
Abstract
Background:
This case study represented a unique opportunity wherein a long-time user of sub-ischial sockets had kept nearly every socket he wore for a decade. This individual let us borrow these sockets so we could digitize them and indirectly assess change in residual limb size over time by calculating changes in socket volume and circumferences over time.
Case Description and Methods:
Over a decade, the subject maintained a relatively stable body weight of 84–88 kg and received nine sub-ischial sockets. The internal surface of each socket was scanned using a mechanical digitizer and volume and circumferences calculated.
Findings and Outcomes:
Socket volume increased 31.3%, from a low of 2659.2 cm3 for the oldest socket to a high of 3490.6 cm3 for the most recent socket. Proximal circumferences increased more than distal circumferences with a 15.9% total increase proximally versus 8.9% total increase distally.
Discussion and Conclusion:
The results suggest that this individual’s residual limb increased in size over time despite the compressive effect of the socket and liner. In addition, the increase in circumference was greater proximally than distally, which is where the remaining muscle bellies are located.
Clinical relevance
This case study provides insight into the long-term effect of the sub-ischial socket on residual limb volume given compression of the soft tissues by the socket system.
Background
Ischial containment sockets are the current standard of care for persons with transfemoral amputation.1,2 However, they fit intimately with the ischium, which may limit hip motion and contribute to proximal socket discomfort, a common complaint among prosthesis users.3 –9 Sub-ischial sockets, such as the newly described Northwestern University Flexible Sub-Ischial Vacuum (NU-FlexSIV) Socket technique, have lower proximal trim lines that do not interact with the ischium, potentially increasing hip motion and improving comfort.10 –12
In addition to lower proximal trim lines, the NU-FlexSIV Socket incorporates a flexible inner socket so muscles can move comfortably within the socket as they contract during activity and splay during sitting. The socket is held securely to the residual limb by vacuum pump suction as well as compression of an undersized liner and socket. Research and development on the NU-FlexSIV Socket technique began at Northwestern University in 2009 and the technique was first taught to prosthetists in 2015.11,12
Unlike other transfemoral socket designs, sub-ischial sockets do not provide pelvic support and hence all weight-bearing loads must be borne by the thigh. It is proposed that in the NU-FlexSIV Socket this is accomplished by a total surface-bearing socket that globally compresses and preloads the residuum soft tissues. It is theorized that the undersized liner and socket compress the residual limb, helping stabilize the socket with respect to the residual limb and decreasing relative motion. 11 Firm, fabric-covered silicone liners with a cylindrical profile are preferred for use as part of the NU-FlexSIV Socket over liners with a conical profile to further compress the softer medial proximal tissues. 11
The idea that soft tissue compression can be used to create stability between the residual limb and socket to more efficiently transfer force between the underlying skeleton and prosthesis is not new and, in fact, is used to some extent in all socket designs.2,13,14 Redhead 15 proposed that the soft tissues of a transfemoral residual limb supported by a suitably shaped socket would behave under load as an elastic solid (i.e. a hydrostatic condition). However, compression of soft tissues by socks, liners, and sockets has been shown to lead to volume loss as extracellular fluids are squeezed out of the residual limb.16 –18 Potentially more concerning, and a question raised when teaching the NU-FlexSIV Socket technique, is whether compression from the liner and socket leads to residual limb muscle atrophy over time.
This case study represented a unique opportunity wherein an individual with transfemoral amputation, who is a long-time user of a sub-ischial socket, had kept nearly every socket he wore for over a decade. This individual was willing to let us borrow his collection of sockets so that we could indirectly assess change in residual limb size over time by digitizing the sockets and calculating changes in volume and circumferences over time.
Case Description and Methods
The University’s Institutional Review Board provided a determination that this case report did not constitute human subjects research.
Subject characteristics
The subject was referred to R.C. for prosthetic clinical care following an injury sustained in a motorcycle accident in the summer of 2002 when he was 20 years of age. The subject sustained multiple injuries to the right upper extremity, pelvis, and right lower extremity that resulted in a long transfemoral amputation. The subject’s initial clinical goals were to return to his previous lifestyle of being active in sports and weight training, as well as working in construction.
In the first 4 years post amputation, the subject was fit with three definitive ischial containment sockets that included a skin-fit suction socket followed by two suction sockets with silicone liners. However, the subject experienced discomfort in the groin from the sockets that was exacerbated by the original pelvic trauma and a hernia in the lower abdomen and groin. In an attempt to alleviate these issues, the subject was willing to trial new socket and suspension technologies, first consisting of an ischial containment socket with vacuum-assisted suspension at the end of 2005 and then delivery of his first definitive sub-ischial socket with vacuum-assisted suspension in March 2006. Since that time, the subject has worn various versions of a sub-ischial socket with vacuum-assisted suspension without any major issues. This makes him the longest user of a sub-ischial socket in our clinical care.
Socket characteristics
The initial sub-ischial sockets this subject received were developed through clinical experimentation by R.C. inspired by transtibial sockets with vacuum-assisted suspension that were emerging at that time (Table 1). As can be seen from the descriptions in Table 1, several changes were made over time to the socket materials and laminations incorporated in the sockets used by this subject to improve comfort, compliance, and durability. The subject’s initial sub-ischial socket included a thermoplastic inner layer of polyethylene terephthalate glycol (PETG) and flexible carbon fiber laminations to reduce the liner and sleeve breakage observed in rigid check socket fittings when the liner was reflected over the proximal brim of the socket. In addition, automotive door edging was adhered around the proximal brim to increase the radius and smoothness of the proximal trim lines of sockets 1–4 (Table 1). Lamination lay-ups were developed using hybrid materials including Carbon, SpectraCarb, and Kevlar to further increase socket flexibility and durability. Initially, single wall sockets were constructed (sockets 1–4; Table 1), but over time the materials became commercially available that facilitated the construction of flexible sockets with rigid frames (sockets 5–9; Table 1). Texturing of the flexible socket to increase surface area and suspension forces, while reducing issues with excessive socket rotation on the residual limb, was incorporated in sockets 5–7 (Table 1).
Socket characteristics.
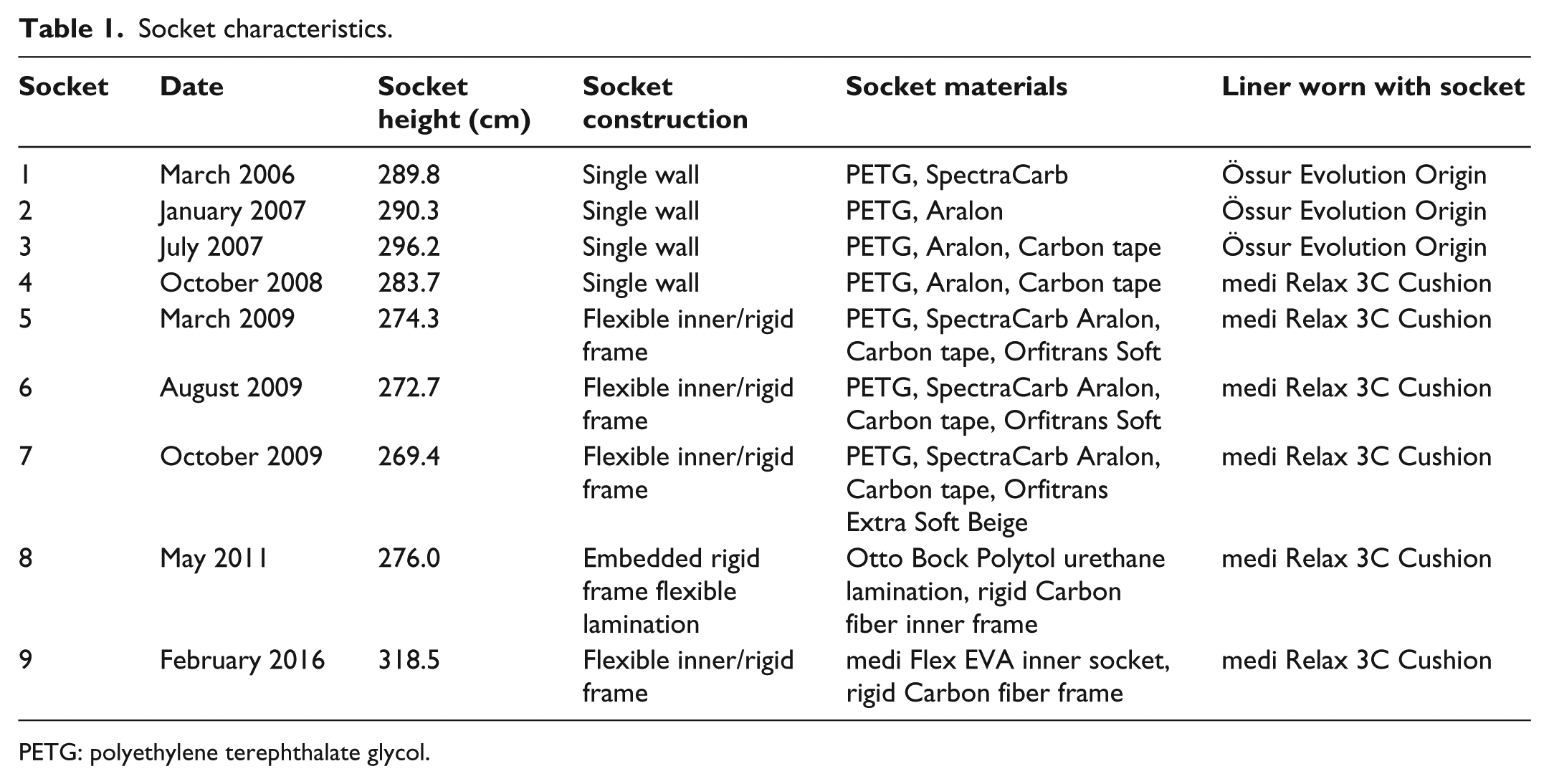
PETG: polyethylene terephthalate glycol.
Collaboration with Northwestern University and development of what has become the NU-FlexSIV Socket began in 2009. Polyurethane resins were used in the production of early NU-FlexSIV Socket prototypes as shown in socket 8 (Table 1). However, discontinuation of the polyurethane resin by the manufacturer led to the use of medi Flex EVA in the current version of the NU-FlexSIV Socket worn by the subject (socket 9; Table 1).
Socket assessment protocol
Nine sockets were provided by the subject with each socket tagged with the month and year the socket was first received (Table 1). One socket received between sockets 8 and 9 was not available for scanning as it was replaced due to damage and discarded when replaced. The internal surface of each socket was scanned using the Provel D1_L Digitizer (Provel, Cle Elum, WA). The digitizer’s mechanical arm was placed at the distal end of each socket and scanned until the arm reached the proximal brim of the socket and fell out, stopping the scanning process. Each digital scan was saved as an American Academy of Orthotists and Prosthetists (AOP) file and then processed using ShapeMaker software (S&S ShapeMaker, Hickory Hills, IL). Using the tracing option in ShapeMaker, socket height was measured from the distal end to the point on the proximal trim line where the scanning process stopped. As the curser was moved proximally along the socket, the socket volume from the distal end to the cursor location was displayed, allowing the circumferences and volumes at the desired height to be calculated by the software program.
For each socket, volume was calculated for the portion of the socket from the distal end to a height of 260 mm. A proximal circumference for each socket was measured at a height of 260 mm from the distal end and a distal circumference for each socket was measured at a height of 55 mm from the distal end. The proximal height of 260 mm was selected as it was the highest digitized point common to all sockets, while the distal height of 55 mm was selected as it is a common clinical point for the measurement of distal residual limb circumferences (Figure 1).
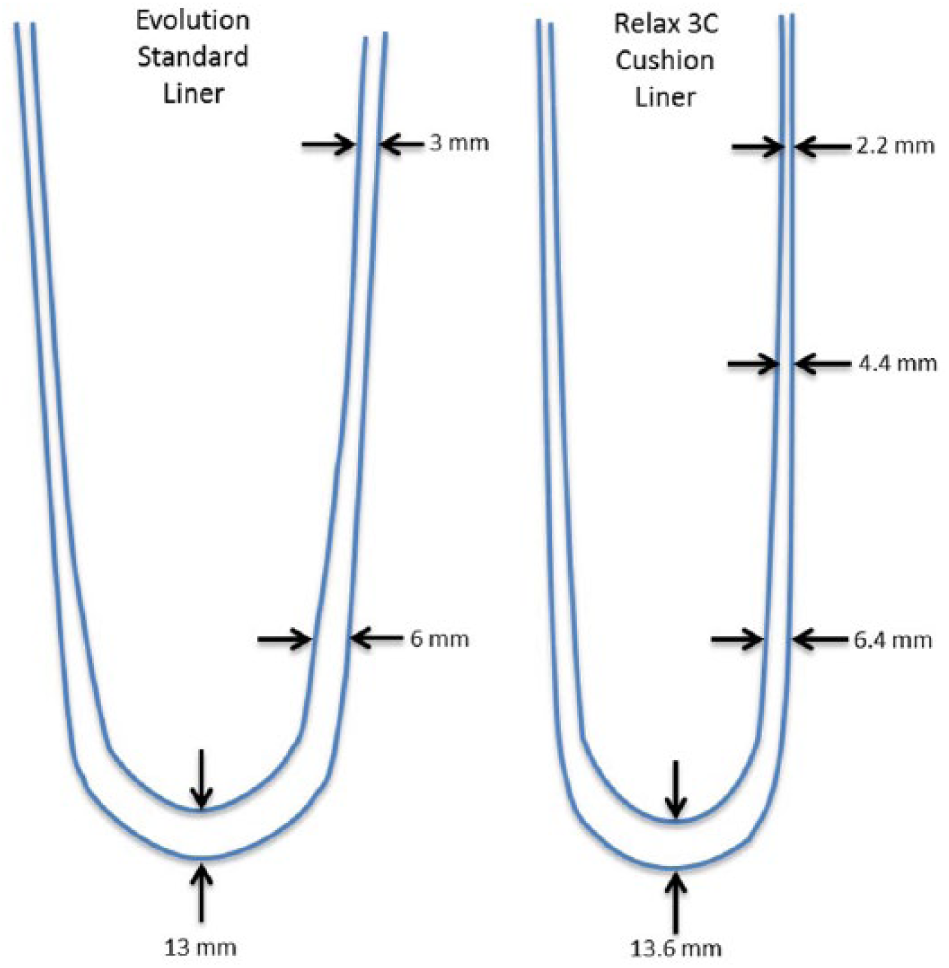
Schematic showing variations in thickness of the liners worn with the sub-ischial socket: (a) Össur Evolution Origin (an uncovered silicone liner) and (b) medi Relax 3C Cushion (a fabric reinforced silicone liner). Schematics were adapted from https://www.ossur.com/prosthetic-solutions/products/all-products/liners-and-sleeves/evolution-liner and https://opedge.com/Shop/Catalog?supplierID=30383560-437A-46EB-A190-E3F83C65E679&categoryID=6200CB82-9610-4AFE-8564-C8A89F19AC5F (accessed on 2 February 2018) and are not to scale.
Findings and Outcomes
From 2006 to 2016, the subject maintained a relatively stable body weight of 84–88 kg. As shown in Table 1, the nine sockets available for scanning varied in height, socket material, and liner with which it was worn, showing the evolution of the sub-ischial socket over time that would eventually become the NU-FlexSIV Socket. Socket volume increased 31.3%, from a low of 2659.2 cm3 in 2006 to a high of 3490.6 cm3 in 2016 (Figures 2(a) and 3). Proximal circumferences increased more than distal circumferences with a 15.9% total increase proximally versus 8.9% total increase distally (Figures 2(b) and 3).
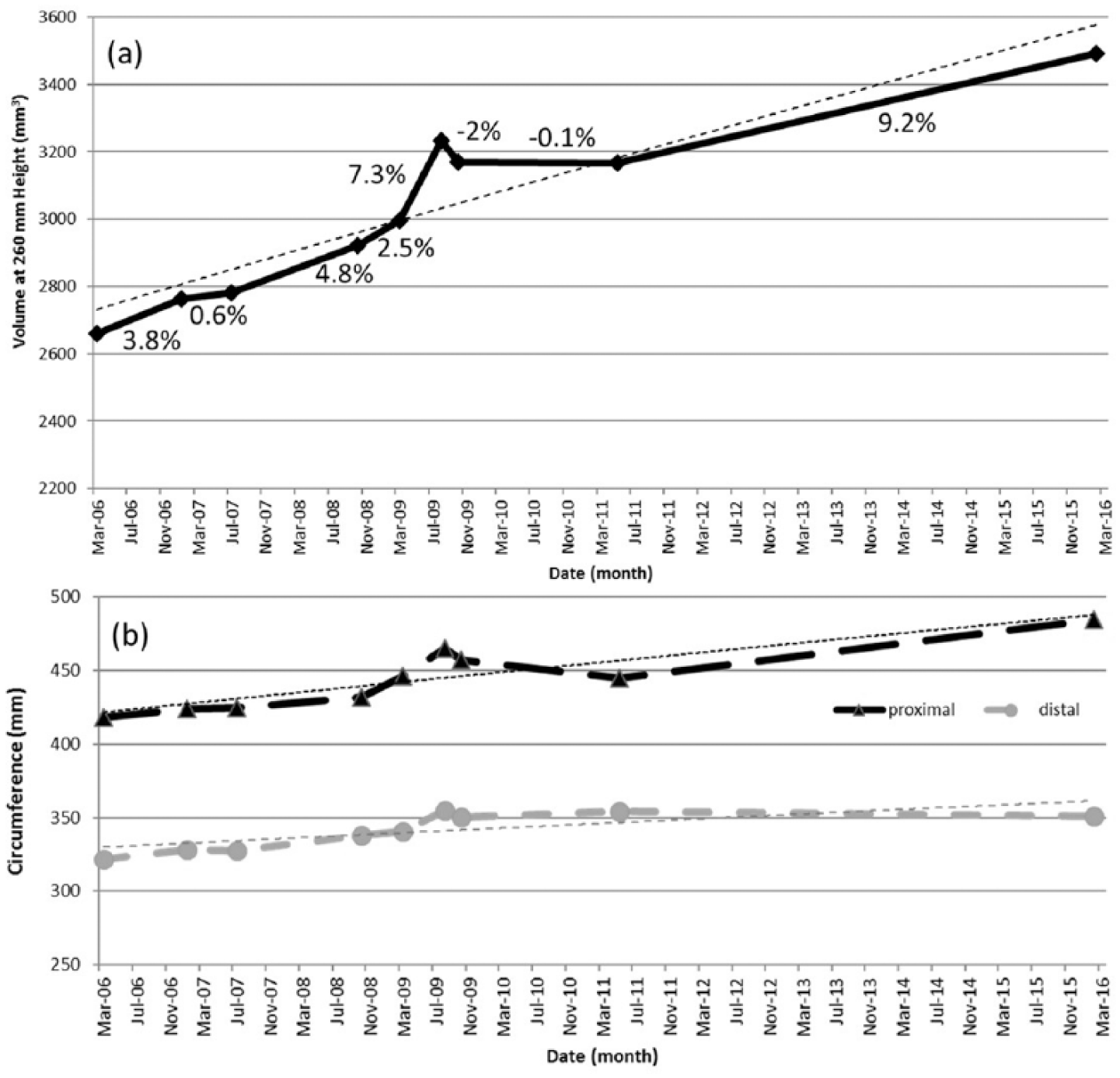
Changes in volume (a) and proximal and distal circumferences (b) over time. Percent change in volume between each socket is shown in (a).
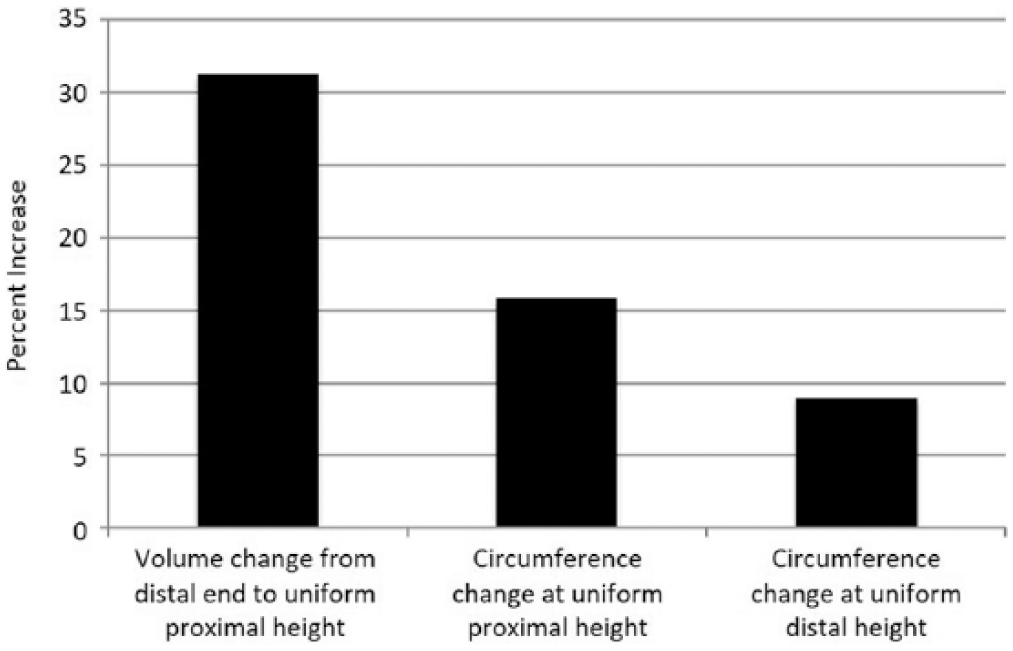
Total percentage increase in volume and proximal and distal circumferences between 2006 and 2016. Uniform proximal height refers to 260 mm proximally from the distal end and uniform distal height refers to 55 m proximally from the distal end.
Discussion
The purpose of this case study was to assess the change in residual limb size over time in a long-time wearer of sub-ischial sockets. Using socket volume and circumferences as a proxy for residual limb size, the results suggest that this individual’s residual limb increased in size over time despite the compressive effect of the socket system. In addition, the increase in circumference was greater proximally than distally, which is likely where the remaining muscle bellies are located. Given these findings and the fact that the subject’s weight remained stable during this period of time, it suggests that the increase in size may have come from muscle hypertrophy. What this means is that, despite the compressive nature of the socket, residual limb atrophy is not a foregone outcome in an amputee who engages in activities such as regular gym workouts and 5K fun runs in addition to an active job working construction. This subject increased his activity level during the 10 years he received these sockets; for example, he learnt to run as an amputee in 2009, coincident with a slight “bump-up” in the volume we calculated.
While residual limb muscular atrophy has been described in the published literature, it is usually discussed in association with disuse of muscles due to the amputation.19,20 In fact, hip extensor strength (which is diminished in persons with lower limb amputation) has been reported to be the strongest predictor of distance walked in persons with lower limb amputation. 21 Although the influence of socket design on hip muscle strength is not known, it is possible that sub-ischial sockets require different hip muscle activation when walking compared to ischial containment sockets. Anecdotal reports from early adopters of the NU-FlexSIV Socket suggest that it may take some individuals a while to adjust to walking in the NU-FlexSIV Socket and that some individuals perceive greater muscular effort initially when walking. There have even been reports from some individuals that they perceive an increase in the size of hip muscles over time, particularly posterior to the hip. The potential relationship between hip muscle strength and socket design would certainly be an interesting one to explore.
Justification for socket replacement is typically based on residual limb volume or shape changes that result in poor socket fit and abrasions to the residual limb or inability to walk. Fernie and Holliday 22 suggested that difficulty with donning the prosthetic socket occurred when residual limb volume increased by 3%–5%. This subject was provided a total of nine sockets over 10 years, which is more than what is typically observed clinically for individuals who wear transfemoral sockets, including the NU-FlexSIV Socket. In addition, some of the percent volume changes did not meet the threshold for socket replacement suggested by Fernie and Holliday. 22 This individual was actively engaged with his prosthetist (R.C.) in the early development of the sub-ischial socket and, as such, received more sockets than clinically necessary, as the prosthetist explored different materials and configurations of socket design. Hence, some of the sockets were provided to accommodate increases in volume and some were to receive feedback on socket iterations. In our experience, clinical application of the NU-FlexSIV Socket does not require replacement of sockets beyond the rate typical for other socket designs.
A limitation of this case study is that we used socket volume as a proxy for residual limb volume. However, the socket was always worn with a liner, the thickness of which will contribute to the total socket volume. Liner thickness can vary across different liners as well as within a liner. Hence, we checked that the liners worn during this study had a similar profile and would therefore have contributed a similarly consistent amount to the calculation of volume across all sockets.
Conclusion
Using socket volume and circumferences as a proxy for residual limb size, we assessed whether the size of the residual limb of a long-time wearer of sub-ischial sockets reduced over time due to the compressive nature of the socket and liner and found that the volume actually increased by 31.3% over a decade.
Footnotes
Acknowledgements
We thank the subject for letting us borrow his sockets; David Firth for assistance with calibration of the digitizer; and Advanced Orthotic and Prosthetic Solutions for providing the ShapeMaker software used in this study.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declarations of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.