
Abstract
Background:
Joint contractures are the main characteristics for children with arthrogryposis multiplex congenita. Orthoses are often used to enable or facilitate walking.
Objectives:
To describe health-related quality of life in children with arthrogryposis multiplex congenita and satisfaction with orthoses in those using orthoses.
Study design:
Cross-sectional study.
Methods:
A total of 33 children with arthrogryposis multiplex congenita participated in the study. Questionnaires were used which measured health-related quality of life (Child Health Questionnaire–Parent Form and EQ-5D youth), mobility and self-care (Paediatric Evaluation of Disability Inventory) and satisfaction with orthoses (Quebec User Evaluation of Satisfaction with Assistive Technology 2.0). Children were divided into groups based on the use of orthoses: Ort-D were dependent on orthoses for walking, Ort-ND used orthoses but were not dependent on them for walking and Non-Ort did not use orthoses.
Results:
Children with arthrogryposis multiplex congenita had significantly lower Child Health Questionnaire scores in 9 of 12 subscales compared to healthy controls. The children’s reported perceived health with EQ-5D youth did not show any difference between children using orthoses or children using only shoes. Paediatric Evaluation of Disability Inventory showed less mobility in Ort-D than in Non-Ort. In total, both orthosis groups were ‘quite satisfied’ with their orthoses.
Conclusion:
Child Health Questionnaire–physical functioning was lowest in children who were dependent on orthoses (Ort-D) for walking. Both Ort-D and Ort-ND were similar satisfied with their orthoses.
Clinical relevance
This study contributes to knowledge about health-related quality of life in a group of ambulatory children with arthrogryposis multiplex congenita. For children using orthoses, it is relevant to capture their opinion about their orthoses but a questionnaire specifically for children should be developed.
Keywords
Background
Arthrogryposis multiplex congenita (AMC) is a heterogeneous condition1,2 with the presence of multiple joint contractures at birth being the main characteristic symptoms. 3 Lower and upper limbs may be involved, but involvement of both are most common. 4 Muscle weakness may occur and has been found to have more impact on walking ability than joint contractures. 5 It has been reported that children with AMC have lower physical activity level 6 and lower functional exercise capacity 7 compared to a healthy control (HC) group.
For many children and their parents, an important goal is to achieve walking function. To enable independent walking by compensating for lower limb deformities and muscle weakness, orthotic support is required. Commonly used orthoses are ankle-foot orthosis (AFO) and knee-ankle-foot orthosis (KAFO) with knee-locking mechanism,7,8 but the use of KAFOs with open knee joints has also been reported.7,8 Because of the heterogeneity among children with AMC, the need of orthoses varies between those walking with solely shoes to those being totally dependent on orthotic support for walking. There is, however, currently no knowledge about how children with AMC perceive their orthoses for walking.
The concept of health-related quality of life (HRQoL) refers to the assessment of various aspects of health and includes physical, mental and social well-being and functioning. 9 For children with motor disorders such as cerebral palsy and myelomeningocele (MMC), parents have reported lower HRQoL compared to a HC group.10,11 In an investigation of health status using EQ-5D-Y (Youth version), 71 children with various motor disorders were included. 12 In this study, the children with AMC reported problems in all of the five dimensions; ‘mobility’, ‘looking after myself’, ‘doing usual activities’, ‘pain or discomfort’ and ‘feeling worried, sad or unhappy’. 12 Since there are only sparse information about HRQoL in children with AMC, the aim of this study was to describe HRQoL in a group of children with AMC and specifically to investigate whether there were any differences between children wearing orthoses compared to those not wearing orthoses. A further aim was to describe the children’s satisfaction with their orthoses.
Methods
Participants
Participants were recruited from three university hospitals in Sweden with well-established treatment for children with AMC. A total of 33 children with mean (standard deviation (SD)) age 10.5 (4.2) (range: 5.0–17.0) years fulfilled the inclusion criteria of (1) AMC with four limb or lower limb involvement, (2) some ambulatory level, (3) age between 5 and 18 years and (4) parent knowledge with reading and understanding the Swedish language, and sufficient knowledge of the child to understand the Swedish language.
Ethical approval for this study was obtained from the Regional Ethical Review Board in Stockholm, Sweden. Written informed consent was obtained from all participants and their parents.
Assessed according to a five-level scale, 13 nine children were household ambulators and wheelchair users for longer indoor distances (Level III). Eleven children were community ambulators, requiring a wheelchair for long distances outdoors only (Level II). Thirteen children were community ambulators with no need for wheelchair use (Level I).
In total, 18 children used orthoses either to enable or to improve walking, of which nine children were found to be dependent on orthoses for walking (Ort-D). Nine children used orthoses but were able to walk short distances indoors without orthoses (Ort-ND). Fifteen children did not use orthoses (Non-Ort).
According to passive range of motion 14 and muscle strength measurements, 15 knee flexion and plantarflexion contractures were more frequently found in Ort-D than in Ort-ND and Non-Ort. Hip flexion contractures did not differ between the groups. Hip and knee flexion contractures were defined as ≥10°, and plantarflexion contractures as ≥5° from a neutral joint position. Twenty-two of the children had some upper limb involvement.
As documented from the medical record, 28 of the 33 children had undergone orthopaedic surgery in their lower limbs and two children had undergone spine surgery. The total number of all performed orthopaedic surgeries was 127, with an average number of 4.4 (range: 1–10) procedures. The number of hip and knee joint procedures did not differ between groups, but foot and ankle surgery was less common in Non-Ort.
Orthoses
The following orthosis types were used by the children: KAFOs with locked knee joints (KAFO-LK), knee orthoses with locked knee joints (KO-LK), KAFOs with open knee joints in the sagittal plane (KAFO-O) and AFOs.7,8 One child used a walking aid. Of the 18 children using orthoses, 14 used them more than 8 h a day, two children between 5 and 8 h a day and two children used their orthoses less than 5 h a day. Twelve children used wheelchair as a complement to walking.
Distribution of functional ambulatory level groups, joint contractures, muscle strength, numbers of performed orthopaedic surgery procedures and orthosis types is shown in Table 1.
Patient characteristics, ambulatory level, joint contractures, muscle strength, performed orthopaedic surgery and orthosis use according to orthosis groups Ort-D (dependent on orthoses for walking), Ort-ND (use orthoses for walking but are not dependent on them) and Non-Ort (do not use orthoses for walking) in a group of children with arthrogryposis multiplex congenita (AMC).
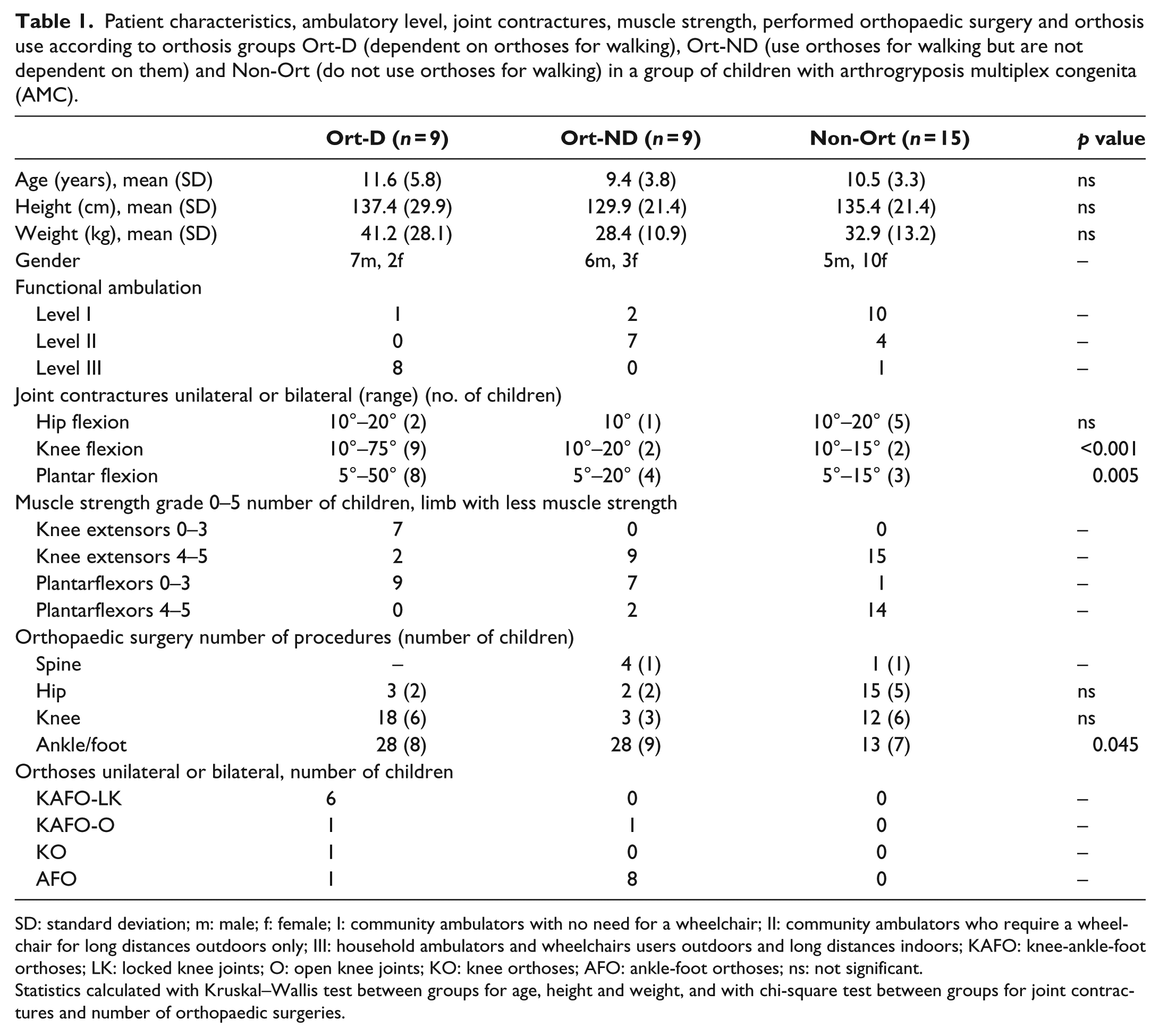
SD: standard deviation; m: male; f: female; I: community ambulators with no need for a wheelchair; II: community ambulators who require a wheelchair for long distances outdoors only; III: household ambulators and wheelchairs users outdoors and long distances indoors; KAFO: knee-ankle-foot orthoses; LK: locked knee joints; O: open knee joints; KO: knee orthoses; AFO: ankle-foot orthoses; ns: not significant.
Statistics calculated with Kruskal–Wallis test between groups for age, height and weight, and with chi-square test between groups for joint contractures and number of orthopaedic surgeries.
Questionnaires
The following instruments were used to gather information about HRQoL, functional capabilities and orthosis satisfaction.
Child Health Questionnaire–Parent Form 50
Child Health Questionnaire (CHQ) is a generic instrument and measures physical and psychosocial components of HRQoL. 16 The Swedish version of the Child Health Questionnaire–Parent Form (CHQ-PF50)17,18 was answered by the parents. The questionnaire consists of 12 subscales, and each is scored from 0 to 100, with 100 reflecting the best function. It is also possible to calculate two summary scores – physical (PhS) and psychosocial (PsS), respectively – each with a norm value of 50. 16 Results from a Swedish reference group of 60 HC with a similar age span (6–18 years) 17 were used for comparison.
EQ-5D-Y
EQ-5D-Y is a generic questionnaire. 19 It is reliable and valid to measure HRQoL in children 8 years or older. 19 The EQ-5D-Y contains of five dimensions and each dimension has three levels of severity: ‘no problems’, ‘some problems’ and a ‘lot of problems’. The questionnaire also contains a visual analogue scale (EQ-VAS) where the child rates its overall health status on a vertical scale between 0 (worst imaginable health) and 100 (best imaginable health). All dimensions and the VAS refer to health state ‘today’. One of the authors (M.E.) was present to answer possible questions for each child. All children aged 8 years or older were considered able to complete the questionnaire
Paediatric Evaluation of Disability Inventory
The Paediatric Evaluation of Disability Inventory (PEDI) measures capabilities and performance of three content domains: self-care, mobility and social function in children aged 6 months to 7 years and 6 months. PEDI can be used for older children if their functional ability is below that expected of 7.5-year-old children with no disabilities. 20 Two out of three content domains were used: self-care and mobility. The functional skills are scored as 0 (unable or limited capability to perform the item in most situations) or 1 (capable of performing item in most situations). The scores were transformed to scaled scores which range from 0 to 100, where 100 reflects the best function. 20 All interviews with the parents were performed by the same person (M.E.).
QUEST 2.0
The Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST 2.0) questionnaire21,22 was used for evaluation of satisfaction with the children’s orthoses and related services. QUEST 2.0 is a valid instrument to capture satisfaction with assistive devices. 21 It comprises 12 items, of which 8 relate to user satisfaction with the device, while 4 relate to service. A 5-level response scale is used to calculate a score for the device, service and a total score 1–5, ‘not satisfied at all’ to ‘very satisfied’. There is also an opportunity to select the three most important items with the device. 21 Children’s understanding of the QUEST 2.0 was tested in a pilot study by one of the authors (L.J.) in a group consisting of eight children with MMC together with their parents. The children with MMC used similar orthoses and were at approximately the same age as the children in our study group of AMC. The pilot study resulted in some modifications in explaining the QUEST items to the parents and the children.
Procedures
CHQ-PF50, EQ-5D-Y and PEDI were administered on the same occasion at the hospital or at the habilitation unit. The parents of all children were asked to answer the CHQ-PF50 questionnaire and were interviewed about their child’s functional capabilities (PEDI) (n = 33). All children aged 8 years or older were asked to fill in the EQ-5D-Y questionnaire (n = 22). For all children using orthoses (n = 18), the parents were given information about the QUEST 2.0 from one of the authors (M.E.). The parents were instructed to answer the questionnaire at home together with the child and send it back to one of the authors (L.V.) who was not involved in manufacturing the orthoses. The parents were asked to include the child’s opinion as much as possible when answering the questions.
Data analysis and statistical analysis
The CHQ-PF50 values were normally distributed except for one domain and a Student’s t-test was used to compare values of the CHQ-PF50 between the entire AMC group and the Swedish control group. A one-way analysis of variance (ANOVA) was used to compare differences between Ort-D, Ort-ND, and Non-Ort. A post hoc analysis was performed.
The Kruskal–Wallis test and post hoc Mann–Whitney U test were used to evaluate differences in PEDI-scaled scores between the Ort-D, Ort-ND, and Non-Ort.
The EQ-5D-Y answers were transformed to percent for each of the five dimensions. The categories ‘some problems’ and a ‘lot of problems’ were combined into the severity level called ‘problems’ before calculation. Because of the low number of participants, the Ort-D (n = 5) and Ort-ND (n = 5) were combined into one group, Ort. To test the differences between Ort and Non-Ort in the percentage of reported problems, the Fischer’s test was used.
The Mann–Whitney U test was used for comparison between Ort and Non-Ort in EQ-5D VAS and between Ort-D and Ort-ND in the QUEST 2.0.
The chi-square test was used to evaluate the presence of contractures and numbers of performed orthopaedic surgery procedures between Ort-D, Ort-ND, and Non-Ort.
Statistical analyses were carried out using commercially available software (SPSS version 23.0). Significance level was set at p < 0.05.
Results
CHQ-PF50
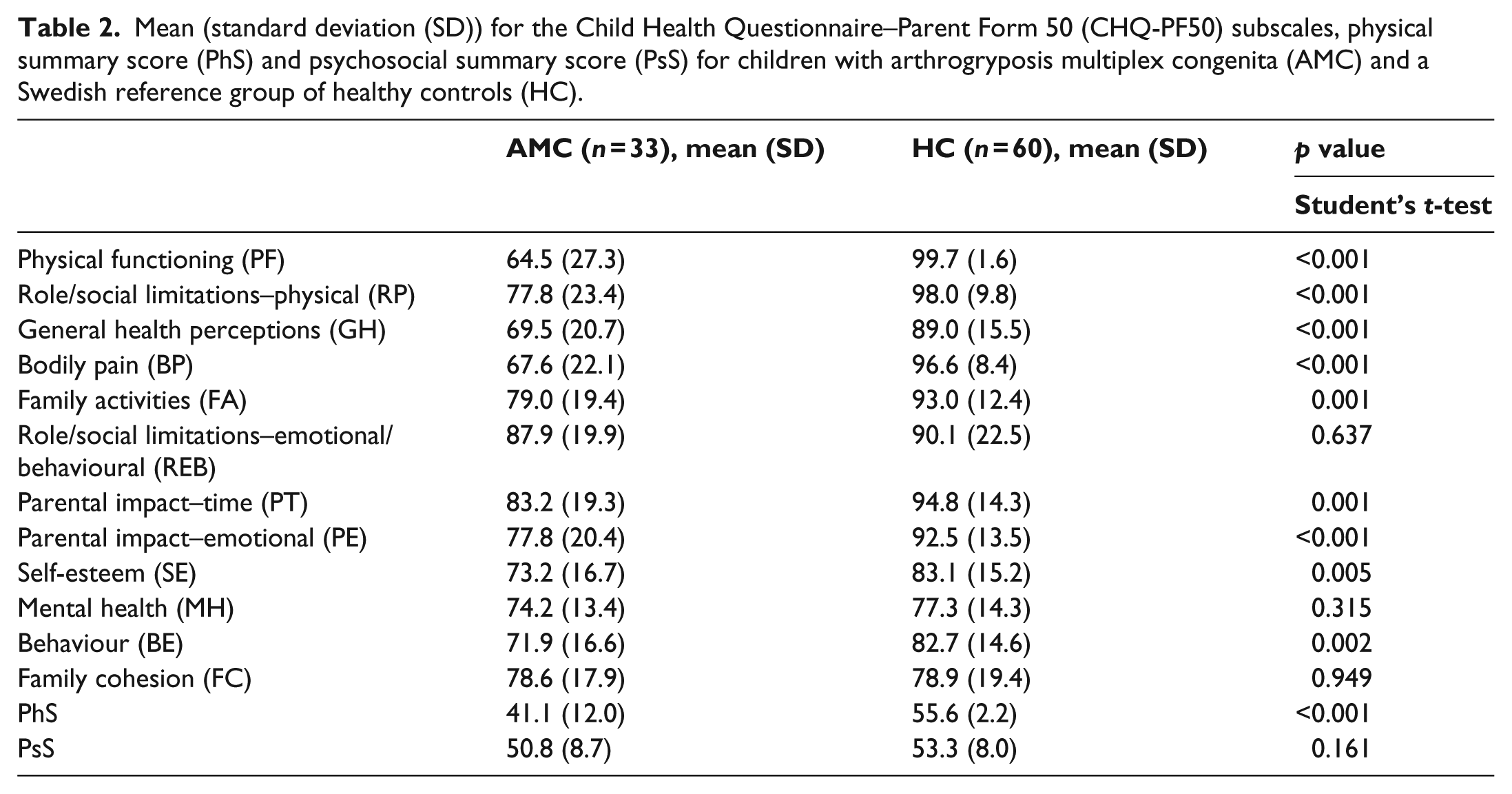
HRQoL measured with the CHQ-PF was significantly reduced in children with AMC as compared to HC in all subscales except role/social limitations–emotional/behavioural (REB), mental health (MH) and family cohesion (FC). The physical summary score was significantly reduced in children with AMC compared to the HC. No difference was found in the psychosocial summary score (Table 2).
Mean (standard deviation (SD)) for the Child Health Questionnaire–Parent Form 50 (CHQ-PF50) subscales, physical summary score (PhS) and psychosocial summary score (PsS) for children with arthrogryposis multiplex congenita (AMC) and a Swedish reference group of healthy controls (HC).
Comparisons of CHQ-PF50 between Ort-D, Ort-ND and Non-Ort, using ANOVA, showed a significant difference in the domain of physical functioning (p = 0.012) with a significant lower score in Ort-D, mean (SD) 38.9 (25.5), compared to Ort-ND, mean (SD) 72.8 (21.1) (p = 0.011) and to Non-Ort, mean (SD) 74.8 (22.2) (p = 0.002).
EQ-5D-Y
The children’s reported perception of their health did not show any difference between Ort and Non-Ort in any of the five dimensions. The mean VAS score was similar between Ort and Non-Ort (Table 3).
Number of children with arthrogryposis multiplex congenita (AMC) aged 8 years and older reporting ‘no problems’ and ‘problems’ in the EQ-5D-Y dimensions, and VAS mean value (SD), in groups Ort (use orthoses for walking) and Non-Ort (do not use orthoses for walking), respectively.
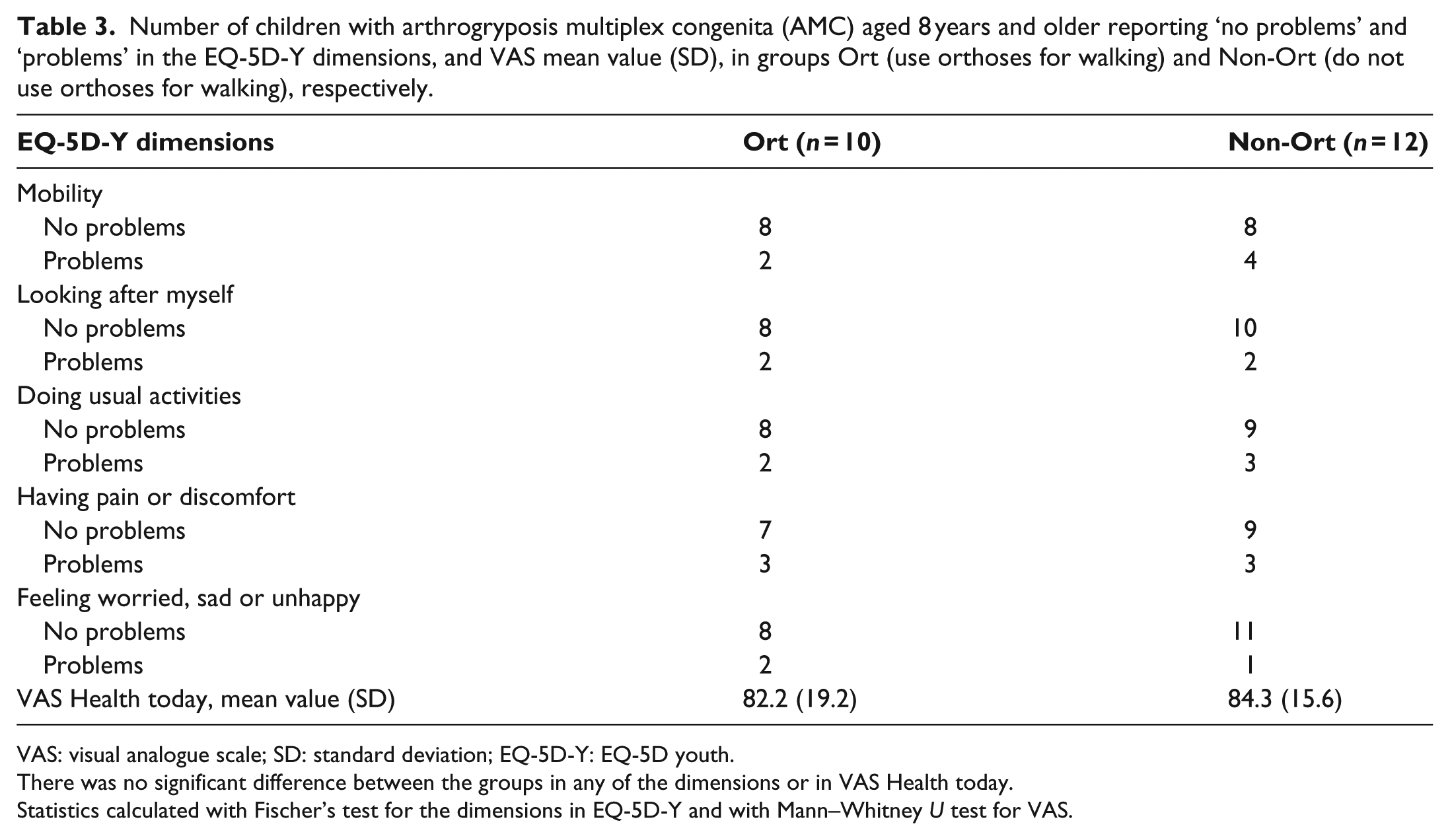
VAS: visual analogue scale; SD: standard deviation; EQ-5D-Y: EQ-5D youth.
There was no significant difference between the groups in any of the dimensions or in VAS Health today.
Statistics calculated with Fischer’s test for the dimensions in EQ-5D-Y and with Mann–Whitney U test for VAS.
PEDI
Mobility scaled scores were reduced in Ort-D compared to Non-Ort (median 79.8 vs 100, p = 0.012). Self-care scaled scores did not differ between the groups (Table 4).
PEDI/functional capabilities in mobility and self-care in children with arthrogryposis multiplex congenita (AMC) reported as median (min–max), in groups Ort-D (dependent on orthoses for walking), Ort-ND (use orthoses for walking but are not dependent on them) and Non-Ort (do not use orthoses for walking), respectively.
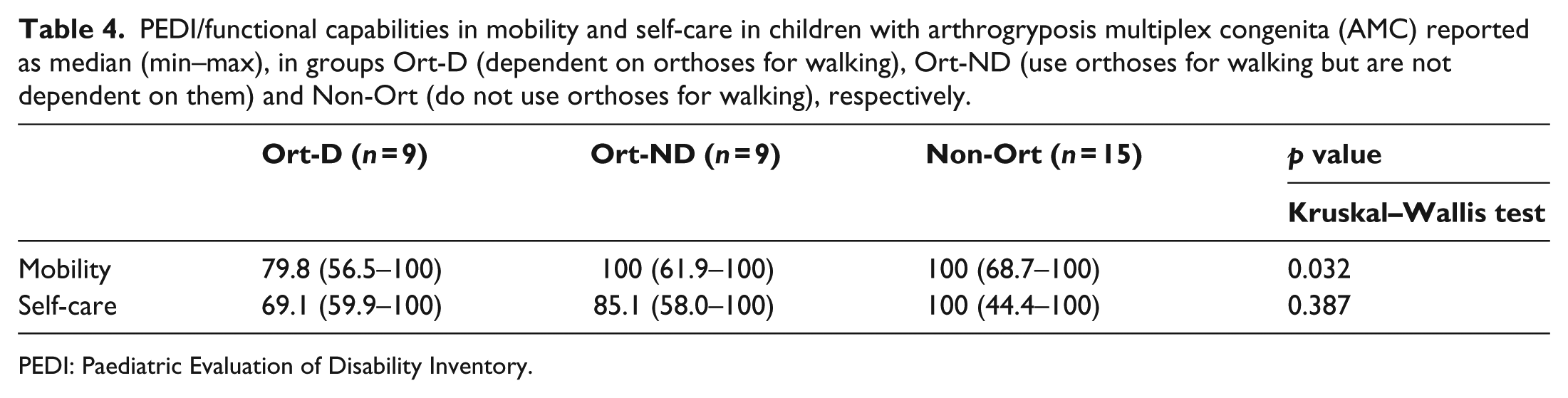
PEDI: Paediatric Evaluation of Disability Inventory.
QUEST 2.0
There was no difference in the total score in the main areas of QUEST 2.0 (Device and Service) between Ort-D and Ort-ND. Ort-D was significantly less satisfied than Ort-ND with the weight of the orthoses (Table 5). The three most important QUEST items reported in Ort-D were Comfort (22.2%), Safety (18.5%) and Easy to use (14.8%), and in Ort-ND they were Easy to use (22.2%), Comfort (22.2%) and Effectiveness (14.8%).
Results of level of satisfaction with orthosis and service measured with the QUEST 2.0 in children with arthrogryposis multiplex congenita (AMC), reported as mean, standard deviation (SD) and median in groups Ort-D (dependent on orthoses for walking) and Ort-ND (use orthoses for walking but are not dependent on them), respectively.
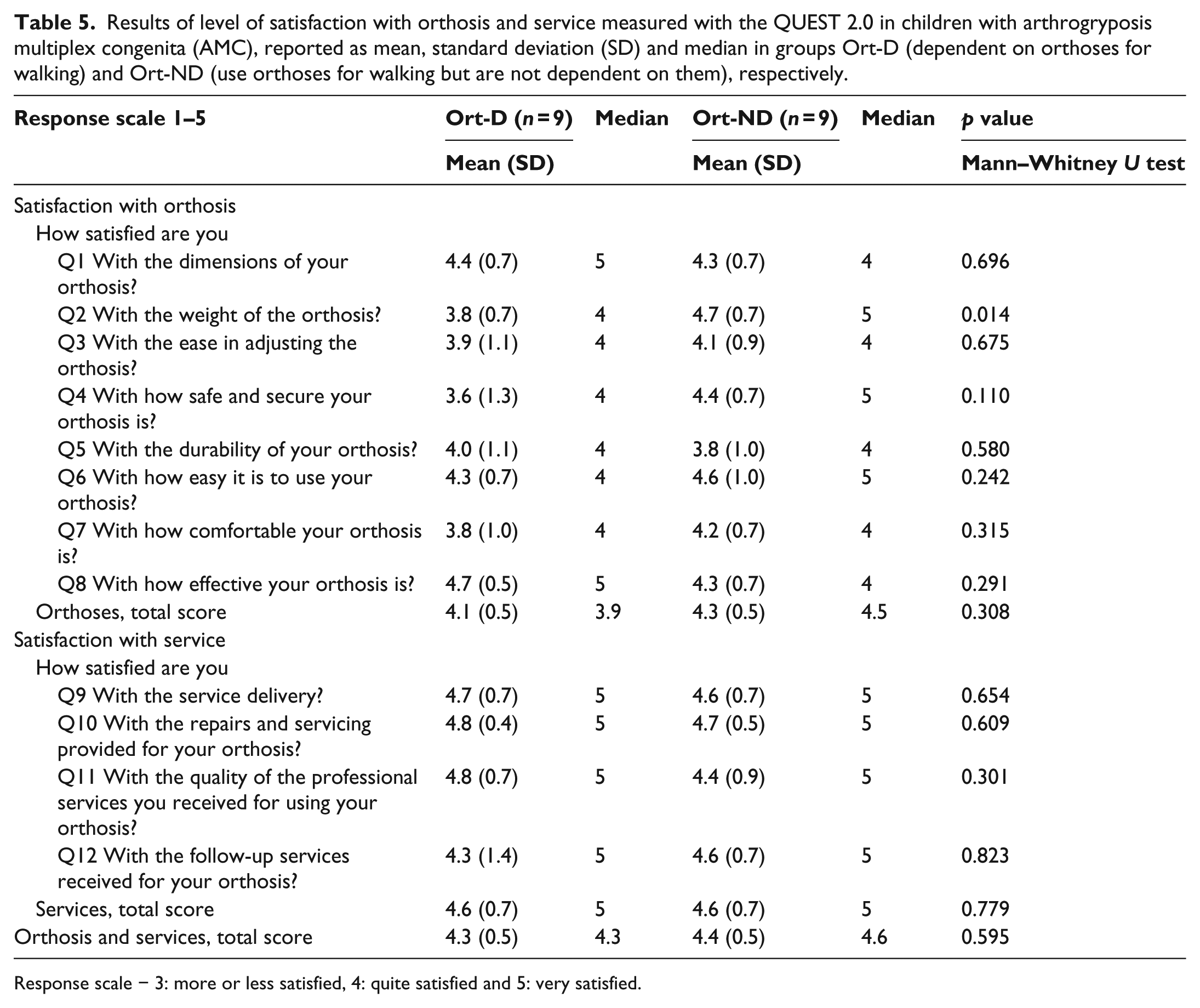
Response scale − 3: more or less satisfied, 4: quite satisfied and 5: very satisfied.
Discussion
When reported by the parents, the children with AMC had lower scores in 9 out of 12 CHQ subscales in comparison with HC. All four subscales relating to physical health and the physical summary score were lower in AMC than in HC. This indicates that lower limb involvement with joint contractures and muscle weakness play an important role for physical health in children with AMC. In the subscales related to psychosocial health, the parents reported lower scores than HC in two of four subscales. The psychosocial summary score, however, was similar between AMC and HC which differs from reported results with lower psychosocial summary scores in children with MMC. 11
In the physical functioning (PF) subscale which measures the presence and extent of physical limitations due to health problems, children with AMC had a lower score than HC. This is in addition to reported findings of lower physical activity 6 and functional exercise capacity 7 in children with AMC compared to HC. Ort-D had no walking ability without orthoses and they had the lowest score in the PF subscale, showing that the children in this group were very limited in performing physical activities. Intensity and frequency of general pain and discomfort (BP subscale) was more frequent in AMC than in HC. In a group of adults with AMC, pain has frequently been reported and was considered to restrict their activities. 23 Satisfaction with school, athletic ability/outlook, looks/appearance, ability to get along with others and family, and life overall (standard error (SE) subscale) was lower in children with AMC than in HC. However, the scores were similar between the groups with AMC indicating that the use of orthoses for walking does not reduce self-esteem compared to those walking without orthoses in this study group.
When reported by the children with EQ-5D-Y, we did not find any difference between the groups in any of the dimensions. With reference to a Swedish general population group aged 8–16 years, 12 our study group of children with AMC reported more problems in ‘mobility’, ‘looking after myself’ and in ‘doing usual activities’. Burström et al. 12 proposed that problems in the dimensions ‘looking after myself’ and in ‘doing usual activities’ might be related to frequent involvement of upper limbs in children with AMC, which was also considered in our study group. The mean EQ-VAS score, imaginable health state today, did not differ between Ort and Non-Ort and was similar to the Swedish general population group. 12 This might be interpreted as children with AMC have a similar perception of their present health state today as the general population group.
As confirmed with PEDI, functional mobility was lowest in Ort-D which may be attributed to the use of locked knee joints in seven out of the nine children. Not being able to flex the knee joint limits walking on stairs and slopes. Furthermore, in those with upper extremity involvement, an inability to grasp the stair railing when walking up and down stairs can also be limiting. We did not find any difference between the groups in self-care, which may be explained by representation of children with upper limb involvement in all groups. As examined with PEDI, children with typical development obtained a scaled score of 100 by the age of 7 years and 6 months; 20 however, in our study, 11 of the children with AMC were below this age which reflects the lower scores in some of the children.
With respect to use of orthoses, both Ort-D and Ort-ND groups achieved a score of four (‘quite satisfied’) by five possible (‘very satisfied’) when grading devices and related services combined. The children in Ort-D were less satisfied with orthosis weight than Ort-ND. This is understandable since Ort-D had less muscle strength as well as orthoses involving thighs and the use of metal knee joints resulting in increased material weight. When choosing one of the three most important items, Ort-D selected ‘safety’ for their orthotic device. This choice by the children confirms the intention of orthotic management to construct orthoses able to withstand strain, thus guaranteeing security. Poor protective responses of the upper extremity have been described 24 which can further explain the importance of feeling safe for those who are dependent on orthoses for walking. Both Ort-D and Ort-ND selected ‘comfort’ as one of the three most important factors. The pilot study showed that the meaning of some words were difficult for children to understand, and thus the item ‘comfort’ was probably proposed by the parent. Our interpretation of ‘comfort’ was that orthoses should be comfortable for the child to wear, and that the orthotic device should correctly fit to the body segments.
It has been reported that there is a higher rate of satisfaction in children who use the device as intended than in those who underutilised the device. 25 In our study, 14 out of 18 children used their orthoses for more than 8 h a day which may be interpreted as a high level of satisfaction with orthoses and emphasises the importance of each child’s opinion. According to the experiences of adults with AMC, professionals have the technical expertise but still the patients know more about their own needs. 23 The QUEST was developed for assessing the satisfaction of assistive devices in general and is not only limited to orthoses and prostheses.21,22 A child version of QUEST 2.0 concerning schoolwork assistive technology has been reported 26 but was not considered useful in children using orthotics for walking. To our knowledge, there is no instrument available today that solely measures the satisfaction of orthoses and prostheses for the child population. Since we instructed parents to fill in the questionnaire together with their child, we believe that the children’s opinions are present as much as possible. QUEST 2.0 has not yet been validated for children; however, from our perspective, the responses seem relevant with respect to the children’s functional disabilities and possibilities. Nevertheless, a questionnaire for children is required in the future to enable valid responses from the child’s point-of-view. A limitation of the study may be seen in the small participant number, allowing only minor differences between the groups with AMC. AMC, however, is a rare disorder including various subtypes, which have to be accounted for both in research and in clinical practice.
Conclusion
Children with AMC had lower HRQoL than HCs in domains related to physical health of which PF was lowest in children who were dependent on orthoses (Ort-D) for walking. There were no differences in children’s perception of health state between children using orthoses (Ort) or not using orthoses (Non-Ort) for walking. Both Ort-D children and Ort-ND children were similar satisfied with their orthoses.
Footnotes
Acknowledgements
The authors would like to thank the children and their parents for participating in the study. This study was supported by the Jerring Foundation and Norrbacka-Eugenia Foundation.
Author contribution
M.E., L.J. and Å.B. designed the study. M.E., L.V. and A.-K.K. collected the data. The manuscript was prepared by M.E. and Å.B. All authors contributed to and have approved the final article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.