
Abstract
Brace treatment is the most commonly used non-surgical treatment method for adolescent idiopathic scoliosis (AIS). This study is to determine the force changes exerted by a brace over time during both day and night-time wear and to explore correlations between force changes to bracing outcomes. Twenty subjects (three male, 17 female) diagnosed with idiopathic scoliosis who had worn their braces for six months participated into this study. However, due to non-continuous brace wear and exclusion of subjects with large curves (Cobb angle >40°), only nine subjects were included into the day-time analysis and 11 subjects were included into night-time analysis. All subjects used a load monitor system from four days up to 14 days with Boston braces. Cobb angle measurements were taken at initiation of brace treatment as well as after weaning upon completion of the treatment. After the monitoring period, the data was extracted and analyzed. Forces were compared between hours 1, 2, and 5 for the day and night groups, and the correlation of force changes to bracing outcomes were analyzed. In daytime wear, a significant decrease in force over time was found. Most of the decrease occurred within hours 1 and 2 of brace wear. There was no significant decrease during night wear. There were no significant correlations between force decline and outcome.
Keywords
Introduction
Scoliosis is a lateral curvature of the spine with vertebral rotation (Kane 1997; Asher and Burton 2006). Adolescent Idiopathic Scoliosis (AIS) represents a subset that accounts for 80% of idiopathic scoliosis, and occurs in about 2 – 3% of 10 to 16-year-olds (Riseborough and Wynne-Davies 1973; Reamy and Slakey 2001; Asher and Burton 2006). With curves greater than 30°, there is a marked increase in female prevalence (10:1 over males). Larger curves are more likely to progress; hence the female population is more likely to undergo treatment. The majority of AIS cases only require observation and follow-up (Lenssinck et al. 2005); approximately 10% of patients require medical treatment. Of all the non-surgical treatments available, bracing is the most commonly used method for AIS and is the only one that has evidence for its efficacy in halting curve progression and preventing surgery (Lonstein and Winter 1994; Nachemson and Peterson 1995). Bracing is used primarily for curves of 25 – 45° in a growing child (Ugwonali et al. 2004), while surgical methods may be necessary for those patients with curves greater than 50° or those with curves greater than 45° and an immature bone age (Lonstein 2006).
Despite the use of bracing for over 40 years, its effectiveness is still questioned (Helfenstein et al. 2006). While there have been studies that confirm the usefulness of bracing in reducing surgeries and preventing curve progression, others have demonstrated that bracing has been not successful in reducing surgery (Lenssinck et al. 2005; Asher and Burton 2006; Goldberg et al. 2001). A potential explanation for the controversy and mixed results is the fact that good compliance is necessary for the brace to be effective (Lou et al. 2004; Perie et al. 2003). In the past, it was very difficult to measure compliance objectively. The most common methods relied on subjective surveying of patients about their brace wear and inspection of the brace wear and tear. New advances in technology have allowed measurement of compliance by devices such as force-sensitive resistors (Havey et al. 2002; Lou et al. 2004) and temperature-humidity gauges (Helfenstein et al. 2006). Recent estimate of compliance was around 65 – 67% (Nicholson et al. 2003).
With force-sensitive sensors, it is possible to accurately measure both the qualitative (amount of force being applied during wear) and quantitative (how many hours a day the brace is worn) aspects of compliance in brace treatment. To our knowledge, no research has been done to study the effects of time on the qualitative compliance. This is important in furthering the benefits of bracing because if the amount of force exerted by the brace diminishes over wear time, the efficacy of the brace may be impaired. The objective of this study is to determine, through objective force measurements within the brace and the pattern of qualitative compliance over time in both day and night wear.
Materials and methods
In a previous study (Lou et al. 2006), 20 subjects (17 females and three males) used a low power load monitoring system over a course of approximately two weeks. These candidates were selected by the following inclusion criteria: Having a diagnosis of AIS, being between the ages of nine and 16, and being treated with full-time bracing (prescribed at least 20 h per day). The selection criteria for the current study included the previous selection criteria as well as the following exclusion criteria: Presenting with an initial Cobb angle of greater than 40° (three excluded), male subjects (three excluded), and not wearing the brace continuously for more than 5 h at a time (five excluded for day wear, three excluded from night wear). In total, there were nine subjects in the day group and 11 in the night group.
Initial Cobb angles were measured from AP radiographs at the first clinic visit. Transducers were installed in the pressure pad area of the brace, which is the main pad that exerts a corrective force to the major curve. The location of the pad was determined according to standard Boston Bracing procedure, and the prescribed pad forces were set by the orthotist. A session was held to train patients in moving with the brace, serving also to ensure that the data logging device was properly working. The subjects then proceeded with normal daily activities for a target period of 14 days. Some subjects returned earlier than expected but some subjects returned exactly on the 14 day. Upon the completion of their fulltime brace treatment (a period of 1 – 3 years), the subjects were weaned for a period of 4 – 6 months by wearing the brace only at night, and their final Cobb angle was measured from radiographs at the next visit to the clinic.
Data logger
The major components of the load monitoring system were a low-power microcontroller, a real time clock (RTC) programmed with a sample frequency of 1 sample per minute and a 256 KByte flash memory. The device was sufficient to store up to four months of data with selected sample frequency and have enough power for 14 days without recharging. The data recorded was a measure of the force (N) applied by the brace and the corresponding sampling time.
Transducer
The transducer had an operating force range of 0 – 6.82 N, and was able to operate adequately over a temperature range of 5 – 50°C. Linearity and hysteresis was measured as ±1.0% and ±0.5% FSS, respectively (FSS, or Full Scale Span, is the algebraic difference between full scale output voltage and the zero level output). Through several in-lab measurements during loading and unloading, the force transducer was shown to have an output that was linear and proportional to the forces. The transducer was embedded underneath the foam lining so that the subjects did not notice any different from their ordinary braces. Force was translated into pressure with this equation:

Detailed description of the data logger and the force transducer can be found in Lou et al. (2002).
Statistical analysis
We analyzed a 5-h interval of continuous data on three continuous days and nights from each of the subjects. For daytime wear, the selected 5-h intervals had to begin with an initial spike in force after a period of non-activity as recorded by the transducer, indicating that they had just put on the brace. At night, the measurements all began at 01:00 am and were recorded until 06:00 am. This period was selected because it was the most likely 5-h window during which the subject was asleep.
The data over each of the first 5 hours was tabulated. The average force experienced during each hour was calculated, and was divided by the prescribed force to give the force ratio. This ratio allows for comparison of data between subjects. Graphs were created to display the changes in force ratio over time.
The statistical difference between the force ratio in hour 1 and hour 5 was determined using a paired two-tailed Student's t-test as well as the Wilcoxon test. T-test results were reported for simplicity, as results obtained with both methods were consistent. A bivariate correlation analysis (Spearman's Rho test) was used to determine correlation between the following sets of variables and the outcome (the change in Cobb angle after the full treatment): Difference in force ratio between hours 1 and 5, force ratio in the first hour, and force ratio in the 5th hour. All of these procedures were done for day as well as night data.
Results
Nine patients were included in the day study and 11 patients were included in the night study (subjects 1 to 9 involve in both daytime and night time analysis, subjects 10 and 11 only in the night time analysis). The average age of the patients was 13.7 ± 1.1 years for the day subjects and 13.5 ± 1.1 years for the night subjects. The subjects were prescribed a force ranging from 0.8 – 2.1 N. The day group wore their monitored braces for an average of 11.4 ± 4.3 days, with the night group averaging 11.6 ± 3.9 days. The average outcome from pre-brace to post-brace wear was an increase in Cobb angle by 0.6° ± 7.2° for the day group, and an increase in 1.0° ± 6.7° for the night group. The greatest increase in angle was 13°, and the greatest decrease in angle was by 9° (Table I). In the day group, two of the nine patients had a progression in Cobb angle of greater than 5°. Two of the subjects improved their Cobb angles by greater than 5°; the remaining five subjects were within 5° of their initial curve. In the night group, three had curve progressions greater than 5°, two had improved their Cobb angles by more than 5°, and six subjects were within 5° of their initial Cobb angle (Table I).
Demographic and clinical information
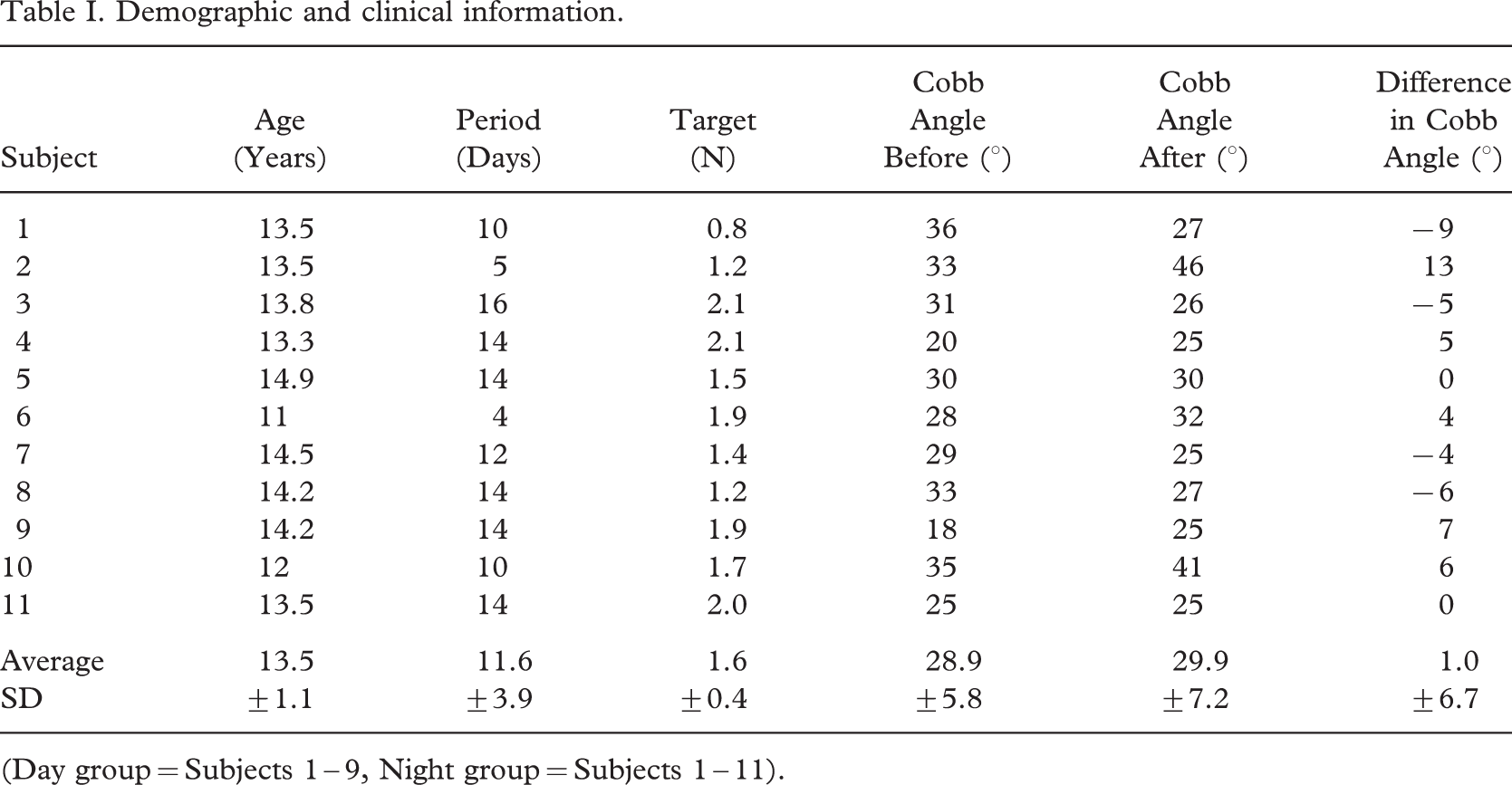
(Day group = Subjects 1 – 9, Night group = Subjects 1 – 11).
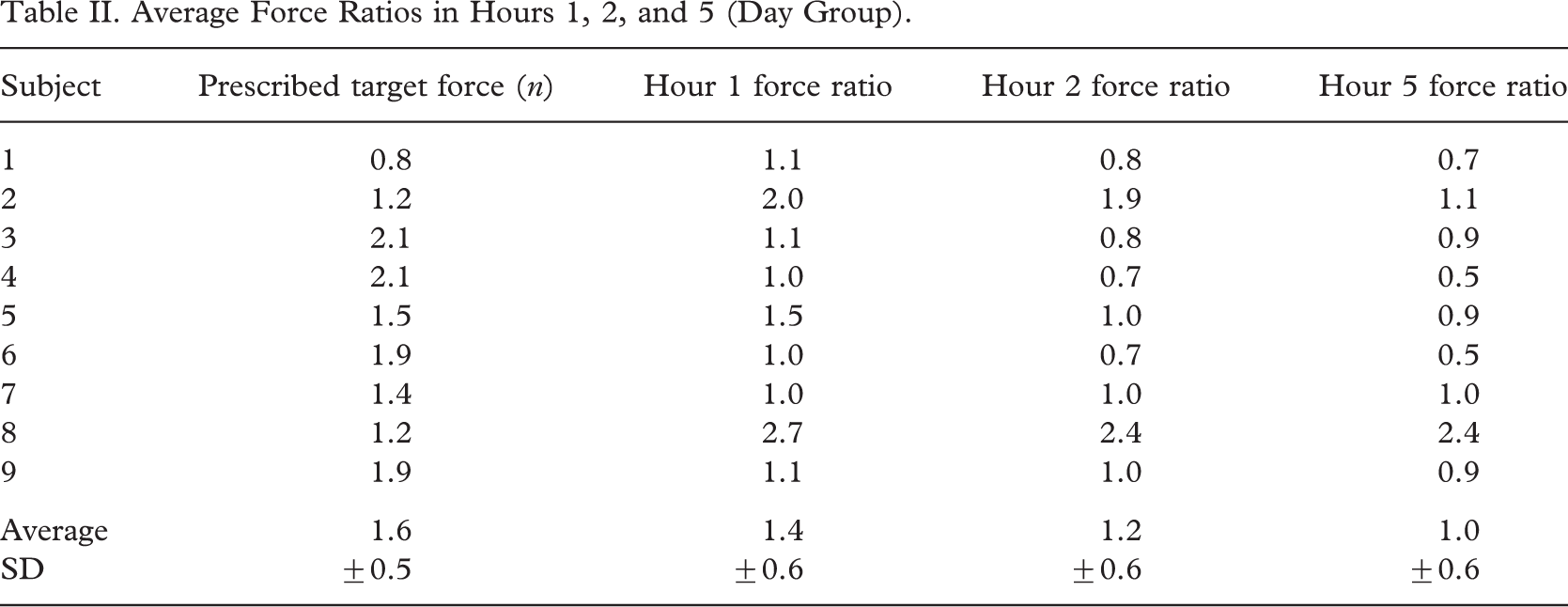
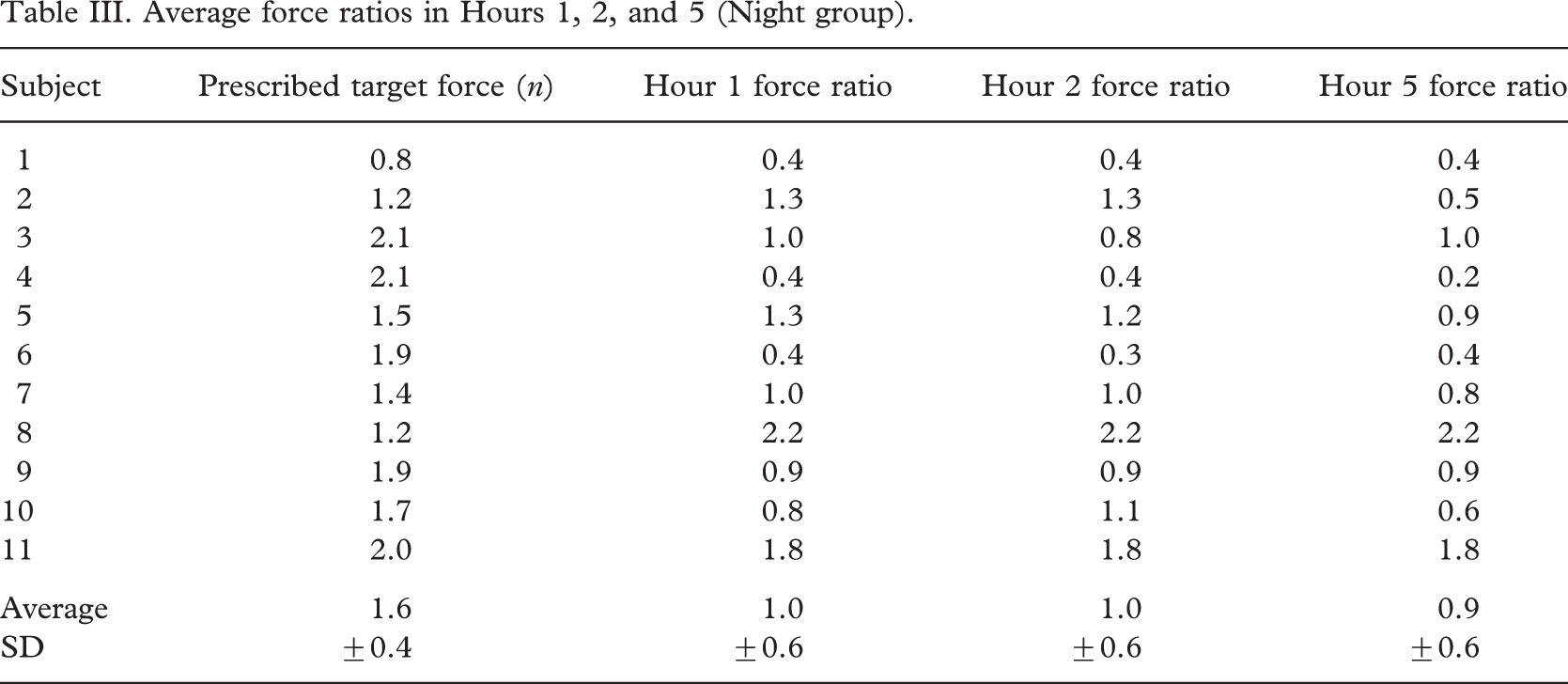
Table II shows the day group with the average force ratios in hour 1, 2, 5 respectively. There was a statistically significant decrease in force within the first 5 h of consecutive brace wear during daytime hours. The decrease was from 1.4 (or, 139% of prescribed force) ±0.6 in the first hour to 1.0 ± 0.6 in the fifth hour, a difference of 0.4, which is a 29% drop from the initial force (Table IV). There were no significant differences amongst the three days of data per patient, and all of the subjects exhibited this consistent decrease in force. Most of the drop in force happened between hour 1 and 2, as the difference in those two hours is 0.2 ± 0.1 (p = 0.001); between hours 2 and 5 the difference did not reach statistical significance (Table IV). The observed difference between hours 1 and 5 (0.2 ± 0.2, p = 0.06) for the night group did not reach significance (Table IV). Only eight of 11 subjects showed a drop in force between hours 1 and 5. Similarly, there was no significant change in force between hours 1 and 2, and subsequently between hours 2 and 5.
Average Force Ratios in Hours 1, 2, and 5 (Day Group)
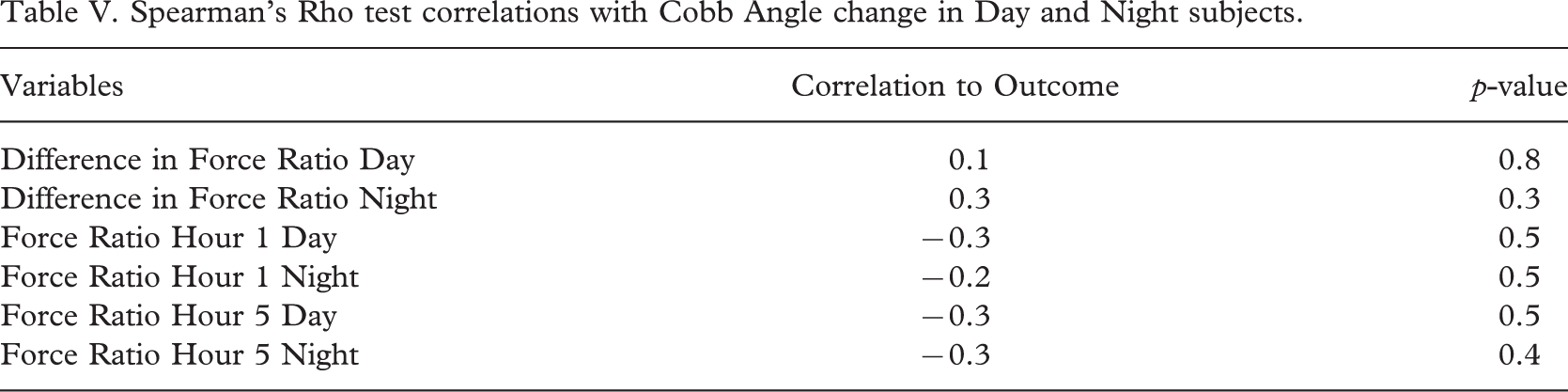
There were no significant correlations between the force monitoring measures and the brace outcome at the end of treatment for both day and night groups. The change in Cobb Angle after weaning was not correlated to the average change in force ratio within the first five hours, the force ratio in the first hour, or the force ratio in the fifth hour (Table V).
Average force ratios in Hours 1, 2, and 5 (Night group)
Student's Paired t-test results

Spearman's Rho test correlations with Cobb Angle change in Day and Night subjects
Discussion
The study of compliance in brace treatments has undergone extensive improvements since the days of relying on brace inspection and patient surveys. New methods using force and temperature sensors have proven to be useful, accurate ways to assess compliance. Rahman et al. (2005) determined that greater quantitative compliance was associated with reduced curve progression, and hence, better outcomes. However, no study to date has looked at the effect of time on the force that the brace is exerting its prescribed pressure level on the back.
Daytime findings
A possible reason for the decline in force is that the level of activity over the course of the day simply reduces the tension of the straps, hence decreasing the amount of force that can be consistently applied to the body. The marked drop in force between the first two hours indicates that the majority of the tension loss happens within a fairly short time. There is a more gradual decrease after hour 2, as shown on Figure 1, indicating a more stable strap tension. Another possible explanation is that the mechanism of action of the brace is not solely force applied by the pads. It may serve as a prompt for the subjects to move the back and spine away from the applied pressure and hence, may result in active correction of the curve. This hypothesis is in accordance with prior research that indicates that there are both passive and active mechanisms which work to produce the corrective forces in bracing treatment (Wynarsky and Shultz 1991; Perie et al. 2003).
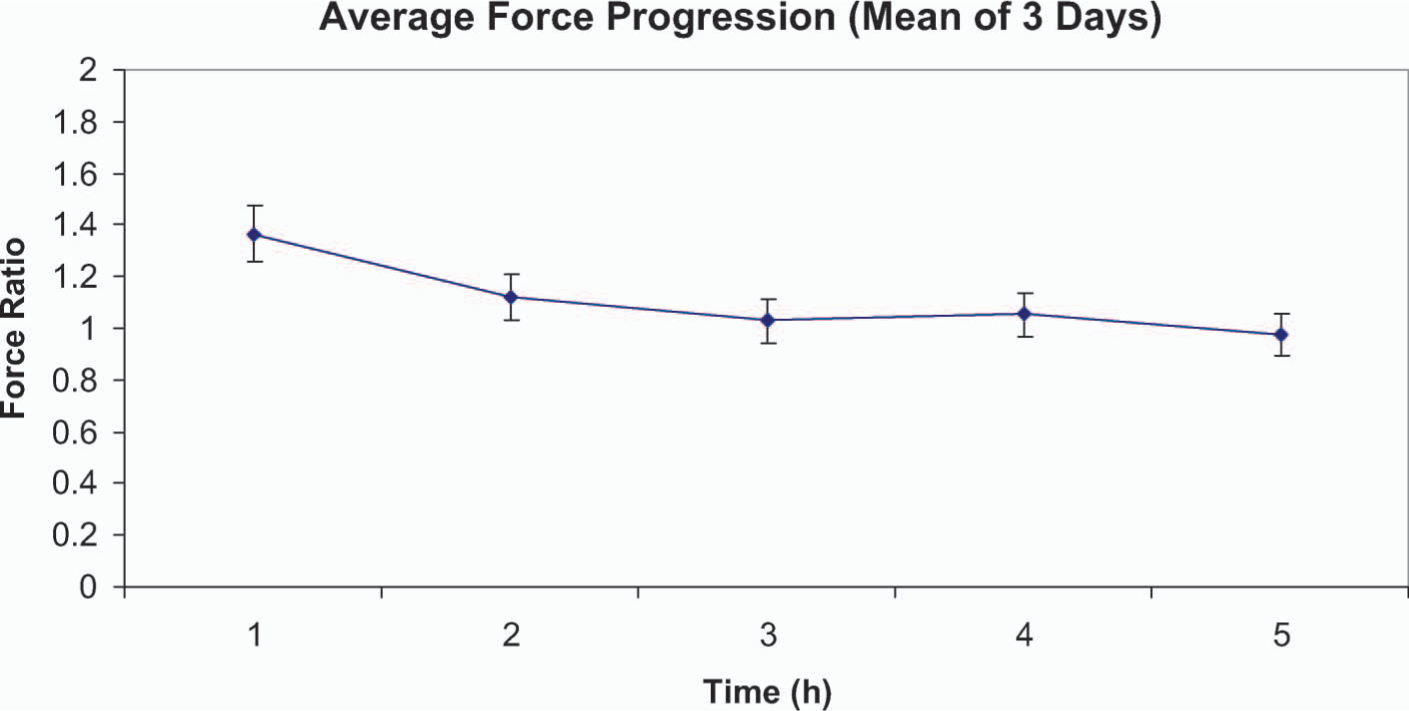
Daytime force profile.
None of the correlations found in this study were significant. However, there was the general trend showing that a larger the force ratio, which indicates the brace is being worn more tightly, is correlated to reduced progression of the final curve. This trend was evident in all three days of data. A larger difference between hour 1 and 5 force ratios correlated with a larger progression of the final curve. Our previous findings (Lou et al. 2004) support the trends from this study, suggesting that the patients who wear their braces more frequently and at a tighter level tend to have better outcomes. Our selection criteria required at least five hours of consecutive wear, which may have biased our sample to include only compliant patients. Had we analyzed less compliant patients with fewer than five hours of brace wear, we may have found significant correlations similar to our previous study. The subjects recruited, as a group, wore their braces tightly. They averaged a force that was almost 100% (Table III) of the prescribed force even after the drop in force over five hours, which probably contributed to our lack of significant correlation findings.
Night-time findings
Although there was a slight drop in force ratio over the five hours (0.15 ± 0.24), this difference was not statistically significant. The profile of the night-time graph compared to the daytime graph illustrates the marked difference in force progression. The night-time force profile varies less, (Figure 2). The results suggest that forces are less likely to decrease over the course of a few hours at night when compared to daytime. The more stable nature of the force progression at night may be due to the lack of movement and muscle contraction during sleep. It is intuitive that movement is much greater while awake, while during certain periods of sleep (REM stage) the body is almost in a state of paralysis. This may contribute to less shifting and movement by the body and consequently less change in force over time.
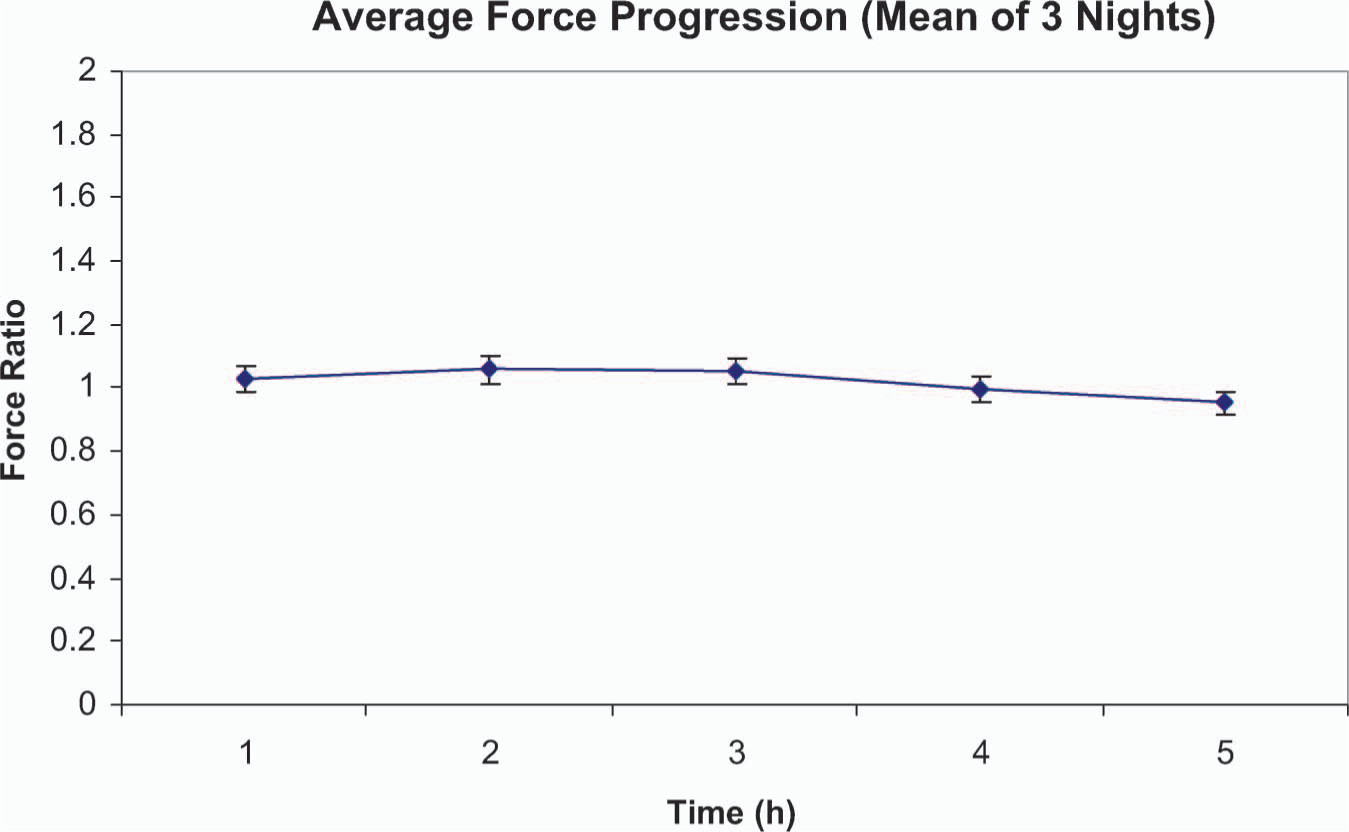
Night-time force profile.
The correlation analysis for the night group was similar to the day group, with no significant correlations found. A one unit increase in the difference in force ratio between hours 1 and 5 correlated to a 0.3° increase in Cobb angle (significance = 0.3). Increases in hour 1 and 5 force ratios did not correlate significantly to decreases in Cobb angle, although the general trend indicated that larger forces may be correlated with better outcomes.
Study limitations
One of the limitations of this study is the small sample size. Few subjects were deemed fit for bracing, met all of our criteria, and were willing to wear the monitoring device, while exhibiting sufficient compliance to provide adequate data for analysis. Had the sample size been larger, some additional findings may have reached statistical significance. The study would also benefit from having a control group without treatment, as well as a group that had constant adjustments made to their brace so that there was no decrease in force over time.
Data was collected for a relatively short period of time (average 11.5 days) with many of the days failing to yield adequate data for analysis; thus, only three days were analyzed. However, this study followed previously established guidelines for monitoring brace wear. An earlier study suggested that the collection of data beyond two weeks would be of little further benefit, because the wearing patterns can clearly be determined within the first fourteen days (Helfenstein et al. 2006).
Standardization of forces, brace wear time, and of the timing interval for the radiograph images would have been desirable. However, the treatment in scoliosis is individualized; standardizing such treatment would be unethical towards the patients in the study.
Results observation
From the results, four subjects showed improvement, five subjects had progression and two subjects had unchanged in their Cobb angles. However, only subject #2 required surgery after the brace treatment. According to the Scoliosis Research Society Committee for bracing, assessment of brace effectiveness should include: (i) The percentage of patients who have ≤5° curve progression and the percentage of patients who have >6° progression at maturity, (ii) the percentage of patients with curves exceeding 45° at maturity and the percentage who have had surgery recommended/undertaken, and (iii) two-year follow-up beyond maturity to determine the percentage of patients who subsequently undergo surgery. All eleven subjects were relatively compliance and most of them wore their braces at least five hours continuously during the study. The results further confirmed that compliance was important to the treatment outcomes. In addition, the subjects 10 and 11 were not included in the day-time analysis; both were night-time brace wearers. Subject 10 had curve progression, but subject 11 had unchanged curve. The noticeable difference was subject 11 had a stable force ratio. However, no conclusive statement could be made from one observation. If SRS guidelines was used, two subjects (Nos. 1 and 8) improved, six subjects saw no change (Nos. 3, 4, 5, 6, 7, 11) and three subjects progressed (Nos. 2, 9, 10). Only subject 8 had high force ratio in both day-time and night-time.
Future directions
This study determined a significant trend in daytime force decrease over five hours of wearing the Boston Brace. The daytime trend of diminished force over time is important because it provides justification for further research in the area of active bracing. Active braces can automatically adjust the brace so that the applied force remains constant over time. Such a system can prevent the decrease in bracing forces over time by making continual adjustments, which may lead to better outcomes. Research to define the reason for the observed force decrease in this study may provide insight into the mechanism of action of the brace treatment.
Conclusion
In the present study, it has been established that daytime forces in a Boston Brace tend to decrease over a period of five hours, mostly within the first two hours. This same decline is not seen at night, where the decrease in force over the same period of time did not reach significance. No significant correlations were found between the effects of the decrease in force and the change in Cobb angle after bracing. These results support future research in bracing methods such as active bracing and in gaining understanding behind the mechanisms that explain the decrease in force.