms of demographic and scoliotic characteristics (Table 1) and outcome measures (Table 2). Right thoracic-left lumbar curves and single thoracolumbar curves were present in both groups.
Comparison of patient characteristics.
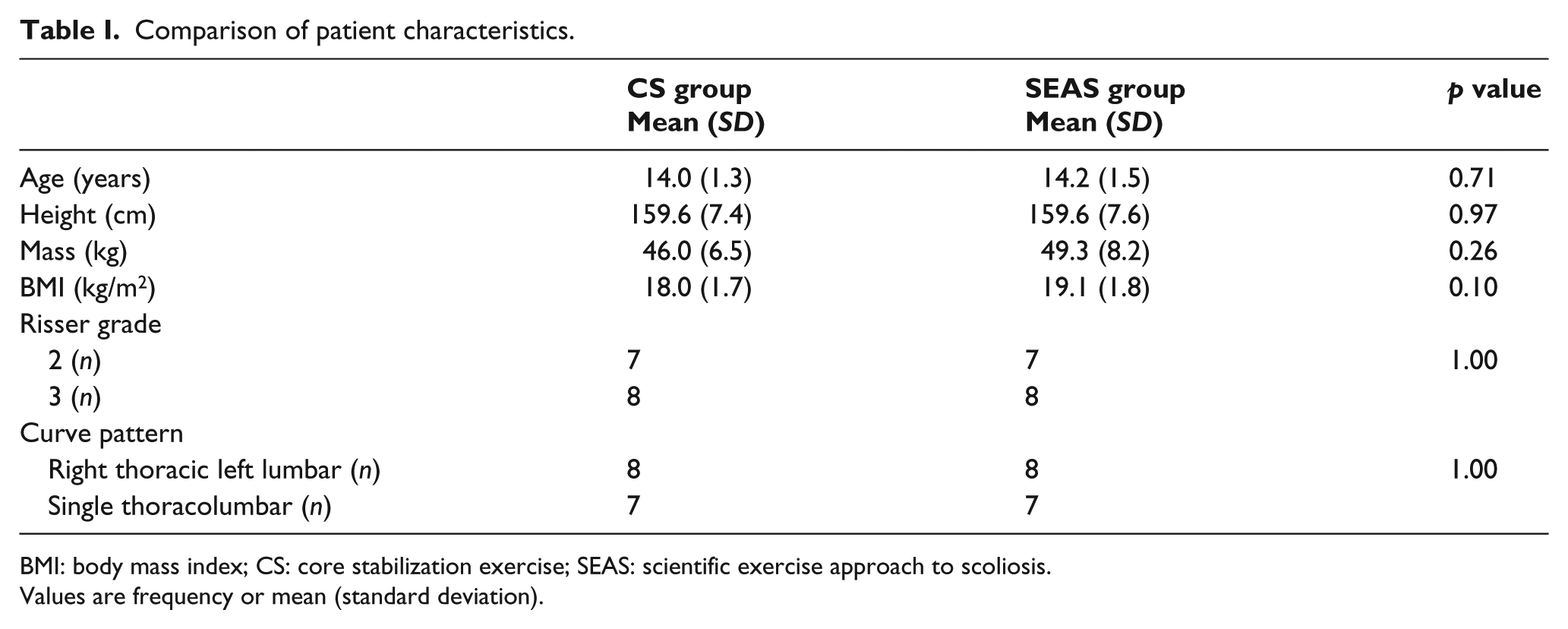
BMI: body mass index; CS: core stabilization exercise; SEAS: scientific exercise approach to scoliosis.
Values are frequency or mean (standard deviation).
Mean (SD) scores, mean (SD) differences within groups, and mean differences between groups (95% CI) for all outcomes.
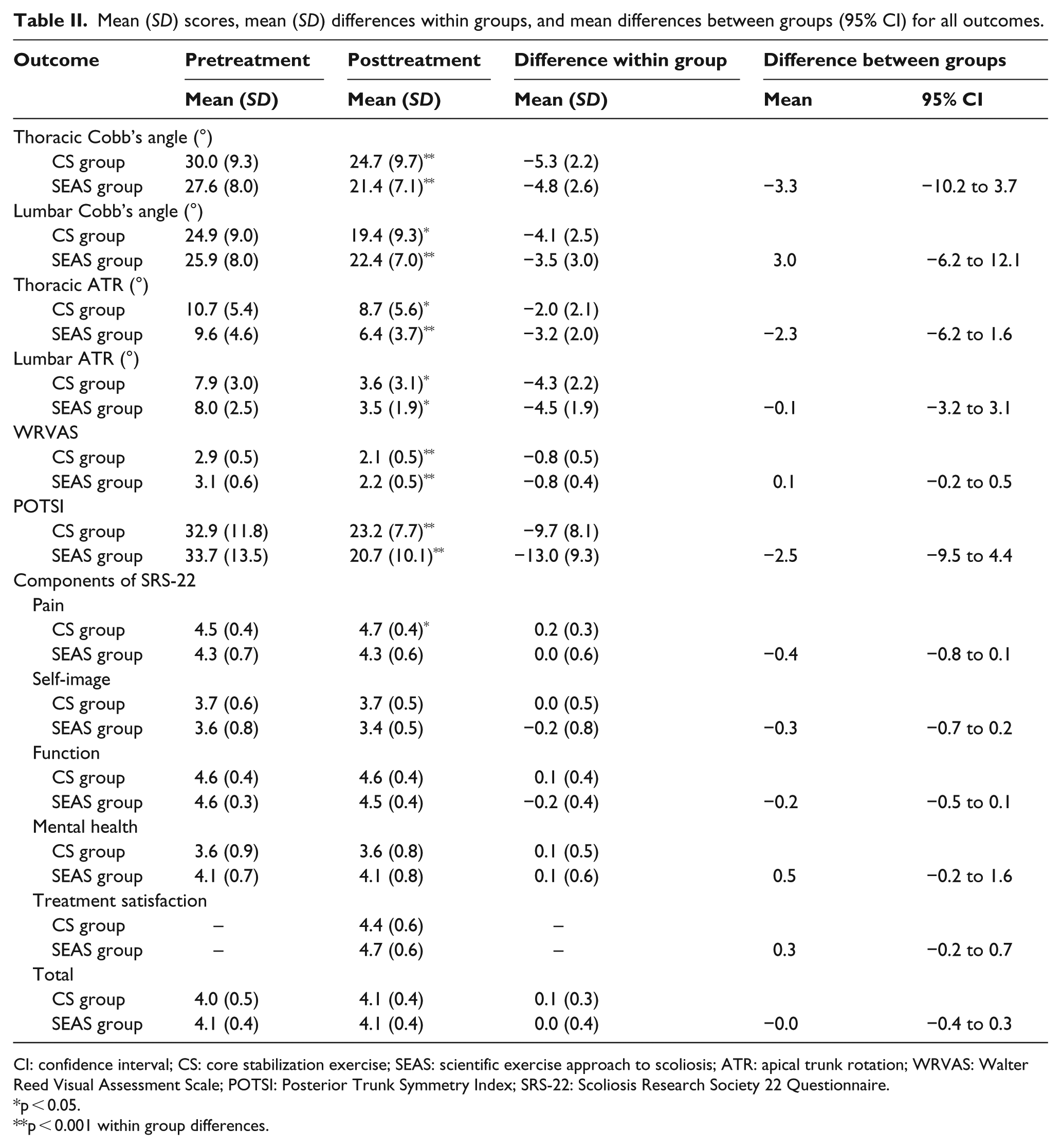
CI: confidence interval; CS: core stabilization exercise; SEAS: scientific exercise approach to scoliosis; ATR: apical trunk rotation; WRVAS: Walter Reed Visual Assessment Scale; POTSI: Posterior Trunk Symmetry Index; SRS-22: Scoliosis Research Society 22 Questionnaire.
p < 0.05.
p < 0.001 within group differences.
Intergroup comparison revealed no significant difference between the groups in thoracic Cobb angle (p = 0.34); lumbar Cobb angle (p = 0.49); thoracic angle of trunk rotation (p = 0.23); lumbar angle of trunk rotation (p = 0.96); WRVAS score (p = 0.39); POTSI score (p = 0.46); total quality of life score (p = 0.83); pain domain (p = 0.09), self-image domain (p = 0.24); function domain (p = −0.18); mental health domain (p = 0.14); and satisfaction with treatment domain (p = 0.20; Table 2). The pre- and posttreatment data and the change in outcome measures are shown in Table 2.
Initial mean in-brace correction for the primary curve was −43.9% (13.1) for the CS group and −44.0% (7.4) for the SEAS group. There was no significant difference between groups in terms of providing initial in-brace correction (mean difference, 0.1; 95% CI, −9.3 to 9.1, p = 0.98).
The two groups were similar on brace and home exercise-compliance variables, with no statistically significant differences (p > 0.05). Compliance with the brace was 88% (11.9) and 79.6% (19.5) in the CS and the SEAS groups, respectively (p = 0.17). Compliance with the home exercise program was 61.6% (17.2) and 63.7% (22.9) in the CS and the SEAS groups, respectively (p = 0.78). Compliance was high with the brace and moderate with the exercise, and patients displayed great care and attention in keeping the diary. They took notes every day on brace use and exercise.
Discussion
The results of this study revealed that combined CS with bracing and SEAS with bracing interventions have similar effects on Cobb angle, angle of trunk rotation, body symmetry, and cosmetic trunk deformity during 4-month treatment period in patients with AIS. These findings confirm the benefits of combined bracing and exercise therapy, whether or not the exercise approach is general spinal stabilization training or scoliosis-specific exercise, in the short-term treatment of moderate AIS.
The Cobb angle and angle of trunk rotation were considered to be important prognostic factors for AIS. 2 Previous studies have focused on the clinical indication of the curve progression, where progression has been defined as a change in Cobb angles at least 5° and in the angle of trunk rotation as 2° for primary curves. 8 Overall, CS and SEAS exercise training, in addition to bracing, had a statistically significant impact on curve progression in this study. In all participants, both thoracic and lumbar Cobb angles of the scoliotic curve decreased. The mean decrease of the Cobb angle of the primary curve was −5.6 (2.7) for the CS group and −5.2 (2.8) for the SEAS group. In addition, there were no patients who had curve progression clinically based on the Cobb angle and angle of trunk rotation scores. Thoracic and lumbar angles of trunk rotation reduced with both treatments as well. These data suggest that both treatment protocols used in the study are effective in preventing curve progression in patients with AIS with moderate curves; however, they have similar effects on Cobb angle. Romano et al. 25 also found SEAS exercises to be effective therapy compared with classical physiotherapy in patients with AIS who were prescribed exercise only. Negrini et al. reported effective curve stabilization with SEAS therapy in mild curves (defined as a Cobb angle of 15.3° and an angle of trunk rotation of 8.9°). Of all patients, 28.9% showed curve improvement clinically, 68.4% were stable, and 2.7% progressed after 1 year of SEAS treatment in their study. 8 In the literature, SEAS was found to be more effective than the usual physiotherapy in AIS.8,25 Task-oriented corrective spinal exercises 26 were other exercises, which also was found more effective than general physiotherapeutic exercises in patients with mild AIS. For moderate curves, SEAS was determined to be helpful in reducing correction loss during brace weaning period. 27 Gur et al. 11 showed that combined CS and bracing protocol was effective than general physiotherapeutic exercises and bracing protocol in patients with moderate AIS.
The assessment of clinical components of scoliotic deformity, such as torso asymmetry and cosmetic deformity, is essential for describing and treating three-dimensional scoliotic deformity. POTSI provides quantitative data for detecting posture changes and reliably find differences that are clinically significant. 17 Body symmetry improved in both the CS and SEAS therapy groups, with no difference in group mean values in this study.
Improvement in cosmetic appearance is the primary objective of scoliosis treatment, which is clearly reported in a consensus by SOSORT. 28 WRVAS was found to have sensitivity to the changes occurring regarding the worsening or improving of the deformity of the scoliosis. 29 Cosmetic deformity improved considerably in all cases in both groups in this study. The significant improvement in cosmetic deformity in both groups after 4 months of exercise and bracing therapy can be attributed to the reduced curve magnitude and improved body symmetry. Both exercise methods used in this study mainly work on improving spinal stability, poor posture, and postural habits.
The negative effects of scoliosis on quality of life and related constructs such as psychosocial health have been reported in the literature. 30 As stated in the 2005 consensus, only 5% of studies on scoliosis included a measure of esthetic appearance and 1.4% a measure of health-related quality of life. 28 Quality of life is considered good if patients had at least four points on SRS-22. 31 But both exercise methods adjunctive to bracing had no impact on the quality of life of the patients with AIS. However in the CS group, there was a trend toward reduction of pain with an average of 0.2 points. 0.2 points was reported as the minimal clinically important difference in pain outcome measure of SRS-22 previously. 32 This may be explained by the fact that the patients increased their back extensor and deep abdominal muscles’ endurance and core stability with CS exercise training. Movements in CS training are performed using all types of muscle contraction (i.e. concentric, eccentric, and isometric), establishing a progressive increase in muscular flexibility, recruitment, and strength. 13 This trend toward reduced pain with CS exercise training suggests further studies to explore the long-term effects of exercise treatments on pain in AIS. Alves de Araujo et al. 10 found reduction in back pain and a trend toward improvement in quality of life with stabilization training in patients with scoliosis, whereas Plaszewski et al. 33 reported that scoliosis-specific exercise treatment in adolescents did not alter adult quality of life in idiopathic scoliosis. The lack of reported details about change in body symmetry, trunk appearance, and quality of life with conservative treatment in scoliosis makes a quantitative comparison impossible with our study.
Psychological distress among patients is of major concern to therapists, given its negative effect on patient compliance. 30 In this study, there was good compliance with bracing and moderate compliance with home exercises in both groups. There was no statistically significant difference between groups in terms of brace and exercise compliance. In addition, patients in both the groups reported satisfaction with treatments in the subdomains of SRS-22.
A limitation of the study is that compliance was not formally measured and, therefore, it was not possible to evaluate fully the effect of compliance with daily home exercises on outcome. The use of additional bracing may have influenced outcome, but this was standardized in both the groups in terms of curve pattern, initial in-brace correction, skeletal maturity, and age. Traditionally, a “bracing only” group would be included in order to make a real comparison of two different exercise interventions, but this would have been difficult to implement for ethical reasons, given that it is necessary to combine bracing and exercise intervention for the improvement of moderate curves. 34 But also a group, which consists of participants who were less compliant with the exercise protocol, would have been used to enlighten the exercise effect. This study shows short-term effect of the two treatment protocols. Future studies are needed to compare long-term effects of CS and SEAS interventions in the conservative treatment of AIS.
In conclusion, the results suggest that both treatment conditions including CS exercise with bracing, or SEAS exercise with bracing reduced curve progression, angle of trunk rotation, improved body symmetry, and cosmetic trunk deformity in the 4-month period. When SEAS and CS exercises were administered with equal intensity in addition to bracing, the results showed no difference regarding the effects of the two different treatment protocols in the 4-month treatment period for moderate AIS.
Footnotes
Authors’ Note
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.